Psychiatry and Clinical Neurosciences (2006), 60, 700–708 doi:10.1111/j.1440-1819.2006.01585.x
Correspondence address: Chia-Yih Liu, MD, Department of Psychi-atry, Chang Gung Memorial Hospital, 5 Fu-Shing St, Kweishan, Taoyuan 333, Taiwan. Email: Liucy752@cgmh.org.tw
Received 26 January 2006; revised 8 May 2006; accepted 21 May 2006.
Regular Article
Depression and somatic symptoms scale: A new scale
with both depression and somatic symptoms emphasized
CHING-I HUNG, md,1 LI-JEN WENG, phd,2 YI-JEN SU, ms2 AND CHIA-YIH LIU, md1
1Department of Psychiatry, Chang Gung Memorial Hospital and Chang Gung University College of Medicine,
Taoyuan and 2Department of Psychology, National Taiwan University, Taipei, Taiwan
Abstract The authors’ preliminary study selected 22 items for Depression and Somatic Symptoms Scale
(DSSS), including depression subscale (DS) and somatic subscale (SS). The aim of the study was to test reliability and validity of the DSSS. The study enrolled 135 consecutive outpatients (34 male and 101 female) experiencing a major depressive episode (the MDE group), 95 of whom (25 male and 70 female) accepted 1 month of treatment (the treatment group). Diagnosis was confirmed by using the Structured Clinical Interview for 4th edition with text revision Diagnostic and Statistical
Manual Axis I Disorders. The DSSS and Hamilton Depression Rating Scale (HAMD) were given and evaluated. Cronbach’s alpha was used to assess internal consistency. The correlation between the improvement percentage (IP) for the HAMD and the IP for the DSSS was calculated for the treatment group. Factor analysis was performed by using the principal-axis factoring method with promax rotation. Cronbach’s alpha values of the DSSS and its subscales ranged from 0.73 to 0.94. Pearson correlation coefficients for the relationship between the DSSS and HAMD ranged from 0.63 to 0.86. In the treatment group, DSSS and HAMD scores were significantly decreased after treatment and the IP for the HAMD and the DSSS were similar and correlated (correlation coefficient = 0.78). The results of the factor analysis demonstrated that most of the items in DS and SS appropriately loaded in Depression and Somatic factors, respectively. The discriminative ability of the DSSS for anxiety comorbidities was not inferior to that of the HAMD. Therefore, the DSSS is reliable and sensitive to the treatment and has acceptable convergent, factorial, and distinct-groups validities. Because it assesses both depression and somatic symptoms, DSSS may overcome the deficiency of other depression scales with few somatic items.
Key words anxiety, depression, psychometrics, questionnaire.
INTRODUCTION
Somatic symptoms among patients with depression are important for several reasons. First, somatic symptoms
may confound or mask the diagnosis of depression.1
Second, residual symptoms, which are often somatic
symptoms, might increase the risk of relapse.2–4
Patients with major affective disorder and somatiza-tion had more and longer depressive episodes as well
as more depressive symptoms than patients without somatization.5 Increased pain severity in patients with
major depressive disorder (MDD) was associated with worse depression, poor health-related quality of life (HRQoL), and a negative impact on treatment response of depression.6 Finally, pain or somatic
symp-toms in depression increase the economic burden of depression.7 Therefore, somatic symptoms have a
sig-nificantly negative impact on diagnosis, treatment, and prognosis of depression.3
Fava reported that the conventional scales for depression used in clinical trials rarely included significant data on somatic symptoms.3,8 It had also
failed to bring the somatic aspect of depression to a level of attention and assessment equal to that of
the psychological symptoms.3,8 For example, the
Hamilton Depression Rating Scale (HAMD) and the Montgomery–Asberg Depression Rating Scale (MADRS) are the most common scales used to evalu-ate depression.9–11 Although the 17-item HAMD scale
contains eight items pertaining to somatic symptoms, six of the eight items are designed to identify vegeta-tive symptoms, including insomnia, loss of appetite, loss of bodyweight, and decreased libido. Other somatic symptoms – for example, fatigue, chest tight-ness, palpitations, headache, muscle soretight-ness, and other types of pain – are coded for by only two items, thereby accounting for only six points, or 11.5% of the total score.3,8 The fact that the codes for several somatic
symptoms are limited to two items makes it almost impossible to track specific somatic symptoms and dimension. Among the 10 items for the MADRS scale, there are only two items for the vegetative symptoms (decreased appetite and insomnia) and none for other somatic symptoms. However, scales for depression without relevant somatic symptoms are problematic for researchers in the field of depression. Studies of somatic issues in depression must use other tools to measure somatic severity, such as the visual analog
scale, the 90-item Hopkins Symptom Checklist,12
Patient Health Questionnaire,13 or HRQoL scale.14
However, these scales are not specifically designed for depression and the question remains as to whether the somatic symptoms in these scales can be used to accurately assess somatic severities in patients with depression.
