Would it matter to expose elderly patients who took digoxin to Chinese Medications?
Hsiang-Wen Lin*1,2, Hsin-Hui Tsai1,2, I-Wen Yu2, Arun Kumar1, Man-Pin Wu1 1. School of Pharmacy and Graduate Institute, China Medical University
2.Department of Pharmacy, China Medical University Hospital BACKGOUND: Elderly patients seem vulnerable to digoxin toxicity due to their diminished organ functions and tendency to encounter drug interactions. The aim of this research was to explore the extent of the concurrent use of digoxin with Chinese medications (CMs), its contributing factors and the relevant consequences.
METHODS: A retrospective population-based cohort study was conducted using Longitudinal Health Insurance databases in Taiwan. Those elderly patients being prescribed with digoxin in outpatient settings in 2006 were evaluated for the
incidence, prevalence, and duration of concurrent use with concentrated CMs in 2006. After 1:1 random matching to select the corresponding digoxin-only elderly users, univariate and multivariate logistic regression analyses were performed to explore factors associated with concomitant incident CM use and incident digoxin-specific CM use. The relevant clinical and economic outcomes for a three-month follow-up period from the initial exposure of incident digoxin-CM use were compared.
RESULTS: Of 185,076 elderly, 6,374 were prescribed with digoxin and 789 were CM-digoxin users in 2006. The prevalence and incidence of concomitant CM use among digoxin elderly users were 0.43% and 0.22%, respectively. While the other factors were not statistically significantly associated with incident CM-digoxin use, patients with heart diseases and with benign prostate hypertrophy (BPH) had an increased likelihood of incident CM-digoxin use of 115% and 102%, respectively.
Almost all of the concerned clinical and economic outcomes were not statistically significantly different between incident exposure or not, except for the use potassium-sparing and non-steroidal anti-inflammatory drugs.
CONCLUSION: There was relatively low incidence of digoxin-CM use among the elderly in Taiwan. Although no significant impacts on clinical and economic
outcomes occurred, it is necessary to monitor digoxin concentrations more
aggressively for those vulnerable elderly using digoxin with CMs, especially for those who tended to expose to incident digoxin-CM use elderly patients.
Introduction
Elderly people, especially those with chronic conditions, are more prone to experiencing drug interactions and adverse drug reactions as they often take many medications together and have diminished body functions, along with multiple chronic illnesses [1-3]. A systematic review reported that there were 1 to 61% of patients, including the elderly, with cardiovascular diseases who utilised
complementary and alternative medicine (CAM), whereas 2 to 46% of them used herbal medicine [4]. In particular, 53% to 60% of CAM users, in which older adults accounted for the majority, tended not to disclose their use to primary health care providers [5, 6]. Less than half of nurses, physicians and pharmacists documented the patients’ use of natural health products in their medical records [7]. Therefore, the World Health Organisation (WHO) has recommended the supervision of western medicine practices together with traditional, complementary and alternative medicines [8]. For those frail elderly, the use of herbal medicine with regular use of Western medications, especially those with narrow therapeutic indexes, might pose potential safety concerns to individuals that could be mitigated by health professionals to some extent.
Digoxin, one of the positive inotropic agents, is used for many conditions, including heart failure (HF) and atrial fibrillation (AF), both of which are very common chronic diseases among elderly patients [9]. Digoxin has a narrow
therapeutic index and tends to have drug interactions with other Western and Chinese medications due to pharmacokinetic mechanisms (e.g., altered renal P-glycoprotein-mediated transport), pharmacodynamic mechanisms (e.g., result in hypopotassemia) and its life threatening toxicities [10]. While more than 0.125 mg of digoxin per day is considered potentially inappropriate for older adults [11], it might be necessary to
concerns the consequences of taking digoxin with other medications concurrently, including Western medications (i.e., clarithromycin, diuretics, sennoside) [12-14], and some herbal medicines (e.g., Chan Su, Lu-Shen-Wan, Dan Shen, Asian ginseng, Siberian Ginseng, and Shan Zha) [15-22].
However, herbal medications such as digitalis have been used to treat ailments since ancient times [23]. People believe that herbal medications do not cause any problems and are safe to use, even if the active ingredients of many herbs may interact with synthetic medications and result in the occurrence of adverse drug reactions [24-28]. For instance, elderly patients with heart failure seem liable to use herbal
medicines in order to receive their benefits [29]. While the concurrent use of herbal medications may show synergistic, agonistic or antagonistic effects on Western medications, those aforementioned studies showed the existence of significant interactions between digoxin and Chinese medications on pharmacokinetic and pharmacodynamic aspects [22]. To date, information on the actual exposure of digoxin with Chinese medications among older adults and its contributing factors is limited, as is information about its good or bad effects on patients.
For the past decade, the use of CAM, including Traditional Chinese Medicine (TCM), has been rising globally [30, 31], as well as in Taiwan [32]. An Australian study in 2007 showed that Chinese medicine usage accounted for 20% of all CAM use among older Australian women [33]. There were 10%, 28%, and 63% of NHI beneficiaries that had reported utilising TCM services in Taiwan in periods of one-month, one-year, and six-years, respectively [34]. In particular, concentrated Chinese medications (CMs), which are the extracts of single CMs, and combined CM remedy products are the most commonly used TCM therapies in Taiwan and the utilisation of concentrated CM has increased [35]. Almost all concentrated CMs have been covered
by Taiwan’s National Health Insurance (NHI) since the NHI program’s inception in 1995. The quality of concentrated CMs is important, and its manufacturers should comply with the current good manufacture practice in Taiwan [36]. Concerning the appropriate medication use and its corresponding clinical impacts among vulnerable older adults, especially for those who took Western medications with a narrow therapeutic index, the aim of this study was to explore the extent of concurrent use of digoxin with CMs, its contributing factors and the relevant consequences for the elderly.
Methods
Study design
This population-based retrospective cohort study was conducted to 1) examine the prevalence and incidence of concurrent use and interactions of digoxin with
concentrated CMs among elderly NHI beneficiaries, and describe their use patterns; 2) explore the contributing factors associated with incident digoxin-CM use and incident digoxin-specific CM interactions; and 3) examine the relevant impacts of incident digoxin-specific CM interactions.
Data sources
This study utilised the two-million sampling claimed data, National Health Research Insurance Database (NHIRD), which represents the entire insured Taiwanese
population (i.e., 23 million individuals). More specifically, we used the Longitudinal Health Insurance Database 2000 and 2005 (LHID 2000 and LHID 2005) for the analyses. This is one of the formal population databases containing information about prescription data of Western mediations and concentrated CMs under the national insurance program. This study was exempt from the Institutional Review Board
because the NHIRD database contains de-identified person data and de-identified health care settings. The NHIRD is publicly available only through the proper application process for researchers.
