Original Articles
Treatment of Chronic Discogenic Pain by Utilizing Both
Nucleoplasty and Epidural Neuroplasty — One Year Follow-Up
Huan-Chieh Chen1, Yu-Ting Tai2,3, I-Jen Wang3,6,7, Woon-Man Kung1, Jia-Wei Lin4, Kuo-Sheng Hung1,5, Wen-Ta Chiu4,5, Tien-Jen Lin1,3,5
Objective: Both nucleoplasty and epidural neuroplasty have emerged as minimally
invasive techniques for treatment of low back pain and sciatica due to contained
herniated discs. Although there were some studies examining their effects on
functional activity and pain medications, the results of a combination of the two
procedures have not been analyzed as yet. The aim of our study was to evaluate the
outcome of a combination therapy in patients with chronic discogenic pain or
sciatica due to nerve root compression by a single-level, contained herniated disc.
Methods: Twenty-nine patients who had undergone the combination therapy of
both nucleoplasty and epidural neuroplasty were included in the analysis and were
evaluated at 3, 6, and 12 months postoperatively. They were asked to quantify their
pain using a visual analog scale ranging from 0 to 10. The Oswestry Disability Index
(ODI) was used to quantify disability by third-party observers. Patients were also
surveyed with regard to their use of pain medications. We compared the data at 3, 6,
and 12 months posttreatment to the baseline.
Results: There was a significant decrease in pain and use of medications in our study
group. The functional status was improved at 3, 6, and 12 months. There were no
complications associated with the procedure and we found continued improvements
over time in the study group.
Conclusion: Nucleoplasty and epidurolysis in combination appear to be safe and
effective in both early and later post-treatment periods. Further randomized,
controlled studies are required to evaluate the long-term efficacy of the combination
therapy.
Key words: discectomy, disc herniation, low back pain, minimally invasive,
nucleoplasty, percutaneous disc decompression, caudal neuroplasty and
epidurolysis
From the 1Department of Neurosurgery, 2Department of Anesthesiology, 3Pain Research Center, Taipei Medical University, Wan Fang
Hospital, Taipei, 4Department of Neurosurgery, Taipei Medical University, Shuang Ho Hospital, 5Graduate Institute of Injury Prevention
and Control, Taipei Medical University, 6Taipei Hospital, Department of Health, Taipei, 7Department of Health Risk Management,
China Medical University, Taichung
T
he general trend in spinal surgery, as in all other kinds of surgical treatment, toward reduction of varieties of devices utilized and minimization of surgery-related trauma, has led to the development of numerous minimally invasive percutaneous techniques for disc decompression and back pain management. Recently, percutaneous disc decompression using nucleoplasty has emerged as an effective, minimally invasive, percutaneous technique for the treatment oflow back pain due to contained herniated discs.1-4 This
procedure is attractive because it does not cause significant intraoperative or postoperative pain, is safe, and provides quick rehabilitation. The nucleoplasty
procedure utilizes Coblation technology1-4which serves
to decompress the disc using radiofrequency energy in a low-temperature environment that is less damaging to the surrounding tissues. The technique uses non-thermal ablation (coblation = controlled ablation) with a 10-20% reduction of the disk volume. This action occurs through an electrode positioned in the nucleus pulposus. By the application of radiofrequency energy to the tissue, breakdown of the molecular ligands produces a fluid with elementary molecules and low molecular weight gases, i.e. oxygen, nitrogen, hydrogen, carbon dioxide, etc. which are easily removed through the introducer needle. This technology using low temperatures (50-70°C) achieves results similar to those in thermal ablation, which uses high temperatures (150-200°C). Therefore, it is apparent that nucleoplasty produces minimal damages to the surrounding tissue, minimal thermal penetration, and a localized effect, in a shorter time period (2-3 min versus 15-17 min).
Epidural neuroplasty (lysis of epidural adhesions) is an interventional technique that was developed at the Texas Tech Health Sciences Pain Center in 1989. It is indicated when conservative management for spinal or radicular pain has failed. The technique is a minimally invasive therapy, where a catheter is placed directly at the herniated disc or the scar tissue compromising the nerve root. Local anesthetics, steroids, and normal saline are then injected through the catheter and the epidural catheter is removed. This procedure showed good results and was associated with only minor complications in a
recent prospective randomized blinded clinical trial.5
Focusing on epidural neuroplasty seems to be one of the promising minimally invasive techniques for adhesiolysis in patients with chronic sciatica with or without low back pain.
