Effects of Elasticity and Structure of Trabecular Bone on the
Primary Stability of Dental Implants
Heng-Li Huang
1Ming-Gene Tu
1Lih-Jyh Fuh
1Yuan-Chien Chen
1Chu-Lung Wu
2Shou-I Chen
3Jui-Ting Hsu
1,*1School of Dentistry, College of Medicine, China Medical University, Taichung 404, Taiwan, ROC 2Department of Special Education, National Taichung University, Taichung 403, Taiwan, ROC
3National Center for High-Performance Computing, Hsinchu 300, Taiwan, ROC
Received 16 Nov 2009; Accepted 15 Jan 2010
Abstract
This study evaluated the effects of elastic modulus and cellular characteristics of trabecular bone on the primary stabilities of dental implants. Artificial jawbone models with six values of elastic modulus (137, 123, 47.5, 22, 12.4, and 6.5 MPa) comprising three kinds of trabecular structure (solid rigid, and cellular rigid with closed-cell and open-cell characteristics) were investigated in terms of the peak insertion torque value (ITV), implant stability quotient (ISQ), and Periotest value (PTV) as measured using a torque meter, OsstellTM resonance frequency analyzer, and PeriotestTM electronic device, respectively. All specimens adhered to 2-mm-thick short-fiber-filled epoxy sheets to mimic the cortical shell, and screw-type implants were placed in the models for measuring the implant stability. In general, the ITV, PTV, and ISQ increased with the elastic modulus of cellular trabecular bone. The differences in the primary stabilities of the implants between closed-cell and open-cell bone specimens (12.4 versus 6.5 MPa) were 52% for ITV, 2-fold for PTV, and 8% for ISQ. The regression correlation coefficient (R2) values between the elasticity of trabecular bone with a cellular (closed-cell) structure and ITV, PTV, and ISQ were 0.73 (with linear regression model), 0.93 (with linear regression model), and 0.89 (with logarithmic regression model), respectively. These linear and logarithmic models demonstrate the strong correlations of the elastic modulus of trabecular bone with the obtained ITV, PTV, and ISQ values. Trabecular bone with an osteoporotic structure decreases the primary implant stability. The use of cellular artificial jawbones as experimental models revealed that the elastic modulus and osteoporotic trabecular bone both influence the ITV, PTV, and ISQ primary implant stability parameters. Due to a similarity of trabecular structure, cellular characteristic of artificial bone might be more appropriate for obtaining accurate values of the primary implant stability than solid-bone blocks.
Keywords: Primary implant stability, Elastic modulus of trabecular bone, Insertion torque value (ITV), Implant stability quotient (ISQ), Periotest value (PTV)
1. Introduction
The dental implant has recently become a reliable and predictable tool for oral rehabilitation. The successful clinical outcome of an implant is influenced by many factors, including the implant body, surgical skill, and oral environment, but the key factor for success is the primary stability at implant placement, which is most affected by the quality of the alveolar bone [1-3]. The primary stability increases with the bone quality, since this improves the osseointegration and thereby increases the survival probability * Corresponding author: Jui-Ting Hsu
Tel: +886-4-22053366 ext. 2308; Fax: +886-4-22014043 E-mail: [email protected]
of the dental implant. The failure rate of dental implants is high in poor-quality bone [4,5], and the bone quality is higher for the mandible than for the maxilla, and higher for the anterior region than for the posterior region [6,7]. In addition, the survival rate is higher for dental implants in the mandible than for those in the maxilla, particularly in the anterior region [1,5,8,9].
Host bone characteristics such as cortical bone thickness and the strength/density of trabecular bone significantly influence the implantation success. The bone quality is clinically classified into types 1–4 according to Lekholm and Zarb [10] based on the amounts of cortical bone versus trabecular bone evident on pantograph film. Misch et al. [11] further characterized these four bone types based on a subjective assessment by the surgeon during drilling.
