Endoscopic diagnosis of intestinal
peni-cilliosis marneffei: report of three cases
and review of the literature
Chow-In Ko, MD, Chien-Ching Hung, MD, Mao-Yuan Chen, MD, Po-Ren Hsueh, MD, Cheng-Hsiang Hsiao, MD, Jau-Min Wong, MD
Diarrhea is the most common GI presentation of
immunocompromised patients, especially those with
acquired immunodeficiency syndrome (AIDS).
1,2More than 50% of patients with AIDS have diarrhea
caused by a variety of pathogens during their
illness.
1,2Intestinal mycoses are uncommon in
immunocompromised patients, however, and may be
caused by Cryptococcus neoformans
3and
Histo-plasma capsulatum.
4Penicillium marneffei, an emerging facultative
intracellular pathogen and the only thermally
dimor-phic fungus of the genus Penicillium, can cause
dis-seminated infection in patients residing in or
travel-ing to areas where the organism is endemic, which
include southeast Asia, southern China, and Hong
Kong.
5-17With the human immunodeficiency virus
(HIV) pandemic, the number of cases of penicilliosis
marneffei has increased markedly during the past 5
years, from 30 cases during the period between 1973
and 1990 to more than 160 by the end of 1995.
16After
extrapulmonary tuberculosis and cryptococcosis,
penicilliosis marneffei ranks as the third most
com-mon opportunistic infection in HIV-infected patients
in Thailand.
14Although P marneffei has become an
increasingly important cause of invasive mycoses in
immunocompromised hosts, it has been rarely
impli-cated as a cause of intestinal mycoses. As of
December 1997, only four cases of intestinal
penicil-liosis marneffei have been reported in English
lan-guage publications and only one was diagnosed
ante-mortem by endoscopy.
8,9,12,17Here we report three
cases in which immunocompromised patients, two
with AIDS and one after renal transplantation,
pre-sented with intestinal penicilliosis marneffei where
early diagnosis was made possible by endoscopy.
CASE REPORT Case 1
A 33-year-old man, who had undergone renal transplan-tation in 1991 and again in 1994, was admitted because of
worsening renal function and passage of tarry stool. He had been otherwise well except for ureteral tuberculosis 3 years earlier for which he was treated with a 12-month course of antituberculous therapy. He gave no history of travel outside of Taiwan and had been treated with prednisolone, azathio-prine and cyclosporine. Ten months earlier cyclosporine was replaced with FK-506 (tacrolimus) because of gradually worsening renal function. Serum creatinine was in the range of 8.3 to 9.6 mg/dL (normal value 0.6-1.2).
He developed cough, purulent sputum, and rhinorrhea without fever during the 2 weeks prior to admission. Physical examination was unremarkable. Chest radiogra-phy was reportedly negative. Cefaclor was given without benefit. In addition to passage of tarry stool, he had devel-oped a tongue ulcer.
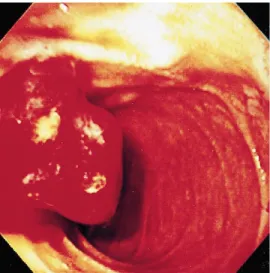
At admission, he appeared pale and looked chronically ill with mild respiratory distress. Temperature was 35.8°C, pulse rate 100/min, respiratory rate 28/min, and blood pressure 110/80 mm Hg. Oral candidiasis was found in addition to an indurated tongue ulcer of 0.8 × 0.8 cm. Hemoglobin was 4.9 gm/dL, white blood cell count 1.350 k/mm3, and platelet 10 k/mm3. Both serum albumin (nor-mal values in parentheses, 3.5-5.0) and globulin (2.3-3.5) were 2.6 gm/dL, blood urea nitrogen 207 mg/dL (4.5-24), creatinine 9.6 mg/dL (0.6-1.2), alkaline phosphatase 483 U/L (69-238), calcium 2.1 mmol/L (2.02-2.60), phosphate 6.6 mmol/L (2.7-4.5), sodium 131 mmol/L (135-148), and potassium 5.7 mmol/L (3.5-5.3). Chest x-ray showed increased interstitial infiltrates in both lung bases. Hemodialysis and transfusion of packed cells and platelets were instituted. On the second hospital day, endoscopy revealed erosion and bleeding in the antrum and a bleed-ing tumor was found at the main duodenal papilla (Fig. 1); biopsies were obtained. On the third hospital day, he devel-oped worsening respiratory distress without fever. Cefotetan was given pending results of blood and urine cultures and histopathologic evaluation of the biopsies. He became obtunded, was intubated for ventilator support because of respiratory failure and hypotension and was admitted to the intensive care unit. Despite the use of inotropic agents and resuscitation with intravenous fluids, hypotension ensued followed by ventricular arrhythmia. Cardiopulmonary resuscitation restored normal sinus rhythm. He became comatose thereafter and his family requested no further therapy. He was discharged against medical advice on the fourth day, intubated and on inotrop-ic agents. Histopathologinotrop-ic evaluation of the biopsies dis-closed ulceration with an inflammatory cell infiltrate, focal papillary hyperplasia, and yeastlike organisms inside his-tiocytes with hematoxylin and eosin staining and septated yeasts with Gomori-methenamine silver (GMS) stain (Fig. 2), consistent with P marneffei. Blood cultures subse-quently yielded P marneffei 1 week after death.