Back and leg pain originating from degeneration or wearing out of the lumbar intervertebral disc is called discogenic pain. Based on the long-standing theory that
Waddell6postulated in 1987, 80-90% of attacks of low
back pain will recover in about six weeks. Therefore, a symptom lasting for more than six weeks is thought to be chronic. Discogenic back pain can sometimes be successfully treated with medications and physical therapy. However, chronic discogenic pain which is severe and debilitating can also limit the individual’s ability to gain access to conventional treatment and within this same context, alternative therapy can be deemed as a treatment of choice.
At present, there are few studies supporting the long-term efficacy of percutaneous disc decompression utilizing nucleoplasty alone for the treatment of chronic discogenic pain, let alone in combination with epidural neuroplasty. Several studies have shown that nucleoplasty alone does effectively reduce pain in
patients with contained herniated discs.7,8Only one study
has so far examined the effect nucleoplasty has on functional activity, pain relief, and pain medication use.
However, this study did not analyze results over time.7,8
The problem of discogenic spinal pain is a result of a complex interplay between biomechanical and biochemical processes. Decompression of the disc alone may not satisfy the need for pain relief. The core theory of this combination therapy derived from reduction in intra-discal pressure by Coblation nucleoplasty and concomitant lessening in levels of inflammatory mediators released into the epidural space by epidural neuroplasty. In our report, the outcomes of 29 non-randomized patients treated with percutaneous disc decompression utilizing nucleoplasty in combination with epidural neuroplasty were examined with regard to the following parameters: reduction of pain over time, improvement in functional activity, and reduction of the use of analgesics longitudinally over 1 year in patients with radicular or axial low back pain secondary to contained herniated discs.
Patient selection
This retrospective study was conducted at the Department of Neurosurgery, Wan Fang Medical center, Taipei Medical University, Taipei, Taiwan. A total of 29 patients with a history of chronic low back pain and sciatica underwent both nucleoplasty and epidural neuroplasty between June and August 2007.
The inclusion criteria in our study were discogenic leg and back pain with MRI evidence of contained disc protrusion with a disk height ≥50%, after failed conservative therapy for 9 weeks. The exclusion criteria were disc height <50%, complete annular disruption
M
ethods
revealed by discography, more than 2 symptomatic levels, history of open disk surgery at suspected levels and moderate to severe spinal stenosis. Provocative discography was then conducted on all subjects following the Guidelines of the International Association for the Study of Pain and the International Spinal Injection Society. A concordant pain response accompanying the demonstration of the contained disc after performance of discography, with a painless response at an adjacent spinal level, became the foundation for inclusion in the study. The medical charts were reviewed, and pertinent data such as age, gender, history of drug and alcohol abuse, location of pain, levels of the performed procedure, duration of the procedure, pre- and post-procedural visual analog scale (VAS) pain scores, Oswestry Disability Index(ODI), and medication intake were carefully evaluated.