The authors’ previous studies investigated the impact of headache on HRQoL and three psychomet-ric scales among patients with MDD.15–17 The authors
found that the difference in depressive severity between MDD patients with and without migraine was partially due to somatic severity. However, no depres-sion scale emphasizing somatic symptoms was avail-able to further explore this difference. One study reported that adding HRQoL subscales for physical and social activity could improve the accuracy of predicting acute treatment response.18 Therefore, a
depression scale that emphasizes somatic symptoms is worth developing. In fact, the demand for such a scale becomes more necessary and urgent because somatic symptoms have a great impact on the prognosis of depression4–6 and new antidepressants also stress their
effect in this area.1
Initially, 102 patients with MDD were enrolled to determine which items should be included in the
Depression and Somatic Symptoms Scale (DSSS).19 A
total of 44 items were used in the preliminary DSSS, including 16 depression items and 28 somatic items, the latter included seven pain-related items. The
prelimi-nary items for depression subscale were modifications of the 4th edition Diagnostic and Statistical Manual (DSM-IV) criteria for MDE, HAMD or MADRS scale items.9,10,20 The preliminary items for somatic subscale
were selected from several sources, including the
HAMD scale,10 the 90-item Hopkins Symptom
Check-list,12 and the common somatic symptoms for MDD
reported in the previous studies.21–25 In selecting
appro-priate items for the DSSS, several principles were con-sidered: (i) somatic items that could reflect the severity of depression or predict the occurrence of depression, or the ones with significant impact on clinical practice or HRQoL;1,21–26 (ii) somatic symptoms that were
com-mon in the present study and previous studies for depression; and (iii) somatic symptoms that improve Cronbach’s alpha value for DSSS. The final DSSS was composed of 22 items with two major subscales, the depression subscale (DS) and the somatic subscale (SS). The DS had 12 items, including three vegetative symptoms and fatigue, and the SS had 10 items, includ-ing five pain items, which comprised the pain subscale (PS). Three vegetative symptoms (insomnia, poor appetite, and loss of interest in sex) and fatigue were included in DS but not in SS because three of the four symptoms were criteria for MDE and the four symp-toms were also included in the HAMD scale. This design made DS more compatible with MDE criteria, HAMD, and other scales for depression. The prelimi-nary results showed that the DSSS and HAMD were significantly correlated, and the Cronbach’s alpha of the DSSS and all subscales fell within an acceptable range. The form of the DSSS is shown in Appendix I. The DS items were even-numbered plus item 21 (fatigue) and the SS items were odd-numbered except for item 21. The purpose of this study was to describe the psychometric characteristics of the DSSS by assess-ing reliability (by evaluatassess-ing the Cronbach’s alpha and test–retest reliability) and validity (by testing the cor-relation between DSSS and HAMD scores, their sen-sitivity to treatment, and correlation of improvement percentages [IP] between the DSSS and HAMD, fac-torial validity, and distinct-groups validity).
SUBJECTS AND METHODS
Four groups (major depressive episode [MDE] group, non-MDE group, treatment group, and test–retest group) were studied. Patients in the MDE group came from the project entitled ‘The impact of headache and somatic symptoms on MDD II’, which was conducted from January 2004 to January 2005 in the psychiatric outpatient clinics of Chang Gung Memorial Hospital, Taoyuan, Taiwan. This project was approved by the institutional review board of the Chang Gung
Memo-rial Hospital. Study participants were recruited from consecutive outpatients, 18–65 years of age, who had not received antidepressant or other psychotropic drug treatment within the past 2 weeks. Screening included an interview with a board-certified psychiatrist using the Structured Clinical Interview for DSM-IV-text revision (TR) Axis I Disorders.27 Patients who met the
DSM-IV-TR criteria for MDD20 and experienced a
MDE were enrolled. Seven anxiety comorbidities were diagnosed by using the Structured Clinical Interview.27
The course of depression was clarified. Chronic depres-sion was defined as chronic major depresdepres-sion for more than 2 years, dysthymic disorder plus current MDE, or previous MDE without full remission plus current MDE with a total course of more than 2 years.28
To minimize confounding of somatic symptoms by other medical conditions, substance abuse, or psychotic symptoms, the following exclusion criteria were estab-lished: (i) a history of substance dependence or abuse without full remission in the previous month; (ii) chotic symptoms, catatonic features, or severe psy-chomotor retardation with obvious difficulty being interviewed; and (iii) regular treatment with medica-tions for medical diseases, such as hypertension or dia-betes mellitus.
In enrolling the non-MDE group, the same exclusion and inclusion criteria, which were applied to the MDE group, were used except for fulfilling MDD in a MDE. Therefore, patients who were not in MDE were enrolled in the non-MDE group. The enrolment of consecutive subjects in the MDE and non-MDE groups started at the same time. Enrolment in the MDE group lasted 1 year and in the non-MDE group for 4 months. Written informed consent was obtained from all subjects prior to the study enrolment.
After subjects were enrolled, subjects were requested to finish the self-administrated DSSS. Psy-chiatrists, who were blind to the DSSS results and psy-chiatric diagnoses, evaluated the HAMD score. In calculating the DSSS score, ‘Absent’ was scored as 0 points, ‘Mild’ as 1 point, ‘Moderate’ as 2 points, and ‘Severe’ as 3 points. The total scores on the DSSS or its subscales were calculated by adding the appropriate item scores. The scores on the DSSS and its subscales and the HAMD between the MDE and non-MDE groups were also compared. Moreover, the correlation between the HAMD and the DSSS and its subscale scores were calculated for the different groups.