Case 2
A 52-year-old man was admitted because of intermit-tent fever, watery diarrhea, and abdominal pain for 3 weeks. He was diagnosed with AIDS three years earlier and had lived in Canton Province of China for 10 years. He
From the Departments of Internal Medicine and Emergency Medicine, Laboratory Medicine, and Pathology, National Taiwan University Hospital, Taipei, Taiwan.
Reprint requests: Jau-Min Wong, MD, Internal Medicine, National Taiwan University Hospital, No. 7, Chung-Shan South Road, Taipei, Taiwan 10017.
Copyright © 1999 by the American Society for Gastrointestinal Endoscopy 0016-5107/99/$8.00 + 0 37/4/96599
had been treated with trimethoprim-sulfamethoxazole, zidovudine and didanosine. Physical examination revealed a pale, feverish patient with a 1 ×0.5 cm erupted papule in the infraclavicular area. The liver was slightly enlarged. Ophthalmologic examination revealed findings consistent with cytomegalovirus retinitis. The rest of physical exami-nation was normal. Hemoglobin was 7.2 gm/dL and white blood cell count 2.92 k/mm3with 65.7% neutrophils. CD4 count was 20/mm3. Abnormal biochemistry tests (normal values in parentheses) were albumin 2.8 gm/dL (3.5-5.0); aspartate aminotransferase 50 U/L (<37); alkaline phos-phatase 385 U/L (67-238);γ-glutamyl transferase 171 U/L (<52); lactate dehydrogenase 548 U/L (230-460); amylase 151 U/L (<220); lipase 320 U/L (<190). Stool examinations of occult blood and parasite ova were nondiagnostic.
Barium enema showed a disorganized mucosa pattern with a mass effect at the terminal ileum. Colonoscopy revealed an 0.3 cm shallow cecal ulcer beside the ileocecal valve with edema and petechiae over the ileocecal valve
(Fig. 3). The mucosa of the rest of the colon appeared nor-mal. Histopathologic evaluation of biopsies from the ulcer showed diffuse histiocytic infiltrates with numerous intracellular yeast cells in the mucosa and lamina pro-pria. GMS and periodic acid-Schiff stains demonstrated scattered round to sausagelike fungi with central septa-tion that were consistent with P marneffei. Cultures of blood, bone marrow and skin all subsequently yielded P marneffei. Amphotericin B was given at a daily dose of 1 mg/kg for 2 weeks followed by itraconazole at a daily dose of 400 mg for maintenance therapy. He had no recurrence of bowel or systemic symptoms.
