Hypertensive Disorders in Pregnancy and Subsequent
Diabetes Mellitus: A Retrospective Cohort Study
I-Kuan Wang, MD,a,bI-Ju Tsai, MS,c,dPei-Chun Chen, PhD,c,dChih-Chia Liang, MD,aChe-Yi Chou, MD,a
Chiz-Tzung Chang, PhD,aHuey-Liang Kuo, MD,aI-Wen Ting, MD,aChung-Chih Lin, MD,aFeng-Rong Chuang, MD,e
Chiu-Ching Huang, MD,a Fung-Chang Sung, PhD, MPH,c,d
a
Division of Kidney Disease andb
Institute of Clinical Medical Science, College of Medicine,c
Management Office for Health Data, and
d
Department of Public Health, China Medical University and Hospital, Taichung, Taiwan;e
Kaohsiung Chang Gung Memorial Hospital Medical Center, Chang Gung University College of Medicine, Kaohsiung, Taiwan.
ABSTRACT
BACKGROUND: Cohort study on the association between hypertensive disorders in pregnancy (HDP) and postpartum diabetes is limited. This retrospective cohort study investigated the incidence of diabetes mellitus after delivery among women with HDP using claims data of a universal insurance system. METHODS: We defined the HDP group as women aged 19-40 years with their first HDP in 2003, excluding those with a history of gestational diabetes mellitus, diabetes mellitus, or hypertension before the date of diagnosis with HDP. Women who had normal pregnancy without HDP were randomly chosen as our comparison group, frequency matched with age and index year of the HDP group. Both groups were followed until December 31, 2008 to evaluate the occurrence of diabetes.
RESULTS: This study consisted of 1139 women with HDP cases and 4527 non-HDP pregnant women. Overall, the subsequent incidence of diabetes mellitus was 5.08-fold higher in the HDP group than in the non-HDP group, with an adjusted hazard ratio of 3.42 (95% confidence interval [CI], 2.07-5.64) after controlling for age, occupation, income, and comorbidity. The hazard ratio of developing diabetes increased to 39.5 (95% CI, 13.0-120.6) for women having HDP, hyperlipidemia, and obesity simultaneously.
CONCLUSIONS: Women with HDP have a high risk of subsequent diabetes. HDP women with obesity and hyperlipidemia are at an extremely high risk of diabetes mellitus. Early identification of women with HDP is needed for prevention, particularly those with other comorbidities.
© 2012 Elsevier Inc. All rights reserved. • The American Journal of Medicine (2012) 125, 251-257 KEYWORDS: Diabetes; Eclampsia; Gestational hypertension; Preeclampsia; Pregnancy
Gestational hypertension and preeclampsia are hypertensive disorders in pregnancy (HDP).1Gestational hypertension is defined as the onset of hypertension (ⱖ140/90 mm Hg) without proteinuria after 20 weeks of gestation, while
preeclampsia is referred to as the onset of hypertension (ⱖ140/90 mm Hg) with proteinuria (ⱖ0.3 g/24 hours), also after 20 weeks of gestation. HDP may complicate 5%-10% of all pregnancies.2 Gestational hypertension evolves into preeclampsia in 10%-20% of cases.3 Pre-eclampsia is one of the common causes of maternal and fetal morbidity and mortality.4 Both case-control and
cohort studies have reported that women with HDP are at an elevated risk of later metabolism disorders and car-diovascular disease.5-7 Metabolic abnormalities, includ-ing obesity, insulin resistance, and dyslipidemia, featur-ing metabolic syndrome, are risk factors for both HDP and cardiovascular disease.8-12 On the other hand, HDP may lead to an exaggeration of insulin resistance and is associated with abnormal metabolic change during
preg-Funding: The work was funded by the Executive Yuan National
Science Council (grant number NSC 99-2621-M-039 -001), the Depart-ment of Health (grant numbers TD-B- 111-004 and DOH100-TD-C-111-005), and the China Medical University Hospital (grant number 1MS1).
Conflict of Interest: None.
Authorship: The work is original and all authors significantly
contrib-uted to this paper and accept responsibility for its scientific content. Requests for reprints should be addressed to Fung-Chang Sung, PhD, MPH, China Medical University and Hospital College of Public Health, 91 Hsueh Shih Road, Taichung 404, Taiwan.
