ORIGINAL PAPER
Cost-effectiveness of Clinical Pathway in Coronary Artery
Bypass Surgery
Yung-Kai Lin&Chia-Pin Chen&Wen-Chen Tsai&
Yu-Ching Chiao&Blossom Yen-Ju Lin
Received: 24 April 2009 / Accepted: 27 July 2009
# Springer Science + Business Media, LLC 2009
Abstract Few studies have been devoted to the exploration of the effect of clinical pathways on coronary artery diseases treated with coronary artery bypass (CAB) surgery. This study was aimed to investigate the cost and effectiveness of the clinical pathway on CAB surgery in a medical center. With a retrospective dataset in 2003–2007, 212 CAB surgery patients were included. Data of the costs and postoperative complica-tion occurrence and length of stays were the focus and patient demographics, surgical risk indicator EuroSCORE, surgical conditions were collected. It revealed that there was differen-tiation across specified cost items in beating heart CAB surgery patients, but not for heart arrest CAB surgery patients with and without clinical pathways enrolled. In addition, there was no difference in postoperative complication occurrence in CAB surgery patients enrolled into clinical pathways. However, robotic beating heart CAB surgery patients enrolled clinical pathways were shown to have less postoperative ordinary ward stay than those not enrolled clinical pathways. CAB surgery patients’ age and surgical risks were related to their postoperative lengths of stay to some extent.
Keywords Clinical pathway . Cost-effectiveness . Coronary artery bypass surgery . Care costs . Care quality
Introduction
The standardization of clinical practice is viewed as a way for reducing the length of stay as well as hospital charges, while maintaining quality of medical care. Approaches have ranged from using general sets of principles called practice guide-lines using specific and detailed outguide-lines for care called clinical pathways [1–3]. In the medical field, clinical pathways have been applied worldwide to the clinical care in surgeries, medical care, and rehabilitation. In particular, cardiovascular treatment is an area in which clinical path-ways have been embraced, due to the high cost associated with cardiovascular diseases and procedures [4–6].
Various results of implementing clinical pathways in surgeries have been found in the evidence-based health care researches. For example, a retrospective study with 780 patients found that critical path group had a significant decrease in hospitals and surgical lengths of stay [7]. A retrospective cohort study from 1988 to 1998 in the department of surgery of an academic medical center in Maryland, USA, reveals that critical pathways may de-crease postoperative stay for some, but not all, surgeries [8]. Furthermore, it was found that critical pathway programs might have limited effectiveness, for example, pathway effectiveness in reducing the length of stay tended to be better for only lower patient severity of illness [8].
In the field of coronary artery bypass (CAB) surgery, limited case studies in the certain hospital facilities have been devoted to understand the effect of clinical pathways in CAB surgery [9]. Within a university hospital in Massachusetts, USA, it was pointed out the length of stay
Y.-K. Lin
Division of Cardiovascular Surgery, Taichung Veterans General Hospital, Taichung, Taiwan, Republic of China C.-P. Chen
:
Y.-C. ChiaoDepartment of Business Administration, National Chung Hsing University, Taichung, Taiwan, Republic of China W.-C. Tsai
:
B. Y.-J. Lin (*)Department of Health Services Administration, China Medical University,
Taichung, Taiwan, Republic of China e-mail: [email protected] DOI 10.1007/s10916-009-9357-7
decreased for CAB surgery after implementing the clinical pathways implemented; however, similar decreases were shown in their neighboring hospitals that did not have critical pathways or other specific efficiency initiatives [10]. Our study was aimed to investigate the cost and effective-ness analyses of the implementation of the clinical pathway on CAB surgery in a medical center in Taiwan. It was expected to stimulate medical professionals to establish best practice and advance the care of patients with coronary artery diseases under CAB surgery.
Methods
Implementation of the clinical pathway of CAB surgery in the medical center
Background
This study was conducted in one veteran general hospital nationally accredited as one of the 14 medical centers in Taiwan. It is located in the middle of Taiwan and owns around 1,400 hospital beds. The average outpatient volume is about 1,500,000 visits per year and the average inpatient volume is 45,000 discharges per year in the period of 2000 to 2006. And seven cardiac surgeons perform about 450– 550 cardiac surgeries per year in the Cardiovascular Department. The clinical pathway of CAB surgery has been demonstrated in the Cardiovascular Department since 1999 and reviewed/revised annually. At this time, the cost and effectiveness analyses were performed to evaluate the feasibility and usefulness of CAB clinical pathway for future implementation.
Design of the clinical pathway for CAB surgery
The clinical pathway for CAB surgery in the studied medical center was formulated by a designer team, which consisted of surgeons, nurse practitioners, pharmacists, rehabilitants, and respiratory physicians/practitioners. In common with those identified in the literature the clinical pathway was designed to have clear daily goals in the admission course [6,11–13]. These daily goals were listed on a checklist and they were prinked by clinical physicians and nurse practitioners every day. The comments and targeted outcomes of the clinical pathway of CAB surgery were routinely revised based on the data collection in the annual review meeting. Further-more, all the revised items were checked monthly to confirm the change being suitable for the patient’s safety and ethic issue. The CAB clinical pathway in the studied medical center is categorized into three parts, including preoperative preparation, postoperative pathway, and rehabilitation (see Appendix1for details).