Study population
We focused on elderly digoxin users, because elderly patients are more likely to be given medication inappropriately, encounter adverse drug reactions (i.e., electrolyte imbalance, gastrointestinal upset) and/or experience drug interactions due to the use of digoxin and other medications together [3, 11]. The prevalence and incidence of the concurrent use of digoxin with CMs in 2005 for all ages of the NHI population in Taiwan were 10.7% and 5.4%, respectively [37]; we further identified those elderly NHI beneficiaries who survived and were prescribed digoxin in 2006. By analysing outpatient records, those elderly who were prescribed CMs with digoxin for at least one day were identified as digoxin-CM elderly users, while the incident digoxin-CM elderly users were those digoxin-CM elderly individuals who had no prescription records about previous CM use for the 6-month period prior to the date of first CM prescription use in 2006.
According to a previous study [22], which performed a systematic review, digoxin has severe evidence-based interactions with the following specific CMs: Da Huang, Hawthorn, Dan Shen, Licorice, Oyster shell, Siberian Ginseng, Senna, and Aloe Vera. Therefore, we further evaluated the occurrence and consequences of their interactions with digoxin. The incidence of digoxin-specific CM interactions among the incident digoxin-CM elderly users was estimated. Further, we randomly selected only one counterpart of digoxin-only users for each incident digoxin-CM elderly user and incident digoxin-specific CM elderly user based on the corresponding propensity scores derived from the combination of the following variables in order to reduce the
selection bias: the month of the index date, the same duration of digoxin use, age, with or without catastrophic illness certification, outpatient clinic visits per year, number of prescribed distinct medications and total medical expenditure. Thus, the index date of the selected digoxin-only elderly user was the same as the
corresponding incident digoxin-CM elderly user.
Potential factors associated with incident digoxin-CM use and occurrence of interactions among the elderly
Those listed factors relevant to incident concurrent use of high-risk western medications and CMs or CAM in previous studies [5, 35, 37, 38] were considered potential factors that were associated with incident digoxin-CM use and incident digoxin-specific CM interactions. In particular, those patients’ information about their co-morbidities (based on the ICD9 CM codes), health service utilisation (i.e.,
outpatient clinic visits, number of prescribed distinct medications, ever
hospitalization, total medical expenditure) were ascertained during the six-month period prior to the dates of first CM prescription, in terms of index dates. The number of prescribed distinct medications infers all items of distinct medications prescribed by either Western medicine physicians and/or Chinese medicine physicians during the six-month period prior to the index dates reported in the NHIRD records.
Impacts associated with incident occurrence of digoxin-specific CM interactions among the elderly
After a three-month follow-up period from the initial exposure of digoxin-specific CM use and that of corresponding digoxin-only use, the elderly patients’ relevant outcomes were further evaluated for their health service utilisation (i.e., all-causes of hospitalisations, three-month medical expenditure after the index dates), clinical outcomes (i.e., digoxin intoxication related clinical outcomes [digoxin intoxication
[ICD9-CM code=971.2], occurrence of arrhythmia [ventricular arrhythmia, atrioventricular block, bradycardia],electrolyte imbalance [hyperpotassemia,
hypopotassemia, acid-based disorders], acute renal failure, checking digoxin levels], factors associated with digoxin toxicity [chronic renal failure, hypomaganesium, hypercalcemia, hypothyroidism]), and other concomitant medications associated with digoxin toxicity (i.e., all types of diuretics, potassium supplements, angiotensin-converting enzyme inhibitors, p-glycoprotein inhibitors, non-steroidal
anti-inflammatory drugs, medication that might cause transcellular potassium shift)[10, 13].
Statistical Analyses
The corresponding findings were presented as meanstandarddeviation, or frequency (relative frequency, %). The differencesbetween groups of patients on continuous variables were analysed using independent t tests and the differences on nominal-scale variables were analysed using Pearson's 2 test. To explore the factors associated with the new concurrent use of digoxin and CMs and the incident
occurrence of digoxin-specific CM interactions among the elderly, patient
characteristics and health service utilisation were compared between the two groups. Univariate and multivariate logistic regression analyses were performed to estimate the crude odds ratios (ORs), adjusted ORs, and 95% confidence interval (CIs) in order to quantify the risk of incident digoxin-CM use and incident digoxin-specific CM interactions. All of the potential factors listed were included in the model for multivariate analyses and all analyses were performed using SAS version 9.2 (SAS Institute Inc., Cary, North Carolina).
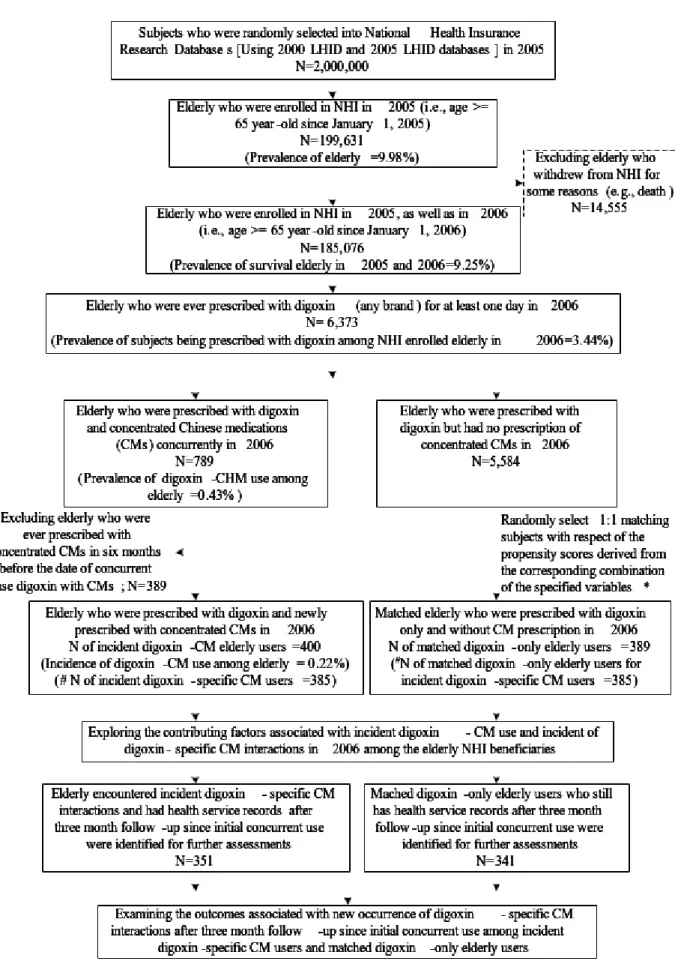
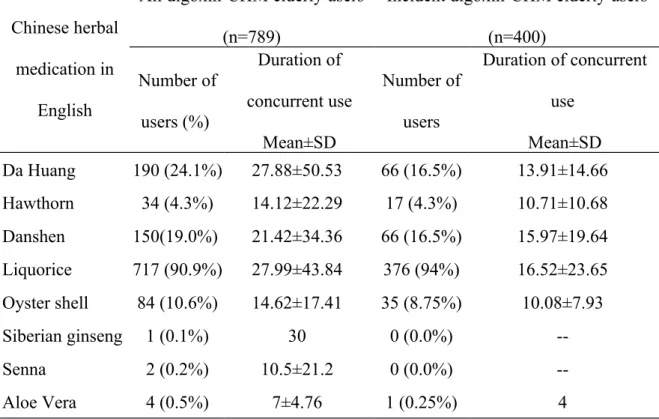
Of the two-million randomly selected National Health Insurance beneficiaries, 9.25% were considered elderly in 2005 and survived to 2006. There were 6,373 elderly individuals prescribed with digoxin (prevalence of digoxin prescription in elderly = 3.4%) (Figure 1) and the average duration of digoxin prescription was 190.41137.02 days (maximum = 365 days) in 2006. In total, 789 patients were prescribed with concentrated CMs for at least one day (prevalence of digoxin-CM use among the elderly = 0.43%). The incidence of digoxin-CM use among the elderly was 0.22% (N=400). The average duration of concurrent use was 17.2523.89 days (Maximum = 228 days) in 2006. Of the 400 incident digoxin-CM elderly users, 385 (96.5%) had ever encountered evidence-approved digoxin-specific CM interactions. The most common occurrence of specific CM interaction was digoxin-licorice (94% of all incident digoxin-CM elderly users and 98% of all incident digoxin-specific CM elderly users) and the average duration of concurrent use was 16.5223.65 days in 2006 (Table 1).