To understand the sensitivity of the DSSS to treat-ment and the correlation between degree of improve-ment in the DSSS and HAMD scores, the MDE patients were treated for 1 month by pharmacological
therapy. At 1 month later, DSSS was given and
HAMD was re-evaluated by the same psychiatrist.
Those who accepted the 1 -month follow-up treatment were considered to be in the treatment group. Scores on the DSSS and its subscales before and after treat-ment were compared to determine the test’s sensitivity to treatment. The IP for the DSSS and its subscales and the HAMD were also compared. The IP calculation was:
(scores before treatment – scores after treatment) × 100%/scores before treatment Moreover, the correlation between IP for the DSSS and its subscales and the HAMD was calculated.
The internal consistency of the DSSS and its sub-scales in the MDE, non-MDE, and the treatment groups were assessed by Cronbach’s alpha. To test the test–retest reliability of the DSSS, psychiatric outpa-tients were enrolled who met two criteria: (i) received treatment in the psychiatric clinic for depression for at least 3 months and were in a stable condition according to patients’ self-report and chart review; and (ii) did not expect change in medications or treatment profile in the following week. Subjects were given the DSSS at the index visit and 1 week later. Then, the Pearson cor-relation was calculated for the corcor-relation between scores on the DSSS in the index visit and scores obtained 1 week later.
The factor structure of DSSS was investigated in the MDE and non-MDE groups. The authors submitted the DSSS items to a principal-axis factor analysis with promax rotation. A two-factor solution appeared to be the best fit based on two considerations. First, in their initial hypothesis for designing DSSS, it was composed of two major subscales: DS and SS. Second, the scree test revealed the possibility of a two or three-factor solution.
To test the discriminative validity of DSSS, subjects in the MDE group were divided into the anxiety comorbidity subgroup and the nonanxiety comorbidity subgroup. The differences of scores between the two groups were compared. Authors selected to test the discriminative ability for anxiety comorbidities because the purpose of DSSS was to emphasize somatic symptoms, which were related to anxiety.
All statistical analyses were carried out using the Statistical Package for the Social Sciences for Win-dows 10.0 (SPSS Inc., Chicago, IL, USA). Pearson correlation was used in these situations: the correla-tion of the DSSS and its subscale scores with the HAMD scores, the correlation between the IP for the DSSS and its subscales and that for the HAMD, and test–retest reliability. Independent or paired t-test was used in appropriate situations. A P-value less than 0.05 was considered statistically significant in all of the tests.
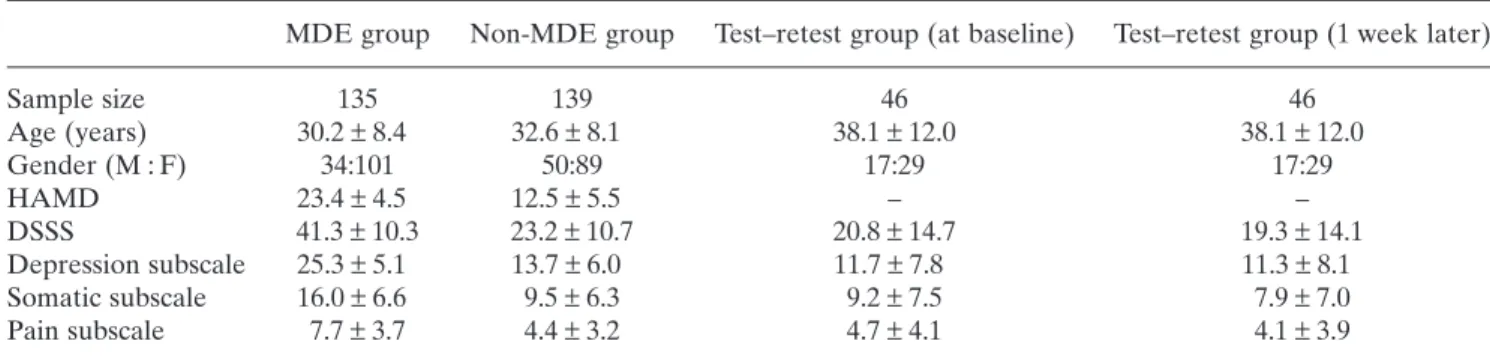
Table 1. Age, gender, and the scores on the Hamilton Depression Rating Scale and Depression and Somatic Symptoms Scale for the different groups†
MDE group Non-MDE group Test–retest group (at baseline) Test–retest group (1 week later)
Sample size 135 139 46 46 Age (years) 30.2 ± 8.4 32.6 ± 8.1 38.1 ± 12.0 38.1 ± 12.0 Gender (M : F) 34:101 50:89 17:29 17:29 HAMD 23.4 ± 4.5 12.5 ± 5.5 – – DSSS 41.3 ± 10.3 23.2 ± 10.7 20.8 ± 14.7 19.3 ± 14.1 Depression subscale 25.3 ± 5.1 13.7 ± 6.0 11.7 ± 7.8 11.3 ± 8.1 Somatic subscale 16.0 ± 6.6 9.5 ± 6.3 9.2 ± 7.5 7.9 ± 7.0 Pain subscale 7.7 ± 3.7 4.4 ± 3.2 4.7 ± 4.1 4.1 ± 3.9
† Differences in the mean scores on the HAMD and DSSS and subscales between the MDE group and non-MDE group were
significant (P < 0.01).
