Association of Caveolin-1 polymorphisms with colorectal cancer susceptibility in Taiwan
Running title: Yang MD et al. Cav-1 polymorphisms in colorectal cancer
Mei-Due Yang, Ru-Yin Tsai, Chiu-Shong Liu, Chao-Hsiang Chang, Hwei-Chung Wang, Yung-An Tsou,Chung-Hsing Wang, Cheng-Chieh Lin, Song-Kun Shyue,and Da-Tian Bau
Mei-Due Yang, Chao-Hsiang Chang, Hwei-Chung Wang, Department of Surgery, China Medical University Hospital, 2 Yuh-Der Road, Taichung, 404 Taiwan
Cheng-Chieh Lin, Chiu-Shong Liu, Department of Family Medicine, China Medical University Hospital, 2 Yuh-Der Road, Taichung, 404 Taiwan
Da-Tian Bau, Chung-Hsing Wang, Yung-An Tsou, Ru-Yin Tsai, Terry Fox Cancer Research Laboratory, China Medical University Hospital, 2 Yuh-Der Road, Taichung, 404 Taiwan
Song-Kun Shyue, Institute of Biomedical Sciences, Academia Sinica, 128 Academia Road, Section 2, Nankang, Taipei 115, Taiwan
Author contributions: Mei-Due Yang designed the research; Mei-Due Yang, Chiu-Shong Liu and Ru-Yin Tsai contributed equally to this work; Da-Tian Bau and Ru-Yin Tsai performed all measurements and evaluated the raw data; Yung-An Tsou and Chung-Hsing Wang performed the statistical analyses; Song-Kun Shyue selected and evaluated all cases, Chao-Hsiang Chang and Cheng-Chieh Lin wrote the manuscript with support from Mei-Due Yang. All authors approved the final manuscript.
Supportive foundations: This study was supported by research grants from the China Medical University and Hospital (DMR-99-041 and CMU-99-NTU-10), the Terry Fox Cancer Research Foundation and the National Science Council (NSC 98-2320-B-039-010-MY3).
Correspondence to: Da-Tian Bau, Terry Fox Cancer Research Laboratory, China Medical University Hospital, 2 Yuh-Der Road, Taichung, 404 Taiwan, R.O.C.
Abstract
AIM: To investigate the association of Cav-1 polymorphisms with colorectal cancer risk in a central Taiwanese population.
METHODS: Three hundred and sixty-two patients with colorectal cancer and same amount of age- and gender-matched healthy controls recruited were genotyped. RESULTS: There were significant differences between CRC and control groups in the distributions of their genotypes (P=1.6*10-12 and 3.0*10-4) and allelic frequencies (P=2.3*10-13 and 4.0*10-5) in the Cav-1 G14713A (rs3807987) and T29107A (rs7804372) polymorphisms, respectively. As for the haplotype analysis, those who had GG/AT or GG/AA at Cav-1 G14713A/T29107A showed a 0.68-fold (95% confidence interval=0.48-0.98) decreased risk of CRC compared to those with GG/TT, while those of any other combinations were of increased risk. There were joint effects of Cav-1 G14713A and T29107A genotype with smoking status on individual CRC susceptibility.
CONCLUSION: This is the first report providing evidence that, Cav-1 being involved in CRC and may be novel useful genomic markers for early detection of CRC.
Key Words: Caveolin-1, Polymorphism, Colorectal cancer, Carcinogenesis, Smoking.
INTRODUCTION
Colorectal cancer is one of the most grave public health problems. There are nearly one million cases of colorectal cancer diagnosis worldwide each year. The prevalent incidence and age-adjusted mortality of CRC has keeping on increasing in the recent years in Taiwan. In 2008, the incidence and mortality of CRC has occupied the third place among the common cancers. Etiological studies have attributed more than 85% of CRC to several environmental factors [1, 2], and in particular meat consumption, cigarette smoking, exposure to carcinogenic aromatic amines, such as arylamines and heterocyclic amines [3-5].
