Brown-sequard syndrome caused by cervical disc herniation: case report and review of the literature.
5
0
0
全文
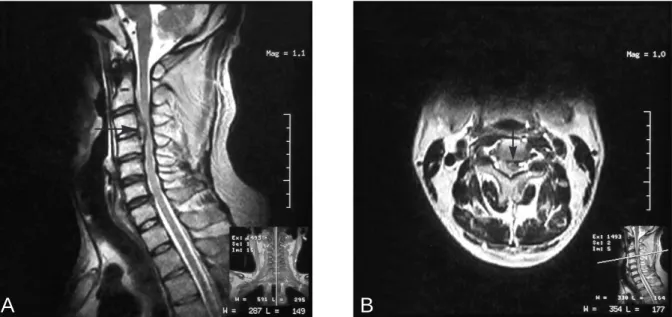
(2) Chih-Hsiu Wang, et al.. A. 63. B. Fig. 1. Preoperative MRI shows a large left extradural paramedian C3-C4 disc herniation, with cord compression. A: Sagital view. B: Axial view.. operation, the patient remained in a rigid cervical collar for 4 weeks. The postoperative course was satisfactory. His weakness and both sensation of pain and temperature had recovered completely one month after surgery. The postoperative MRI and X-rays showed total decompression of the cord and roots and interbody fusion with the polyetheretherketone (PEEK) cage (Fig. 2). DISCUSSION. Fig. 2. Postoperative X-rays show interbody fusion with a polyetheretherketone (PEEK) cage.. performed with a polyetheretherketone (PEEK) cage (Stryker) containing a core of triosite (Zimmer) [1,2]. Before the closure of the superficial layers, an intraoperative lateral radiograph control was taken, and the correct position of the implant was checked. After the. Only a few cases of Brown-Sequard syndrome produced by cervical disc herniation have been published since 1928. However, cervical disc herniation is a common disorder. Large paracentral disc herniation with severe hemicord compression is also not unusual. We believe that Brown-Sequard syndrome produced by cervical disc herniation is not rare and is often underdiagnosed. The first characteristic finding of discogenic Brown-Sequard syndrome is contralateral deficit in sensation of pain and temperature. This is an obscure perception and is often ignored by patients themselves. Without this chief complaint, physicians can detect the deficit only by very detailed neurological examination. However, there are many reasons why physicians.
(3) 64. Brown-Sequard Syndrome and Cervical Disc Herniation. skip detailed neurological examininations to a brief one. Hemiparasis without significant cervical symptoms is the first reason. In our patient, the initial presentation was hemiparasis without neck pain. This symptom pointed to a supratentorium cerebral vascular accident. However, when the brain MRI showed normal findings, we revised our neurological examination and found contralateral analgesia and thermanesthesia. Brown-Sequard syndrome caused by cervical lesion was suspected. Cervical MRI then confirmed the diagnosis of discogenic BrownSequard syndrome. Severe and definite radicular sign is another reason. When patients come to the clinic with severe pain and parathesia of neck and limb, they are quickly diagnosed as having cervical disc herniation with radiculopathy after the cervical MRI. However, contralateral deficit in sensation of pain and temperature may coexist but is often disregarded. This is a special condition, which needs to be evaluated. In the literature, half of the cases of Brown-Sequard syndrome produced by cervical disc herniation (12 of 24) had preceded or accompanied radicular signs and symptoms [3-11]. Pure Brown- Sequard syndrome is rare. Fragments of the syndrome plus additional symptoms and signs are more common [11]. The second characteristic finding of discogenic Brown-Sequard syndrome is paracentral protrusion of the disc with cervical spinal stenosis. In the literature, the location of the cervical disc herniation was paracentral in the majority of cases (22 of 24) [6-15]. When a paracentral protrusion of the disc with cervical spinal stenosis is noted from cervical MRI, the sensation of pain and temperature showed be evaluated. The number of reports of Brown-Sequard syndrome produced by cervical disc herniation is increasing because of the easy application of MRI. Accurate diagnosis has made rapid operation and promising recovery possible. Brown-Sequard syndrome produced by a cervical disc herniation is presumably often. underdiagnosed. Characteristic findings in most cases of discogenic Brown-Sequard syndrome are contralateral deficit in sensation of pain and temperature of more than a few levels below the level of cord compression and paracentral protrusion of the disc with cervical spinal stenosis. Outcomes are generally more favorable in patients for whom rapid diagnosis on MRI leads to spinal cord decompression treatment using surgical approach. REFERENCES. 