Case 3
A 30-year-old Chinese man from Thailand presented with dyspepsia, intermittent abdominal cramping pain and watery diarrhea for 2 months prior to admission. He also developed intermittent fever, bloody stool and a weight loss of 6 kg. Physical examination revealed a pale and emaciated patient with mild tenderness in the left lower abdomen. Liver and spleen were not enlarged. Hemoglobin was 10.5 gm/dL and white blood cell count was 4.34 k/mm3with 54% neutrophils and 15% lympho-cytes. Results of routine biochemical tests were normal except for serum albumin of 3.0 gm/dL. A test for antibody to HIV was positive. The stool contained no blood or mucus and microscopic examinations for parasites were negative. CT of abdomen showed mesenteric lym-phadenopathy and edematous small intestine. Colonos-copy revealed multiple solitary shallow ulcers with and without elevated margins in the cecum, ascending and transverse colons. The mucosa of the rest of the colon appeared normal. Biopsies from the ulcers showed muco-sal ulceration and infiltration of the lamina propria and mucosa by mononuclear cells, eosinophils, and markedly distended histiocytes laden with yeastlike microorgan-isms, suggestive of H capsulatum or P marneffei. GMS stain showed central septation of yeasts. Culture of the blood yielded P marneffei. Culture of bone marrow showed no growth of fungi. The patient was given amphotericin B
C-I Ko, C-C Hung, M-Y Chen, et al. Endoscopic diagnosis of intestinal penicilliosis marneffei
112 GASTROINTESTINAL ENDOSCOPY VOLUME 50, NO. 1, 1999
Figure 2. Microscopic appearance of a biopsy from the lesion in Figure 1 revealing septated yeast (arrow) inside his-tiocytes (Gomori-methenamine silver stain; orig. mag.×400), a finding characteristic of Penicillium marneffei.
Figure 3. Colonoscopic appearance of a shallow cecal ulcer in a patient with AIDS due to colonic penicilliosis marneffei. Figure 1. Endoscopic appearance of a bleeding tumor at
at a daily dose of 1 mg/kg for 2 weeks. Diarrhea, abdomi-nal pain and fever resolved promptly. Colonoscopy after 2 weeks of therapy revealed only two healing ulcers over the ileocecal valve; the rest of the colonic mucosa was normal. Colonic biopsies demonstrated complete clearance of yeast in the colonic mucosa. The patient was maintained on oral itraconazole at a daily dose of 400 mg and had no recur-rence of symptoms.
DISCUSSION
P marneffei can infect both healthy and
immuno-compromised individuals but the majority of the
cases are reported in patients with AIDS in areas
where the organism is endemic.
5-17In renal
trans-plant recipients receiving immunosuppressive
ther-apy, only one previous case of penicilliosis
marnef-fei has been reported.
18The most common
manifes-tations of disseminated penicilliosis marneffei in
patients with AIDS are fever, anemia, weight loss
and skin lesions. GI symptoms associated with
penicilliosis marneffei are relatively common.
14Diarrhea was present in 31% of patients with AIDS
and disseminated penicilliosis marneffei in a series
of 92 patients from Thailand
14and in 23.2% of
cases in another review of 155 HIV- and
non-HIV-infected patients.
16Despite the frequency of GI
symptoms, histopathologic documentation of GI
involvement with penicilliosis marneffei has rarely
been described.
8,9,12,15,17Including the 3 cases in the present report,
intesti-nal penicilliosis marneffei has been diagnosed in 7
patients by histopathology or culture of intestinal
tis-sues (Table 1).
8,9,12,17Intestinal involvement in cases
of disseminated penicilliosis may have been
under-diagnosed because the diagnostic yield of cultures of
blood, bone marrow, and skin are high enough to have
rendered investigation of intestinal tract by
endos-copy unnecessary. In contrast to diagnostic yields of
76%, 90%, and 100% for cultures of blood, skin
biop-sy, and bone marrow aspirate,
14respectively, the
organism has been infrequently isolated from stool
cultures. Only 6 cases with positive stool cultures for
P marneffei have been documented.
5,7,10-13The
sig-nificance of positive stool cultures remains unclear,
however, because in none of these cases was there
histopathologic evidence of intestinal penicilliosis.
Endoscopic diagnosis of intestinal penicilliosis marneffei C-I Ko, C-C Hung, M-Y Chen, et al.