Procedures
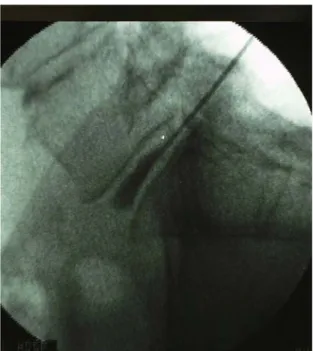
All patients were treated on an inpatient basis in the operating room of the surgery center. Percutaneous disc decompression using nucleoplasty was performed under monitored anesthesia care in the usual sterile fashion. Under fluoroscopic guidance with the patient in the prone position, a 17-gauge, 6-inch Crawford needle was advanced via a left or right posterolateral discography approach to the junction of the annulus and nucleus. The
needle was inserted on the same side as the patient's pain (that is, the side ipsilateral to the disc herniation).The Spine Wand (ArthroCare Spine, Inc., Sunnyvale, CA) was then inserted into the disc through the needle (Fig 1). The proximal and distal limits for intradiscal movement of the wand were identified, and disc decompression was started (Fig 2). After confirming desired placement, Coblation channels were created in the following sequence: The Spine Wand’s handle was turned to the “12 o’clock” position. Using the ablation mode, the Spine Wand was advanced to the pre-determined depth. The advancing of the Spine Wand was then stopped, and ablation was also discontinued at the depth of gauge. The Spine Wand was then withdrawn with exertion of coagulation mode. The Spine Wand was stopped from withdrawing when the reference mark was adjacent to the needle hub. The SpineWand’s handle was then rotated until it was at the “2 o’clock” position, and the same Coblation steps described above were performed. Additional channels at the 4, 6, 8, and “10 o’clock” positions were created. Therefore, at each level, a total of 6 channels were made circumferentially at the 12, 2, 4, 6, 8, and 10 o’clock positions. Every channel was created by advancement of the wand in the ablation mode and by its retraction in the coagulation mode. After withdrawal of the wand, no medication was injected, and the needle was removed. There were no complications and there
Fig 1. Lateral fluoroscopic images: positioning of the
Fig 2. The proximal and distal limits for intradiscal movement of the wand were identified, and disc
were no instances in which the intrathecal space was violated or increased resistance was noted.
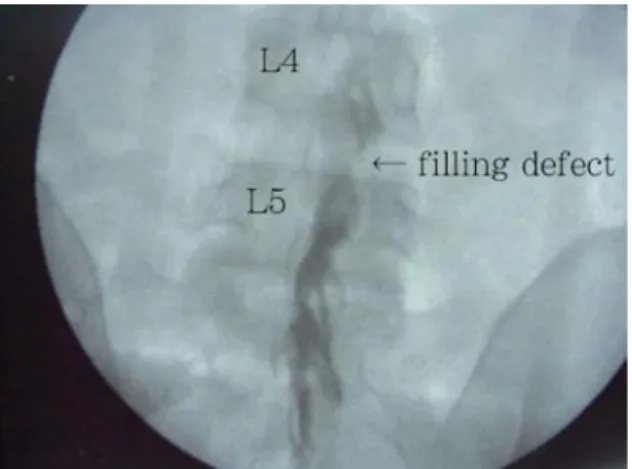
A caudal approach was selected to perform the epidural neuroplasty. The patient was still in the prone position with sterile drapes in place. A 15- or 16-gauge RKTM epidural needle was inserted via the sacral hiatus on the side opposite the suspected pathology after local anesthetic infiltration of the skin on the top of the gluteal fold. With confirmation of the correct placement of the needle in the epidural space, we injected 10 mL of iohexol (Omnipaque 240TM) after negative aspiration and visualized spread of the contrast medium (epidurogram). If a filling defect corresponding to the area of pain was present, we threaded a Racz catheter towards the filling defect (Fig 3). Confirmation of ventral placement of the catheter was done with the help of a lateral fluoroscopic view. After correct placement, 10 mL of preservative-free normal saline was injected into the filling defect. Injection of an additional 2 to 3 mL of iohexol to visualize the opening of the scarred area and to assure the spread of the injectate was within the epidural space. Both the needle and catheter were removed after injection of 4 ml of 40 mg/ml methylprednisolone.
Outcome measures
Patients were evaluated by an independent evaluator preoperatively and at 3, 6, and 12 months post-operatively. The data collected included VAS pain scores, pain medication intake, and Oswestry Disability Index, including changes in performance levels of activities of daily living. At each evaluation, patients were asked to quantify their overall pain using a VAS pain score ranging from 0 to 10. Good reasons for use of the VAS
included ease of use, previous validation and widespread use for measuring sensitivity to treatment effects, and its allowance for quantifiable statistical evaluations of significance.
Functional status
The Oswestry Disability Index (ODI), the most commonly used and recommended outcome measure tool, was used for assessing the disabling effects of lumbar spinal disorders.
Analgesic intake
Patients were also surveyed in regard to their use of analgesics. For the purposes of this study, the analgesic use was considered to be reduced if the patient reported complete termination of analgesics intake or a daily reduction of 50% or more.
