O
BSESSIVE
-
COMPULSIVE
S
YMPTOMS
A
SSOCIATED
WITH
C
LOZAPINE
AND
R
ISPERIDONE
T
REATMENT
: T
HREE
C
ASE
R
EPORTS
AND
R
EVIEW
OF
THE
L
ITERATURE
Chiao-Li Ke, Cheng-Fang Yen, Cheng-Chung Chen, Shang-Ju Yang, Weilun Chung, and Ming-Jen Yang
Department of Psychiatry, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan.
Treatment-emergent obsessive-compulsive symptoms (OCSs) have raised concern since the widespread introduction of serotonin-dopamine antagonists (SDAs) for the treatment of schizophrenia. Further investigations of SDA-emergent OCSs and their response to anti-obsessional agents will be beneficial for clinicians in helping patients who suffer from this problem. We present three cases of schizophrenia in which distressing OCSs occurred during clozapine or risperidone treatment. OCSs were assessed consecutively using the Yale-Brown Obsessive-Compulsive Scale. The OCSs of these three patients were responsive to anti-obsessional agents, including fluvoxamine, clomipramine, and paroxetine. We also review the current literature and discuss the possible pathophysiology and psychopathology of SDA-emergent OCSs.
Key Words: obsessive-compulsive symptoms, clozapine, risperidone, schizophrenia, serotonin-dopamine antagonists
(Kaohsiung J Med Sci 2004;20:295–301)
Received: February 5, 2004 Accepted: April 2, 2004 Address correspondence and reprint requests to: Dr. Cheng-Fang Yen, Department of Psychiatry, Kaohsiung Medical University, 100 Tzyou 1st Road, Kaohsiung 807, Taiwan.
E-mail: [email protected]
Clozapine and risperidone bind strongly to serotonin (5-HT2) and dopamine (D2) receptors, improving both the
positive and negative symptoms of schizophrenia [1]. Serotonin-dopamine antagonists (SDAs) carry a smaller risk of extrapyramidal symptoms than dopamine recep-tor antagonists, and eliminate the need for concurrent anticholinergic drugs with adverse effects [2]. SDAs have been recommended for patients with schizophrenia in various clinical stages [3].
However, the adverse effects of SDAs reported in the literature are numerous [1]. One of the side effects is treatment-emergent obsessive-compulsive symptoms (OCSs) in patients with a favorable antipsychotic response to clozapine [4,5], risperidone [6,7], and olanzapine [8].
Although the imbalance in serotonin-dopamine neuro-transmission with a preponderance of serotonin antago-nism was proposed as a possible explanation of this side effect [5,9], the causal relationship between OCSs and SDA treatment has not been established. Few of the case reports discuss the effects of anti-obsessional agents, including fluvoxamine [9], sertraline [10,11], and clomipra-mine [12], in the treatment of SDA-emergent OCSs. Fur-ther investigation of the pathophysiology and psychopatho-logy of treatment-emergent obsessive-compulsive fea-tures is needed, as well as research into the pathology of OCSs and the pharmacologic mechanisms of SDAs and anti-obsessional agents.
We report three cases with a diagnosis of schizophre-nia according to DSM-IV [13], in which OCSs emerged dur-ing the course of clozapine or risperidone treatment. The response of OCSs to anti-obsessional agents, including flu-voxamine, clomipramine, and paroxetine, is also reported. OCSs were assessed consecutively using the Yale-Brown Obsessive-Compulsive Scale (YBOCS) [14] during a trial of anti-obsessional agents with ongoing clozapine or
ris-peridone treatment with at least a 7-month follow-up. In current reviews, only a few case reports of OCSs have been assessed using rating scales [8,9,12,15]. To the best of our knowledge, this is the first report demonstrating the effica-cy of paroxetine treatment of SDA-related OCSs in schizo-phrenic patients. We also review the current literature and discuss the possible pathology of SDA-emergent OCSs.
C
ASEP
RESENTATIONSCase 1
A 24-year-old man met the DSM-IV criteria for schizophre-nia at the age of 19, with initial manifestations of severe auditory and visual hallucination, disorganized speech and behaviors, and delusions of reference and persecution. He had been hospitalized four times in our hospital’s acute ward, and received multiple trials of conventional anti-psychotics, SDAs, and electroconvulsive therapy. He had no history of obsessive-compulsive disorder (OCD) or personality disorder (OCPD). However, during a trial of risperidone 6 mg/day, he obsessively worried that his father would die, and complained that he felt disgusted while intrusive sexual images were overplayed in his mind. Clozapine treatment was started and titrated up to 400 mg/day, with significant improvement of auditory hallucination and delusion.