Previous research has shown that only 3% of implants placed in bone of type 1, 2, or 3 are lost, whereas the failure rate was 35% in type-4 bone, corresponding to a thin cortical shell and softer trabecular bone [4]. Both orthopedic and dental implant research has indicated that the strength of trabecular bone significantly influences the holding strengths of implants [12,13].
Greater primary stability, which corresponds to less micromotion between the implant and bone, is required for osseointegration during the healing period. In both clinical and laboratory situations, several noninvasive measures – including the peak insertion torque value (ITV), Periotest value (PTV), resonance frequency analysis (RFA) (usually evaluated as the implant stability quotient, ISQ) [14], and peak removal torque value (RTV) [15,16] – can be used to diagnose the stability problems of an implant that might be related to a thin cortical bone thickness or poor quality of trabecular bone [17,18]. The bone quality can differ with the implant location, which therefore greatly affects the probability of implant success. It is about 4% higher in the mandible than in the maxilla, and higher in the anterior region than in the posterior region (about 12% and 4% in the maxilla and mandible, respectively). The literature suggests that dental implants are most successful in the anterior mandible and least successful in the posterior maxilla [1], which might be explained by another study’s finding that the mean bone density was highest in the anterior mandible, followed by the anterior maxilla, posterior mandible, and posterior maxilla [19].
The clinical use of the Lekholm and Zarb classification only provides a rough assessment of the quality and quantity of jaw bone – the precise relationships of bone quality and quantity with implant stability are still unclear and remain to be determined [10]. Therefore, this study evaluated how the primary stability of an implant is affected by the elastic modulus of trabecular bone.
2. Materials and methods
2.1 Specimen preparation
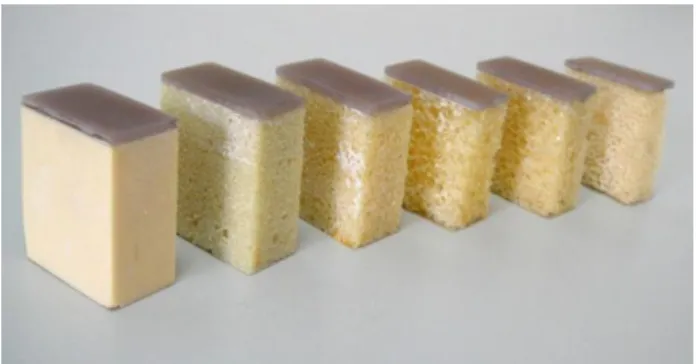
One solid-and-rigid (elastic modulus of 123 MPa) and four cellular-but-rigid (elastic moduli of 137, 47.5, 23, and 12.4 MPa) polyurethane-foam blocks of artificial jawbones (models 1522-02, 1522-09, 1522-10, 1522-11, and 1522-12, Pacific Research Laboratory, Vashon Island, WA, USA) were used to mimic the trabecular bone of the jaw. Osteoporosis was simulated using another cellular trabecular bone block with the open-cell characteristic (elasticity equal to 6.5 MPa; model 1522-505, Pacific Research Laboratory). All the trabecular-bone blocks were attached to 2-mm-thick cortical shells made from short-fiber-filled epoxy sheets with an elastic modulus similar to that of human cortical bone (16,700 MPa; model 3401-01, Pacific Research Laboratory) (Fig. 1).
Figure 1. Models of trabecular bone used in the experiments. From left to right: 123-MPa solid-and-rigid polyurethane-foam block; 137-, 47.5-, 23-, and 12.4-MPa closed-cell blocks; and 6.5-MPa open-cell block. All blocks had 2-mm-thick cortex attached.