In the recent years, investigators have got interested to caveolae to define how these lipid domains participate in the pathogenesis of human cancers and what their possible utility may be for the detection and treatment [6].Caveolae are vesicular invaginations of the plasma membrane, which has been thought to play a critical role in transcytosis, communication between cell surface membrane receptors and intracellular signaling protein cascades such as apoptosis and tumorigenesis [7, 8]. Caveolins are the major structural proteins of caveolae and this family contains three members in mammals, Caveolin-1 (Cav-1), Caveolin-2 and Caveolin-3 [7, 9], in which Cav-1 is the principal structural protein. It has been demonstrated that Cav-1 is down-regulated in sarcoma, lung carcinoma, and ovarian carcinoma [10-12]. However, elevated expression of Cav-1 has been associated with the metastasis of esophageal squamous cell carcinoma and prostate cancer and negatively correlated with patient survival [13, 14]. These findings indicate that the role of Cav-1 may vary considerably, depending on the tissue involved.
The emerging evidence pointing to the role of Cav-1 in carcinogenesis led us to study whether different alleles of this gene are associated with CRC. Thus, the aims of the current study were to determine the genotypic frequency of six polymorphisms of
the Cav-1 gene at C239A (rs1997623), G14713A (rs3807987), G21985A (12672038), T28608A (rs3757733), T29107A (rs7804372), and G32124A (rs3807992), and their association with CRC susceptibility. To the best of our knowledge, this is the largest study carried out to evaluate the contribution of Cav-1 polymorphisms in colorectal oncology.
MATERIALS AND METHODS
Study population and sample collection
The study population consisted of 362 CRC patients and 362 cancer-free control volunteers. Patients diagnosed with CRC were recruited at the outpatient clinics of general surgery between 2002-2008 at the China Medical University Hospital, Taichung, Taiwan, Republic of China. The clinical characteristics of patients, including histological details, were all graded and defined by expert surgeons (Dr. Yang’s team). All patients voluntarily participated, completed a self-administered questionnaire and provided peripheral blood samples. An equal number of non-cancer healthy volunteers were selected as controls by matching for age, gender and some indulgences after initial random sampling from the Health Examination Cohort of the hospital. The exclusion criteria of the control group included previous malignancy, metastasized cancer from other or unknown origin, and any familial or genetic diseases. This study was approved by the Institutional Review Board of the China Medical University Hospital and written-informed consent was obtained from all participants.
Genotyping conditions
Genomic DNA was prepared from peripheral blood leucocytes using a QIAamp Blood Mini Kit (Blossom, Taipei, Taiwan) and further processed according to our
previous papers [15-23]. Briefly, the following primers were used for Cav-1 C239A (rs1997623):
5’-GTGTCCGCTTCTGCTATCTG-3’ and 5’-GCCAAGATGCAGAAGGAGTT-3’;
for Cav-1
G 1 4 7 1 3 A ( r s 3 8 0 7 9 8 7 ) : 5 ’ - C C T T C C A G T A A G C A A G C T G T - 3 ’ a n d 5’-CCTCTCAATCTTGCCATAGT-3’; for Cav-1 G21985A (12672038): 5’-GGTGTCAGCAAGGCTATGCT-3’ and 5’-CCAGACACTCAGAATGTGAC-3’;