Study subjects
Seven hundred and four patients administered by the CAB surgery in the studied medical center in the period from Jan 2003 to Dec 2007, with 574 patients (81.5%) as elective surgeries and 130 patients (18.5%) as emergent surgeries, were considered. Because the possible differ-ences in preoperative length of stay, angiography, and percutaneous coronary intervention might exist between elective and non-elective CAB surgery patients in the costs analyses [13], only the patients undergoing elective CAB surgery were selected in this study. Furthermore, those who died, were barely found the patient surgery episode course and records, and were suffered from severe complications (see Appendix 2) were excluded. Finally, 212 CAB surgery patients were included for the cost and effectiveness analyses of CAB surgery clinical pathways in this study.
Previous studies have shown that there might exist different outcomes between conventional CAB surgery (i.e., heart arrest) and off-pump CAB surgery (i.e., beating heart) [13–16]. Furthermore, the medical center has introduced robotic CAB surgery in these 5 years for beating heart CAB surgeries. Therefore, the included 212 CAB surgery patients could be divided into three major strat-ifications, that is, patients with heart arrest CAB surgeries, non-robotic beating heart CAB surgeries, and robotic beating heart CAB surgeries. The included patient sample treated entirely in the cardiovascular department was undergone the implementation of CAB surgery clinical pathways and those referred from other medical specialty departments were not enrolled in the CAB surgery clinical pathways (see Table 1).
Measurements
To understand the cost and effectiveness of clinical path-ways for the CAB surgery patients, costs and postoperative complication and length of stay (i.e., ICU stay and ordinary ward stay) were measured in this study. The cost measure-ments for CAB surgery patients included costs of visiting, ICU wards, ordinary wards, examinations, radiology, disposals, operation, anesthesia, specific medical materials for operations, blood transfusion, and medication. Patient demographics such as age [17–19], gender [20, 21] and patient surgical risk indicator, EuroSCORE [22–25], were collected. And the surgery relevant data such as the number of surgical graft bypass [19] done in operation were also traced. Patient demographics, surgical risk indicator (Euro-SCORE), and the number of surgical graft bypass were collected to adjust CAB surgery patients’ cost and effectiveness comparisons for exploring the effect of the implementation of clinical pathways.
Data collection
This is a retrospective study with secondary data for analysis. Medical records carried the demographic and medical information for CAB surgery patients and the hospital administrative dataset provided the cost infor-mation for the individual CAB surgery patients. The data acquisition was approved by the studied medical center.
Statistical techniques
The data were first analyzed descriptively with means and standard deviations calculated for continuous variables, and frequency and percentages for categorical variables. The univariate analyses including Wilcoxon W, ANOVA, and Fisher’s exact tests, multiple regression analyses, and logistic regressions were performed in this study, with SPSS 12.0 and EXCEL software.
Table 1 Personal and medical backgrounds of CAB surgery patients in the preoperative, operative and postoperative stages
Total (n=212) Heart arrestb(n=48) Beating heartb(n=164) CP enrolled (n=25) Non-CP enrolled (n=23) CP (non-robotic) enrolled (n=65) CP (robotic) enrolled (n=41) Non-CP enrolled (n=58)
<Patient group 1> <Patient group 2> <Patient group 3> <Patient group 4> <Patient group 5> Freq. (mean) % (SD) Freq. (mean) % (SD) Freq. (mean) % (SD) Freq. (mean) % (SD) Freq. (mean) % (SD) Freq. (mean) % (SD) Preoperative stage Age (64.35) (10.52) (64.80) (10.75) (64.52) (9.95) (64.18) (10.77) (64.76) (11.64) (63.98) (9.85) Gender Female 40 19 7 28 5 22 13 20 5 12 10 17 Male 172 81 18 72 18 78 52 80 36 88 48 83 EuroSCORE (3.72) (2.26) (4.20) (2.48) (3.78) (2.15) (3.85) (2.18) (3.46) (2.70) (3.53) (1.98) <6a 164 77 17 68 17 74 51 78 30 73 49 84 ≥6 48 23 8 32 6 26 14 22 11 27 9 16
Enrolled clinical pathway
No 81 38 Yes 131 62 Operative stage Operation procedure Heart arrest 48 23 25 100 23 100 0 0 0 0 0 0 Beating heart (non-robotic) 123 58 0 0 0 0 65 100 0 0 58 100
Beating heart (robotic) 41 19 0 0 0 0 0 0 41 100 0 0
Number of surgical graft bypass (3.08) (0.74) (3.04) (0.79) (3.26) (0.86) (3.02) (0.70) (3.00) (0.59) (3.17) (0.80) Postoperative stages Complicationc No 23 92 21 91 61 94 39 95 53 91 Yes 2 8 2 9 4 6 2 5 5 9 Length of postoperative stay (days) ICU (2.61) (1.16) (2.80) (1.15) (2.87) (1.14) (2.38) (1.32) (2.56) (1.07) (2.71) (1.03) Ordinary wardd (5.91) (2.48) (6.92) (2.31) (7.09) 4.16 (5.86) (1.52) (4.24) (1.59) (6.24) (2.54) CP clinical pathway a
EuroSCORE <6 means patient with low risk for CAB surgery