Due to a seizure attack after 17 weeks of clozapine treatment, medication dosage was reduced to 300 mg/day. Eight months after administration of clozapine 300 mg/ day, the patient became anxious and restless, compulsively
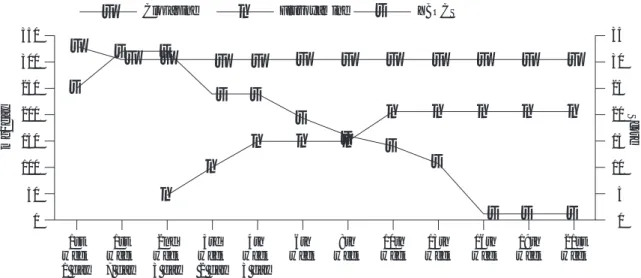
asked the same questions, and repeatedly asked for con-firmation from the staff in our day hospital. He was ob-sessed with minutiae and was often preoccupied with thoughts of breakage of the wash basin and viral infec-tion of his liver. He persistently requested laboratory examinations to evaluate his liver function even after re-assurance had been given. In addition, he worried irra-tionally that the traffic signals might not work, and he therefore rode a motorcycle about, checking repeatedly to make sure that the traffic lights worked. His obsessive and compulsive behavior caused significant distress and impairment of his daily activities and function. For these OCSs, clozapine was increased to 325 mg/day with the consideration of super-sensitivity of 5-HT receptors with long-term clozapine treatment. However, his OCSs were not responsive to this treatment and persisted. Clo-zapine was decreased back to 300 mg/day and fluvox-amine treatment was added, beginning with 50 mg/day and progressively increased to 200 mg/day in incre-ments of 50 mg. The severity of OCSs decreased after the initiation of fluvoxamine treatment. Fourteen weeks later, the total YBOCS score had decreased from 32 to 1 (Fig-ure 1). Interestingly, his obsession with viral infection of his liver recurred when fluvoxamine was tapered to 100 mg/day. This obsessive symptom subsided again after the dosage of fluvoxamine was increased back to 150 mg/day. Improvement of OCSs remained after 10 months’ follow-up with fluvoxamine at 150–200 mg/day.
Case 2
A 20-year-old man had a 3-year history of schizophrenia,
Figure 1. Medication dosages and Yale-Brown Obsessive-Compulsive Scale (YBOCS) scores in Case 1.
■
■
■
■
■
■
■
■
■
■
■
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
◆
◆
◆
◆
◆
◆
◆
◆
◆
◆
◆
◆
◆
mg/day 350 300 250 200 150 100 50 0 1st 1st 2nd 3rd 4th 6th 8th 10th 13th 16th 19th 21st week week week week week week week week week week week week 1 day 7 day 3 day 2 day 3 dayClozapine Fluvoxamine YBOCS
Score 35 30 25 20 15 10 5 0
paranoid type, episodic with inter-episode residual symp-toms. He presented with progressive social withdrawal, apathy, affective flattening, poor personal care, auditory hallucination, and delusion of persecution in the initial episode, and he was treated using electroconvulsive therapy. Risperidone 3 mg/day was prescribed in the following 2 years. With this treatment, he was able to join a rehabilitation program and even obtain sheltered work. There was no history of OCSs.
Risperidone was increased to 4 mg/day for persistent voice commenting and delusion of reference. However, 2 weeks later, he suffered from severe egodystonic obses-sion symptoms and was preoccupied with ruminations about past unpleasant events. Recurrent sexual images were experienced as intrusive. The severity of obsessive thinking led to a trial of clomipramine 25 mg/day. Three weeks after clomipramine was introduced, the obsessive symptoms attenuated, with the YBOCS score decreasing from 14 to 1. Simultaneously, risperidone was adjusted again due to apparent positive symptoms. Unfortunately, obsessive thinking about mistakes, with obsessive anxiety and compulsive behaviors, developed again 2 weeks later when the dosage of risperidone reached 6 mg/day. Paro-xetine 20 mg/day was added to replace clomipramine, with ongoing risperidone regimen. A marked reduction in his obsession was found 2 weeks later (Figure 2). The substan-tial improvement was observed at 10 months’ follow-up with paroxetine at doses of 20–30 mg/day. However, these obsession symptoms worsened when paroxetine was
decreased, and even relapsed transiently over a 2-month period of treatment with paroxetine 20 mg/day.