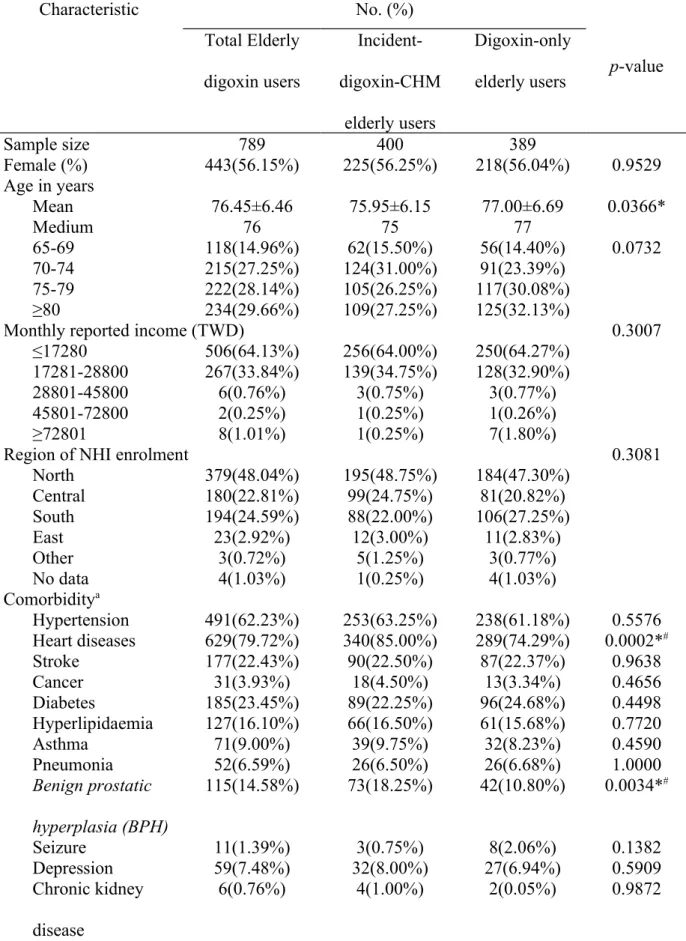
Although the 1:1 matching approach using specified propensity score was performed, there were some different characteristics between incident digoxin-CM elderly users and digoxin-only elderly users, in terms of mean age, presence of heart diseases or BPH, number of outpatient clinic visits per month, and number of
prescribed distinct medications (Table 2). This implies that incident digoxin-CM elderly users had a higher prevalence of heart diseases and BPH than digoxin-only elderly users. The other potential factors were the same between these two groups of elderly patients, in terms of not reaching statistical significance.
The univariate and multivariate logistic regression analyses also indicated that the crude ORs and adjusted ORs for those patients with the diagnoses of heart diseases and BPH were statistically significantly different between incident digoxin-CM
elderly users and digoxin-only users, as well as significantly different between those digoxin elderly users who encountered interactions with specific CMs and their counterpart digoxin-only users (Table 3). While the other factors were not statistically significantly associated with incident CM-digoxin use, patients with heart diseases and BPH had an increased likelihood of incident CM-digoxin use of 115% and 102%, respectively. Definitely, those elderly who made 2 to 5 outpatient visits per month and who had ever been prescribed more distinct medications tended to newly use digoxin with CMs. Those elderly NHI beneficiaries enrolled in the South Region were approximately 38% less likely to encounter incident digoxin-CM concurrent use.
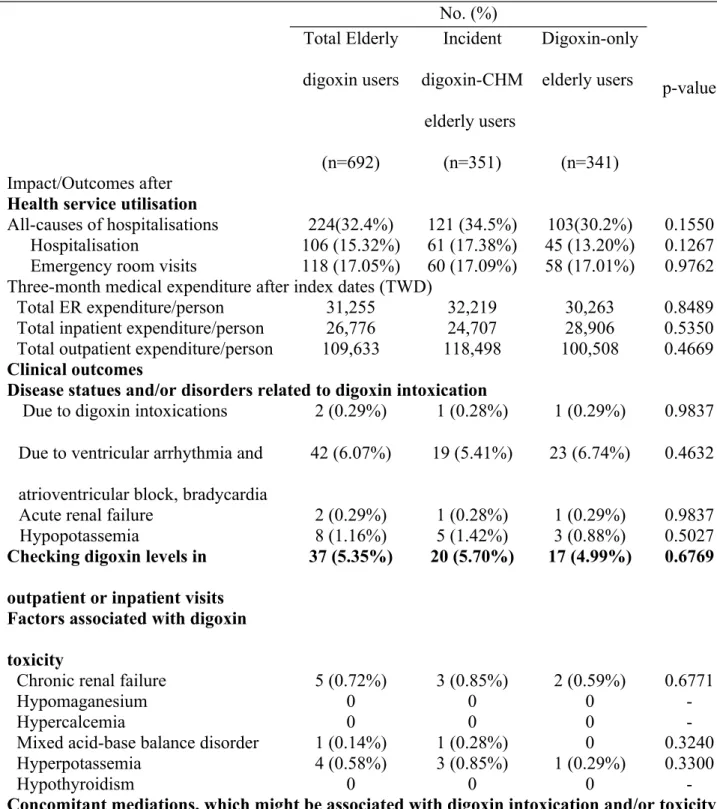
Of those elderly who we evaluated for their outcomes (N=692), after three months follow-up from the index dates of digoxin-specific CM use and the counterpart digoxin-only use, there was a higher occurrence of all-cause
hospitalisations, more diagnoses with hypopotassemia, more checks of digoxin levels, more concurrent prescriptions of potassium-sparing and non-steroidal
anti-inflammatory drugs (NSAIDs), and higher mean total medical expenditure on emergency room visits and outpatient visits among the incident digoxin-specific CM elderly users. However, almost all of these outcomes were not statistically
significantly different, except for the use of potassium-sparing medications and NSAIDs (p=0.016 and <0.001, respectively) (Table 4).