E-mail address:[email protected]
0002-9343/$ -see front matter © 2012 Elsevier Inc. All rights reserved. doi:10.1016/j.amjmed.2011.07.040
nancy.13Vascular and metabolic abnormalities occurring in HDP may persist through postpartum.14-16Therefore, it is likely that women predisposed to insulin resistance are more likely to develop HDP and more likely to have subsequent hypertension, atherosclerosis, and type 2 di-abetes mellitus in later life,
which eventually lead to cardio-vascular disease.
Limited cohort studies have re-ported the association between HDP and subsequent diabetes mellitus (DM) for Western popu-lations.6,17-19The Danish National Patient Registry study found that preeclampsia is associated with 3.12-3.68 –fold risk of developing type 2 diabetes.6 The risk of dia-betes is much greater for women with preeclampsia who undergo preterm delivery and deliver in-fants who are small for gestational age. However, no study has inves-tigated the interaction of pregnant hypertensive disorders with other metabolic abnormalities for the subsequent DM. This retrospec-tive cohort study investigated the
risk of DM after delivery for Asian women with HDP and interaction with other metabolism abnormalities, using pop-ulation-based universal insurance claims data.
MATERIALS AND METHODS
Data Source
Data used in this study were extracted from National Health Insurance Research Database, an electronic claims database of the Taiwan National Health Insurance (NHI) program. Details of the NHI have been described elsewhere.20 Briefly, NHI is a universal health insurance program re-formed in providing health care services to 99% of the population of Taiwan. More than 90% of health care insti-tutions have contracted with the NHI. For this study, we used a subset of the National Health Insurance Research Database containing comprehensive health care data includ-ing files of inpatient claims, ambulatory care claims, and prescriptions for one million people randomly selected from the entire 23 million beneficiaries of NHI. We linked these files using the encrypted unique personal identifiers to ob-tain longitudinal medical history of each individual. Diag-noses were based on the International Classification of Dis-eases, Ninth Revision, Clinical Modification (ICD-9-CM). The scrambled personal identifications secured the individ-ual’s confidentiality, preventing ethical violation of the claims data.
Study Subjects
We conducted the retrospective cohort analysis to determine the association between HDP (ICD-9 code 642) and DM (ICD-9 code 250 or A-code A181). From the 1997-2003 claims data, we identified 1520 women aged 19-40 years with their first HDP. Exclusions were those with a baseline history of gestational DM (n⫽ 280; ICD-9 code 648.0 and 648.8), and those with DM (n⫽ 55) or hypertension (n⫽ 146) identified before the date of diagnosis with HDP. The remain-ing 1139 women with the first HDP were considered as the HDP cohort. Women who had normal pregnancy (ICD-9 code 650 or A-code A41) without HDP were randomly cho-sen as our comparison group, fre-quency matched on age (every 5 years) and the index year of HDP group, using the inclusion criteria similar to the HDP group. The HDP and non-HDP groups were selected in a 1:4 ratio in order to enhance the power of statistical tests. All subjects were fol-lowed-up to evaluate the occur-rence of diabetes until December 31, 2008 or censored because of death, withdrawal from the insurance program, or loss to follow-up. Comorbidities including obesity (ICD-9 code 278.0 or A-code A183), hyperlipidemia (ICD-9 code 272 or A-code A182), preterm delivery (ICD-9 code 644), and abruption (ICD-9 code 641.2) were consid-ered in data analyses.
Statistical Analysis
Data analyses first calculated the incidences of DM devel-oped in both HDP and non-HDP groups and the HDP-to-non-HDP rate ratios by demographic status and comorbidi-ties such as obesity, hyperlipidemia, preterm delivery, and placenta abruption. The Cox proportional hazardous regres-sion analyses measured corresponding hazard ratios (HRs) with 95% confidence intervals (95% CIs). Both crude HRs and multivariable adjusted HRs were measured. Simple linear regression was used to evaluate trends of rate ratios for diabetes in HDP vs non-HDP groups for age, occupa-tion, and income. Logistic regression model was used to measure odds ratios with 95% CIs to evaluate the associa-tions between HDP and baseline comorbidities, including obesity, hyperlipidemia, and the history of preterm delivery or placenta abruption. We plotted the Kaplan-Meier curves to compare the probability of diabetes developing between women with HDP and without HDP during the study period and used the log-rank test to examine the significance of difference between the 2 groups. To differentiate how the risk of diabetes was associated with age between the HDP
CLINICAL SIGNIFICANCE
● The postpartum incidence of diabetes mellitus is approximately 5-fold higher in women with hypertensive disorders in pregnancy (HDP) than in women without HDP.