bThere is no testing difference for age, gender, EuroSCORE between CAB surgery patients enrolled in clinical pathway and not enrolled in
clinical pathway, within heart arrest group and beating heart group, respectively
cFisher’s Exact Test, p>0.05 for heart arrest and beating heart CAB surgery patients, respectively, with and without clinical pathways d
Results
Among the 212 studied CAB surgery cases studied, most cases were male (81%), and with lower EuroSCORE (<6, 77%). The average patient age was 64 years old. Forty-eight cases (22%) underwent heart arrest CAB surgery and 164 cases (78%) were administered with beating heart CAB surgery. Of the 48 patients with heart arrest CAB surgeries, 25 cases (50%) were enrolled with clinical pathways. Of the 164 patients with beating heart CAG surgeries, 106 cases (65%) were enrolled with clinical pathways.
There did not exist statistically significance in age, gender, and EuroSCORE of heart arrest CAB surgery patients and beating heart CAB surgery patients respectively, with and without enrolled clinical path-ways (p > 0.05). In terms of medical backgrounds of CAB surgery patients in the operative stage, the total 212 cases studied went through three graft bypass surgeries on average (see Table1: column“Total”). Of the heart arrest (i.e., patient group 1 and 2) and beating heart (i.e., patient group 3, 4, and 5) CAB surgery patients, respectively, no statistical significance in the number of graft bypass surgeries was observed. Detailed information on the personal and medical backgrounds of the CAB surgery patients is shown in Table1.
Cost analysis for heart arrest CAB surgery patients Details of costs in the full course of disease treatment were analyzed in patients who received heart arrest CAB surgery with and without enrolling into the clinical pathway (i.e., Patient Group 1 & 2) (Table 2). Overall, surgery-related costs, including surgery operation, anes-thesia, special medical materials (item 16) were the largest costs in the heart arrest CAB surgery patients, followed by ward costs, including ICU and ordinary wards (item 4), and medication-related costs (item 20). To compare the costs of the heart arrest CAB surgery patients enrolled into clinical pathways with those not-enrolled, Wilcoxon W testing showed that there was no statistical significance in the costs across all individual cost items (p > 0.05).
To understand the effect of clinical pathways imple-mented for heart arrest CAB surgery patients in costing structures, we adjusting the patient personal and medical characteristics into the cost modeling, including age, gender, EuroSCORE and number of surgical graft bypass. It was found that the heart arrest CAB surgery patients’ total costs were not relevant to the implementation of clinical pathways (p>0.05, Table3). However, lengths of the postoperative ICU stays and ordinary ward stays were positively related to CAB patients’ total costs (p<0.001, Table3).
Cost analysis for beating heart CAB surgery patients Details of costs in the full course of disease treatment were analyzed in patients received beating heart CAB surgery with and without enrolled into the clinical pathway (i.e., Patient Groups 3, 4, & 5) (Table4). Overall, surgery-related costs, including operation, anesthesia, and special medical materi-als (items 16) were the largest costs in the beating heart CAB surgery patients, followed by ward costs, including ICU and ordinary wards (item 4), and medication-related costs (item 20). To compare the costs of the beating heart CAB surgery patients, ANOVA analyses showed that beating heart CAB surgery patients without enrolled in clinical pathways (i.e., Patient Group 5) had higher radiology costs than non-robotic beating heart CAB surgery patients without enrolled clinical pathways (i.e., Patient Group 3) (p<0.05). The treatment costs, blood transfusion costs, and medication-related costs were higher than robotic beating heart CAB surgery patients with enrolled clinical pathways (i.e., Patient Group 4) (p< 0.05). However, beating heart CAB surgery patients without enrolled in the clinical pathways (i.e., Patient Group 5) had lower costs in examination and anesthesia than non-robotic beating heart CAG surgery patients with enrolled clinical pathways (i.e., Patient Group 3) and robotic beating heart CAG surgery patients with enrolled clinical pathways (i.e., Patient Group 4), respectively (p<0.05).
To understand the effect of clinical pathways imple-mented for beating heart CAB surgery patients in costing structures, we adjusting the patient personal and medical characteristics into the cost modeling, including age, gender, EuroSCORE and number of surgical graft bypass. It was found that the beating heart CAB surgery patients’ total costs were not relevant to the implementation of clinical pathways (p>0.05, Table 5). However, complica-tion occurrence and lengths of the post-operative ICU stays and ordinary ward stays, were positively related to beating heart CAB patients’ total costs (p<0.05, Table5).