DISCUSSION
In this study, we found that only 3% of elderly NHI beneficiaries were prescribed with digoxin in 2006. Also, they were less likely to be prescribed with concentrated CMs with digoxin (0.43%) and only half of them were newly prescribed with concentrated CM (0.22%) in 2006. While digoxin was prescribed for 190 days on
average toward those NHI elderly beneficiaries in 2006, the concentrated CMs were somewhat less commonly prescribed concomitantly (i.e., average duration was approximately 17 days). The following factors were statistically significantly associated with the incremental incidence of concurrent digoxin-CM use and the incremental occurrence of digoxin-specific CM interactions: previous diagnosis of heart diseases or BPH, outpatient clinic visits per month ranging from 2 to 5 times, or more distinct medications prescribed in 2006. In contrast, those elderly NHI
beneficiaries enrolled in the South Region were less likely to encounter incident digoxin-CM concurrent use and incident digoxin-specific CM interactions. More than 96% of all incident digoxin-CM elderly users had encountered the evidence-approved digoxin-specific CM interactions; their 3-month follow-up medical outcomes after the initial occurrence were evaluated, but no statistically significant findings were found.
In this study, we found that elderly patients were relatively less likely to be prescribed with this narrow therapeutic index medication, digoxin, in Taiwan, while 17% of older adults were initially prescribed with digoxin in the United States [39], 38% of all age heart failure NHI beneficiaries were prescribed with digoxin and 26% were newly prescribed in Taiwan [14]. Although 7 to 21% of patients with
cardiovascular symptoms took herbal medicine in the US and other countries [40, 41], there was a relatively low prevalence and incidence of digoxin-CM use among the elderly in this study (0.43% and 0.22%, respectively). Such rates were comparatively lower than the findings obtained from a national wide survey in Taiwan in 2001 (i.e., 4.3% of all survey participants utilised both NHI covered Western medication and TCM)[42] and that of our previous population-based cohort study using one-million NHIRD data for all ages of digoxin users (10.7%, 5.4%, respectively) in 2005 [37]. In addition, the duration of concurrent use in this study was approximately 2 day less
than that obtained from all age incident digoxin-CM users (19.329.9 days) in 2005 [37]. One study showed that 28% of all NHI beneficiaries had utilised NHI covered TCM services in 2001, 62.5% had used covered TCM services at least once from 1996 to 2001 and 86% had ever been prescribed with concentrated CMs in Taiwan [43]. In this sense, our study showed that those Western medicine physicians who prescribed digoxin for the elderly in Taiwan were more conservative than those in other countries, than for all heart failure patients, and for all age digoxin users in Taiwan. Also, those Chinese medicine physicians more stringently prescribed CMs for elderly patients with digoxin due for some reasons. Nevertheless, it is unknown whether this phenomenon occurred due to concern over potential digoxin toxicities upon the announcement of Beer’s criteria in 2003 [44] or due to other reasons.
Furthermore, we found that those elderly with heart diseases and BPH were 2.15 and 2.02 times, respectively, likely to be newly prescribed with concentrated CMs when they had a prescription of digoxin at the same time, compared with those who did not have these diseases; this was also true when controlled for other factors. In contrast, there were no statistically significant differences in the extent of ORs among those who had chronic kidney diseases, myocardium infarction, ventricular
arrhythmias and heart failure during the six-month period prior to the index date. Using propensity scores to reduce the likelihood of selection bias in this study, it implies that those elderly on digoxin and with heart diseases and BPH were more likely to be newly prescribed with concentrated CMs, whereas such occurrence existed beyond that which is possible due to chance. In fact, our findings were different from a previous study focusing on all age adults who were ever prescribed with seven high-risk Western mediations (aspirin, clopidogrel, dipyridamole, ticlopidine, heparin, warfarin, and digoxin) in Taiwan [37]. A systematic review
showed that Chinese herbal medicine is more impressive with regard to the
improvement in quality of life, reduction of prostate volume and the occurrence of adverse events compared to Western medications, although the evidence is not robust to support the efficacy of Chinese herbal medicine for BPH [45]. While the number of patients with prostate cancers utilising covered CMs increased from 1996 to 2008 (i.e., 72.8% to 78.8% of all TCM therapies) in Taiwan [46], it is understandable that the usage of CMs with digoxin among those elderly with BPH in Taiwan might increase for the aforementioned reasons. We only focused on one year of NHI utilisation in Taiwan (2006); therefore, further exploration about utilisation of CMs with Western medications for prostate-related diseases across time might be
necessary.
In Taiwan, the implementation of National Health Insurance (NHI) as a single-payer, social insurance plan has provided almost all citizens with modest cost sharing. At present, the coverage of the population is as high as 97%, so the Bureau of NHI (BNHI) has provided the NHIRD for corresponding researches on issues related to cost, quality of health services, medical practice patterns, accessibility to health care programs, and treatment outcomes at the national or local level. The BNHI has had contracts with 97% of registered hospitals, which provide Western and/or Chinese medicine services, since 1996 to ensure sufficient accesses in Taiwan. Approximately 92% of all hospitals which provided Chinese medicine services were contracted by the BNHI to offer TCM medical care. In our study, we found that those elderly NHI beneficiaries enrolled in the South Region were less likely to encounter incident digoxin-CM concurrent use and incident digoxin-specific CM interactions, while there was no difference among the other regions. Such finding is inconsistent with our previous study, as well as with the results of other studies [35, 37, 42, 47, 48]. In
contrast, all of the other studies showed that NHI beneficiaries enrolled in the Central Region were more likely to be prescribed concentrated CMs with Western
medications, including digoxin, while no differences were identified among the other regions in this study.
It is reasonable to hypothesise that those elderly NHI beneficiaries who ever visited Western and Chinese medicine clinics in the same period of time would require a greater number of outpatient visits and would be prescribed with more distinct medications, including Western and Chinese medications. Consequently, these two factors were statistically associated with the incremental incidence of digoxin-CM concurrent use and digoxin-specific CM interactions. However, those who had made 2 to 5 outpatient clinic visits per month were more likely to encounter new digoxin-CM concurrent use and digoxin-specific CM interactions; this was different from our previous study focusing on all age NHI adult beneficiaries for high risk western medications (including anticoagulants and digoxin) in 2005 [37].
Importantly, this study retrieved the three-month follow-up information about relevant clinical and economic consequences after the new occurrence of digoxin-specific CM interactions among the NHI elderly beneficiaries, which accounted for almost all incident digoxin-CM elderly users. While those who encountered digoxin intoxications might also experience ventricular arrhythmia, atrioventricular block, bradycardia, acute renal failure, or hypopotassemia, and may require follow-up digoxin level evaluations, we were also concerned about the other relevant outcomes, including medical care expenditure, abnormal electrolyte disorders, and concomitant prescribed medications, which might be associated with digoxin toxicities, other than the all-cause hospitalisations. Finally, we did not find any statistically significant
difference in these potentially relevant outcomes, the factors associated with digoxin toxicity, or the concomitant medications.