Case 3
A 31-year-old man had been diagnosed with schizophrenia, paranoid type, 4 years previously, with presentations of severe auditory and visual hallucination and delusions of persecution, reference, and grandeur for several years. He was troubled by psychotic symptoms and reacted irritably and violently, abusing alcohol to overcome fear and per-ceptual disturbance. Neither a history of OCD nor OCPD had been reported.
Risperidone was administered at 4–6 mg/day during hospitalization 1 year ago. His condition was responsive to the treatment but, unfortunately, he suffered from post-psychotic depression after nearly full remission of delusion and hallucination, under treatment with risperi-done 4 mg/day. The depressive episode, which was care-fully differentiated from negative symptoms and extra-pyramidal symptoms, resolved 1 month later without any antidepressant medication. However, he suddenly be-came obsessive 3 months after risperidone was intro-duced. He was totally preoccupied by the thought of his drunken state and a past contractual obligation. He repeti-tively talked about the same thing all day long, even af-ter his family confirmed to him that he was not respon-sible for this contract. He was extremely worried that he would be arrested and jailed because he had not fulfilled it, and he attempted suicide by drug overdose. The
obses-1st 3rd 3rd 4th 5th 6th 8th 9th 10th 11th 13th 15th week week week week week week week week week week week week
1 day 4 day 4 day 4 day 4 day 4 day 4 day 30 25 20 15 10 5 0 mg/day Score
■
■
■
■
■
■
▲
▲
▲
▲
●
●
●
●
●
●
●
●
●
●
●
●
◆
◆
◆
◆
◆
◆
◆
◆
◆
◆
◆
◆
30 25 20 15 10 5 0 Risperidone Clomipramine Paroxetine YBOCS■
▲
◆
●
sive thinking persisted and was not responsive to benzo-diazepine and paroxetine 20 mg/day over a 1-month period. Clomipramine was started. Risperidone was with-drawn later and olanzapine was administered. The OCSs improved with a 3-week regimen of olanzapine 10 mg/day and clomipramine 75 mg/day, and YBOCS score de-creased from 39 to 5 (Figure 3). The improvement per-sisted in the following 7 months’ follow-up. Clomipra-mine was decreased gradually without recurrence of OCSs.
D
ISCUSSIONReports of atypical antipsychotic drug-related OCSs are mostly linked to clozapine and risperidone, and are found in up to 10% of clozapine-treated patients [16]. A few cases with olanzapine [8] and quetiapine [17] have also been re-ported. All these SDAs have potent 5-HT2 and D2
antago-nism at therapeutic doses. The hypothesis of the role that serotonin plays in OCD was based on the observation that treatment involves manipulating serotonin activities [18]. It has been suggested that the anti-serotonergic effects of SDAs are responsible for the emergence of OCSs [10]. The favorable responses of the treatment-emergent OCSs to selective serotonin reuptake inhibitors (SSRI), clomipramine, and potent serotonin reuptake inhibitors further support this viewpoint.
In addition, several lines of evidence show that dopamine is implicated in the mediation of some obsessive-compulsive behaviors [19,20]. The importance of anatomic and function-al interactions between serotonergic and dopaminergic neurons must be considered. The decreases in 5-HT tonic
inhibitory influences on dopamine neurons could lead to increased dopaminergic function due to the functional connections between dopamine and 5-HT neurons in the basal ganglion [19,20]. As a result, it has been postulated that the hyperactivity of the dopaminergic system in the striatum contributes to the rise in OCSs [12].
Norepinephrine is another member of the monoamine system involved in the pathophysiology of OCSs [21]. Both Cases 2 and 3 experienced a clinical improvement in OCSs with clomipramine and paroxetine treatment. Both drugs inhibit serotonin reuptake and display po-tent norepinephrine reuptake antagonism [19]. This in-directly suggests that abnormalities in norepinephrine may play a role in SDA-related OCSs.
All three cases had no history of OCD or OCPD. In previous studies, some cases had a history of OCD [5–7,9, 22], but most had no history of OCD or OCPD [6,9,10,12,16, 18,23,24]. Remington and Adams reported that a subgroup of schizophrenic patients who already manifest obsessive-compulsive features as a part of their illness may be at particular risk for treatment-emergent OCSs [22].