DSSS, Depression and Somatic Symptoms Scale; HAMD, Hamilton Depression Rating Scale; MDE group, subjects with major depressive disorder currently in a major depressive episode; non-MDE group, subjects not in a major depressive episode.
RESULTS
Sample characteristics and scores in different groups
The sample size, mean age, mean scores on the HAMD and the DSSS and its subscales among different groups are shown in Table 1. The MDE group’s scores on the DSSS and its subscales and the HAMD were signifi-cantly different from the non-MDE group’s scores (P < 0.01).
Among the 135 subjects in the MDE group, 95 (70.4%; 25 men and 70 women; mean age,
31.3 ± 8.2 years) completed the required 1 -month
follow-up visit and, therefore, were considered as the treatment group. The HAMD scores at baseline
(23.8 ± 4.9) in 40 subjects (29.6%) who dropped out
were not significantly different from those of the treatment group (23.3 ± 4.4). The coefficient of vari-ance (standard deviation/mean) of the HAMD scores in the treatment group (at the 1 month follow-up point) was higher than in the MDE group (at base-line; 0.55 vs. 0.19). Therefore, the HAMD scores in the MDE group were more homogeneous, compared to those in the treatment group after the 1-month treatment.
Internal consistency reliability
The Cronbach’s alpha values for the different groups are shown in Table 2. All Cronbach’s alpha values of the DSSS and SS for the three groups were >0.8 and the Cronbach’s alpha values of the DS and PS were in an acceptable range (>0.7). Of the groups, the treatment group had a higher Cronbach’s alpha value.
Test–retest reliability
The scores of DSSS at the index visit and 1 week later are shown in Table 1. The difference in DSSS scores between the two evaluations was not significant as indi-cated by the paired t-test. The Pearson correlation coefficients calculated between the DSSS scores at the index visit and 1 week later were as follows: DSSS, 0.92; DS, 0.88; SS, 0.90; and PS, 0.90 (all P < 0.01).
Convergent validity and sensitivity to treatment
The correlation between the scores on the HAMD and DSSS are shown in Table 3. The scores on the DSSS
Table 2. The Cronbach’s alpha of the Depression and Somatic Symptoms Scale and its subscales†
MDE group Non-MDE group Treatment group DSSS 0.87 0.88 0.94 Depression subscale 0.73 0.79 0.90 Somatic subscale 0.88 0.88 0.90 Pain subscale 0.82 0.77 0.85
† The Cronbach’s alpha values in the MDE and the
non-MDE groups were obtained at baseline and the results in the treatment group were obtained at the 1-month follow-up point.
DSSS, Depression and Somatic Symptoms Scale; MDE group (n = 135), subjects with major depressive disorder currently in a major depressive episode; non-MDE group (n = 139), subjects not in a major depressive episode; Treatment group (n = 95), subjects in MDE group who accepted 1 month of treatment.
and its subscales were significantly correlated with those on the HAMD. Among the three groups, the cor-relation between the scores on the HAMD and DSSS was higher for the treatment group than for the MDE or non-MDE groups. Among DSSS subscales, DS score was best correlated with HAMD score.
The scores on the different scales before and after treatment are shown in Table 4. The scores on the HAMD and DSSS decreased significantly post treat-ment (all P-values <0.01). The IP of the HAMD, DSSS, and DS were similar. The difference in IP between the
HAMD and DSSS (P = 0.31), the HAMD and DS
(P = 0.51), the HAMD and SS (P = 0.14), the HAMD
and PS (P = 0.11), the DS and SS (P = 0.18), and the
DS and PS (P = 0.16) was not significant. Moreover,
the IP of the DSSS and its subscales were significantly correlated with that of the HAMD. The IP of the DS was most correlated with that of the HAMD (correla-tion coefficient = 0.81).