However, the incident digoxin-specific CM elderly users were prescribed with more potassium-sparing diuretics and NSAIDs than their counterpart digoxin-only elderly users. It is unclear whether the potassium-sparing diuretics were prescribed to manage the problem of hypopotassemia, to prevent the occurrence of digoxin
toxicities or for other reasons. While 0.39% of new digoxin users were diagnosed with digoxin intoxication (ICD9 code=972.1) among all 590,955 heart failure patients from 2001 to 2004 in Taiwan in Wang’s study [14], only one elderly individual in each group was documented to have encountered digoxin intoxication in the three months after the index dates of the incident occurrence of digoxin-specific CM interactions in this study. In other words, the incidence of documented digoxin
intoxication was relatively low (i.e., 0.03%) among all elderly prescribed with digoxin in 2006 in this study. While the nested case-control studies using open cohorts were performed to explore the risks of exposing interactions between digoxin and diuretics, clarithromycin and sennoside, respectively in other studies [13, 14, 49, 50], further studies using different study designs (e.g., nested case-control study, case cross-over study) to involve more subjects and compare subjects by themselves might be necessary to confirm our findings.
A previous study demonstrated that higher serum digoxin concentrations were statistically associated with incremental mortality for those patients with heart failure [51]. The use of digoxin was associated with a significant increase in all-cause
mortality in patients with AF [52]. Although HF and AF are common diseases among the elderly, digoxin utilisation is indeed decreased in Taiwan compared to heart failure-related findings obtained from Wang’s study between 2001 and 2004 [14]. It is
presumed that one reason for this might be due to the inferior effectiveness of treatment compared to beta-adrenergic inhibitors, angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers for HF [10]. Nevertheless, several studies have recommended not overlooking digoxin toxicities, especially for those with older age, female patients, with low lean body weight, with renal insufficiency and their concomitant medication use [10, 13, 37, 51, 52]. All of these studies suggest that checking digoxin concentration is necessary to evaluate the risk and benefit for those digoxin users for any condition. However, only approximately 5% of all elderly individuals with digoxin prescriptions were ordered to check their digoxin levels in the three months following the date of incident digoxin-specific CM interactions and the corresponding digoxin-only use in this study. Further studies might be necessary to examine the rationale and the actual risks and benefits of this phenomenon.
Although 32% of all-cause hospitalisations were found in the following three months after exposure of digoxin-specific CM interactions, there were relatively rare occurrences of digoxin intoxication, arrhythmia, bradycardia, acute renal failure or hypopotassemia in this study. These might be due to underreporting or under-documenting the relevant signs, symptoms, precipitant factors, and associated concomitant medications in the health care settings and/or the fact that no actual harmful impact occurred for some reasons. With the relatively less common use of digoxin, incident digoxin-CM use and incident digoxin-specific CM interactions, the rare occurrence of clinical and economic consequences in any aspect might encounter a Type II error since the sample size is not big enough for the assessment of
outcomes. Further studies utilising open cohort across several study years to recruit more subjects might be able to overcome this pitfall, in particular if digoxin use and digoxin-CM concurrent use were not as rare as our findings suggest.
Several other limitations in our study need to be addressed. First, there is limited information describing actual medication use patterns (NHI covered medications only), disease status (up to 3 diagnoses were documented in outpatient datasets and up to 5 diagnoses in inpatient datasets) and health service utilisation (only NHI covered and co-payment) using the NHIRD databases, which are derived from the LHID administrative claimed datasets. While only 6% of adults had ever used non-covered TCM therapies [53] and the majority of all NHI beneficiaries using TCM therapies had ever been prescribed with concentrated CMs in Taiwan [43], this study explored the actual concurrent use patterns of digoxin with CMs among the elderly. Second, the extent of concurrent use in this study was different from that of other studies due to the different data resources, study designs, and focused populations, as well as the definitions of Western medications and Chinese medications. Third, the specified propensities scores were used to 1:1 match the counterpart digoxin-only elderly users with incident digoxin-CM elderly users and incident digoxin-specific CM users. There were still some different characteristics between incident digoxin-CM elderly users/incident digoxin-specific CM elderly users and the corresponding digoxin-only elderly users. Thus, we did not perform conditional logistic regression, as other studies did [12-14], in order to examine the factors associated with new concurrent use and interactions of digoxin and CMs; instead we conducted traditional univariate and multivariate logistic regression analyses, which assumed that individuals were independent from each other. Further, while our findings could be an example to other countries practicing Chinese medicine or CAMs commonly, future cross-nation studies in Asia or worldwide might be needed to verify the findings and enhance their generalisation.
In conclusion, there were relatively rare incidents of digoxin prescription, digoxin-CM use and the occurrence of new digoxin-specific CM interactions among the elderly in Taiwan. While those who utilised more outpatient services and
medications might increase the exposure of incident digoxin-CM use and incident digoxin-specific CM interactions among the elderly, more attention should be paid to those elderly with specific diseases (heart disease and BPH) and checking their digoxin concentration more aggressively to follow-up the risks and benefits. We recognise this study as an initiative to explore the elderly concurrent use of Chinese medications with digoxin, and demonstrated that no significant harm occurred. Overall, these findings are substantial and informative to support that Taiwanese physicians practicing either Western medicine or Chinese medicine are very
responsible for prescribing medications cautiously for the elderly in order to mitigate problems associated with a system that has patients using multiple prescribers and visiting multiple hospital settings, possibly without any concern about medication toxicities that the patient may experience.
Acknowledgements
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The interpretation and
conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health or National Health Research Institutes, and financial sponsors. This study was fully supported by the National Science Council (NSC 99-2320-B-039-031-MY3), and partially sponsored by (CCMP-102-RD-003). The funding agencies had no role in the study implementation, analysis or interpretation of data, or preparation, review or approval of the manuscript.None of the authors have any conflicts of interest that are directly relevant to the content of this article.
References:
1. Merle L, Laroche ML, Dantoine T, Charmes JP: Predicting and preventing adverse drug reactions in the very old. Drugs Aging 2005, 22(5):375-392. 2. Gallagher P, Barry P, O'Mahony D: Inappropriate prescribing in the
elderly. J Clin Pharm Ther 2007, 32(2):113-121.
3. Obreli-Neto PR, Nobili A, de Oliveira Baldoni A, Guidoni CM, de Lyra Junior DP, Pilger D, Duzanski J, Tettamanti M, Cruciol-Souza JM, Gaeti WP et al: Adverse drug reactions caused by drug-drug interactions in elderly outpatients: a prospective cohort study. Eur J Clin Pharmacol 2012, 68(12):1667-1676.
4. Grant SJ, Yu SB, Kiat H, Chang D: The use of complementary and
alternative medicine by people with cardiovascular disease: a systematic review. BMC public health 2012, 12(1):299.
5. Cheung CK, Wyman JF, Halcon LL: Use of complementary and alternative therapies in community-dwelling older adults. J Altern Complement Med 2007, 13(9):997-1006.
6. Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, Kessler RC: Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA 1998, 280(18):1569-1575.
7. Alherbish A, Charrois TL, Ackman ML, Tsuyuki RT, Ezekowitz JA: The prevalence of natural health product use in patients with acute
cardiovascular disease. PloS one 2011, 6(5):e19623.
8. Chung VC, Hillier S, Lau CH, Wong SY, Yeoh EK, Griffiths SM: Referral to and attitude towards traditional Chinese medicine amongst western medical doctors in postcolonial Hong Kong. Social science & medicine
(1982) 2011, 72(2):247-255.