Effectiveness analysis for CAB surgery patients
The effectiveness measures for CAB surgery patients in this study were complication occurrence and lengths of the post-operative ICU stay and ordinary ward stay as indicators. It was found that there was no significant difference between the subgroups of patients with heart arrest procedure and tri-groups of patients with beating heart procedure (p>0.05) on the postoperative complication indicator (Table 1). Furthermore, adjusting the patient personal and medical characteristics, including age, gender, EuroSCORE and number of surgical graft bypass, it was found that the CAB surgery patients’ complication occur-rence were not relevant to the implementation of clinical pathways (Tables 3and5).
Table 2 Costs comparisons for heart arrest CAB surgery patients with vs. without clinical pathways enrolled
Costs (US$) Total CP enrolled (n=25) Non-CP enrolled (n=23) <Patient group 1> <Patient group 2>
Mean SD Mean SD Mean SD
1. Visiting 156.50 50.65 154.53 39.24 158.65 61.57 2. ICU wards 260.79 114.86 248.89 97.00 273.20 132.04 3. Ordinary wards 687.01 245.46 669.31 192.57 706.25 295.84 4. Sub-costs: wards (2.+3.) 942.36 356.91 908.24 293.04 979.45 419.16 5. Infusion and diets 24.13 10.31 25.08 10.81 21.62 10.45 6. General examination 687.79 186.87 635.19 136.10 744.97 218.71 7. Radiology 61.41 53.50 65.51 56.32 56.96 51.14 8. Sub-costs: examination (6.+7.) 749.21 212.94 700.69 155.47 801.94 254.79 9. General treatment 541.21 146.66 536.93 143.07 545.85 153.56 10. Infusion technique 78.44 38.09 76.31 27.12 80.75 47.82 11. Sub-costs: treatment (9.+10.) 619.65 175.50 613.24 163.49 626.61 191.16 12. Rehabilitation 112.03 59.60 113.07 49.97 110.85 70.18 13. Surgery 2,895.26 435.19 2,850.50 299.25 2,943.92 549.69 14. Anesthesia 1,043.32 229.78 1,075.06 231.28 1,008.82 228.15 15. Special medical materials 2,208.93 713.59 2,279.17 740.47 2,132.57 691.38 16. Sub-costs: surgery-related (13.+14.+15.) 6,147.51 1,083.18 6,204.73 828.63 6,085.32 1,322.77 17. Blood transfusion 379.72 228.84 337.43 179.59 425.69 269.16 18. Medication 860.07 378.23 860.99 366.57 859.08 398.80 19. Medication dispensing and management 33.62 10.66 33.60 7.64 33.64 13.38 20. Sub-costs: medication-related (18.+19.) 893.69 385.72 894.59 371.68 892.72 408.82 21. Total costs 10,003.86 1,928.40 9,934.54 1,417.75 10,079.21 2,395.92 Wilcoxon W testing for comparison patient group 1 vs. patient group 2 across all cost items. No statistical significances were found. CP clinical pathway
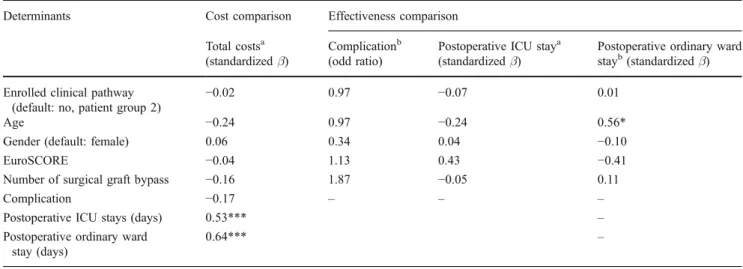
Table 3 Outcome comparisons for heart arrest CAB surgery patients with vs. without clinical pathways enrolled (adjusted models) Determinants Cost comparison Effectiveness comparison
Total costsa (standardizedβ)
Complicationb (odd ratio)
Postoperative ICU staya (standardizedβ)
Postoperative ordinary ward stayb(standardizedβ) Enrolled clinical pathway
(default: no, patient group 2)
−0.02 0.97 −0.07 0.01
Age −0.24 0.97 −0.24 0.56*
Gender (default: female) 0.06 0.34 0.04 −0.10
EuroSCORE −0.04 1.13 0.43 −0.41
Number of surgical graft bypass −0.16 1.87 −0.05 0.11
Complication −0.17 – – –
Postoperative ICU stays (days) 0.53*** – Postoperative ordinary ward
stay (days)
0.64*** –
*p<0.05; **p<0.01; ***p<0.001
a
Multiple regression analysis
b
In terms of lengths of the postoperative ICU stay and ordinary ward stay, we found that the implementation of clinical pathways was not relevant to lengths of postoper-ative stay (p>0.05, Table 3) in heart arrest CAB surgery patients. However, heart arrest CAB surgery patients’ ages played an important role in postoperative ordinary ward stay (p<0.05, Table3). On the other hand, robotic beating heart CAB surgery patients enrolled clinical pathways (Patient Group 4) were shown to have less postoperative ordinary ward stay than those not enrolled clinical
path-ways (Patient Group 5) (p<0.001, Table5). In addition, it was found that beating heart CAB surgery patients with higher surgical risks (measured as EuroSCORE) had higher postoperative ICU stays (p<0.05, Table5).