VOLUME 50, NO. 1, 1999 GASTROINTESTINAL ENDOSCOPY 113
Table 1. Summary of clinical characteristics of 7 cases of intestinal penicilliosis marneffei
Underlying Involved organ
Case Age (yr)/ Area of disease/ Clinical or tissue Endoscopic Treatment/
[reference] gender report medications presentations (diagnostic methods)* findings maintenance† Outcome
1 [8] 0.33/M China NM Fever, diarrhea, Lymph nodes, liver, ND None Died
anemia, lung, bone marrow lymphadenopathy, spleen, bowel, kidney (A) hepatosplenomegaly
2 [9] 58/M Hong Kong Hemolytic Fever, anemia, Descending colon ND Amphotericin B Died anemia/ hepatosplenomegaly (C+H); liver,
steroids lung (A)
3 [12] 72/M Hong Kong AIDS Anorexia, Small intestine ND NM Died
dysphagia, (B+C);
weight loss, mesenteric lymph GI bleeding node, liver (A)
4 [17] 32/M Hong Kong AIDS Fever, diarrhea, Cecum, transverse Multiple Amphotericin B/ Survived night sweats, and descending solitary itraconazole
dry cough colon (B+C) ulcers
5 [PR] 33/M Taiwan Renal transplant Fever, diarrhea, Duodenum (B) Erosion at None Died
recipient/ septic shock, antrum and
cyclosporine, duodenal tumor ampulla Vater
azathioprine, with bleeding tumor with
steroids, bleeding
tacrolimus
6 [PR] 52/M Taiwan AIDS Fever, diarrhea, Skin, bone Shallow Amphotericin B/ Survived anemia, marrow (B+C); ulcers itraconazole
abdominal colon (B) pain
7 [PR] 30/M Taiwan AIDS Dyspepsia, Cecum, ascending Shallow Amphotericin B/ Survived diarrhea, fever, and transverse ulcers itraconazole
abdominal pain, colons (B) bloody stool,
weight loss
ND, Not done; NM, not mentioned; PR, present report.
*Diagnostic methods to demonstrate P marneffei were autopsy (A), biopsy (B), culture (C) or histopathology (H).
†Case 2 developed peritonitis after receiving amphotericin B for 4 days and died after surgical treatment. Case 4 received tericin B with a cumulative dose of 650 mg and maintenance therapy with itraconazole 400 mg/day. Cases 6 and 7 received ampho-tericin B with a daily dose of 1 mg/kg for 2 weeks and maintenance therapy with itraconazole 400 mg/day.
GI tract involvement by disseminated
penicillio-sis marneffei may range from esophagus
15to colon
(Table 1).
8,9,12,17Endoscopic findings include
shal-low ulcers that are not easily differentiated from
those of intestinal histoplasmosis.
4In this report,
we described another endoscopic finding of
intesti-nal penicilliosis marneffei, a bleeding tumor of the
main duodenal papilla, that has not been described
previously. Histopathologic examination of
speci-mens from the margins of the ulcers often discloses
lymphocytes and histiocytes distended with yeasts.
Microscopically, it is difficult to differentiate
intra-histiocytic yeast cells of P marneffei from those of
H capsulatum; outside of the histiocytes, the former
shows much more variation in morphology than the
latter.
6The demonstration of characteristic central
septation and elongated sausage-shaped forms by
GMS stain, and the absence of buds attached by a
narrow neck clearly distinguish P marneffei from
H capsulatum.
6The mortality rate for patients with P marneffei
infection is extremely high; the reported rate for
untreated HIV-infected patients with disseminated
penicilliosis marneffei was 75%.
19Delay in
diagno-sis and treatment is the most likely explanation for
the high mortality rate, therapy often being delayed
while awaiting microbiologic results for 1 or 2
weeks.
13The diagnosis of intestinal penicilliosis
marneffei as part of the presentation of
disseminat-ed penicilliosis may not be made until autopsy
(Table 1). In our patients the diagnosis was made by
endoscopy earlier than was possible by relying on
conventional microbiologic cultures and led to
suc-cessful therapy in 2 patients with AIDS although
the patient who underwent renal transplantation
died before antifungal therapy could be instituted.
Intestinal penicilliosis marneffei should be
included in the differential diagnosis of diarrhea
and fever in immunocompromised hosts who are
visitors to or residents of endemic areas.
Perfor-mance of endoscopy to obtain tissue specimens for
histopathology and culture may lead to earlier
diag-nosis and improve survival.