f o r
C a v - 1 T 2 8 6 0 8 A ( r s 3 7 5 7 7 3 3 ) : 5 ’ - G C T C A A C C T C A T C T G A G G C A - 3 ’ a n d
5’-GGCC TATTGT TGAGTGGATG-3’; for C a v - 1 T29107A (rs7804372): 5’-GCCTGAATTGCAATCCTGTG-3’ and
5’-ACGGTGTGAACACGGACATT-3’; and for
C a v - 1 G 3 2 1 2 4 A ( r s 3 8 0 7 9 9 2 ) : 5 ’ - G G T G T C T T G C A G T T G A A T G - 3 ’ a n d
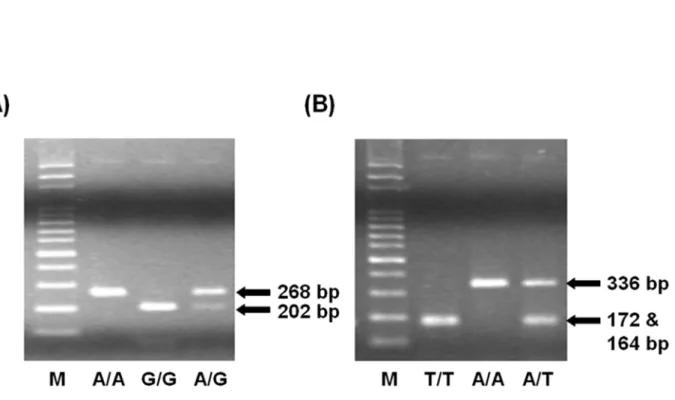
5’-ACGGAGCTACTCAGTGCCAA-3’. The following cycling conditions were performed: one cycle at 94oC for 5 min; 35 cycles of 94oC for 30 s, 55oC for 30 s, and 72oC for 30 s; and a final extension at 72oC for 10 min. The PCR products were studied after digestion with Avr II, Bfa I, Hae III, Tsp509 I, Sau3AI and Nla III, restriction enzymes for Cav-1 C239A (cut from 485 bp C type into 170+315 bp T type), Cav-1 G14713A (cut from 268 bp A type into 66+202 bp G type), Cav-1 G21985A (cut from 251+43 bp A type into 153+98+43 bp G type), Cav-1 T28608A (cut from 298 bp T type into 100+198 bp A type), Cav-1 T29107A (cut from 336 bp A type into 172+164 bp T type), and Cav-1 G32124A (cut from 213+142+67 bp A type into 142+118+95+67 bp T type), respectively.
Statistical analyses
into final analyzing. To ensure that the controls used were representative of the general population and to exclude the possibility of genotyping error, the deviation of the genotype frequencies of Cav-1 single nucleotide polymorphisms (SNP) in the control subjects from those expected under the Hardy-Weinberg equilibrium was assessed using the goodness-of-fit test. Pearson’s Chi-square test or Fisher’s exact test (when the expected number in any cell was less than five) was used to compare the distribution of the Cav-1 genotypes between cases and controls. Cancer risk associated with the genotypes was estimated as odds ratio (ORs) and 95% confidence intervals (CIs) using unconditional logistic regression. Data was recognized as significant when the statistical P-value was less than 0.05. To evaluate effect modification by smoking, stratified analyses were conducted for chosen SNPs to compare the association across exposure categories of smoking status (never-smokers and smokers). All statistical tests were performed using SAS, Version 9.1.3 (SAS Institute Inc., Cary, NC, USA) on two sided probabilities.
RESULTS
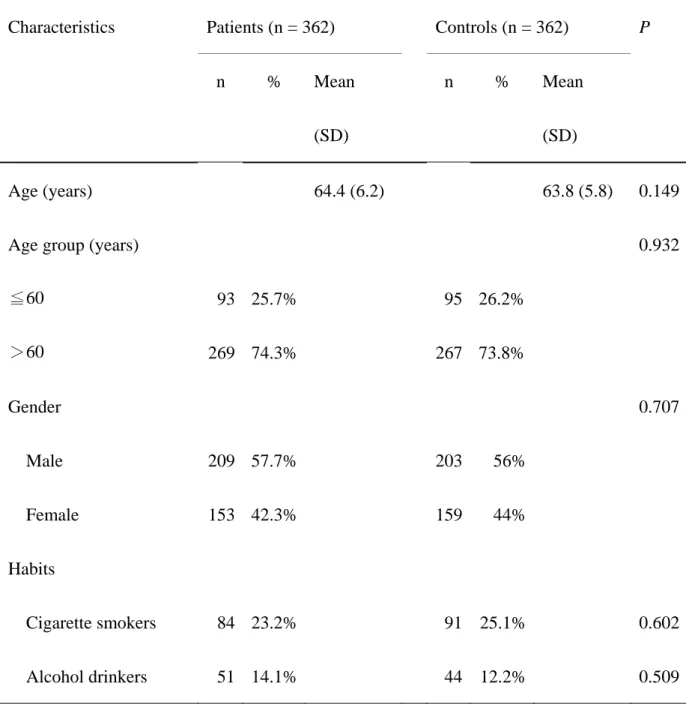
The frequency distributions of selected characteristics of CRC patients and controls are shown in Table I. These characteristics of patients and controls are all well matched. None of these differences between groups were statistically significant (P>0.05) (Table I). The frequencies of the genotypes for the Cav-1 C239A, G14713A, G21985A, T28608A, T29107A and G32124A between controls and CRC patients are shown in Table II. Genotype distribution of various genetic polymorphisms of Cav-1 G14713A and T29107A were significantly different between CRC and control groups (P=1.6*10-12 and 3.0*10-4, respectively), while those for Cav-1 C239A, G21985A, T28608A and G32124A were not significant (P>0.05) (Table II). To sum up, the polymorphism of Cav-1 G14713A and T29107A are associated with CRC risk and
may be a biomarker for CRC early detection. The representative PCR-based restriction analyses for the Cav-1 G14713A and T29107A polymorphisms were shown in Figure 1.