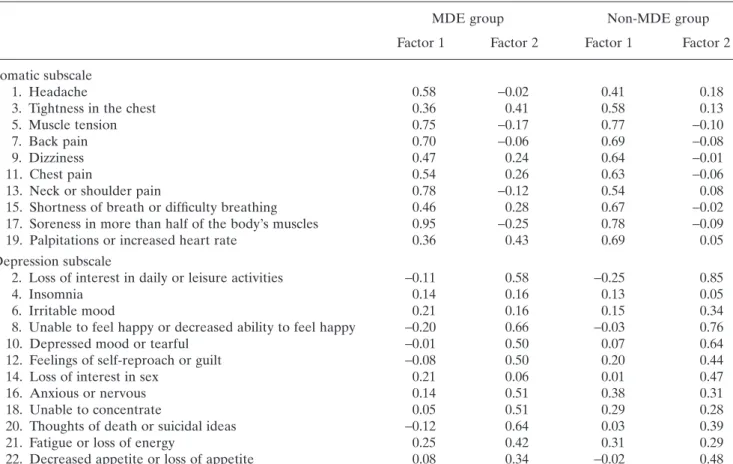
Factorial validity
The results of factor analysis were presented in Table 5. Factors 1 and 2 appeared to be the Somatic factor and the Depression factor, respectively. In the MDE group, eight items in the SS loaded substantially on Factor 1. Although tightness in the chest and palpitation loaded on both factors, all items in the SS had a factor loading >0.35 on Factor 1. Nine items in the DS loaded on Fac-tor 2 with a facFac-tor loading >0.3. Insomnia, loss of inter-est in sex, and irritable mood did not appropriately load on both factors.
In the non-MDE group, Factor 1 included all items in the SS with a factor loading >0.4. All items in the DS except for ‘unable to concentrate’, ‘insomnia’, and ‘fatigue’ had a factor loading >0.3 in Factor 2. Three items in the DS, ‘anxious’, ‘unable to concentrate’, and ‘fatigue’ tended to load on both factors.
The two factors were moderately correlated (corre-lation coefficient = 0.51 in the MDE group and 0.45 in the non-MDE group). The two-factor solution accounted for 34.1% of the variance in the MDE group and 35.5% of that in the non-MDE group.
Table 3. The Pearson correlation coefficients of the Hamil-ton Depression Rating Scale and Depression and Somatic Symptoms Scale†‡ MDE group Non-MDE group Treatment group HAMD – DSSS 0.63 0.66 0.86 HAMD – DS 0.65 0.68 0.84 HAMD – SS 0.49 0.48 0.78 HAMD – PS 0.39 0.50 0.71 DSSS – DS 0.84 0.87 0.95 DSSS – SS 0.91 0.88 0.93 DSSS – PS 0.82 0.81 0.87 DS – SS 0.54 0.52 0.77 DS – PS 0.45 0.49 0.72 SS – PS 0.93 0.91 0.93
† The Pearson correlation coefficients in the MDE and the
non-MDE groups were obtained at baseline and the results in the treatment group were obtained at the 1-month follow-up point.
‡ All these correlations were statistically significant
(P < 0.01).
DS, Depression Subscale; DSSS, Depression and Somatic Symptoms Scale; HAMD, Hamilton Depression Rating Scale; MDE group (n = 135), subjects with major depressive disorder currently in a major depressive episode; non-MDE group (n = 139), subjects not in a major depressive episode; PS, Pain Subscale; SS, Somatic Subscale; Treatment group (n = 95), subjects in MDE group who accepted one month of treatment.
Table 4. The improvement percentage for all scales and the Pearson correlation coefficients between improvement percentages for the Hamilton Depression Rating Scale and Depression and Somatic Symptoms Scale in the treatment group (n = 95)
Scores before treatment Scores post treatment† IP (%)‡ Correlation coefficients§
HAMD 23.3 ± 4.4 12.8 ± 7.1 44.9 ± 29.3 –
DSSS 41.6 ± 10.1 23.5 ± 13.2 42.6 ± 35.9 0.78
Depression subscale 25.2 ± 5.2 13.9 ± 7.6 43.5 ± 34.6 0.81
Somatic subscale 16.4 ± 6.0 9.6 ± 6.4 39.3 ± 46.6 0.61
Pain subscale 7.9 ± 3.5 4.9 ± 3.5 37.2 ± 52.0 0.51
† Scores post treatment decreased significantly for all scales and subscales (P < 0.01).
‡ The IP was calculated as follows: (scores before treatment – scores after treatment) × 100%/scores before treatment. § The Pearson correlations between the IP for the HAMD and DSSS were significant (P < 0.01).
Distinct-groups validity
The percentage and score of anxiety comorbidities and chronic depression are shown in Table 6. Chronic depression and all anxiety comorbidities except for generalized anxiety disorder (GAD) had higher scores on the HAMD and DSSS. Among seven anxiety comorbidities, significant differences of scores between anxiety comorbidity subgroup versus non-anxiety comorbidity subgroup were noted in five anxiety comorbidities by using the DSSS. However, the HAMD only could differentiate the severity of three anxiety comorbidities. Significant differences of scores in the DS and SS also were noted in four anxiety comorbidities.
DISCUSSION
The scores on the DSSS and its subscales were signifi-cantly correlated with those on the HAMD. This cor-relation was less for the MDE group than the treatment group. This might be partially attributed to more homogeneity in severity of depression in the
MDE group (at baseline) than in the treatment group (at the 1 -month follow-up point) because subjects in the treatment group might have different degrees of improvement after the 1-month treatment. Among the DSSS subscales, DS was most correlated with the HAMD. This result was compatible with the design of the DSSS because the items in the DS were modified items from the HAMD and based on DSM-IV criteria for MDE.