1. Cho DY, Liau WR, Lee WY, et al. Preliminary experience using a polyetheretherketone (PEEK) cage in the treatment of cervical disc disease. Neurosurgery 2002;51:1343-50. 2. Cho DY, Lee WY, Sheu PC, et al. Cage containing a biphasic calcium phosphate ceramic (Triosite) for the treatment of cervical spondylosis. Surg Neurol 2005; 63:497-504. 3. Stookey B. Compression of the spinal cord due to ventral extradural cervical chondromas. Diagnosis and surgical treatment. Arch Neurol Psychiatry 1928;20:275-91. 4. Eisenberg RA, Bremer AM, Northup HM. Intradural herniated cervical disk: a case report and review of the literature. AJNR Am J Neuroradiol 1986;7:492-4. 5. Finelli PF, Leopold N, Tarras S. Brown-Sequard syndrome and herniated cervical disc. Spine 1992;17: 598-600. 6. Antich PA, Sanjuan AC, Girvent FM, et al. High cervical disc herniation and Brown-Sequard syndrome. A case report and review of the literature. J Bone Joint Surg Br 1999;81:462-3. 7. Clatterbuck RE, Belzberg AJ, Ducher TB. Intradural cervical disc herniation and Brwon-Sequard's syndrome. Report of three cases and review of the literature. [Review] J Neurosurg 2000;92(2 Suppl): 236-40. 8. Borm W, Bohnstedt T. Intradural cervical disc herniation. Case report and review of the literature. [Review] J Neurosurg 2000;92(2 Suppl):221-4. 9. Iwamura Y, Onari K, Kondo S, et al. Cervical intradural disc herniation. Spine 2001;26:698-702. 10. Kobayashi N, Asamoto S, Doi H, et al. BrownSequard syndrome produced by cervical disc herniation: report of two cases and review of the literature. [Review] Spine J 2003;3:530-3..
(4) Chih-Hsiu Wang, et al.. 11. Mastronardi L, Ruggeri A. Cervical disc herniation producing Brown-Sequard syndrome: case report. Spine 2004;29:28-31. 12. Roda JM, Gonzalez C, Blazquez G, et al. Intradural herniated cervical disc. Case report. J Neurosurg 1982; 57:278-80. 13. Rumana CS, Baskin DS. Brown-Sequard syndrome produced by cervical disc herniation: case report and literature review. Surg Neurol 1996;45:359-61.. 65. 14. Kohno M, Takahashi H, Yamakawa K, et al. Postoperative prognosis of Brown-Sequard-type myelopathy in patients with cervical lesions. Surg Neurol 1999;51:241-6. 15. Schneider SJ, Grossman RG, Bryan RN. Magnetic resonance imaging of transdural herniation of a cervical disk. [Report] Surg Neurol 1988;30:216-9..
(5) 66. Brown-Sequard Syndrome. 44. B r ow n -. Sequard syndrome. Brown-Sequard syndrome 1). 2) Brown-Sequard syndrome 2006;11:62-6. Brown-Sequard syndrome. 403. 2. 2005. 5. 25. 2005. 8. 30. 2005. 8. 12.
(6)
數據
相關文件
Crystal-storing histiocytosis (CSH), a rare condition in which crystalline material accumulates in the cytoplasm of histiocytes, is typically associated with disorders that
The hypothesis of heterotopia may explain the origin of sali- vary tissue in parotideal lymph nodes, in the periparoti- deal region and the upper neck, but fails to explain the
“Cowden’s syndrome affecting the mouth, gastrointestinal, and central nervous system: a case report and review of the literature,” Oral Surgery, Oral Medicine, Oral Pathology,
The percentage of positive LSGBs was significantly higher in patients in whom the biopsy was performed by or on the request of either the department of Rheumatology and Internal
Axial (A), sagittal (B) and coronal (C) CBCT sections demonstrating a well defined radiolucency, with the attenuation of air, at the inferior margin of the C2 vertebral body,
On magnetic resonance imaging (MRI), the presentation is less specific. The lesion demonstrates hypointense signals on both T1- and T2-weighted images, without gadolinium
The authors report a case of a 71-year-old woman in which the numb chin syndrome was the first symptom of the diffuse large B-cell lymphoma, which caused infiltration and
(2) In each side of the mandible, the impacted teeth (the second and third molars) had their occlusal surfaces contac ng each other in a single follicular space.. Treatment