There may be a subset of patients vulnerable to the development of obsessive phenomena associated with atypical antipsychotics [6]. At high doses, SDAs block the postsynaptic receptors in the nigrostriatal dopamine pathway rather than mesolimbic pathway, and are, there-fore, responsible for extrapyramidal side effects and more commonly associated with the emergence of OCSs [19, 20]. This differential dose effect on dopamine and 5-HT systems, along with the beneficial effect of low doses of SDAs on refractory OCD, may indicate that the pri-mary abnormality is in the serotonin-dopamine balance.
Figure 3. Medication dosages and Yale-Brown Obsessive-Compulsive Scale (YBOCS) scores in Case 3.
2nd 3rd 5th 5th 5th 5th 6th 8th 8th 10th 20th 31st week week week week week week week week week week week week 4 day 4 day 2 day 4 day 6 day 7 day 7 day 1 day 4 day 4 day 4 day 5 day 80 60 40 20 0 mg/day Score
■
■
■
■
■
■
■
■
■
■
■
■
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
▲
◆
◆
◆
◆
◆
◆
◆
◆
◆
◆
◆
◆
●
●
●
●
●
●
●
●
●
●
●
●
40 20 0 Risperidone Olanzapine Clomipramine■
YBOCS▲
◆
●
Greater sensitivity for the development of extrapyrami-dal side effects in patients may be consistent with this abnormality [6]. However, the underlying mechanisms and risk factors are far from clear.
There is no gender prevalence in OCD [2], but SDA-induced OCSs are more common in men according to previous reported cases. We have reviewed 28 cases of clozapine- or risperidone-induced OCSs [5–7,9,10,12,16, 18,22–26] reported between 1990 and 2003. There were 24 male patients and only four females [5,6,18]. Their ages ranged from 19 to 56 years, with most patients in their twenties or thirties. Our three cases were young male pa-tients, which is consistent with previous studies. The effect of gender and age factors should be further investigated.
SDA-induced OCSs seem to be dose-related. Several case reports suggest that clozapine-induced OCSs emerge only at doses above a certain threshold; the mean dose of the cases in the literature is moderate to high at 454.2 ± 187.9 mg [8]. In all reported cases, the risperidone dose exceeded 3 mg/day [6]. However, the onset of OCSs does not seem to be predictable. Treatment-induced OCSs emerged within weeks to months of SDA therapy or dose increase [5–7,9,10,12,16,18,22–26]. Biondi et al reviewed cases and reported that the latency of appear-ance of OCSs related to the beginning of clozapine treat-ment ranged from 2 months to 1 year [12]. In risperidone-treated patients, the OCSs, which emerged within days to weeks, appeared earlier than in clozapine-treated patients [6,7,18,22,26].
Poyurovsky et al reported that OCSs appeared during the period of clozapine dose titration in reviewed cases [16]. In certain vulnerable individuals treated chronically with clozapine, “withdrawal” or “tardive” OCSs may develop, possibly because of the pathophysiologic development of a super-sensitivity in 5-HT receptors as a result of the potent 5-HT antagonistic activity of clozapine [27].
In contrast, Poyurovsky et al also reported the dis-appearance of OCSs in two cases during a subsequent ti-tration of clozapine [9]. Two other patients in their report [9] and our first case showed improvement with the addition of fluvoxamine, which had a similar effect to the addition of fluoxetine [9] or clomipramine [12] to cloza-pine pharmacotherapy. However, it is likely that pa-tients had their clozapine “dose” effectively increased by the addition of fluvoxamine [28] due to significant drug interaction between clozapine (metabolized through liver P450 2D6 and IA2 isoenzymes) and fluvoxamine (inhibition of P450 IA2) [19]. On the other hand, it may
and simultaneously increasing serotonin activity im-proves SDA-induced OCSs. Rahman et al reported that the addition of fluvoxamine interfered with the efficacy of clozapine, even though the plasma level was higher [25]. Fluvoxamine is effective in risperidone-induced OCSs [7].
R
EFERENCES1. Schatzberg AF, Nemeroff CB. Textbook of Psychopharmacology, 2nd
edition. Washington, DC: American Psychiatric Press, 2003.
2. Sadock BJ, Sadock VA. Kaplan & Sadock’s Synopsis of Psychiatry:
Behavioral Science/Clinical Psychiatry, 9th edition. Philadelphia: Lippincott Williams & Wilkins, 2003.
3. American Psychiatric Association. Practice guideline for the treatment of patients with schizophrenia. Am J Psychiatry 1997;154(4 Suppl):1–63.