The scores on the DSSS and its subscales signifi-cantly decreased after treatment. The IP for the HAMD and DSSS were similar and significantly cor-related (Table 4). These results demonstrated that the DSSS was sensitive to treatment, and its validity as a tool to monitor the severity of depression during treat-ment was good.
The Cronbach’s alpha values for the DSSS and SS were good (>0.8) and those for the DS and PS were acceptable (>0.7). The test–retest reliability of scores on the DSSS at baseline was also highly correlated with scores 1 week later, indicating that the reliability of the DSSS was acceptable.
Table 5. Factor analysis of Depression and Somatic Symptoms Scale by using the principal-axis factoring method with promax rotation
MDE group Non-MDE group
Factor 1 Factor 2 Factor 1 Factor 2
Somatic subscale
1. Headache 0.58 −0.02 0.41 0.18
3. Tightness in the chest 0.36 0.41 0.58 0.13
5. Muscle tension 0.75 −0.17 0.77 −0.10
7. Back pain 0.70 −0.06 0.69 −0.08
9. Dizziness 0.47 0.24 0.64 −0.01
11. Chest pain 0.54 0.26 0.63 −0.06
13. Neck or shoulder pain 0.78 −0.12 0.54 0.08
15. Shortness of breath or difficulty breathing 0.46 0.28 0.67 −0.02
17. Soreness in more than half of the body’s muscles 0.95 −0.25 0.78 −0.09
19. Palpitations or increased heart rate 0.36 0.43 0.69 0.05
Depression subscale
2. Loss of interest in daily or leisure activities −0.11 0.58 −0.25 0.85
4. Insomnia 0.14 0.16 0.13 0.05
6. Irritable mood 0.21 0.16 0.15 0.34
8. Unable to feel happy or decreased ability to feel happy −0.20 0.66 −0.03 0.76
10. Depressed mood or tearful −0.01 0.50 0.07 0.64
12. Feelings of self-reproach or guilt −0.08 0.50 0.20 0.44
14. Loss of interest in sex 0.21 0.06 0.01 0.47
16. Anxious or nervous 0.14 0.51 0.38 0.31
18. Unable to concentrate 0.05 0.51 0.29 0.28
20. Thoughts of death or suicidal ideas −0.12 0.64 0.03 0.39
21. Fatigue or loss of energy 0.25 0.42 0.31 0.29
22. Decreased appetite or loss of appetite 0.08 0.34 −0.02 0.48
MDE group (n = 135), subjects with major depressive disorder currently in a major depressive episode; non-MDE group (n = 139), subjects not in a major depressive episode.
In the factor analysis, most of the items in the DS and SS loaded on the Depression factor and the Somatic factor, respectively. Insomnia, loss of interest in sex, and irritable mood in the MDE group did not appropriately load on both factors. However, the three symptoms were common depressive symptoms in MDE and also included in some scales for depression,
such as the HAMD and Zung Depression scale.10,29
Therefore, the Depression and Somatic factor reflected the common depressive and somatic symptoms among patients with a MDE, respectively.
The discriminative ability of the DSSS was not infe-rior to that of the HAMD. This might partially result from the fact that the DSSS had more somatic compo-nents. All anxiety comorbidities had higher scores of the HAMD or DSSS except for GAD. Subjects during MDE with the symptoms of GAD were not diagnosed as GAD according to the hierarchy rule of DSM-IV-TR.20 Therefore, only patients with a short duration of
MDE, which had less severity compared with chronic
depression (Table 6), had an opportunity to fulfil a diagnosis of GAD in the present study. Moreover, near half of the present study’s subjects (45.9%) had chronic depression. These two circumstances might partially explain the lower frequency of GAD (3.7%) and MDD with GAD having a less depressive severity in the present study.