The frequencies of the alleles for the Cav-1 C239A, G14713A, G21985A, T28608A, T29107A and G32124A between controls and CRC patients are shown in Table III. The two SNPs of Cav-1 found to be associated with CRC in Table II, G14713A and T29107A, are also found to be associated with higher CRC susceptibility in their allele frequency analysis here. As for other four SNPs, the distributions of their allele frequencies are not significantly different in controls and CRC patients (Table III).
Considering potential interactions between the two significant SNPs of Cav-1 gene and CRC susceptibility, the risk of CRC related to haplotype distributions of
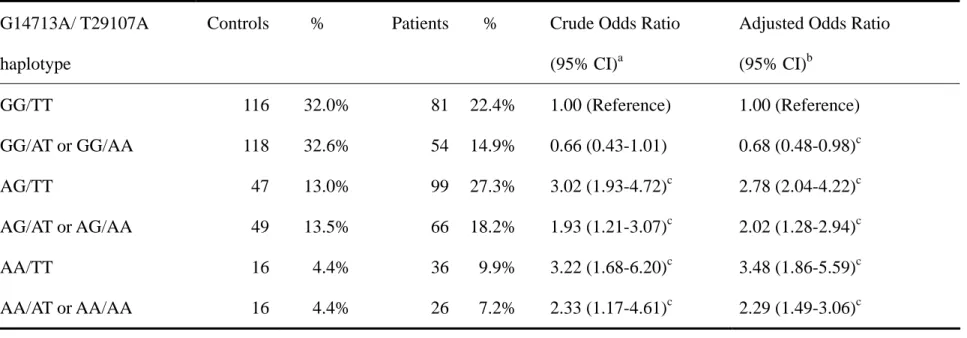
Cav-1 G14713A and T29107A were further analyzed (Table IV). Compared with
GG/TT haplotype of Cav-1 G14713A and T29107A, the GG/AT or GG/AA group has a 0.68-fold lower risk of CRC (95% CI=0.48-0.98). Other combinations of AG/TT, AG/AT or AG/AA, AA/TT, and AA/AT or AA/AA conferred 2.78-fold (95% CI=2.04-4.22), 2.02-fold (95% CI=1.28-2.94), 3.48-fold (95% CI=1.86-5.59) and 2.29-fold (95% CI=1.49-3.06) increased risks compared to the GG/TT haplotype, respectively (Table IV).
Since smoking is the predominant risk factor for CRC, the interaction between
Cav-1 genotype and individual smoking habits was also analyzed by stratified
individual smoking status (Table V). We noticed that subjects with the hetero- or homozygous AA for Cav-1 G14713A had higher risks of CRC in both smoker and non-smoker groups, no matter before or after adjusting their age, gender and smoking pack-years. In the case of Cav-1 T29107A, the homozygous AA had lower risks of CRC in both smoker and non-smoker groups. The heterozygous AT of Cav-1
T29107A also had protective effects in smoker group. To sum up, there was an obvious interaction between smoking status and Cav-1 genotypes in the CRC susceptibility.