● Among women with HDP, those with pre-eclampsia/eclampsia are more likely to develop diabetes mellitus than women with only gestational hypertension. ● The hazard ratio of developing diabetes
mellitus increased to approximately 40-fold higher for women with HDP, hyper-lipidemia, and obesity simultaneously.
and non-HDP cohorts, we measured the HR for each age group, compared with non-HDP subjects aged 19-24 years. Interactions between HDP and baseline metabolism abnor-malities in association with developing diabetes also were measured. Information on metabolism abnormalities in terms of obesity and hyperlipidemia is available in the claims data. For the HDP group, we further classified them into 2 groups: women with only gestational hypertension (ICD-9 code 642.3) and women with preeclampsia/eclamp-sia (ICD-9 codes 642.4-642.6) to examine whether the se-verity of the hypertensive disorder correlated with the HR of developing diabetes. We used SAS software (version 9.1 for windows; SAS Institute Inc., Cary, NC) for all statistical analyses. All significant levels were set at a 2-tailed P value of⬍.05. Kaplan-Meier curves were plotted using R (version 2.11.1; R Development Core Team, Vienna, Austria, 2010).
RESULTS
This study consisted of 1139 women with HDP and 4527 non-HDP women for data analyses after excluding ineligi-ble subjects. The mean ages were similar in the HDP and
non-HDP groups (29⫾ 4.8 years). The mean follow-up pe-riods were 8.1⫾ 2.1 years in the HDP cohort and 8.2 ⫾ 2.0 years in the non-HDP cohort (data not shown).
Table 1 demonstrates the incidences of DM in both cohorts, HDP-to-non-HDP rate ratios, and HRs of DM by socioeconomic status and comorbidity. The incidence of diabetes was 5.08-fold greater in the HDP women than in non-HDP women (42.4 vs 8.34 per 10,000 person-years); it increased with age in both groups. The age-specific inci-dence of diabetes increased much more in the HDP group than in the non-HDP group (P for trend ⬍.0001). The incidence rate ratio also increased with age, from 2.67 for women aged 19-24 years to 9.64 for those aged 35-40 years, with an HR of 4.15 (95% CI, 1.52-11.4) for the oldest women compared with the youngest women. The incidence of diabetes was 87.3 per 10,000 person-years in the oldest HDP women, nearly 10-fold greater than their counterpart non-HDP women. Among the comorbidities, the risk of developing diabetes had strong association with hyperlipid-emia (adjusted HR 12.2; 95% CI, 7.47-19.9) and obesity (adjusted HR 6.61; 95% CI, 3.17-13.8) but not with preterm
Table 1 Comparisons of Diabetic Incidences Between Women With and Without Hypertensive Disorders of Pregnancy and Associated Hazard Ratios by Sociodemographic Status and Comorbidity
Variables
Non-HDP HDP
Rate
Ratio Crude HR (95% CI)
Adjusted† HR (95% CI)
n Cases PY Rate* n Cases PY Rate*