Statistical analyses
Outcome measure data at the baseline were compared longitudinally with evaluations taken at 3, 6, and 12 months post-treatment. The Wilcoxon matched-pairs signed-ranks test was used for VAS pain score analysis. Furthermore, Fisher ’s exact test and the Wilcoxon ranks sum test were used to identify factors that were significantly associated with changes in other variables. All statistical tests were two-sided, and P values <0.05 were considered to be statistically significant.
Patient demographics and baseline data
Analysis of outcomes of percutaneous disc decompression utilizing nucleoplasty and epidural neuroplasty were performed on 29 patients (14 men, 15 women; 42±23 years of age). All patients gave written consent, and the study fulfilled the criteria of the ethics committee of Wan Fang Hospital.
Axial back pain was reported by 20% of patients, while 80% reported back and leg pain. Most patients (80%) had pain for more than 12-months. The mean procedure duration was 8 minutes per disc and 15 minutes for the epidural neuroplasty treatment.
Post-surgical outcomes
All patients were successfully treated without any significant complications during the procedure. No patient suffered pain caused by the Coblation procedure itself. Hospital stays ranged from 2 to 4 days, with an average of 2.14 days. The mean follow-up period was
R
esults
Formos J Surg 2010 • 43 • No 3
Fig 3. Anteroposterior view of correct placement of the catheter with confirmation by dye spread. Note that a filling defect was observed at the L4/5 disc space.
12±1.6 months.
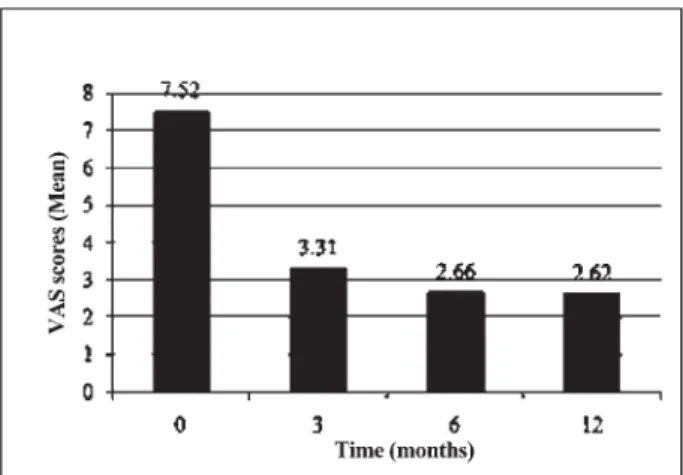
Mean VAS was reduced from a pre-procedure score of 7.52 to a post-procedure score of 3.31 at 3 months, 2.66 at six months and 2.62 at 12 months in the combination therapy group (Fig 4). Analgesic consumption was stopped or reduced in 20 patients at 3 months. Overall patient satisfaction was 81% at 3 months, 80% at 6 months, and 83% at the latest follow-up. Two patients were lost to 1 year follow-follow-up. Twelve months of follow-up showed that 16 patients were completely satisfied with the treatment (mean score 0-2) and had complete resolution of symptoms, 8 patients had satisfactory results (mean score 3-4), 3 patients had little benefit (mean score 5-7), and in 2 patients the results were completely unsatisfactory (mean score 8-9). VAS pain scores significantly decreased (VAS reduction more then 4 in scale) for 79.3%, 82.8%, and 86.2% of patients at 3, 6, and 12 months, respectively with a mean decrease of 4.21 (P<0.0001), 4.86 (P<0.0001), and 4.9 (P<0.0001) noted, respectively (Table 1).
The ODI decreased in treated patients with combination procedures from the pre-procedure score of 24.1±8.4 to the post-procedure score of 10.4±6.9 at 3 months, 10.6±7.3 at six months and 10.8±9 at 12 months.
The percentage of patients reporting a reduction in analgesic intake was 57.3% at 3 months (P<0.0001), 79.3% at 6 months (P<0.0001), and 80% at 12 months (P<0.0001).
Failure of treatment and complications
We did not find any significant factors related to failure of treatment. In our study, there were no intraoperative or postoperative complications associated with nucleoplasty and epidurolysis.