2.2 Implant stability determination
Pilot holes were drilled into each bone block specimen using a 3.2-mm drill, and a 4-mm 12-mm screw-type implant (ATLAS Implant System, Cowell Medi, Busan, South Korea) (Fig. 2) was inserted. The peak ITV (in N•cm) was recorded three times for each specimen using a digital torque meter (TQ-8800, Lulton Electronic Enterprise, Taipei, Taiwan). Then the OsstellTM resonance frequency analyzer (Osstell, Göteborg, Sweden) (Fig. 3a) was used to measure implant stability. The L-shaped transducer (Type F1 L5, Osstell) was maintained perpendicular to the implant and screwed by hand into the implant body, as recommended by the manufacturer. After connecting a 6-mm length of temporary abutment (implant temporary hex cylinder, 3i implant innovation, palm beach, FL, USA), the mobility of the implants was measured using the PeriotestTM device (Siemens, Bensheim, Germany) (Fig. 3b). The tip of the measurement device was placed perpendicular to the abutment at a distance of 2 mm, and it impacted the implant four times per second for 4 seconds. The synthetic bone had a rectangular shape with dimensions of 38 mm × 20 mm × 42 mm. Three specimens of each combination of artificial cortical and trabecular bone were prepared for implant stability measurements.
(a)
(b)
Figure 3. Setups for measuring (a) the OsstellISQ and (b) the PTV.
2.3 Statistical analysis
The measures of primary stabilities (ITV, PTV, and ISQ) of the implants for the designed scenarios of the elastic moduli values of trabecular bone were summarized as mean ± standard deviation (SD) values, with differences between them tested using one-way analysis of variance. The nonlinear relation between stability and the elastic modulus of trabecular bone with a closed-cell structure was modeled separately with linear and logarithmic regression models. All statistical analyses were performed with SAS software (v9.1.2, SAS Institute, Cary, NC, USA).
3. Results
Table 1. Elastic modulus and peak insertion torque value (ITV), Periotest value (PTV), and implant stability quotient (ISQ) of artificial jawbone specimens.
Specimen structure Elastic modulus ITV (mean±SD) PTV (mean±SD) ISQ (mean±SD) Solid and rigid 123 34.3±2.9 -6.3±0.6 88.0±1.0
Cellular but rigid
137.0 31.3±2.9 -4.3±0.6 82.7±1.5 47.5 27.2±2.8 1.3 ±0.6 78.3±0.6 23 23.3±2.1 2.7±1.2 74.0±2.0 12.4 16.3±1.2 6.0±1.0 63.7±0.6 Open cell but rigid 6.5 7.8±0.6 18.3±2.5 58.7±1.5
Unit MPa N•cm
P* <0.001 <0.001 <0.001
*
One-way analysis of variance
The ITV, PTV, and ISQ values of all specimens are listed in Table 1. In general, ITV and ISQ increased and PTV decreased as the elastic modulus of the trabecular bone increased. Additionally, the apparent differences in primary stabilities of implants between bone specimens with
closed-cell and open-cell structures (12.4 versus 6.5 MPa) were 52% for ITV, 2-fold for PTV, and 8% in ISQ.
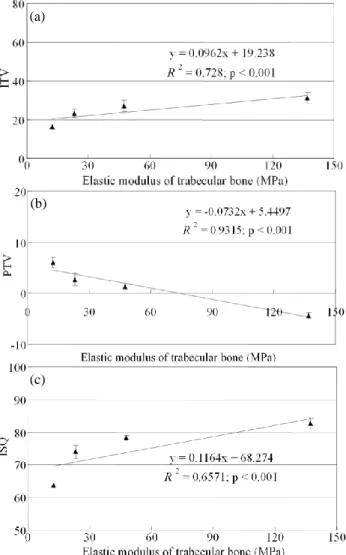
The linear regression correlation coefficient (R2) values between the elasticity of trabecular bone with the cellular (closed-cell) structure and ITV, PTV, and ISQ are shown in Fig. 4, and were 0.73, 0.93, and 0.66, respectively. These results suggest that ITV and PTV are more linearly correlated with the biomechanical properties (i.e., the elastic modulus) of bone.
Figure 4. Linear regression models of the relationships of the elastic modulus of trabecular bone with (a) the peak ITV, (b) PTV, and (c) ISQ.
4. Discussion
Several studies have indicated that the survival rate of a dental implant is greatly affected by the host bone quality [1-3]. Therefore, evaluating the bone condition is essential to the dentist ensuring the long-term success of an implant before implant surgery. X-ray and cone-beam computed tomography are useful techniques for noninvasively obtaining information on the bone quality, including the structure of the bone tissue and its density.