All 4527 31 37,155 8.34 1139 39 9204 42.4 5.08 5.1 (3.19-8.18)‡ 4.99 (3.11-8.00)‡ Age, years 19-24 804 3 6686 4.5 201 2 1669 12.0 2.67 1.00 (Reference) 1.00 (Reference) 25-29 1540 9 12,562 7.2 385 8 3124 25.6 3.57 1.84 (0.68-5.00) 1.94 (0.71-5.27) 30-34 1520 14 12,385 11.3 380 17 3036 56.0 4.95 3.35 (1.30-8.62) 3.52 (1.36-9.13)§ 35-40 663 5 5522 9.1 173 12 1375 87.3 9.64 4.06 (1.50-10.99)§ 4.15 (1.52-11.35)§ Occupation
White collar 2988 20 24,176 8.3 745 18 5989 30.1 3.63 1.00 (Reference) 1.00 (Reference)
Blue collar 949 7 8320 8.4 250 12 2081 57.7 6.85 1.38 (0.80-2.40) 1.42 (0.80-2.51) Unemployed㛳 590 4 4659 8.6 144 9 1134 79.4 9.25 1.81 (0.96-3.39) 2.14 (0.97-4.70) Income ⬍15,000 1462 8 12,186 6.6 378 18 3085 58.3 8.89 1.00 (Reference) 1.00 (Reference) 15,000-29,999 2361 13 19,235 6.8 578 18 4622 38.9 5.76 0.77 (0.46-1.30) 0.89 (0.48-1.62) ⱖ30,000 704 10 5734 17.4 183 3 1497 20.0 1.15 1.07 (0.55-2.09) 1.23 (0.54-2.77) Co-morbidities Obesity No 4472 28 36,684 7.6 1086 34 8771 38.8 5.08 1.00 (Reference) 1.00 (Reference) Yes 55 3 471 63.6 53 5 433 115.4 1.81 6.33 (3.03-13.2) 6.61 (3.17-13.8) Hyperlipidemia No 4156 14 34,015 4.1 959 13 7694 16.9 4.11 1.00 (Reference) 1.00 (Reference) Yes 371 17 3140 54.1 180 26 1510 172.1 3.18 13.8 (8.53-22.4) 12.2 (7.47-19.9) Preterm delivery No 4502 26 36,942 7.0 1057 27 8471 31.9 4.53 1.00 (Reference) 1.00 (Reference) Yes 25 5 213 234.7 82 12 733 163.7 0.70 2.02 (0.63-6.42) 1.84 (0.58-5.85) Abruption No 4527 31 37,155 8.3 1133 39 9150 42.6 5.11 1.00 (Reference) 1.00 (Reference) Yes 0 0 0 – 6 0 54 0.0 – – –
CI⫽ confidence interval; HDP ⫽ hypertensive disorders in pregnancy; HR ⫽ hazard ratio; PY ⫽ person-years. *Per 10,000 person-years.
†Adjusted for age, occupation, and income. ‡P⬍.0001.
§P⬍.01.
delivery and abruption. The Kaplan-Meier analysis shows that the cumulative incidence of diabetes was 6% greater in the HDP group than in the non-HDP group, more prominent after the 7-year follow-up (P⬍.001) (Figure).
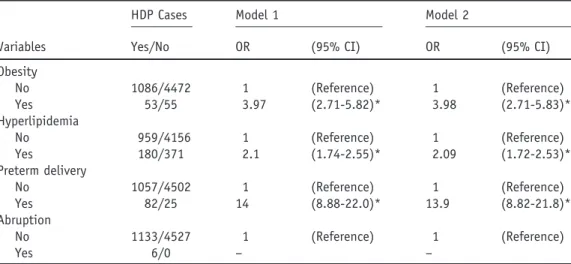
Table 2shows the prevalence of selected morbidities in association with HDP in the study subjects. Patients with HDP were more prevalent with obesity (4.7% vs 1.2%, P⬍.001), hyperlipidemia (15.8% vs 8.2%, P ⬍.001), and preterm delivery (7.2% vs 0.6%, P⬍.001).
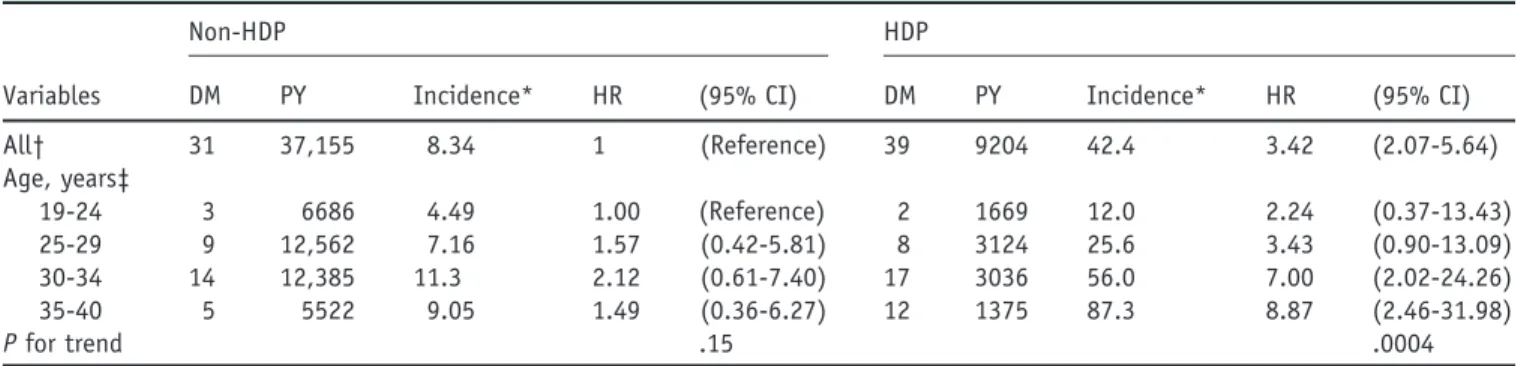
Table 3 shows the age-specific hazard of diabetic development for HDP and non-HDP groups separately,
comparing with 19- to 24-year-old women in the non-HDP group, after controlling for occupation, obesity, hyperlipidemia, and abruption. Age interacted with HDP. The increase of diabetic risk in the HDP group was particularly strong for patients aged 30-34 years and above with an adjusted HR of 8.87 (95% CI, 2.46-32.0) (P for trend .0004). Overall, the HDP cohort had a higher risk of diabetes than the non-HDP cohort, with an ad-justed HR of 3.42 (95% CI, 2.07-5.64) after controlling for age, occupation, income, and comorbidity.