Discussion
With a retrospective study of 2003–2007, in this study, it was found that there was differentiation across specified
Table 4 Costs comparisons for beating heart CAB surgery patients with vs. without clinical pathways enrolled
Cost (US$) Total CP enrolled NO CP enrolled ANOVA
Non-robotic Robotic
<Patient group 3> <Patient group 4> <Patient Group 5>
Mean SD Mean SD Mean SD Mean SD
1. Visiting 134.25 39.40 137.33 40.05 120.22 31.66 140.72 41.71 Group (5)>(4)* 2. ICU wards 214.63 105.06 202.33 100.29 201.86 85.19 237.45 119.83
3. Ordinary wards 583.56 193.17 593.37 195.02 524.80 150.98 614.10 210.87 4. Sub-costs: wards (2.+3.) 798.19 285.91 795.70 282.51 726.66 229.86 851.55 317.00 5. Infusion and diets 27.88 18.16 28.90 19.65 30.57 21.09 20.91 6.76
6. General examination 573.89 105.17 607.99 19.91 549.17 134.14 553.17 127.90 Group (3)>(4)** Group (3)>(5)** 7. Radiology 71.75 59.72 43.80 1.35 106.05 68.81 78.82 71.33 Group (4)>(3)***
Group (5)>(3)*** 8. Sub-costs: examination (6.+7.) 645.64 123.82 651.79 18.55 655.22 173.54 631.99 148.39
9. General treatment 479.56 112.23 502.11 119.65 425.77 99.53 492.31 100.83 Group (3)>(4)** Group (5)>(4)* 10. Infusion technique 69.76 21.14 69.59 20.93 73.25 22.04 67.49 20.76
11. Sub-costs: treatment (9.+10.) 549.32 123.25 571.71 131.97 499.02 116.05 559.80 109.23 Group (3)>(4)* Group (5)>(4)* 12. Rehabilitation 86.84 46.90 90.61 50.25 72.52 40.68 92.75 45.78
13. Surgery 2,254.68 159.60 2,276.29 112.86 2,280.17 118.77 2,212.43 214.07
14. Anesthesia 930.53 186.83 881.95 137.50 1,136.90 150.72 839.08 144.26 Group (4)>(3)*** Group (4)>(5)*** 15. Special medical materials 1,799.08 787.20 1,709.77 806.65 1,648.60 791.44 2,005.53 730.19
16. Sub-costs: surgery-related (13.+14.+15.) 4,984.28 875.87 4,868.01 836.77 5,065.67 843.13 5,057.04 939.78
17. Blood transfusion 199.35 157.84 203.24 141.84 130.50 150.14 244.44 165.59 Group (5)>(4)** 18. Medication 695.35 235.73 788.48 243.10 558.08 168.40 688.02 221.71 Group (3)>(4)***
Group (3)>(5)* Group (5)>(4)* 19. Medication dispensing and management 29.82 8.14 31.60 8.14 25.76 6.14 30.68 8.52 Group (3)>(4)***
Group (5)>(4)** 20. Sub-costs: medication-related (18.+19.) 725.16 239.77 820.08 246.67 583.84 170.43 718.69 225.87 Group (3)>(4)***
Group (3)>(5)* Group (5)>(4)* 21. Total costs 8,142.13 1,335.02 8,149.62 1,318.94 7,859.61 1,199.97 8,333.44 1,427.67
CP clinical pathway
cost items in beating heart CAB surgery patients, but not for heart arrest CAB surgery patients with and without clinical pathways enrolled. In addition, there was no difference in postoperative complication occurrence in CAB surgery patients enrolled into clinical pathways. However, robotic beating heart CAB surgery patients enrolled clinical pathways (Patient Group 4) were shown to have less postoperative ordinary ward stay than those not enrolled clinical pathways (Patient Group 5). CAB surgery patients’ age and surgical risk (EuroSCORE) were related to their postoperative lengths of stay to some extent.