Measuring the primary implant stability is another method for clinically predicting implant success. Since the primary stability of an implant is also significantly related to
(a)
(b)
bone quality and quantity [14], many studies have used ITV, PTV, and ISQ values as stability indexes. However, the subjective estimation approach of the Lekholm and Zarb [10] bone-type classification only provides rough information on the quality and quantity of jaw bone. However, obtaining standardized samples with similar bone quality and quantity for clinical studies and laboratory experiments is very difficult. Therefore, artificial bone might be an option for investigating the primary implant stability of trabecular bone with a precisely known strength [13,20-23].
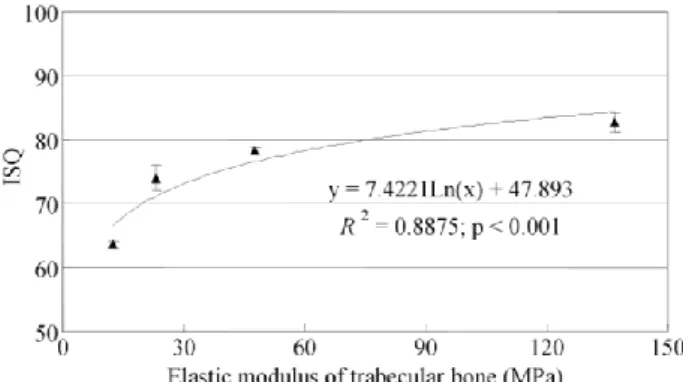
In this study, the indexes of primary stabilities (ITV, PTV, and ISQ) varied with the elastic modulus of trabecular bone. Additionally, linear regression models revealed that only PTV has a strong and linear correlation with the elastic modulus of trabecular bone (R2 > 0.93 for PTV, R2 > 0.66 for ISQ). However, according to the result of logarithmic regression model of ISQ (Fig. 5), PTV has a strong relationship with the elastic modulus of trabecular bone (R2 >0.89 for ISQ). These results suggest that the initial stabilities of implants as measured by RFA and PTV are influenced by the strength of trabecular bone, with PTV decreasing linearly and ISQ increasing logarithmically as the strength of trabecular bone increases (Fig. 5). This result may reflect a stronger bone-to-nonosseointegrated implant anchorage [24], since dense cellular structure of trabecular bone may provide more contact area between implant and bone. There was also a linear correlation between ITV and the elastic modulus of trabecular bone (R2 > 0.73).
Figure 5. Logarithmic regression models of the relationships of the elastic modulus of trabecular bone with ISQ.
The present results indicate that the elastic modulus of bone is not the only factor affecting the primary stability of an implant. ISQ was higher and PTV was lower for the solid-and-rigid jawbone model than for the cellular-but-rigid jawbone model, even though the elastic modulus was lower for the former (123 versus 137 MPa). This indicates that caution is necessary when using jawbone specimens as experimental bone models. If the porous and cellular morphology of trabecular bone is not present, the experimental outcomes might produce erroneous predictions, especially when investigating the primary stability (PTV and ISQ) of an implant. The present study indicated that bone models with a cellular structure might be superior for elucidating the importance of primary implant stability, because their architecture is similar to that of trabecular bone.
Osteoporosis is associated with a decrease in bone mass and density and a resulting increase in bone fragility, leading to an increased risk of fracture [25]. Even though there is a general consensus that osteoporosis is not a risk factor for poor implant osseointegration [26,27], recent studies have found a significant association between osteoporosis and early implant failure [28,29]. The open-cell structure of osteoporotic bone reduces the initial implant stability. It is suggested that the clinical diagnosis of the primary implant stability is especially important for patients who are potentially at risk of osteoporosis (e.g., the elderly and women aged 50–75 years, due to a sudden decrease in sex hormone levels), in order to improve implant osseointegration if they receive medical treatment [29].