The HDP women were further stratified into 2 subgroups by the severity of hypertensive disorders. Women with preeclampsia/eclampsia had a higher risk of developing diabetes (adjusted HR 4.15; 95% CI, 2.48-6.95) (Table 4), while women with only gestational hypertension were less likely to develop diabetes (adjusted HR 1.73; 95% CI, 0.78-3.81).
Data analyses further observed whether comorbidity interacted with HDP in the subsequent development of DM. The incidences of DM associated with HDP and preterm delivery or placenta abruption were not large enough to observe the effect. However, hyperlipidemia interacted strongly with HDP and obesity. The HR of developing diabetes increased to 39.5 (95% CI, 13.0-120.6) for women with HDP, hyperlipidemia, and obesity simultaneously (Table 5).
DISCUSSION
To the best of our knowledge, this study is the first one observing a high risk of subsequent DM associated with HDP for Asian women. The pathogenesis of preeclampsia is likely related to both maternal and fetal/placental fac-tors.21-23 It is likely that preeclampsia develops when
ab-normal placentation, through the release of anti-angiogenic factors, interacts with maternal constitutional metabolic
Figure The Kaplan-Meier model measured the diabetes-free proportions in the study cohorts with and without hypertensive disorders in pregnancy (HDP) during the follow-up period.
Table 2 Odds Ratio of HDP in Association with Comorbidities in Univariate and Multivariate Logistic Regression Models
Variables
HDP Cases Model 1 Model 2
Yes/No OR (95% CI) OR (95% CI)
Obesity No 1086/4472 1 (Reference) 1 (Reference) Yes 53/55 3.97 (2.71-5.82)* 3.98 (2.71-5.83)* Hyperlipidemia No 959/4156 1 (Reference) 1 (Reference) Yes 180/371 2.1 (1.74-2.55)* 2.09 (1.72-2.53)* Preterm delivery No 1057/4502 1 (Reference) 1 (Reference) Yes 82/25 14 (8.88-22.0)* 13.9 (8.82-21.8)* Abruption No 1133/4527 1 (Reference) 1 (Reference) Yes 6/0 – –
CI⫽ confidence interval; HDP ⫽ hypertensive disorders in pregnancy; OR ⫽ odds ratio. Model 1: Unadjusted; Model 2: Adjusted for age and occupation.
syndrome.24 Gestational hypertension may share the same
pathophysiological effect as preeclampsia.
Several cohort studies have demonstrated that insulin resistance in early pregnancy predisposes to HDP.9,11-12
Cross-sectional studies also have shown that HDP is asso-ciated with increased insulin resistance and metabolic syn-drome in the third trimester (relative to normal preg-nancy).13,25 Insulin resistance and associated metabolic
syndrome may still persist after delivery.14-16These studies
have clearly indicated an important relationship of poten-tially predisposing insulin resistance to HDP. Moreover, insulin resistance is exaggerated in HDP and persists after delivery in women with a history of HDP. In our study, obesity and hyperlipidemia, components of metabolic syn-drome, interact strongly with HDP for developing DM.