Because of different surgical procedures, which make different results in short term or long term outcomes, the data are separated into two major groups: those who received heart arrest CAB surgery and those who received beating heart CAB surgery to compare the effect of clinical pathway and non-clinical pathway. However, smaller case number in patients who received heart arrest CAB surgery might exist fewer heterogeneity in the data and in turns, might deter to identify the statistical relationships in cost and effectiveness with or without the implementation of clinical pathways. On the other hand, it was found that various cost portraits in beating heart CAB surgery patients with and without enrolled into clinical pathways. The one-by-one cost investigation could make the medical profes-sionals to understand the detailed resources utilized. The clinical pathway contains multidisciplinary plans that outline the sequence and timing of actions necessary to achieve expected patient outcomes with optimal efficiency. The impact of clinical pathways is greatly influenced by the pathway development and implementation process. It
suggests that the CAB surgery multidisciplinary team could re-examine the care processes to identify the causes of resource utilization and better surgical techniques. For example, robotic beating heart CAB surgery has been budding in recent 5 years and it was introduced in this studied medical center in the past 2 years. It might be the reason why it costs more for anesthesia; in other words, more surgical time is demanded. However, prolonged surgical time does not seem to affect the length of ordinary ward stay in the studied patients and the cost of robotic CAB surgery was still less than the traditional beating heart surgery. It’s reasonable to presume that robotic CAB surgery makes a greater difference in traditional beating heart surgery if robotic procedures are matured in the future.
Some studies pointed out that CAB surgery patients with shorter ICU stay begin ambulation sooner and in turn, reduced the risk of postoperative complication as well as cost [26], and verified that short-stay intensive care is a safe and cost-effective approach for low-risk CAB surgery patients [27]. In this study, there were no difference in the ICU length of stay between/among clinical pathway and non-clinical pathway groups; however, we found that length of ordinary ward stay exist larger variety, which were related to clinical pathway enrolled for beating heart CAB surgery patients and elder heart arrest CAB surgery patients. It might be the timing for the medical professio-nals in the studied medical center to explore the possible causes or mechanisms which driven the higher utilization of length of ordinary ward stay in the CAB postoperative stage. Furthermore, the lengths of ICU and hospital stay are closely relative to the time for tracheal extubation [28]. We
Table 5 Outcome comparisons for beating heart CAB surgery patients with vs. without clinical pathways enrolled (adjusted models) Determinants Cost comparison Effectiveness comparison
Total costsa
(standardizedβ)
Complicationb
(odd ratio)
Postoperative ICU staya
(standardizedβ)
Postoperative ordinary ward staya(standardizedβ)
Enrolled clinical pathway (default: no enrolled <patient group 5>) Clinical pathway enrolled
robotic <patient group 4>
0.00 0.50 −0.07 −0.43*** Clinical pathway enrolled
non-robotic <patient group 3>
0.01 0.37 −0.10 −0.10
Age −0.04 1.08 −0.01 0.14
Gender (default: female) 0.07 0.49 −0.03 0.04
EuroSCORE 0.06 1.35 0.25* 0.05
Number of surgical graft bypass 0.09 0.61 0.08 −0.09
Complication 0.47*** – – –
Postoperative ICU stays (days) 0.23** – – – Postoperative ordinary ward stay (days) 0.14* – – – *p<0.05; **p<0.01; ***p<0.001
aMultiple regression analysis b
could try to reduce the postoperative intubation time by effort and then shorten the hospital stay.
There are several limitations in this study. The first is that well documented data was available for only 5 years and it leads to smaller case number in patients who received traditional heart arrest CAB surgery, which may be the reason for the effective verification of the effect of clinical pathways. Furthermore, the exclusive criteria in this study were made by Bureau of National Health Insurance in Taiwan also led to smaller sample size to be enrolled into the clinical pathway and it might dissemble the reality of clinical pathway administration.
Second, EuroSCORE was used to evaluate cardiac surgery patients for risk factors. Another indicator for short-term outcomes such as in-hospital mortality and prolonged length of stay for CAB surgery patients [29] might be used for risk stratification in the future. Further-more, failures to account for the length of stay in the rehabilitation of health care facilities or at homes [30,31] might be one limitation in our retrospective study.
Another limitation was that the details of the clinical pathway are revised annually in the studied medical center. These might lead to the changed contents of clinical pathways and changing medical professional behaviors
annually. Or variance from the clinical pathway might be decreased significantly after continued implementation [32]. In addition to implementing the pathway itself, education process accompanying pathway adoption is also a key for the value of pathways and it argued that clinical pathways could improve patient quality of care even if they do not reduce the length of stay [32]. The trend in this study might provide substantial insights and more clinical outcome indicators such as morbidity, mortality rate, readmission rate [33], quality of life indicators such as patient comfort of post-operation, and medical professional management and team approach issues should be included to ensure quality improvement, rather than cost reduction [12,34,35] in the future. Furthermore, clinical benchmark-ing could be learned from the peers in other countries to improve clinical pathways with CAB surgery in the future.
Acknowledgement This study was supported by Taichung Veterans General Hospital for provisions of administrative and medical data.