Pathological basis of discogenic pain
Discogenic pain is the result of a complex interplay of biomechanical and biochemical processes. Not only the nerve root is capable of pain sensation, because innervation of the ventral epidural space is extensive. Histopathological studies have demonstrated extensive sinuvertebral nerve and sympathetic innervation over this
confined space.9These structures may become highly
sensitized, resulting in chronic low back pain.
Intervertebral disc-related pain can be caused by structural abnormalities, such as degeneration or herniation. The first to create widespread interest in the disc as a source of pain in the American literature were
Mixter and Barr10 with their description of the herniated
nucleus pulposus. In a review of the literature, Benzon11
pointed out that abnormalities of the intervertebral disc include degeneration, bulging, and herniation. Bulging of the disc distends the posterior longitudinal ligament and causes localized back pain. If bulging of the disc increases, pressure may be exerted on the adjacent nerve roots, producing radicular pain.
Chemical irritation is also a major contributing factor in the origin of pain. Radicular pain can occur without disc herniation. Internal disc disruption, or IDD, is a condition in which the internal architecture of the disc is disrupted but its external surface remains essentially
intact.12Stolker13believed that mechanical factors are not
the only causative factors of radicular pain. Nerve roots
D
iscussion
Fig 4. Mean pain VAS scores post-treatment in one-year follow up.
may be exposed to chemical irritant substances from degenerated intervertebral discs or facet joints, which can
generate pain. Mixter and Ayers14 also demonstrated the
same conclusion. The leaked nucleus pulposus has been identified as a source of chemicals which produce
annoyance.15Substances that produce inflammation
include lactic acid, glycoprotein, cytokines, and histamine. In addition, it has been theorized that material from the nucleus pulposus might act as a foreign protein and trigger an autoimmune reaction.
The identification of fibrosis as the origin of low back pain has never been debated. In patients who had undergone prior surgeries, there was always some degree of perineural fibrosis. Although scar tissue itself was never tender, the nerve root was frequently very
sensitive. Kuslich et al.16suggested that the presence of
scar tissue compounded pain associated with the nerve root by fixing it in one position and thus increasing the susceptibility of the nerve root to tension or compression.
Conservative treatment for discogenic
pain
Treatment of discogenic pain usually involves prescription of opioids, non-steroidal anti-inflammatory drugs (NSAIDs) or physical therapy, but they may not be the optimal solution. Opioids may be addictive and patients may build up drug tolerance. NSAIDs have potentially dangerous side-effects, and physical therapy
may be ineffective.17,18Though NSAIDs for acute low
back pain usually work, the risks and benefits must be closely evaluated when NSAIDs are used in chronic
conditions.19,20 Moreover, many patients suffering with
chronic discogenic pain become refractory to medical management after some time. Minimally invasive techniques should therefore be made available to these patients.
Minimally invasive procedures
avail-able for disc decompression
Various interventions are designed to achieve disc decompression for pain relief. The most popular procedures are:
1. Chemonucleolysis: Dissolving nuclear proteoglycans by the injection of chymopapain was the first percutaneous technique used to treat radicular pain
caused by herniated nucleus pulposus.21 Available
since 1964, this technique has been associated with
long-term success rates between 66 and 88%.21
2. Automated percutaneous lumbar diskectomy (APLD):
In 1984, Onik et al22developed a method of removing
nuclear material through a 2 mm probe introduced through a 2.5 mm cannula. The early reports of a 75%
success rate led to its wide-spread use, but its use
declined after a randomized trial by Revel et al23
published in 1993, which compared chemonucleolysis with APLD and showed only a 33% success rate. 3. Laser diskectomy: Also in 1984, Choy et al (24)
reported on YAG laser diskectomy, a system based on intradiskal pressure reduction using laser energy introduced through a needle in the nucleus pulposus. This yielded success rates between 63 and 89%, with
pain relief lasting over 12 years.25
4. Intradiskal electrothermal annuloplasty (IDET): First performed in 1998, the procedure followed the concept of “annuloplasty,” in which thermal heating of the annulus seals annular tears and denervates the outer one third of the annulus by coagulation of the type C afferent nerve fibers. The outcome was favorable with
a success rate around 70%.26
However, all these percutaneous decompression approaches are considered to be related to potential complications, limitations, or poor outcomes. Chemonucleolysis using chymopapain digestion may lead to over-decompression due to difficulty in predicting the amount of the nucleus that would be digested and can cause paralysis due to transverse myelitis. Percutaneous lumbar diskectomy breaks annular integrity due to the substantial incision required to reach the nucleus. This may speed up future disc degeneration. Laser diskectomy is lengthy, requires bulky and expensive equipment, may impose endplate damage, and may elicit significant intraoperative and postoperative pain and spasm. Disadvantages of IDET are the potential hazard of annular perforation and the amount of intraoperative pain experienced by patients during the procedure secondary
to the thermal effect.27These potential risks have far
outweighed the potential benefit of these procedures.