Several other recent studies also have demonstrated that HDP is associated with developing subsequent DM.6,17-19A
cohort study by Libby et al19 found that mothers with
preeclampsia had an adjusted odds ratio of 1.40 (95% CI, 1.12-1.75) for developing type 2 DM. But they did not exclude women with preexisting or gestational diabetes for their study. Callaway et al17performed a survey and found
that HDP was associated with subsequent diabetes 21 years after the pregnancy, with an adjusted odds ratio of 1.76 (95% CI, 1.21-2.56). However, that study also did not
exclude women with gestational diabetes. Carr et al18
re-ported that preeclampsia was associated with a high risk of subsequent diabetes, with an HR of 1.86 (95% CI, 1.22-2.84).18 But their study did not adjust for confounding
variables such as obesity and lifestyle. A Denmark regis-try-based study showed that the HRs of subsequent type 2 DM were 3.12 (95% CI, 2.63-3.70) for women with gestational hypertension and 3.63 (95% CI, 3.34-3.93) for women with preeclampsia. For women with preterm delivery and preeclampsia, the HR increased to 6.59 (95% CI, 5.34-8.13).6They also found that women with
2 episodes of preeclampsia had increased risk of subse-quent type 2 diabetes, compared with women with only 1 episode of preeclampsia. But this study also failed to exclude gestational diabetes and adjust for the confound-ing effect of obesity and hyperlipidemia.
In our study, we excluded women with preexisting hy-pertension, diabetes, or gestational diabetes at the baseline to reduce the confounding effect of gestational diabetes and preexisting hypertension. HDP was associated with subse-quent diabetes with an HR of 3.42 after controlling for age, occupation, and comorbidities. The risk is significantly in-creased with maternal age, and much stronger than in women without HDP. Among women with HDP, those with preeclampsia/eclampsia have more severe hypertensive
dis-Table 3 Age-specific Incidence of Diabetes in Women With and Without HDP and Cox Proportional Hazard Regression Measured Age-specific Hazard Ratio Compared With 19-24 Years Group in Non-HDP Group
Variables
Non-HDP HDP
DM PY Incidence* HR (95% CI) DM PY Incidence* HR (95% CI)
All† 31 37,155 8.34 1 (Reference) 39 9204 42.4 3.42 (2.07-5.64) Age, years‡ 19-24 3 6686 4.49 1.00 (Reference) 2 1669 12.0 2.24 (0.37-13.43) 25-29 9 12,562 7.16 1.57 (0.42-5.81) 8 3124 25.6 3.43 (0.90-13.09) 30-34 14 12,385 11.3 2.12 (0.61-7.40) 17 3036 56.0 7.00 (2.02-24.26) 35-40 5 5522 9.05 1.49 (0.36-6.27) 12 1375 87.3 8.87 (2.46-31.98) P for trend .15 .0004
CI⫽ confidence interval; DM ⫽ diabetes mellitus; HDP ⫽ hypertensive disorders in pregnancy; HR ⫽ hazard ratio; PY ⫽ person-years. *Per 10,000 person-years.
†Adjusted for age, occupation, obesity, and hyperlipidemia. ‡Adjusted for occupation, obesity, and hyperlipidemia.
Table 4 Multivariable Cox Proportional Hazard Regression Analysis for Risk of Diabetes in Women With and Without Hypertensive Disorders in Pregnancy
Group n DM PY Incidence* HR (95% CI)
Non-HDP 4527 31 37,155 8.34 1.00 (Reference)
GHT only 488 8 3864 20.70 1.73 (0.78-3.81)
Preeclampsia/eclampsia 651 31 5340 58.05 4.15 (2.48-6.95)†
CI⫽ confidence interval; DM ⫽ diabetes mellitus; GHT ⫽ gestational hypertension; HDP ⫽ hypertensive disorders in pregnancy; HR⫽ hazard ratio; PY ⫽ person-years. Adjusted for age, occupation, obesity, hyperlipidemia.
*Per 10,000 person-years. †P⬍.001.
orders. Most diabetes cases developed subsequently were in women who had experienced preeclampsia/eclampsia.
Another important finding in this study is that the women simultaneously having HDP, hyperlipidemia, and obesity are at extremely high risk of subsequent development of DM. This interaction term has not been reported previously. However, the interaction between preterm delivery and HDP was not significant in this study (P⫽ .99; data not shown). Because there was only 1 woman who had HDP twice (data not shown), we also failed to observe a signif-icant trend in the development of diabetes associated with multiple HDP episodes.