DISCUSSION
Although several investigations have shown that Cav-1 plays a critical role in many tumors [10-14], few data are available which consider Cav-1 for genetic predisposition to cancers [24, 25]. In 2004, the inactivation of Cav-1 by mutation models or via reducing its expression was found to involve in the pathogenesis of oral cancer [25]
. In that study, the exon 1 and 3 sequences of Cav-1 were investigated in 74 oral squamous cell carcinomas and 15 oral cancer cell lines, and the expression of Cav-1 was examined. It was reported that only five mutations (1 missense and 4 silent mutations) of Cav-1 were identified in so many cases, and they were all found in exon 3 [25]. Since sequencing of exonic and promoter regions had not revealed and variants in Cav-1 that might have been directly involved in any cancer risk, it is reasonable for us to select intronic single nucleotide polymorphisms (SNPs) from the NCBI database, and to evaluate the role of Cav-1 polymorphisms, which have never been reported to be associated with CRC risk.
The main finding of this study is that Cav-1 G14713A (rs3807987) and T29107A (rs7804372) polymorphisms are associated with the susceptibility to CRC (Table II and III), while the other four polymorphisms were not. The combinative analysis about Cav-1 G14713A (rs3807987) and T29107A (rs7804372) showed that when taking G14713A/T29107A GG/TT haplotype as a reference, those with GG/AT or GG/AA were of lower CRC risk, while those with other haplotypes, including AG/TT, AG/AT or AG/AA, AA/TT, AA/AT or AA/AA, were of 1.93- to 3.22-fold higher risk. The data also supported that A allele of G14713A was risky, and A allele of T29107A
was protective. Although these genetic variations do not direct result in amino acid coding change, it is plausible to suspect the alternative splicing, intervention, modification, determination or involvement of these SNPs influence the expression level or stability of the Cav-1 protein. In our immunohistochemistry detection of tumor tissue from oral cancer patients, taking the distant parts from the same subjects as internal control, we have found that Cav-1 was down-regulated in the tumor sites (unpublished data).
Environmental factors such as cigarette smoking were reported to be closely related to CRC carcinogenesis. In this study, the joint effects of Cav-1 gene and individual smoking behaviors were analyzed, and both significant genetic-environmental interactions were observed in Cav-1 G14713A (rs3807987) and T29107A (rs7804372) (Table V). The sample size and similar trends of significant data after age- and behavior-adjustments strengthen the accuracy and reliability of our findings, and the frequencies of Cav-1 polymorphisms variant alleles were similar to those reported in the NCBI website in other Asian population studies. For instance, the minor A allele frequencies of Cav-1 G14713A are 22.1% in our control group, close to those of 16.7% for Beijing and 22.2% for Tokyo populations in NCBI, which strongly suggest no selection bias for the subject’s enrolments in terms of genotypes. The smoking population in our patient group is rather low, so that the data itself and that of matched control group are disadvantageous for us to do the stratified analysis of smoking status (Table V). We agree that it is important to verify our findings in further larger studies and clarify the role of Cav-1 with more phenotypic and functional evidence in CRC and other cancer. In conclusion, this is the first report to provide evidence for Cav-1 G14713A and T29107A, but not C239A, G21985A, T28608A, or G32124A, were associated with higher susceptibility to CRC. They both have joint effects with smoking status on CRC susceptibility. The G allele
of Cav-1 G14713A and the A allele of Cav-1 T29107A might become potential biomarkers for the CRC early detection, prediction and targets for integrative cancer therapy.
Acknowledgements
We are grateful to Wen-Shin Chang, Hsiu-Min Hsieh, Judy Wang and the Tissue Bank in China Medical University Hospital for their technical assistance. This study was supported by research grants from the China Medical University and Hospital (DMR-99-041 and CMU-99-NTU-10), the Terry Fox Cancer Research Foundation and the National Science Council (NSC 98-2320-B-039-010-MY3).