Lack of somatic items in depressive scales might lead to underestimate the impact of somatic symptoms on depression and HRQoL and fail to monitor somatic dimension. The DSSS emphasized depression and somatic symptoms simultaneously and had several advantages. First, the design of the DSSS enables the researcher to observe and monitor different dimen-sions of depression during treatment. Second, each item of the DSSS deals with only one symptom. There-fore, the DSSS could be used as a symptom-checklist for depression. This design facilitates monitoring of individual somatic symptoms during treatment. Third, the discriminative ability of the DSSS for anxiety
Table 6. The scores (mean ± standard deviation) of the Hamilton Depression Rating Scale and the Depression and Somatic Symptoms Scale between the comorbid group versus the non-comorbid group among 135 subjects with major depressive disorder† HAMD DSSS DS SS PS Chronic depression Yes (n = 62; 45.9%) 24.5 ± 4.5** 44.4 ± 9.3** 26.2 ± 4.7 18.2 ± 5.9** 8.8 ± 3.5** No (n = 73) 22.5 ± 4.4 38.8 ± 10.5 24.6 ± 5.3 14.2 ± 6.6 6.8 ± 3.7 Panic disorder Yes (n = 24; 17.8%) 26.2 ± 4.2** 47.2 ± 10.0** 28.0 ± 4.5** 19.2 ± 6.4** 9.1 ± 3.9* No (n = 111) 22.7 ± 4.3 40.1 ± 10.0 24.8 ± 5.1 15.3 ± 6.4 7.4 ± 3.7 Agoraphobia Yes (n = 22; 16.3%) 26.5 ± 3.9** 47.6 ± 7.7** 27.5 ± 4.1* 20.1 ± 4.9** 9.6 ± 3.3** No (n = 113) 22.8 ± 4.4 40.1 ± 10.3 24.9 ± 5.2 15.2 ± 6.6 7.3 ± 3.7 Social phobia Yes (n = 42; 31.1%) 24.5 ± 4.3 44.1 ± 10.3* 26.5 ± 5.5 17.6 ± 6.0 8.6 ± 3.6 No (n = 93) 22.9 ± 4.6 40.1 ± 10.1 24.8 ± 4.8 15.3 ± 6.7 7.3 ± 3.7 Specific phobia Yes (n = 36; 26.7%) 24.8 ± 4.2* 46.1 ± 9.1** 27.3 ± 4.9** 18.8 ± 5.5** 9.1 ± 3.1** No (n = 99) 22.9 ± 4.6 39.6 ± 10.2 24.6 ± 5.0 15.0 ± 6.7 7.2 ± 3.8
Post-traumatic stress disorder
Yes (n = 13; 9.6%) 25.4 ± 3.5 46.2 ± 10.2 27.4 ± 4.1 18.8 ± 7.7 9.2 ± 4.3
No (n = 122) 23.2 ± 4.6 40.8 ± 10.2 25.1 ± 5.2 15.7 ± 6.4 7.5 ± 3.7
Obsessive–compulsive disorder
Yes (n = 17; 12.6%) 25.0 ± 5.0 47.8 ± 9.8** 28.2 ± 4.2* 19.6 ± 6.8* 9.4 ± 4.2
No (n = 118) 23.2 ± 4.5 40.4 ± 10.1 24.9 ± 5.1 15.5 ± 6.4 7.4 ± 3.6
Generalized anxiety disorder
Yes (n = 5; 3.7%) 22.6 ± 6.6 36.2 ± 16.2 21.4 ± 9.2 14.8 ± 7.2 8.0 ± 3.7
No (n = 130) 23.5 ± 4.5 41.5 ± 10.0 25.5 ± 4.9 16.1 ± 6.6 7.7 ± 3.8
† The difference between groups was compared by the independent t-test (* P < 0.05; ** P < 0.01).
DS, Depression Subscale; DSSS, Depression and Somatic Symptoms Scale; HAMD, Hamilton Depression Rating Scale; PS, Pain Subscale; SS, Somatic Subscale.
comorbidities was not inferior to that of the HAMD. Finally, the DSSS is a simple and self-administrated scale with only 281 words in the Chinese version.
Some methodological issues or limitations should be addressed. First, the DSSS was compared with the HAMD because the HAMD is one of the most popular scales used in evaluating the severity of depression.11
Second, the test–retest reliability of two scores 1 week apart, which is a short interval, was selected because the DSSS was sensitive to treatment and the severity of depression might change after a longer period. Third, this study focused on the HAMD to test the validity of the DSSS. Other methods to test validity of the DSSS were indicated, such as comparing the SS to other somatic scales and the correlation of the DSSS and scales for HRQoL. Moreover, interpretations, limita-tions, or cultural differences associated with the DSSS might need to be further studied.
In conclusion, the results of the present study dem-onstrate that the DSSS and its subscales are reliable and sensitive to the treatment and have acceptable convergent validity, factorial validity, and distinct-groups validity. The DSSS is able to assess both depres-sion and somatic symptoms and may overcome the deficiency of other scales for depression that include few somatic symptoms. Therefore, DSSS could serve as an instrument to monitor the severity of depression and somatic symptoms.
ACKNOWLEDGMENT
This study was supported in part by National Science Council grants (NSC 93-2314-B-182A-200 and NSC 94-2314-B-182A-207).
REFERENCES
1. Greden JF. Physical symptoms of depression: unmet needs. J. Clin. Psychiatry 2003; 64 (Suppl. 7): 5–11. 2. Bakish D. New standard of depression treatment:
remis-sion and full recovery. J. Clin. Psychiatry 2001; 62 (Suppl. 26): 5–9.
3. Fava M. Depression with physical symptoms: treating to remission. J. Clin. Psychiatry 2003; 64 (Suppl. 7): 24– 28.
4. Paykel ES, Ramana R, Cooper Z, Hayhurst H, Kerr J, Barocka A. Residual symptoms after partial remission: an important outcome in depression. Psychol. Med. 1995; 25: 1171–1180.
5. Lipowski ZJ. Somatization and depression. Psychoso-matics 1990; 31: 13–21.
6. Bair MJ, Robinson RL, Eckert GJ, Stang PE, Croghan TW, Kroenke K. Impact of pain on depression treatment response in primary care. Psychosom. Med. 2004; 66: 17– 22.
7. Greenberg PE, Leong SA, Birnbaum HG, Robinson RL. The economic burden of depression with painful symp-toms. J. Clin. Psychiatry 2003; 64 (Suppl. 7): 17–23. 8. Fava M. Somatic symptoms, depression, and
antidepres-sant treatment (commentary). J. Clin. Psychiatry 2002; 63: 305–307.