Appendix 1 Design of clinical pathway for coronary artery bypass surgery in the studied medical center
Appendix 2 Criteria excluded from clinical pathways for CAB surgery patients proposed by Bureau of National Health Insurance
Infection diseases 1. Septicemia
2. Perioperative pneumonia 3. Meningitis
4. Tuberculous disorders
5. Viral hepatitis B with hepatic coma 6. Candidiasis
Renal diseases 1. Acute renal failure Lung diseases
1. Pulmonary embolism Neural diseases 1. Cerebral infarction
2. Diabetes with hyperosmolar coma Cardiovascular diseases
1. Acute and subacute bacterial endocarditis 2. Postoperative acute myocardial infarction 3. Aortic dissection
4. Preoperative cardiogenic shock
References
1. Battista, R. N., and Hodge, M. J., Clinical practice guidelines: between science and art. Can. Med. Assoc. J. 148:385–8, 1993. 2. Gilmore, A., Clinical practice guidelines: weapons for patients, or
shields for MDs. Can. Med. Assoc. J. 148:429–431, 1993. 3. Hayward, R. S. A., and Laupacis, A., Initiating, conducting and
maintaining guidelines development programs. Can. Med. Assoc. J. 148:507–512, 1993.
4. DeSomma, M., Divekar, A., Galloway, A. C., Colvin, S. B., Artman, M., and Auslender, M., Impact of a clinical pathway on the postoperative care of children undergoing surgical closure of atrial septal defects. Appl. Nurs. Res. 15 (4)243–248, 2002. 5. National Heart Attack Alert Program (NHAAP) coordinating
committee critical pathways writing group, Critical pathways for management of patients with acute coronary syndromes: an assessment by the National Heart Attack Alert Program. Am. Heart J. 143:777–789, 2002.
6. Ranjan, A., Tarigopula, L., Srivastava, R. K., Obasanjo, O. O., and Obah, E., Effectiveness of the clinical pathway in the management of congestive heart failure. South. Med. J. 96 (7) 661–663, 2003.
7. Pearson, S. D., Kleefield, S. F., Soukop, J. R., Cook, E. F., and Lee, T. H., Critical pathways intervention to reduce length of hospital stay. Am. J. Med. 110 (3)175–80, 2001.
8. Barnes, R. V., Lawton, L., and Briggs, D., Clinical benchmarking improves clinical paths: experience with coronary artery bypass grafting. Joint Comm. J. Qual. Improv. 20 (5)267–276, 1994. 9. Rumble, S. J., Jernigan, M. H., and Rudisill, P. T., Determining
the effectiveness of critical pathways for coronary artery bypass
graft patients: retrospective comparison of readmission rates. J. Nurs. Care Qual. 11 (2)34–40, 1996.
10. Dy, S. M., Garg, P., Nyberg, D., Dawson, P. B., Pronovost, P. J., Morlock, L., Rubin, H., and Wu, A. W., Critical pathway effectiveness: assessing the impact of patient, hospital care, and pathway characteristics using qualitative comparative analysis. Health Serv. Res. 40 (2)499–516, 2005.
11. Davis, J. T., Allen, H. D., Felver, K., Rummell, H. M., Powers, J. D., and Cohen, D. M., Clinical pathways can be based on acuity, not diagnosis. Ann. Thorac. Surg. 59:1074–1078, 1995. 12. Ibarra, V. L., Mueller, T., Rossi, N., Schillig, K., and Swearingen,
J., Interdisciplinary quality improvement from the perspective of a clinical pathway team. J. Nurs. Care Qual. 12 (3)19–29, 1998. 13. Williams, M. L., Muhlbaier, L. H., Schroder, J. N., Hata, J. A.,
Peterson, E. D., Smith, P. K., Landolfo, K. P., Messier, R. H., Davis, R. D., and Milano, C. A., Risk-adjusted short- and long-term outcomes for on-pump versus off-pump coronary artery bypass surgery. Circulation (Cardiovascular Surgery Supple-ment). 112 (9 Supplement)1366–1370, 2005.
14. Bolton, J. E. R., and Connally, J. E., Results of a phase one study on robotically assisted myocardial revascularization on the beating heart. Ann. Thorac. Surg. 78:154–158, 2004.
15. Kirk, K. C., Aldridge, R. A., Sistino, J. J., Zellner, J. L., Crumbley, A. J., Kratz, J. M., Crawford, F. A. Jr., and Reeves, S. T., Coronary artery bypass grafting with and without cardiopulmonary bypass: a comparison analysis. J. Extra-Corpor. Technol. 33 (2)86–90, 2001.
16. Sedrakyan, A., Wu, A. W., Parashar, A., Bass, E. B., and Treasure, T., Off-pump surgery is associated with reduced occurrence of stroke and other morbidity as compared with traditional coronary artery bypass grafting: a meta-analysis of systematically reviewed trials. Stroke. 37 (11)2759–2769, 2006.