REFERENCES
1 Doll R, Peto R. The causes of cancer: quantitative estimates of avoidable risks of cancer in the United States today. J Natl Cancer Inst 1981; 66: 1191-1308
2 Munro MH, Blunt JW, Dumdei EJ, Hickford SJ, Lill RE, Li S, Battershill CN, Duckworth AR. The discovery and development of marine compounds with pharmaceutical potential. J Biotechnol 1999; 70: 15-25
3 Giovannucci E, Colditz GA, Stampfer MJ, Hunter D, Rosner BA, Willett WC, Speizer FE. A prospective study of cigarette smoking and risk of colorectal adenoma and colorectal cancer in U.S. women. J Natl Cancer Inst 1994; 86: 192-199
4 Giovannucci E, Rimm EB, Stampfer MJ, Colditz GA, Ascherio A, Kearney J, Willett WC. A prospective study of cigarette smoking and risk of colorectal adenoma and colorectal cancer in U.S. men. J Natl Cancer Inst 1994; 86: 183-191
5 Heineman EF, Zahm SH, McLaughlin JK, Vaught JB. Increased risk of colorectal cancer among smokers: results of a 26-year follow-up of US veterans and a review. Int J Cancer 1994; 59: 728-738
6 Carver LA, Schnitzer JE, Anderson RG, Mohla S. Role of caveolae and lipid rafts in cancer: workshop summary and future needs. Cancer Res 2003; 63: 6571-6574
7 Juhasz M, Chen J, Tulassay Z, Malfertheiner P, Ebert MP. Expression of caveolin-1 in gastrointestinal and extraintestinal cancers. J Cancer Res Clin Oncol 2003; 129: 493-497 8 Smart EJ, Graf GA, McNiven MA, Sessa WC, Engelman JA, Scherer PE, Okamoto T,
Lisanti MP. Caveolins, liquid-ordered domains, and signal transduction. Mol Cell Biol 1999; 19: 7289-7304
9 Galbiati F, Engelman JA, Volonte D, Zhang XL, Minetti C, Li M, Hou H, Jr., Kneitz B, Edelmann W, Lisanti MP. Caveolin-3 null mice show a loss of caveolae, changes in the microdomain distribution of the dystrophin-glycoprotein complex, and t-tubule abnormalities. J Biol Chem 2001; 276: 21425-21433
carcinoma and acts as a candidate tumor suppressor gene. Chest 2004; 125: 106S
11 Wiechen K, Diatchenko L, Agoulnik A, Scharff KM, Schober H, Arlt K, Zhumabayeva B, Siebert PD, Dietel M, Schafer R, Sers C. Caveolin-1 is down-regulated in human ovarian carcinoma and acts as a candidate tumor suppressor gene. Am J Pathol 2001; 159: 1635-1643
12 Wiechen K, Sers C, Agoulnik A, Arlt K, Dietel M, Schlag PM, Schneider U. Down-regulation of caveolin-1, a candidate tumor suppressor gene, in sarcomas. Am J
Pathol 2001; 158: 833-839
13 Kato K, Hida Y, Miyamoto M, Hashida H, Shinohara T, Itoh T, Okushiba S, Kondo S, Katoh H. Overexpression of caveolin-1 in esophageal squamous cell carcinoma correlates with lymph node metastasis and pathologic stage. Cancer 2002; 94: 929-933
14 Yang G, Truong LD, Wheeler TM, Thompson TC. Caveolin-1 expression in clinically confined human prostate cancer: a novel prognostic marker. Cancer Res 1999; 59: 5719-5723
15 Bau DT, Tseng HC, Wang CH, Chiu CF, Hua CH, Wu CN, Liang SY, Wang CL, Tsai CW, Tsai MH. Oral cancer and genetic polymorphism of DNA double strand break gene Ku70 in Taiwan. Oral Oncol 2008; 44: 1047-1051