The advantages of the combination
treatment
Our idea of treating discogenic low back pain is based on the decrease in intradiscal pressure using Coblation nucleoplasty and concomitant reduction in levels of inflammatory mediators released into the epidural space by epidural neuroplasty. Compared with other minimally invasive procedures, our treatment has minimal damages to the surrounding tissue, minimal thermal penetration with localized effect conducted in a shorter time period, leading to less intraoperative and postoperative pain, allowing quick rehabilitation. Our retrospective study of combined treatment demonstrated a statistically significant improvement in VAS pain scores and functional status and a reduction in medication intake in a group of patients with radicular or
axial low back pain who had failed conservative treatment.
Although other studies have also shown an overall reduction in pain scores following percutaneous disc decompression using nucleoplasty, these studies have only shown a general decline in pain relief over time. Interestingly, pain scores and medication use continued to decrease and functional status continued to improve in our patients over the 12-month follow-up period compared with other previous investigations. Pre-procedural discography provided substantial importance for assurance that no extravasations of contrast material were present and the concordant level of the disc to the origin of discogenic pain was the target before proceeding with the intervention thus allowing the result of the treatment to be optimum. While we believe the risk to be small, it should be taken under advisement while evaluating patient eligibility.
The limitation of our study
To the best of our knowledge, there are as yet no data from a randomized clinical study investigating whether this therapy is superior to treatment with physiotherapy. Our study has several limitations. The retrospective nature of this study is a disadvantage .The sample size is small and results may not be applicable to all patient populations. Despite these inherent shortcomings, the study does help to provide a preliminary outline for the planning of future prospective, randomized, controlled studies combining nucleoplasty with other minimally invasive interventional techniques.
The findings of this retrospective study suggest that nucleoplasty and epidural neuroplasty can be a safe and effective procedure for patients with radicular and axial low back pain secondary to contained herniated discs. Further prospective, randomized, controlled studies are needed to evaluate the long-term efficacy of percutaneous disc decompression and resolution of discogenic pain using both nucleoplasty and epidurolysis.
1. Sharps LS, Isaac Z: Percutaneous disc decompression using nucleoplasty. Pain Physician 2002;5:121-6.
2. Singh V, Piryani C, Liao K, et al: Percutaneous disc
250-9.
3. Singh V, Piryani C, Liao K: Evaluation of percutaneous disc decompression using coblation in chronic back pain with or without leg pain. Pain Physician 2003;6:273-80.
4. Reddy AS, Loh S, Cutts J, et al: New approach to the management of acute disc herniation. Pain Physician 2005;8: 385-90.
5. Veihelmann A, Devens C, Trouillier H, et al: Epidural neuroplasty versus physiotherapy to relieve pain in patients with sciatica: a prospective randomized blinded clinical trial. J Orthop Sci. 2006 Jul;11:365-9.
6. Waddell G: 1987 Volvo award in clinical science. A new clinical model for the treatment of low-back pain. Spine 1987;12:632-44.
7. Yakovlev A, Tamimi MA, Liang H, et al: Outcomes of Percutaneous Disc Decompression Utilizing Nucleoplasty for the Treatment of Chronic Discogenic Pain. Pain Physician 2007;10:319-28.