5. Conclusions
This study obtained the relationships of the implant stabilities (ITV, PTV, and ISQ) with precised value of strength of trabecular bone; however, there are still limitations (e.g., a lack of anatomic geometry and viscoelastic properties of bone) which may influence stability of implant and remained the further investigation. Within the limitations of this study, the following conclusions can be drawn:
(1) The elastic modulus of trabecular bone influences parameters that reflect the primary stability, such as ITV, PTV, and ISQ. Additionally, linear and logarithmic models indicate the strong correlations of the elastic modulus of trabecular bone with the obtained ITV, PTV, and ISQ values. Trabecular bone with an osteoporotic structure reduces the primary stability of an implant.
(2) Caution is required when using artificial jawbones as experimental models since characteristic of bone type is also a factor influencing primary implant stability. Using bone models with a cellular structure might be more appropriate for obtaining accurate values of the primary implant stability than solid-bone blocks, because their architecture is similar to that of trabecular bone.
Acknowledgements
The study was supported by the Metal Industries Research & Development Centre, China Medical University (CMU96-277 & CMU98-S-52) and the National Science Council (NSC 98-2320-B-039-005 MY3) in Taiwan.
References
[1] L. Tolstunov, “Implant zones of the jaws: implant location and related success rate,” J. Oral Implantol., 33: 211-220, 2007. [2] R. B. Johns, T. Jemt, M. R. Heath, J. E. Hutton, S. McKenna, D.
C. McNamara, D. van Steenberghe, R. Taylor, R. M. Watson and I. Herrmann, “A multicenter study of overdentures supported by Branemark implants,” Int. J. Oral Maxillofac. Implants., 7: 513-522, 1992.
[3] R. Lazzara, A. A. Siddiqui, P. Binon, S. A. Feldman, R. Weiner, R. Phillips and A. Gonshor, “Retrospective multicenter analysis of 3i endosseous dental implants placed over a five-year period,” Clin. Oral Implants Res., 7: 73-83, 1996.
[4] R. A. Jaffin and C. L. Berman, “The excessive loss of Branemark fixtures in type IV bone: a 5-year analysis,” J. Periodontol., 62: 2-4, 1991.
[5] T. Jemt and U. Lekholm, “Implant treatment in edentulous maxillae: a 5-year follow-up report on patients with different degrees of jaw resorption,” Int. J. Oral Maxillofac. Implants., 10: 303-311, 1995.
[6] I. Turkyilmaz, T. F. Tozum and C. Tumer, “Bone density assessments of oral implant sites using computerized tomography,” J. Oral Rehabil., 34: 267-272, 2007.
[7] R. C. de Oliveira, C. R. Leles, L. M. Normanha, C. Lindh and R. F. Ribeiro-Rotta, “Assessments of trabecular bone density at implant sites on CT images,” Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod., 105: 231-238, 2008.
[8] R. Adell, U. Lekholm, B. Rockler and P. I. Branemark, “A 15-year study of osseointegrated implants in the treatment of the edentulous jaw,” Int. J. Oral. Surg., 10: 387-416, 1981. [9] M. Esposito, J. M. Hirsch, U. Lekholm and P. Thomsen,
“Biological factors contributing to failures of osseointegrated oral implants. (II). Etiopathogenesis,” Eur. J. Oral Sci., 106: 721-764, 1998.
[10] U. Lekholm and G. A. Zarb, “Patient selection and preparation,” in: P. I. Brånemark, G. A. Zarb, T. Albrektsson (Eds.), Tissue-Integrated Prostheses: Osseointegration in Clinical Dentistry, Chicago: Quintessence, 199-209, 1985.
[11] C. Misch, “Classifications and treatment options of the completely edentulous arch in implant dentistry,” Dent. Today, 9: 8-30, 1990.
[12] J. Seebeck, J. Goldhahn, H. Städele, P. Messmer, M. M. Morlock and E. Schneider, “Effect of cortical thickness and cancellous bone density on the holding strength of internal fixator screws,” J. Orthop. Res., 22: 1237-1242, 2004.