16 Chang CH, Chiu CF, Liang SY, Wu HC, Chang CL, Tsai CW, Wang HC, Lee HZ, Bau DT. Significant association of Ku80 single nucleotide polymorphisms with bladder cancer susceptibility in Taiwan. Anticancer Res 2009; 29: 1275-1279
17 Chang CH, Wang RF, Tsai RY, Wu HC, Wang CH, Tsai CW, Chang CL, Tsou YA, Liu CS, Bau DT. Significant association of XPD codon 312 single nucleotide polymorphism with bladder cancer susceptibility in Taiwan. Anticancer Res 2009; 29: 3903-3907
18 Chiu CF, Tsai MH, Tseng HC, Wang CL, Tsai FJ, Lin CC, Bau DT. A novel single nucleotide polymorphism in ERCC6 gene is associated with oral cancer susceptibility in Taiwanese patients. Oral Oncol 2008; 44: 582-586
single nucleotide polymorphism in XRCC4 gene is associated with oral cancer susceptibility in Taiwanese patients. Oral Oncol 2008; 44: 898-902
20 Chiu CF, Wang CH, Wang CL, Lin CC, Hsu NY, Weng JR, Bau DT. A novel single nucleotide polymorphism in XRCC4 gene is associated with gastric cancer susceptibility in Taiwan. Ann Surg Oncol 2008; 15: 514-518
21 Hsu CF, Tseng HC, Chiu CF, Liang SY, Tsai CW, Tsai MH, Bau DT. Association between DNA double strand break gene Ku80 polymorphisms and oral cancer susceptibility. Oral Oncol 2009; 45: 789-793
22 Wang HC, Chiu CF, Tsai RY, Kuo YS, Chen HS, Wang RF, Tsai CW, Chang CH, Lin CC, Bau DT. Association of genetic polymorphisms of EXO1 gene with risk of breast cancer in Taiwan. Anticancer Res 2009; 29: 3897-3901
23 Yang MD, Hsu YM, Kuo YS, Chen HS, Chang CL, Wu CN, Chang CH, Liao YM, Wang HC, Wang MF, Bau DT. Significant association of Ku80 single nucleotide polymorphisms with colorectal cancer susceptibility in Central Taiwan. Anticancer Res 2009; 29: 2239-2242
24 Conde MC, Ramirez-Lorca R, Lopez-Jamar JM, Molero E, Ramirez-Armengol JA, Moreno Nogueira JA, Pascual MH, Ruiz A, Martin-Cordova CG, Real LM, Royo JL. Genetic analysis of caveolin-1 and eNOS genes in colorectal cancer. Oncol Rep 2006; 16: 353-359
25 Han SE, Park KH, Lee G, Huh YJ, Min BM. Mutation and aberrant expression of Caveolin-1 in human oral squamous cell carcinomas and oral cancer cell lines. Int J
Figure Legend
Fig 1. PCR-based restriction analysis of the G14713A (A) and T29107A (B) polymorphisms of
Cav-1 gene shown on 3% agarose electrophoresis. M: 100 bp DNA size marker, (A) A/A:
indivisible homozygote, A/G: heterozygote, and G/G: divisible homozygote. (B) A/A: indivisible homozygote, A/T: heterozygote, and T/T: divisible homozygote.
Table I Frequency distributions of characteristics among colorectal cancer patients and controls.
Characteristics Patients (n = 362) Controls (n = 362) P
n % Mean
(SD)
n % Mean
(SD)
Age (years) 64.4 (6.2) 63.8 (5.8) 0.149
Age group (years) 0.932
≦60 93 25.7% 95 26.2% >60 269 74.3% 267 73.8% Gender 0.707 Male 209 57.7% 203 56% Female 153 42.3% 159 44% Habits Cigarette smokers 84 23.2% 91 25.1% 0.602 Alcohol drinkers 51 14.1% 44 12.2% 0.509 a
Table II. Distribution of Cav-1 genotypes among colorectal cancer patients and controls
Genotype Controls % Patients % Pa