Limitations
Our study has several limitations. First, the National Health Insurance Research Database provided limited information on sociodemographic characteristics, with information un-available on marital status, educational level, smoking habit, and laboratory data. These variables could not be adjusted in the analysis. However, controlling for smoking habit and parity resulted in only a small change in odds ratio according to a previous study.17Moreover, we were able to use occupation and income for adjustment. Second, some information on chronic conditions, such as hyperlipidemia and obesity, was unavailable for a few individuals. How-ever, this situation happened in both groups. Finally, pnatal care may be different between medical centers, re-gional hospitals, local hospitals, and obstetrician clinics. The prenatal care at clinics has been standardized to adhere to the insurance system. Insurance claims are subject to be reviewed and validated by auditors of medical records to insure the accuracy of the claims. It is not likely that the prenatal care diagnosis of HDP will vary. Most women receive their prenatal care at hospitals. Our further data analysis showed that women in the HDP group and the non-HDP group had made 140 and 120 clinic visits on average, respectively, during the study period. Examination for DM was likely included in the routine clinic check-up.
CONCLUSIONS
In conclusion, our study results can be generalized to preg-nant women in Taiwan for the association between HDP and diabetes risk because we used a representative pregnant population data. The risk of subsequent diabetes in women with HDP was 3.4 times more than in those with uncom-plicated pregnancy. The risk doesn’t increase further for women with both HDP and preterm delivery, but increases drastically for women with HDP and comorbidities of hy-perlipidemia and obesity. Moreover, older pregnant women with HDP may have a much higher risk of subsequent diabetes than younger pregnant women with HDP. Close surveillance for diabetes should be considered for women with HDP, particularly for those with a history of pre-eclampsia/eclampsia. Lifestyle or pharmacological inter-ventions also should be considered for these high-risk women.
ACKNOWLEDGMENT
This study used insurance claims data obtained from Tai-wan National Health Research Institute.
References
1. Helewa ME, Burrows RF, Smith J, Williams K, Brain P, Rabkin SW. Report of the Canadian Hypertension Society Consensus Conference: 1. Definitions, evaluation and classification of hypertensive disorders in pregnancy. CMAJ. 1997;157(6):715-725.
2. Saftlas AF, Olson DR, Franks AL, Atrash HK, Pokras R. Epidemiol-ogy of preeclampsia and eclampsia in the United States, 1979-1986.
Am J Obstet Gynecol. 1990;163(2):460-465.
3. Saudan P, Brown MA, Buddle ML, Jones M. Does gestational hyper-tension become pre-eclampsia? Br J Obstet Gynaecol. 1998;105(11): 1177-1184.
4. Hauth JC, Ewell MG, Levine RJ, et al. Pregnancy outcomes in healthy nulliparas who developed hypertension. Calcium for Preeclampsia Prevention Study Group. Obstet Gynecol. 2000;95(1):24-28. 5. Bellamy L, Casas JP, Hingorani AD, Williams DJ. Pre-eclampsia and
risk of cardiovascular disease and cancer in later life: systematic review and meta-analysis. BMJ. 2007;335(7627):974.
Table 5 Interaction between HDP and Preterm Delivery Associated with Diabetes in Cox Regression Analysis Controlling for Sociodemographic Factors and Other Comorbidities
Variables
n DM PY Incidence*
Model 1 Model 2
HDP Obesity Hyperlipidemia HR (95% CI) HR (95% CI)
No No No 4180 14 34,240 0.41 1 (Reference) 1 (Reference) No Yes No 40 0 341 0.00 – – No No Yes 354 14 2992 4.68 11.2 (5.31-23.4) 10.1 (4.78-21.2) No Yes Yes 17 3 148 20.2 46.4 (13.3-161.5) 40.9 (11.7-142.6) Yes No No 946 12 795 1.58 3.90 (1.81-8.44) 3.94 (1.82-8.51) Yes Yes No 27 1 221 4.52 11.0 (1.44-83.3) 12.6 (1.66-96.3) Yes No Yes 155 22 1306 16.8 39.5 (20.2-77.3) 33.0 (16.7-65.1)
Yes Yes Yes 27 4 218 18.3 44.9 (14.8-136.3) 39.5 (13.0-120.6)
CI⫽ confidence interval; DM ⫽ diabetes mellitus; HDP ⫽ hypertensive disorders in pregnancy; HR ⫽ hazard ratio; PY ⫽ person-years. Model 1: Unad-justed; Model 2: Adjusted for age, occupation.