REFERENCES
1. Simon D, Brandt LJ. Diarrhea in patients with the acquired immunodeficiency syndrome. Gastroenterology 1993;105:1238-42. 2. Chui DW, Owen RL. AIDS and the gut. J Gastroenterol
Hepatol 1994;9:291-303.
3. Bonacini M, Nussbaum J, Ahluwalia C. Gastrointestinal,
hepatic, and pancreatic involvement with Cryptococcus
neo-formans in AIDS. J Clin Gastroenterol 1990:12:295-7.
4. Cappell MS, Mandell W, Grimes MM, Neu HC. Gastrointestinal histoplasmosis. Dig Dis Sci 1988;33:353-60.
5. So SY, Chau PY, Jones BM, Wu PC, Pun KK, Lam WK, et al. A case of invasive penicilliosis in Hong Kong with immuno-logic evaluation. Am Rev Respir Dis 1985;131:662-5. 6. Deng Z, Connor DH. Progressive disseminated penicilliosis
caused by Penicillium marneffei: report of eight cases and dif-ferentiation of the causative organism from Histoplasma
cap-sulatum. Am J Clin Pathol 1985;84:323-7.
7. Piehl MR, Kaplan RL, Haber MH. Disseminated penicilliosis in a patient with acquired immunodeficiency syndrome. Arch Pathol Lab Med 1988;112:1262-4.
8. Deng Z, Ribas JL, Gibson DW, Connor DH. Infections caused by Penicillium marneffei in China and Southeast Asia: review of eighteen published cases and report of four more Chinese cases. Rev Infect Dis 1988;10:640-52.
9. Tsang DNC, Chan JKC, Lau YT, Lim W, Tse CH, Chan NK.
Penicillium marneffei infection: an underdiagnosed disease?
Histopathology 1988;13:311-8.
10. Ma KF, Tsui MS, Tsang DNC. Fine needle aspiration diagno-sis of Penicillium marneffei infection. Acta Cytol 1991;35: 557-9.
11. Tsang DNC, Li PCK, Tsui MS, Lau YT, Ma KF, Yeoh EK.
Penicillium marneffei: another pathogen to consider in
patients infected with human immunodeficiency virus. Rev Infect Dis 1991;13:766-7.
12. Tsui WMS, Ma KF, Tsang DNC. Disseminated Penicillium
marneffei infection in HIV-infected subject. Histopathology
1992;20:287-93.
13. Hilmarsdottir I, Meynard JL, Rogeaux O, Guermonprez G, Datry A, Katlama C, et al. Disseminated Penicillium
marnef-fei infection associated with human immunodeficiency virus:
a report of two cases and a review of 35 published cases. J Acquir Immune Defic Syndr 1993;6:466-71.
14. Supparatpinyo K, Khamwan C, Baosoung V, Nelson KE, Sirisanthana T. Disseminated Penicillium marneffei infection in Southeast Asia. Lancet 1994;344:110-3.
15. Remadi S, Lotfi C, Finci V, Ismail A, Rogiano D, Vassilakos P, et al. Penicillium marneffei infection in patients infected with the human immunodeficiency virus: a report of two cases. Acta Cytol 1995;39:798-802.
16. Duong TA. Infection due to Penicillium marneffei, an emerg-ing pathogen: review of 155 reported cases. Clin Infect Dis 1996;23:125-30.
17. Leung R, Sung JY, Chow J, Lai CKW. Unusual cause of fever and diarrhea in a patient with AIDS: Penicillium marneffei infection. Dig Dis Sci 1996;41:1212-5.
18. Hung CC, Hsueh PR, Chen MY, Hsiao CH, Chang SC, Luh KT. Invasive infection caused by Penicillium marneffei: an emerging pathogen in Taiwan. Clin Infect Dis 1998;26: 202-3.
19. Supparatpinyo K, Nelson KE, Merz WG, Breslin BJ, Cooper CR, Kamwan C, et al. Response to antifungal therapy by human immunodeficiency virus infected patients with dis-seminated Penicillium marneffei infections and in vitro sus-ceptibilities of isolates from clinical specimens. Antimicrob Agents Chemother 1993;37:2407-11.
C-I Ko, C-C Hung, M-Y Chen, et al. Endoscopic diagnosis of intestinal penicilliosis marneffei