C239A rs1997623 0.3837 CC 355 98.1% 357 98.6% AC 7 1.9% 5 1.4% AA 0 0.0% 0 0.0% G14713A rs3807987 1.6*10-12 GG 234 64.6% 135 37.3% AG 96 26.5% 165 45.6% AA 32 8.8% 62 17.1% G21985A rs12672038 0.9722 GG 211 58.2% 214 59.1% AG 124 34.3% 122 33.7% AA 27 7.5% 26 7.2% T28608A rs3757733 0.8964 TT 209 57.7% 214 59.1% AT 120 33.2% 118 32.6% AA 33 9.1% 30 8.3% T29107A rs7804372 0.0003 TT 179 49.5% 216 59.7% AT 120 33.1% 117 32.3% AA 63 17.4% 29 8.0% G32124A rs3807992 0.8583 GG 179 49.4% 172 47.5% AG 144 39.8% 148 40.9% AA 39 10.8% 42 11.6% a
Table III. Distribution of Cav-1 alleles among colorectal cancer patients and controls
Allele Controls % Patients % Pa
C239A rs1997623 0.5621 Allele C 717 99.0% 719 99.3% Allele A 7 1.0% 5 0.7% G14713A rs3807987 2.3*10-13 Allele G 564 77.9% 435 60.1% Allele A 160 22.1% 289 39.9% G21985A rs12672038 0.8064 Allele G 546 75.4% 550 76.0% Allele A 178 24.6% 174 24.0% T28608A rs3757733 0.6279 Allele T 538 74.3% 546 75.4% Allele A 186 25.7% 178 24.6% T29107A rs7804372 4.0*10-5 Allele T 478 66.0% 549 75.8% Allele A 246 34.0% 175 24.2% G32124A rs3807992 0.5711 Allele G 502 69.3% 492 68.0% Allele A 222 30.7% 232 32.0% a
Table IV Distribution of Cav-1 G14713A/ T29107A haplotypes among colorectal cancer patients and controls G14713A/ T29107A
haplotype
Controls % Patients % Crude Odds Ratio
(95% CI)a
Adjusted Odds Ratio (95% CI)b GG/TT 116 32.0% 81 22.4% 1.00 (Reference) 1.00 (Reference) GG/AT or GG/AA 118 32.6% 54 14.9% 0.66 (0.43-1.01) 0.68 (0.48-0.98)c AG/TT 47 13.0% 99 27.3% 3.02 (1.93-4.72)c 2.78 (2.04-4.22)c AG/AT or AG/AA 49 13.5% 66 18.2% 1.93 (1.21-3.07)c 2.02 (1.28-2.94)c AA/TT 16 4.4% 36 9.9% 3.22 (1.68-6.20)c 3.48 (1.86-5.59)c AA/AT or AA/AA 16 4.4% 26 7.2% 2.33 (1.17-4.61)c 2.29 (1.49-3.06)c a
95% CI, 95% confidence interval. b
95% CI, 95% confidence interval, and date were calculated by unconditioned logistic regression and adjusted for age, gender, smoking, alcohol drinking and betel quid chewing behaviors.
c
Table V. Distribution of Cav-1 G14713A and T29107A genotypes and colorectal cancer after stratification by smoking habit.
Overall Never smokers Ever smokers
SNP/Genotype Controls N (%) Cases N (%) Adjusteda OR (95% CI)c Controls N (%) Cases N (%) Adjustedb OR (95% CI)c Controls N (%) Cases N (%) Adjustedb OR (95% CI)c G14713A (rs3807987) GG AG AA 234 (64.6) 96 (26.5) 32 ( 8.8) 135 (37.3) 165 (45.6) 62 (17.1) 1.00 (Ref.d) 2.98 (2.14-4.14) 3.36 (2.09-5.41) 171 (63.1) 75 (27.7) 25 (9.2) 107 (38.5) 124 (44.6) 47 (16.9) 1.00 (Ref.d) 2.64 (1.81-3.84) 3.00 (1.75-5.17) 63 (69.2) 21 (23.1) 7 (7.7) 28 (33.3) 41 (48.8) 15 (17.9) 1.00 (Ref.d) 4.39 (2.21-8.75) 4.82 (1.77-13.13) T29107A (rs7804372) TT AT AA 179 (49.5) 120 (33.1) 63 (17.4) 216 (59.7) 117 (32.3) 29 (8.0) 1.00 (Ref.d) 0.79 (0.57-1.11) 0.37 (0.23-0.58) 136 (50.2) 89 (32.8) 46 (17.0) 164 (59.0) 91 (32.7) 23 (8.3) 1.00 (Ref.d) 0.84 (0.54-1.21) 0.40 (0.22-0.71) 43 (47.3) 52 (34.1) 17 (18.6) 52 (61.9) 26 (31.0) 6 (7.1) 1.00 (Ref.d) 0.40 (0.22-0.76) 0.28 (0.21-0.79) a
Adjusted for age, gender and smoking (pack-years). b
Adjusted for age and gender. c
OR, odds ratio; CI, confidence interval. d