[13] J. T. Hsu, C. H. Chang, H. L. Huang, M. E. Zobitz, W. P. Chen, K. A. Lai and K. N. An, “The number of screws, bone quality, and friction coefficient affect acetabular cup stability,” Med. Eng. Phys., 29: 1089-1095, 2007.
[14] L. Molly, “Bone density and primary stability in implant therapy,” Clin. Oral Implants Res., 17: 124-135, 2006. [15] A. Tabassum, G. J. Meijer, J. G. Wolke and J. A. Jansen.
“Influence of the surgical technique and surface roughness on the primary stability of an implant in artificial bone with a density equivalent to maxillary bone: a laboratory study,” Clin. Oral Implants Res., 20: 327-332, 2009.
[16] M. Akkocaoglu, S. Uysal, I. Tekdemir, K. Akca and M. C. Cehreli, “Implant design and intraosseous stability of immediately placed implants: a human cadaver study,” Clin. Oral Implants Res., 16: 202-209, 2005.
[17] I. Miyamoto, Y. Tsuboi, E. Wada, H. Suwa and T. Iizuka, “Influence of cortical bone thickness and implant length on implant stability at the time of surgery: clinical, prospective,
biomechanical, and imaging study,” Bone, 37: 776-780, 2005. [18] G. Alsaadi, M. Quirynen, K. Michiels, R. Jacobs and D. van
Steenberghe, “A biomechanical assessment of the relation between the oral implant stability at insertion and subjective bone quality assessment,” J. Clin. Periodontol., 34: 359-366, 2007.
[19] L. J. Fuh, H. L. Huang, C. S. Chen, K. L. Fu, Y. W. Shen, M. G. Tu, W. C. Shen and J. T. Hsu, “Variations in bone density at dental implant sites in different regions of the jawbone,” J. Oral Rehabil., doi: 10.1111/j.1365-2842.2010.02061.x, 2010. [Epub ahead of print]
[20] J. T. Hsu and D. J. Lin, “Effects of eccentric screwing on the initial stability of the acetabular cup in bone of different qualities,” Artif. Organs, 34: E10-E16, 2009.
[21] D. C. Markel, N. Hora and M. Grimm. “Press-fit stability of uncemented hemispheric acetabular components: a comparison of three porous coating systems,” Int. Orthop., 26: 72-75, 2002. [22] M. Baleani, R. Fognani and A. Toni. “Initial stability of a
cementless acetabular cup design: experimental investigation on the effect of adding fins to the rim of the cup,” Artif. Organs, 25: 664-669, 2001.
[23] E. Nkenke, M. Hahn, K. Weinzierl, M. Radespiel-Tröger, F. W. Neukam and K. Engelke, “Implant stability and histomorphometry: a correlation study in human cadavers using stepped cylinder implants,” Clin. Oral Implants Res., 14: 601-619, 2003.
[24] W. A. Peck, P. Burckhardt, C. Christiansen, H. A. Fleisch, H. K. Genant, C. Gennari, T. J. Martin, L. Martini, R. Morita and E. Ogata, “Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis,” Am. J. Med., 94: 646-650, 1993.
[25] T. T. Dao, J. D. Anderson and G. A. Zarb, “Is osteoporosis a risk factor for osseointegration of dental implants?” Int. J. Oral Maxillofac. Implants., 8: 137-144, 1993.
[26] I. N. Tsolaki, P. N. Madianos and J. A. Vrotsos, “Outcomes of dental implants in osteoprotic patients. A literature review,” J. Prosthodont., 18: 309-323, 2009.
[27] G. Alsaadi, M. Quirynen, A. Komárek and D. van Steenberghe, “Impact of local and systemic factors on the incidence of oral implant failures, up to abutment connection,” J. Clin. Periodontol., 34: 610-617, 2007.
[28] P. L. Moy, D. Medina, V. Shetty and T. L. Aghaloo, “Dental implant failure rates and associated risk factors,” Int. J. Oral Maxillofac. Implants., 20: 569-577, 2005.
[29] J. C. Baxter and L. Fattore, “Osteoporosis and osseointegration of implants,” J. Prosthodont., 2: 120-125, 1993.