4. Ghaemi SN, Zarate CA, Popli AP, et al. Is there a relation-ship between clozapine and obsessive-compulsive disor-der? A retrospective chart review. Compr Psychiatry 1995;36: 267–70.
5. Backer RW, Chengappa KN, Baird JW, et al. Emergence of obsessive-compulsive symptoms during treatment with clozapine. J Clin Psychiatry 1992;53:439–42.
6. Alevizos B, Lykouras L, Zervas IM, et al. Risperidone-induced obsessive-compulsive symptoms: a series of six cases. J Clin
Psychopharmacol 2002;22:461–7.
7. Kopala L, Honer WG. Risperidone, serotonergic mechanisms and obsessive-compulsive symptoms in schizophrenia. Am J
Psychiatry 1994;151:1714–5.
8. Backer RW, Ames D, Umbricht DS, et al. Obsessive-compulsive symptoms in schizophrenia: a comparison of olanzapine and placebo. Psychopharmacol Bull 1996;32:89–93.
9. Poyurovsky M, Hermesh H, Weizman A. Fluvoxamine treatment in clozapine-induced obsessive-compulsive symptoms in schizophrenic patients. Clin Neuropharmacol 1996; 19:305–13.
10. Allen L, Tejera C. Treatment of clozapine-induced obsessive-compulsive symptoms with sertraline. Am J Psychiatry 1994; 151:1096–7.
11. Dodt JE, Byerly MJ, Cuadros C, Christensen RC. Treatment of risperidone-induced obsessive-compulsive symptoms with sertraline. Am J Psychiatry 1997;154:582.
12. Biondi M, Fedele L, Arcangeli T, Pancheri P. Development of obsessive-compulsive symptoms during clozapine treatment in schizophrenia and its positive response to clomipramine.
Psychother Psychosom 1999;68:111–2.
13. American Psychiatric Association. Diagnostic and Statistical
Manual of Mental Disorders DSM-IV, 3rd edition. Washington DC: American Psychiatric Press, 1994.
14. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive scale. I. Development, use and reliability. Arch Gen Psychiatry 1989;46:1006–11.
symptoms associated with clozapine. Br J Psychiatry 1994;164: 687–8.
16. Poyurovsky M, Bergman Y, Shoshani D, et al. Emergence of obsessive-compulsive symptoms and tics during clozapine withdrawal. Clin Neuropharmacol 1998;21:97–100.
17. Khullar A, Chue P, Tibbo P. Quetiapine and obsessive-compulsive symptoms (OCS): a case report and review of a typical antipsychotic-induced OCS. J Psychiatry Neurosci 2001;26: 55–9.
18. Aalzaid K, Jones BD. A case report of risperidone-induced obsessive-compulsive symptoms. J Clin Psychopharmacol 1997; 17:58–9.
19. Stahl SM. Essential Psychopharmacology: Neuroscience Basis and
Practical Applications. Cambridge: Cambridge University Press,
2000.
20. Stahl SM. Basal ganglia neuropharmacology and obsessive and compulsive disorder: the obsessive-compulsive disorder hypothesis of basal ganglia dysfunction. Psychopharmacol Bull 1988;24:370–4.
21. McDougle CJ, Barr LC, Goodman WK, Price LH. Possible role
of neuropeptides in obsessive compulsive disorder.
Psycho-neuroendocrinology 1999;24:1–24.
22. Remington G, Adams M. Risperidone and obsessive-compulsive symptoms. J Clin Psychopharmacol 1994;14:358–9.
23. Patil VJ. Development of transient obsessive-compulsive symptoms during treatment with clozapine. Am J Psychiatry 1992;149:272.
24. Mahendran R. Obsessive-compulsive symptoms with ris-peridone. J Clin Psychiatry 1999;60:261–3.
25. Rahman MS, Grace JJ, Pato MT, et al. Sertraline in the treatment of clozapine-induced obsessive-compulsive behavior. Am J
Psychiatry 1998;115:1629–30.
26. Bakaras P, Georgoussi M, Liakos A, et al. Development of obsessive and depressive symptoms during risperidone treatment. Br J Psychiatry 1999;174:559. Erratum in: Br J
Psychiatry 1999;175:394.
27. Meltzer HY. The mechanism of action of novel antipsychotic drugs. Schizophr Bull 1991;17:263–87.
28. Markowitz JS. Clozapine-fluvoxamine interaction. Clin