8. Masala S, Massari F, Fabiano S, et al: Nucleoplasty in the Treatment of Lumbar Diskogenic Back Pain: One Year Follow-Up. Cardiovasc Intervent Radiol 2007;30:426-32.
9. Cautico W, Parker JC Jr, Pappert E, et al: An anatomical and clinical investigation of spinal meningeal nerves. Acta Neurochir (Wien) 1988;90:139-43.
10. Mixter WJ, Barr JS: Rupture of the intervertebral disc with involvement of the spinal canal. N Eng J Med 1934;211:210-4. 11. Benzon HT: Epidural steroid injections for low back pain and
lumbosacral radiculopathy. Pain. 1986 Mar;24(3):277-95. 12. Crock HV: Isolated lumbar disc resorption as a cause of nerve
root canal stenosis. Clin Orthop Relat Res 1976;115:109-15. 13. Stolker RJ, Vervest AC, Groen GJ: The management of chronic
spinal pain by blockades: A review. Pain 1994;58:1-20. 14. Mixter WJ, Barr Js: Herniation or rupture of the intervertebral
disc into the spinal canal. J Neurosurgery 1964;21:74-81. 15. Racz GB, Noe C, Heavner JE: Selective spinal injections for
lower back pain. Curr Rev Pain 1999;3:333-41.
16. Kuslich SD, Ulstrom CL, Michael CJ: The tissue origin of low back pain and sciatica: A report of pain response to tissue stimulation during operation on the lumbar spine using local anesthesia. Orthop Clin North Am 1991;22:181-7.
17. Hawkey CJ, Cullen DJ, Greenwood DC, et al: Prescribing of nonsteroidal anti-inflammatory drugs in general practice: determinants and consequences. Aliment Pharmacol Ther 1997;11:293-8.
18. Brussen J: Physical therapy has little effect on acute low back pain. BMJ 1996;313:1262-3.
19. Van Tulder MW, Scholten RJ, Koes BW, et al: Nonsteroidal anti-inflammatory drugs for low back pain. Cochrane Database Syst Rev 2000; 2: CD000396.
20. Smith D, McMurray N, Disler P: Early intervention for acute back injury: can we finally develop an evidence-based
R
eferences
Formos J Surg 2010 • 43 • No 3
21. Smith L: Enzyme dissolution of the nucleus pulposus in humans. JAMA1964;187:137-40.
22. Onik G, Maroon J, Day A, et al: Automated percutaneous discectomy: Preliminary experience. Acta Neurochir Suppl (Wien), 1988;43:58-62.
23. Revel M, Payan C, Vallee C, et al: Automated percutaneous lumbar discectomy versus chemonucleolysis in the treatment of sciatica. A randomized multicenter trial. Spine 1993;18:1-7. 24. Choy DS, Case RB, Fielding W, et al: Percutaneous laser
nucleolysis of lumbar disks. N Engl J Med 1987;317:771-2. 25. Choy DS: Percutaneous laser disc decompression (PLDD): 352
cases with an 8 1/2-year follow-up. J Clin Laser Med Surg 1995;13:17-21.
26. Saal JA, Saal JS: Intradiscal electrothermal treatment for chronic discogenic low back pain: A prospective outcome study with minimum 1-year follow-up. Spine 2000;25:2622-7. 27. Freeman BJ, Fraser RD, Cain CM, et al: A randomized,
double-blind, controlled trial: Intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine 2005;30:2369-77.
Henrich Cheng
1. The treatment methods, essentially nucleoplasty and epidural neuroplasty, were developed and designed for different pathological conditions. Theoretically, combination of these two treatment methods must aim at those patients who were proved having these two pathological conditions.
2. According to the inclusion criteria, most patients were discogenic leg and back pain after failed conservative treatment for 9 weeks. Non patient has proved spinal or radicular pain caused by epidural adhesion.
3. There’s also no clear evidence the coblation nucleoplasty will cause the release of inflammation mediator into epidural place or even cause the epidural adhesion.
4. I think further high selection of patient and prospective study may actually prove the efficacy of this combination treatment.
1 2,3 3,6,7 1 4 1,5 4,5 1,3,5
29
0 10
Oswestry Disability Index ODI