9. Ahmed A: DEFEAT - Heart Failure: a guide to management of geriatric heart failure by generalist physicians. Minerva medica 2009, 100(1):39-50. 10. Yang EH, Shah S, Criley JM: Digitalis toxicity: a fading but crucial
complication to recognize. The American journal of medicine 2012, 125(4):337-343.
11. American Geriatrics Society Beers Criteria Update Expert P: American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012, 60(4):616-631.
12. Chan AL, Wang MT, Su CY, Tsai FH: Risk of digoxin intoxication caused by clarithromycin-digoxin interactions in heart failure patients: a population-based study. Eur J Clin Pharmacol 2009, 65(12):1237-1243. 13. Wang MT, Li IH, Lee WJ, Huang TY, Leu HB, Chan AL: Exposure to
sennoside-digoxin interaction and risk of digoxin toxicity: a population-based nested case-control study. Eur J Heart Fail 2011.
14. Wang MT, Su CY, Chan AL, Lian PW, Leu HB, Hsu YJ: Risk of digoxin intoxication in heart failure patients exposed to digoxin-diuretic interactions: a population-based study. Br J Clin Pharmacol 2010, 70(2):258-267.
15. Chow L, Johnson M, Wells A, Dasgupta A: Effect of the traditional Chinese medicines Chan Su, Lu-Shen-Wan, Dan Shen, and Asian ginseng on serum digoxin measurement by Tina-quant (Roche) and Synchron LX system (Beckman) digoxin immunoassays. J Clin Lab Anal 2003, 17(1):22-27.
16. Dasgupta A, Szelei-Stevens KA: Neutralization of free digoxin-like immunoreactive components of oriental medicines Dan Shen and Lu-Shen-Wan by the Fab fragment of antidigoxin antibody (Digibind).
American journal of clinical pathology 2004, 121(2):276-281.
17. Mao JY, Xu WR, Wang HH: [Clinical study on effect of shengmai injection on serum concentration and pharmacokinetic parameters of digoxin in patients with congestive heart failure]. Zhongguo Zhong Xi Yi Jie He Za Zhi 2003, 23(5):347-350.
18. Reyes MA, Actor JK, Risin SA, Dasgupta A: Effect of Chinese medicines Chan Su and Lu-Shen-Wan on serum digoxin measurement by Digoxin III, a new digoxin immunoassay. Ther Drug Monit 2008, 30(1):95-99. 19. Tankanow R, Tamer HR, Streetman DS, Smith SG, Welton JL, Annesley T,
Aaronson KD, Bleske BE: Interaction study between digoxin and a
preparation of hawthorn (Crataegus oxyacantha). J Clin Pharmacol 2003, 43(6):637-642.
20. Zeilmann CA, Dole EJ, Skipper BJ, McCabe M, Low Dog T, Rhyne RL: Use of herbal medicine by elderly Hispanic and non-Hispanic white patients.
Pharmacotherapy 2003, 23(4):526-532.
21. Zlotogorski Hurvitz A, Littner M: [Potential risks, adverse effects and drug interactions associated with herbal medicine in dental patients].
22. Tsai HH, Lin HW, Lu YH, Chen YL, Mahady GB: A review of potential harmful interactions between anticoagulant/antiplatelet agents and Chinese herbal medicines. PloS one 2013, 8(5):e64255.
23. Mashour NH, Lin GI, Frishman WH: Herbal medicine for the treatment of cardiovascular disease: clinical considerations. Arch Intern Med 1998, 158(20):2225-2234.
24. Izzo A, Ernst E: Interactions Between Herbal Medicines and Prescribed Drugs. Drugs 2001, 61(15):2163-2175.
25. Marrone CM: Safety issues with herbal products. The Annals of
pharmacotherapy 1999, 33(12):1359-1362.
26. Yaheya Mohammad IM: HERB-DRUG INTERACTIONS AND PATIENT COUNSELING. International Journal of Pharmacy and Pharmaceutical
Sciences 2009, 1:151-159.
27. MHRA-Medicines and Healthcare Products Regulatory Agency U-PD: Public Health Risk with Herbal Medicines: an Overview. July 2008:1-6.
28. World Health Organization G, 2004: WHO Guidelines on Safety
Monitoring of Herbal Medicines in Pharmacovigilance Systems. 2004:1-82.
29. Albert NM, Rathman L, Ross D, Walker D, Bena J, McIntyre S, Philip D, Siedlecki S, Lovelace R, Fogarty AM et al: Predictors of over-the-counter drug and herbal therapies use in elderly patients with heart failure. J
Card Fail 2009, 15(7):600-606.
30. Tindle HA, Davis RB, Phillips RS, Eisenberg DM: Trends in use of
complementary and alternative medicine by US adults: 1997-2002. Altern
Ther Health Med 2005, 11(1):42-49.
31. Rossler W, Lauber C, Angst J, Haker H, Gamma A, Eich D, Kessler RC, Ajdacic-Gross V: The use of complementary and alternative medicine in the general population: Results from a longitudinal community study.
Psychol Med 2007, 37(1):73-84.
32. Chou P: Factors related to utilization of traditional Chinese medicine in Taiwan. Zhonghua yi xue za zhi = Chinese medical journal; Free China ed 2001, 64(4):191-202.
33. Sibbritt D, Adams J, Murthy V: The prevalence and determinants of
Chinese medicine use by Australian women: analysis of a cohort of 10,287 women aged 56-61 years. The American journal of Chinese medicine 2013, 41(2):281-291.
34. Shih CC, Liao CC, Su YC, Tsai CC, Lin JG: Gender differences in
traditional Chinese medicine use among adults in Taiwan. PloS one 2012, 7(4):e32540.
35. Chang LC, Huang N, Chou YJ, Lee CH, Kao FY, Huang YT: Utilization patterns of Chinese medicine and Western medicine under the National Health Insurance Program in Taiwan, a population-based study from 1997 to 2003. BMC Health Serv Res 2008, 8:170.
36. 中藥藥品許可證查詢
[http://www.ccmp.gov.tw/information/license_search.asp? relno=513&level=C]
37. Tsai HH, Lin HW, Chien CR, Li TC: Concurrent use of antiplatelets, anticoagulants, or digoxin with Chinese medications: a population-based cohort study. European Journal of Clinical Pharmacology 2012:1-11.
38. Mehta DH, Phillips RS, Davis RB, McCarthy EP: Use of complementary and alternative therapies by Asian Americans. Results from the National Health Interview Survey. J Gen Intern Med 2007, 22(6):762-767.
39. Gagne JJ, Polinski JM, Kesselheim AS, Choudhry NK, Hutchins D, Matlin OS, Tong A, Shrank WH: Patterns and predictors of generic narrow therapeutic index drug use among older adults. J Am Geriatr Soc 2013, 61(9):1586-1591.
40. Bin YS, Kiat H: Prevalence of dietary supplement use in patients with proven or suspected cardiovascular disease. Evid Based Complement
Alternat Med 2011, 2011:632829.