6. Lykke JA, Langhoff-Roos J, Sibai BM, Funai EF, Triche EW, Paidas MJ. Hypertensive pregnancy disorders and subsequent cardiovascular morbidity and type 2 diabetes mellitus in the mother. Hypertension. 2009;53(6):944-951.
7. McDonald SD, Malinowski A, Zhou Q, Yusuf S, Devereaux PJ. Cardiovascular sequelae of preeclampsia/eclampsia: a systematic re-view and meta-analyses. Am Heart J. 2008;156(5):918-930. 8. Kaaja R. Insulin resistance syndrome in preeclampsia. Semin Reprod
Endocrinol. 1998;16(1):41-46.
9. Parretti E, Lapolla A, Dalfra M, et al. Preeclampsia in lean normoten-sive normotolerant pregnant women can be predicted by simple insulin sensitivity indexes. Hypertension. 2006;47(3):449-453.
10. Sibai BM, Gordon T, Thom E, et al. Risk factors for preeclampsia in healthy nulliparous women: a prospective multicenter study. The Na-tional Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. Am J Obstet Gynecol. 1995;172(2 Pt 1):642-648.
11. Solomon CG, Graves SW, Greene MF, Seely EW. Glucose intolerance as a predictor of hypertension in pregnancy. Hypertension. 1994;23(6 Pt 1):717-721.
12. Wolf M, Sandler L, Munoz K, Hsu K, Ecker JL, Thadhani R. First trimester insulin resistance and subsequent preeclampsia: a prospective study. J Clin Endocrinol Metab. 2002;87(4):1563-1568.
13. Kaaja R, Laivuori H, Laakso M, Tikkanen MJ, Ylikorkala O. Evidence of a state of increased insulin resistance in preeclampsia. Metabolism. 1999;48(7):892-896.
14. Girouard J, Giguere Y, Moutquin JM, Forest JC. Previous hyperten-sive disease of pregnancy is associated with alterations of markers of insulin resistance. Hypertension. 2007;49(5):1056-1062.
15. Laivuori H, Tikkanen MJ, Ylikorkala O. Hyperinsulinemia 17 years after preeclamptic first pregnancy. J Clin Endocrinol Metab. 1996; 81(8):2908-2911.
16. Pouta A, Hartikainen AL, Sovio U, et al. Manifestations of metabolic syndrome after hypertensive pregnancy. Hypertension. 2004;43(4): 825-831.
17. Callaway LK, Lawlor DA, O’Callaghan M, Williams GM, Najman JM, McIntyre HD. Diabetes mellitus in the 21 years after a pregnancy that was complicated by hypertension: findings from a prospective cohort study. Am J Obstet Gynecol. 2007;197(5):492 e491-e497. 18. Carr DB, Newton KM, Utzschneider KM, et al. Preeclampsia and risk
of developing subsequent diabetes. Hypertens Pregnancy. 2009;28(4): 435-447.
19. Libby G, Murphy DJ, McEwan NF, et al. Pre-eclampsia and the later development of type 2 diabetes in mothers and their children: an intergenerational study from the Walker cohort. Diabetologia. 2007; 50(3):523-530.
20. Lu JF, Hsiao WC. Does universal health insurance make health care unaffordable? Lessons from Taiwan. Health Aff (Millwood). 2003; 22(3):77-88.
21. Granger JP, Alexander BT, Bennett WA, Khalil RA. Pathophysiology of pregnancy-induced hypertension. Am J Hypertens. 2001;14(6 Pt 2):178S-185S.
22. Levine RJ, Maynard SE, Qian C, et al. Circulating angiogenic factors and the risk of preeclampsia. N Engl J Med. 2004;350(7): 672-683.
23. Roberts JM, Cooper DW. Pathogenesis and genetics of pre-eclampsia.
Lancet. 2001;357(9249):53-56.
24. Ness RB, Sibai BM. Shared and disparate components of the patho-physiologies of fetal growth restriction and preeclampsia. Am J Obstet
Gynecol. 2006;195(1):40-49.
25. Dane B, Dane C, Kiray M, Koldas M, Cetin A. A new metabolic scoring system for analyzing the risk of hypertensive disorders of pregnancy. Arch Gynecol Obstet. 2009;280(6):921-924.