9. Montgomery SA, Asberg M. A new scale designed to be sensitive to change. Br. J. Psychiatry 1979; 134: 382– 389.
10. Hamilton M. Development of a rating scale for primary depressive illness. Br. J. Soc. Clin. Psychol. 1967; 6: 278– 296.
11. Demyttenaere K, De Fruyt J. Getting what you ask for: on the selectivity of depression rating scales. Psychother. Psychosom. 2003; 72: 61–70.
12. Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L. The Hopkins symptom checklist (HSCL): a self-report symptom inventory. Behav. Sci. 1974; 19: 1–15. 13. Kroenke K, Spitzer RL, Williams JB. The PHQ-15:
validity of a new measure for evaluating the severity of somatic symptoms. Psychosom. Med. 2002; 64: 258–266. 14. Ware JE, Snow KK, Kosinski M, Gandek B. SF-36
Health Survey-Manual and Interpretation Guide. The Health Institute, New England Medical Center, Boston, MA, 1993.
15. Hung CI, Wang SJ, Hsu KH, Juang YY, Liu CY. Risk factors associated with migraine or chronic daily head-ache in outpatients with major depressive disorder. Acta Psychiatr. Scand. 2005; 111: 310–315.
16. Hung CI, Liu CY, Fuh JL, Juang YY, Wang SJ. Comor-bid migraine is associated with a negative impact on qual-ity of life in patients with major depression. Cephalalgia 2006; 26: 26–32.
17. Hung CI, Liu CY, Juang YY, Wang SJ. The impact of migraine on patients with major depressive disorder. Headache 2006; 46: 469–477.
18. Pyne JM, Bullock D, Kaplan RM et al. Health-related quality-of-life measure enhances acute treatment response prediction in depressed inpatients. J. Clin. Psy-chiatry 2001; 62: 261–268.
19. Hung CI, Weng LJ, Su YJ, Liu CY. Preliminary study of a scale measuring depression and somatic symptoms. Psychological reports 2006; 99: 379–389.
20. American Psychiatric Association. Diagnostic and Statis-tical Manual of Mental Disorders, 4th edn, Text Revision. American Psychiatric Association, Washington, DC, 2000.
21. Von Korff M, Resche LL, Dworkin SF. First onset of common pain symptoms: a prospective study of depres-sion as a risk of factor. Pain 1993; 55: 251–258.
22. Von Knorring L, Perris C, Eisemann M, Eriksson U, Perris H. Pain as a symptom in depressive disorder. I. Relationship to diagnostic subgroup and depressive symptomatology. Pain 1983; 15: 19–26.
23. Mathew RJ, Weinman ML, Mirabi M. Physical symp-toms of depression. Br. J. Psychiatry 1981; 139: 293–296. 24. De Wester JN. Recognizing and treating the patient with somatic manifestations of depression. J. Fam. Pract. 1996; 43: S3–S15.
25. Gerber PD, Barrett JE, Barrett JA et al. The relationship of presenting physical complaints to depressive symp-toms in primary care patients. J. Gen. Intern. Med. 1992; 7: 170–173.
26. Wang SJ, Fuh JL, Lu SR, Juang KD. Quality of life dif-fers among headache diagnoses: analysis of SF-36 survey in 901 headache patients. Pain 2001; 89: 285–292. 27. First MB, Spitzer RL, Gibbon M, Williams JBW.
Struc-tured Clinical Interview for DSM-IV-TR Axis I Disorders,
Research Version. Patient Edition (SCID-I/P). New York State Psychiatric Institute, Biometrics Research, New York, 2002.
28. Dunner DL. Acute and maintenance treatment of chronic depression. J. Clin. Psychiatry 2001; 62 (Suppl. 6): 10–16.
29. Zung WWK. A self-rating depression scale. Arch. Gen. Psychiatry 1965; 12: 63–70.
APPENDIX I
Depression and somatic symptoms scale
Date: __/__/__ Please evaluate the severity of these symptoms you have experienced in the past week (7 days):
Absent: no symptoms.
Mild: symptoms caused slight discomfort or disturbance.
Moderate: symptoms caused significant discomfort or disturbance. Severe: symptoms caused very significant discomfort or disturbance.
Please check one of absent, mild, moderate, or severe to indicate the severity of the following symptoms.
Absent Mild Moderate Severe
1. Headache
2. Loss of interest in daily or leisure activities 3. Tightness in the chest
4. Insomnia 5. Muscle tension 6. Irritable mood 7. Back pain
8. Unable to feel happy or decreased ability to feel happy 9. Dizziness
10. Depressed mood or tearful 11. Chest pain
12. Feelings of self-reproach or guilt 13. Neck or shoulder pain (or soreness) 14. Loss of interest in sex
15. Shortness of breath or difficulty breathing 16. Anxious or nervous
17. Soreness in more than half of the body’s muscles 18. Unable to concentrate
19. Palpitations or increased heart rate 20. Thoughts of death or suicidal ideas 21. Fatigue or loss of energy