41. Yeh GY, Davis RB, Phillips RS: Use of complementary therapies in patients with cardiovascular disease. The American journal of cardiology 2006, 98(5):673-680.
42. Shih CC, Lin JG, Liao CC, Su YC: The utilization of traditional Chinese medicine and associated factors in Taiwan in 2002. Chin Med J (Engl) 2009, 122(13):1544-1548.
43. Chen FP, Chen TJ, Kung YY, Chen YC, Chou LF, Chen FJ, Hwang SJ: Use frequency of traditional Chinese medicine in Taiwan. BMC Health Serv
Res 2007, 7:26.
44. Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH:
Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a US consensus panel of experts. Arch Intern
Med 2003, 163(22):2716-2724.
45. Ma CH, Lin WL, Lui SL, Cai XY, Wong VT, Ziea E, Zhang ZJ: Efficacy and safety of Chinese herbal medicine for benign prostatic hyperplasia:
systematic review of randomized controlled trials. Asian journal of
andrology 2013, 15(4):471-482.
46. Lin YH, Chen KK, Chiu JH: Trends in Chinese Medicine Use Among Prostate Cancer Patients Under National Health Insurance in Taiwan: 1996-2008. Integr Cancer Ther 2011.
47. Lin HC, Yang WC, Lee HC: Traditional Chinese medicine usage among schizophrenia patients. Complement Ther Med 2008, 16(6):336-342. 48. Liao HL, Ma TC, Li YC, Chen JT, Chang YS: Concurrent Use of
Corticosteroids with Licorice-Containing TCM Preparations in Taiwan: A National Health Insurance Database Study. J Altern Complement Med 2010, 16(5):539-544.
49. National Health Insurance Research Database [http://www.nhri.org.tw/nhird/en/index.htm]
50. Chan ALF, Leung HWC, Wu J-W, Chien T-W: Risk of hemorrhage associated with co-prescriptions for Ginkgo biloba and antiplatelet or anticoagulant drugs. Journal of Alternative & Complementary Medicine 2011, 17(6):513-517.
51. Rathore SS, Curtis JP, Wang Y, Bristow MR, Krumholz HM: Association of serum digoxin concentration and outcomes in patients with heart failure.
JAMA 2003, 289(7):871-878.
52. Whitbeck MG, Charnigo RJ, Khairy P, Ziada K, Bailey AL, Zegarra MM, Shah J, Morales G, Macaulay T, Sorrell VL et al: Increased mortality among patients taking digoxin--analysis from the AFFIRM study. Eur Heart J 2013, 34(20):1481-1488.
53. Shih SF, Lew-Ting CY, Chang HY, Kuo KN: Insurance covered and non-covered complementary and alternative medicine utilisation among adults in Taiwan. Soc Sci Med 2008, 67(7):1183-1189.
* for each incident digoxin-CM elderly user, we randomly selected a digoxin user from the propensity score derived from the combination of the following variables: the month of the index date, the same duration of digoxin use, age, with or without catastrophic certification, outpatient clinic visits per year, number of prescribed distinct medications, total medical expenditure.
#: There were 385 incident digoxin-CM elderly users prescribed with specific CMs, which were proven to have interactions with digoxin (i.e., incidence of digoxin-specific CM interaction among elderly=0.21%) so that another 385 elderly who were prescribed with digoxin only were matched accordingly upon the propensity score LHID=longitudinal health insurance database; NHI=national health insurance; CM=Chinese medication
Table 1. Duration of concurrent use in days of digoxin with specific CMs, which had evidence of digoxin-CM interactions, in 2006
Chinese herbal medication in
English
All digoxin-CHM elderly users (n=789)
Incident digoxin-CHM elderly users (n=400) Number of users (%) Duration of concurrent use Mean±SD Number of users Duration of concurrent use Mean±SD Da Huang 190 (24.1%) 27.88±50.53 66 (16.5%) 13.91±14.66 Hawthorn 34 (4.3%) 14.12±22.29 17 (4.3%) 10.71±10.68 Danshen 150(19.0%) 21.42±34.36 66 (16.5%) 15.97±19.64 Liquorice 717 (90.9%) 27.99±43.84 376 (94%) 16.52±23.65 Oyster shell 84 (10.6%) 14.62±17.41 35 (8.75%) 10.08±7.93 Siberian ginseng 1 (0.1%) 30 0 (0.0%) -- Senna 2 (0.2%) 10.5±21.2 0 (0.0%) -- Aloe Vera 4 (0.5%) 7±4.76 1 (0.25%) 4
Table 2: Comparisons of patient characteristics between incident digoxin-CM elderly users and the corresponding matched digoxin-only elderly users
Characteristic No. (%) p-value Total Elderly digoxin users Incident-digoxin-CHM elderly users Digoxin-only elderly users Sample size 789 400 389 Female (%) 443(56.15%) 225(56.25%) 218(56.04%) 0.9529 Age in years Mean 76.45±6.46 75.95±6.15 77.00±6.69 0.0366* Medium 76 75 77 65-69 118(14.96%) 62(15.50%) 56(14.40%) 0.0732 70-74 215(27.25%) 124(31.00%) 91(23.39%) 75-79 222(28.14%) 105(26.25%) 117(30.08%) ≥80 234(29.66%) 109(27.25%) 125(32.13%)
Monthly reported income (TWD) 0.3007
≤17280 506(64.13%) 256(64.00%) 250(64.27%)
17281-28800 267(33.84%) 139(34.75%) 128(32.90%)
28801-45800 6(0.76%) 3(0.75%) 3(0.77%)
45801-72800 2(0.25%) 1(0.25%) 1(0.26%)
≥72801 8(1.01%) 1(0.25%) 7(1.80%)
Region of NHI enrolment 0.3081
North 379(48.04%) 195(48.75%) 184(47.30%) Central 180(22.81%) 99(24.75%) 81(20.82%) South 194(24.59%) 88(22.00%) 106(27.25%) East 23(2.92%) 12(3.00%) 11(2.83%) Other 3(0.72%) 5(1.25%) 3(0.77%) No data 4(1.03%) 1(0.25%) 4(1.03%) Comorbiditya Hypertension 491(62.23%) 253(63.25%) 238(61.18%) 0.5576 Heart diseases 629(79.72%) 340(85.00%) 289(74.29%) 0.0002*# Stroke 177(22.43%) 90(22.50%) 87(22.37%) 0.9638 Cancer 31(3.93%) 18(4.50%) 13(3.34%) 0.4656 Diabetes 185(23.45%) 89(22.25%) 96(24.68%) 0.4498 Hyperlipidaemia 127(16.10%) 66(16.50%) 61(15.68%) 0.7720 Asthma 71(9.00%) 39(9.75%) 32(8.23%) 0.4590 Pneumonia 52(6.59%) 26(6.50%) 26(6.68%) 1.0000 Benign prostatic hyperplasia (BPH) 115(14.58%) 73(18.25%) 42(10.80%) 0.0034*# Seizure 11(1.39%) 3(0.75%) 8(2.06%) 0.1382 Depression 59(7.48%) 32(8.00%) 27(6.94%) 0.5909 Chronic kidney disease 6(0.76%) 4(1.00%) 2(0.05%) 0.9872
Outpatient clinic visits in 2006a Mean 3.28±2.15 3.60±2.14 2.91±2.08 <0.0001*# Medium 2.2 3.3 2.2 <13 168(21.29%) 55(13.75%) 113(29.05%) <0.0001* 13-24 230(29.15%) 113(28.25%) 117(30.08%) 25-36 159(20.15%) 93(23.25%) 66(16.97%) 37-48 87(11.03%) 53(12.79%) 34(8.74%) 49-60 55(6.97%) 34(8.50%) 21(5.40%) ≥61 90(11.41%) 52(13.00%) 38(9.77%)
Number of prescribed distinct medications a
Mean 22.26±14.39 25.12±15.18 18.89±12.31 <0.0001*#
Medium 19 21.5 16
Total items of prescribed distinct medications a <0.0001*#
<10 126(15.97%) 39(9.75%) 87(22.37%) 10-19 296(37.52%) 142(35.50%) 154(39.59%) 20-29 176(22.31%) 93(23.25%) 83(21.34%) 30-39 104(13.18%) 66(16.50%) 38(9.77%) ≥40 87(11.03%) 60(15.00%) 27(6.94%) Ever hospitalisationa* 163(20.66%) 82(20.50%) 81(20.82%) 0.9301 Total medical expenditure( TWD)a
Mean 44,892.41 42,433.44 47,545.67 0.1634
(Min-Max) (0-1,293,339) (782-1,177,231) (0-1,293,339)
Medium 21,219.50 21,869 19,804
Interval of total medical expenditure*a 0.0654
<10000 181(22.94%) 78(19.50%) 103(26.48%)
10001-29999 340(43.09%) 181(45.25%) 159(40.87%) 30000-49999 119(15.08%) 68(17.00%) 51(13.11%)
≥50000 149(18.88%) 73(18.25%) 76(19.54%)
a: Ascertained during the 6-month period prior to the date of first CM prescription #: There were statistically significant differences between elderly encountered
incident digoxin-specific CM interactions and the corresponding digoxin-only elderly users.