17. Järvinen, O., Huhtala, H., Laurikka, J., and Tarkka, M. R., Higher age predicts adverse outcome and readmission after coronary artery bypass grafting. World J. Surg. 27 (12)1317–1322, 2003. 18. Paone, G., Higgins, R. S., Havstad, S. L., and Silverman, N. A.,
Does age limit the effectiveness of clinical pathways after coronary artery bypass graft surgery. Circulation. 98 (19 Suppl) II41–II45, 1998.
19. Roscitano, A., Benedetto, U., Capuano, F., Simon, C., Tonelli, E., Ruvolo, G., and Sinatra, R., Off-pump versus on-pump coronary artery bypass: does number of grafts performed represent a selection bias in comparative studies? Results from a matched cohort comparison. Ital. Heart J. 6 (9)740–744, 2005.
20. Becker, E. R., and Rahimi, A., Disparities in race/ethnicity and gender in in-hospital mortality rates for coronary artery bypass surgery patients. J. Natl. Med. Assoc. 98 (11)1729–1739, 2006. 21. Steuer, J., Blomqvist, P., Granath, F., Rydh, B., Ekbom, A., de
Faire, U., and Ståhle, E., Hospital readmission after coronary artery bypass grafting: are women doing worse? Ann. Thorac. Surg. 73 (5)1380–1386, 2002.
22. D’Errigo, P., Seccareccia, F., Rosato, S., Manno, V., Badoni, G., Fusco, D., and Perucci, C. A., Comparison between an empirically derived model and the EuroSCORE system in the evaluation of hospital performance: the example of the Italian CABG Outcome Project. Eur. J. Cardio-Thorac. Surg. 33:325–333, 2008. 23. Gogbashian, A., Sedrakyan, A., and Treasure, T., EuroSCORE: a
systematic review of international performance. Eur. J. Cardio-Thorac. Surg. 25:695–700, 2004.
24. Toumpoulis, I. K., Anagnostopoulos, C. E., DeRose, J. J., and Swistel, D. G., Does EuroSCORE predict length of stay and specific postoperative complications after cardiac surgery. Eur. J. Cardio-Thorac. Surg. 27:128–133, 2005.
25. Youn, Y. N., Kwak, Y. L., and Yoo, K. J., Can the EuroSCORE predict the early and mid-term mortality after off-pump coronary artery bypass grafting. Ann. Thorac. Surg. 83 (6)2111–2117, 2007.
26. Anderson, B., Higgins, L., and Rozmus, C., Critical pathways: application to selected patient outcomes following coronary artery bypass graft. Appl. Nurs. Res. 12 (4)168–174, 1999.
27. van Mastrigt, G. A., Heijmans, J., Severens, J. L., Fransen, E. J., Roekaerts, P., Voss, G., and Maessen, J. G., Short-stay intensive care after coronary artery bypass surgery: randomized clinical trial on safety and cost-effectiveness. Crit. Care Med. 34 (1)65–75, 2006.
28. Scott, B. H., Seifert, F. C., Grimson, R., and Glass, P. S., Resource utilization in on- and off-pump coronary artery surgery: factors influencing postoperative length of stay—an experience of 1,746 consecutive patients undergoing fast-track cardiac anesthesia. J. Cardiothorac. Vasc. Anesth. 19 (1)26–31, 2005.
29. Curtis, L. H., Phelps, C. E., McDermott, M. P., and Rubin, H. R., The value of patient-reported health status in predicting short-term outcomes after coronary artery bypass graft surgery. Med. Care. 40 (11)1090–1100, 2002.
30. Cowper, P. A., DeLong, E. R., Hannan, E. L., Muhlbaier, L. H., Lytle, B. L., Jones, R. H., Holman, W. L., Pokorny, J. J., Stafford,
J. A., Mark, D. B., and Peterson, E. D., Trends in postoperative length of stay after bypass surgery. Am. Heart J. 152 (6)1194– 1200, 2006.
31. Kim, S., Losina, E., Solomon, D. H., Wright, J., and Katz, J. N., Effectiveness of clinical pathways for total knee and total hip arthroplasty: literature review. J. Arthroplast. 18 (1)69–74, 2003. 32. Chang, P. L., Wang, T. M., Huang, S. T., Hsieh, M. L., Chuang, Y. C., and Chang, C. H., Improvement of health outcomes after continued implementation of a clinical pathway for radical nephrectomy. World J. Urol. 18 (6)417–421, 2000.
33. Hannan, E. L., Racz, M. J., Walford, G., Ryan, T. J., Isom, O. W., Bennett, E., and Jones, R. H., Predictors of readmission for complications of coronary artery bypass graft surgery. JAMA. 290 (6)773–780, 2000.
34. Broder, M. S., and Bovone, S., Improving treatment outcomes with a clinical pathway for hysterectomy and myomectomy. J. Reprod. Med. 47 (12)999–1003, 2000.
35. CABG path yields savings, but proves ‘user unfriendly’. Hosp. Case Manag. 5(7):129–123, 1997.