Note: we used chi-square tests and t-test to compare differences between incident digoxin-CM elderly users and digoxin-only elderly users for nominal scale and continuous variables.
Table 3: Factors associated with exposure of incident concurrent use of digoxin with CHM among the elderly (logistic regression)
Crude odds ratio after single logistic regression
analysis OR (95% CI)
Adjusted odds ratio after multivariate logistic regression analysis Adjusted OR (95% CI) Gender Male Female 1 0.995 (0.737-1.344) 1 1.282 (0.910-1.806) Age in years 65-69 70-74 75-79 ≧80 1 1.024 (0.637-1.644) 0.734 (0.458-1.177) 0.766 (0.479-1.226) 1 1.070 (0.646-1.773) 0.689 (0.416-1.140) 0.735 (0.442-1.221) Monthly reported income
(TWD) ≦17280 17281-28800 28801-45800 1 0.957 (0.695-1.316) 0.593 (0.191-1.839) 1 1.049 (0.739-1.489) 0.851 (0.252-2.871) Region of NHI enrolment
North Central South East Other 1 1.172 (0.800-1.717) 0.694 (0.479-1.005) 1.131 (0.527-2.425) 0.307 (0.032-2.977) 1 1.050 (0.692-1.592) 0.621 (0.413-0.934)* 0.923 (0.401-2.122) 0.396 (0.037-4.244) Disease statusesa With Hypertension 1.011 (0.745-1.372) 1.014 (0.727-1.416) With heart disease+ 1.986 (1.359-2.901)* 2.151 (1.428-3.240)*
With MI 0.773 (0.301-1.982) 0.630 (0.228-1.735)
With Ventricular arrhythmias
1.188 (0.747-1.891) 1.168 (0.698-1.953)
With Heart failure 0.848 (0.541-1.331) 0.911 (0.548-1.514) With stroke 1.050 (0.731-1.509) 1.047(0.695-1.576)
a: Ascertained during the 6-month period prior to the date of first CM prescription * represent these variables were statistically significant factors associated with occurrence of digoxin-specific CHM interactions, where 95% CI not included 1.
Table 4: Impact of concurrent use of digoxin with CHM after three-month follow-up since initial concurrent use
No. (%) p-value Total Elderly digoxin users (n=692) Incident digoxin-CHM elderly users (n=351) Digoxin-only elderly users (n=341) Impact/Outcomes after
Health service utilisation
All-causes of hospitalisations 224(32.4%) 121 (34.5%) 103(30.2%) 0.1550 Hospitalisation 106 (15.32%) 61 (17.38%) 45 (13.20%) 0.1267 Emergency room visits 118 (17.05%) 60 (17.09%) 58 (17.01%) 0.9762 Three-month medical expenditure after index dates (TWD)
Total ER expenditure/person 31,255 32,219 30,263 0.8489
Total inpatient expenditure/person 26,776 24,707 28,906 0.5350 Total outpatient expenditure/person 109,633 118,498 100,508 0.4669 Clinical outcomes
Disease statues and/or disorders related to digoxin intoxication
Due to digoxin intoxications 2 (0.29%) 1 (0.28%) 1 (0.29%) 0.9837 Due to ventricular arrhythmia and
atrioventricular block, bradycardia
42 (6.07%) 19 (5.41%) 23 (6.74%) 0.4632
Acute renal failure 2 (0.29%) 1 (0.28%) 1 (0.29%) 0.9837
Hypopotassemia 8 (1.16%) 5 (1.42%) 3 (0.88%) 0.5027
Checking digoxin levels in outpatient or inpatient visits
37 (5.35%) 20 (5.70%) 17 (4.99%) 0.6769
Factors associated with digoxin toxicity
Chronic renal failure 5 (0.72%) 3 (0.85%) 2 (0.59%) 0.6771
Hypomaganesium 0 0 0
-Hypercalcemia 0 0 0
-Mixed acid-base balance disorder 1 (0.14%) 1 (0.28%) 0 0.3240
Hyperpotassemia 4 (0.58%) 3 (0.85%) 1 (0.29%) 0.3300
Hypothyroidism 0 0 0
-Concomitant mediations, which might be associated with digoxin intoxication and/or toxicity (AV block, arrhythmia); *censor up to December 31, if no health service utilisation reported in 2006
All types of diuretics
thiazides 40 (5.78%) 20 (5.70%) 20 (5.87%) 0.9250 Loop 237 (34.25%) 124 (35.33%) 113 (33.14%) 0.5439 Potassium-sparing 77 (11.13%) 49 (13.96%) 28 (8.21%) 0.0162* Potassium supplements 22 (3.18%) 14 (3.99%) 8 (2.35%) 0.2182 Angiotensin-converting enzyme inhibitors (ACEI) 186 (26.88%) 98 (27.92%) 88 (25.81%) 0.5306 P-glycoprotein inhibitors 204 (29.48%) 109 (31.05%) 95 (27.86%) 0.3568 Non-steroidal anti-inflammatory drugs (NSAID) 328 (47.40) 196 (55.84%) 132 (38.71%) <0.0001 * Medications that might cause
transcellular potassium shift