18F-FDG PET for Evaluation of Bone Marrow Involvement in
Non-Hodgkin’s Lymphoma
A Meta-analysis
Yen-Kung Chen, MD, PhD,*† Chia-Lu Yeh, MD,* Chih-Cheng Tsui, MSc,* Ji-An Liang, MD,‡§
Jin-Hua Chen, PhD,¶ and Chia-Hung Kao, MD§
储
Background: In recent years, the use of 18F-fluorodeoxyglucose (FDG)
positron emission tomography/computed tomography (PET/CT) has become widespread for the staging of lymphoma. In non-Hodgkin lymphoma (NHL), the bone marrow (BM) involvement is a sign of extensive disease, and the iliac crest BM biopsy (BMB) is the established method for the detection of BM infiltration. However, iliac crest BMB is associated with a high rate of false-negative results. We assess the ability of FDG PET or PET/CT scan to ascertain the presence of BM involvement in aggressive and indolent NHL.
Methods: The authors conducted a systematic MEDLINE search of articles
published (last update, May 2010). Two reviewers independently assessed the methodological quality of each study. A meta-analysis of the reported sensitivity and specificity of each study was performed.
Results: Eight studies met the inclusion criteria. The studies had several
design deficiencies. Pooled sensitivity and specificity for the detection of non-Hodgkin’s aggressive lymphoma were 0.74 (95% CI, 0.65– 0.83) and 0.84 (95% CI, 0.80 – 0.89), respectively. Pooled sensitivity and specificity for the detection of non-Hodgkin’s indolent lymphoma were 0.46 (95% CI, 0.33– 0.59) and 0.93 (95% CI, 0.88 – 0.98), respectively.
Conclusions: The diagnostic accuracy of FDG PET or PET/CT scans was
slightly higher but without significant statistical difference (P⫽ 0.1507) in patients with non-Hodgkin’s aggressive lymphoma as compared with those with non-Hodgkin’s indolent lymphoma. The sensitivity to detect indolent lymphoma BM infiltration was low for FDG PET or PET/CT.
Key Words: aggressive non-Hodgkin’s lymphoma, indolent lymphoma,
bone marrow involvement, PET/CT, FDG (Clin Nucl Med 2011;XX: 000 – 000)
L
ymphoma is the most common form of hematological malig-nancy, or “blood cancer,” in the developed world. Subtypes of lymphoma differ in molecular characteristics and biologic behavior. Compared with Western regions, Asian countries have been reported to have higher rates of non-Hodgkin’s lymphoma (NHL) and a low incidence of Hodgkin’s lymphoma.1On the basis of the clinical
characteristics, this entity is divided into aggressive and indolent types. The most important factors influencing therapeutic decisions and prognosis are histologic subtype and extent of disease.2
Bone marrow biopsy (BMB) is an important part of the routine staging of lymphoma. Bone marrow (BM) involvement by lymphoma confers advanced-stage disease and may affect both treatment and prognosis. Histologic evidence of lymphoma in the BM is found in approximately 50% to 80% of patients with low-grade and 25% to 40% of high-low-grade NHL.3
18
F-fluorodeoxyglucose (18
F-FDG) positron emission tomogra-phy (PET) in the staging and restaging of patients with lymphoma has a median sensitivity of 90.3% and a median specificity of 91.1%, respectively.4
In another meta-analysis, a good, but not excellent cor-relation was demonstrated between18
F-FDG PET focal uptakes and BMB in the detection of BM involvement in the staging of patients with malignant HL and NHL lymphoma.5
However, it is still under discus-sion whether18
F-FDG PET (or PET/CT, computed tomography) can reduce the need for staging iliac BMB.6,7
So, we further analyzed the accuracy of18
F-FDG PET or PET/CT in detecting BM infiltration in aggressive (high grade) and indolent (low grade) NHL.
MATERIALS AND METHODS
Data Search
A search of the biomedical literature was performed by 2 researchers (Y.K.C. and C.H.K.) working independently, using the PubMed/MEDLINE and EBM Review search engines to identify stud-ies involving human subjects (Fig. 1). Each researcher used searches with last update of May 2010. They used the combination of search terms “lymphoma” “bone marrow,” and “positron emission tomogra-phy.” There was no language restriction. Additional studies were manually searched using the references of the retrieved articles. A total of 163 potential studies were retrieved from these searches.
Data Selection
Studies were eligible for inclusion based on the following crite-ria: (1) they evaluated lymphoma staging, non-Hodgkin’s lymphoma, including aggressive and/or low-grade (indolent) lymphoma, (2) bone involvement and/or BM infiltration, and (3) FDG PET and/or PET/CT images. Studies were excluded based on the following criteria: (1) only Hodgkin’s lymphoma, (2) non-Hodgkin’s lymphoma, without further description of subtype, (3) totals of true positives, false positives, true negatives, and false negatives were not provided, and (4) no data from a subanalysis were provided. Unpublished data and conference pro-ceedings were not included. On the basis of these criteria, 8 studies were eligible for this study.
Data Extraction
Two reviewers independently assessed the methodological quality of the selected studies. The criteria list recommended by the Cochrane Methods Working Group on Systematic Review of Screening and Diagnostic Tests was used. Some items on the list
Received for publication October 8, 2010; revision accepted November 17, 2010. From the *Department of Nuclear Medicine and PET Center, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan; †School of Medicine, Fu Jen Catholic University, Taipei, Taiwan; ‡School of Medicine, China Medical University, Taichung, Taiwan; §Department of Radiation Therapy and On-cology, China Medical University Hospital, Taichung, Taiwan; ¶Biostatistics Center and Graduate Institute of Biostatistics, China Medical University, Taichung, Taiwan, and储Department of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung, Taiwan.
J.H.C. and C.H.K. contributed equally to this work.
Supported by the study projects (DMR-97–103, DMR-97–104) in our hospital and Taiwan Department of Health, Cancer Research Centers for Excellence (DOH99-TD-C-111– 005).
Reprints: Chia-Hung Kao, MD, Department of Nuclear Medicine and PET Center, China Medical University Hospital, No. 2, Yuh-Der Rd, Taichung 404, Taiwan. E-mail: [email protected].
Copyright © 2011 by Lippincott Williams & Wilkins ISSN: 0363-9762/11/0000-0001
Clinical Nuclear Medicine • Volume XX, Number XX, XXX 2011 www.nuclearmed.com | 1
AQ: 1
AQ:5
were modified for this specific review. The complete criteria list used is presented in Table 1. Internal validity criteria (IV) were scored as “positive” (adequate methods), “negative” (inadequate methods, potential bias), or “unclear” if insufficient information had been provided on a specific item. External validity criteria (EV) were assessed to evaluate generalizability. Standard performance of FDG PET or PET/CT was scored positive when the type of PET or PET/CT camera, the dose of FDG, the time between injection and scanning, and the method of reconstruction were described. The
criteria for external validity were scored positive if sufficient infor-mation was provided to judge generalizability of findings. After the consensus meeting, we decided to score unclear scores as negative. Agreement between both reviewers was quantified by Cohen’s.8
Quality scores were expressed as a percentage of the maximum score. Subtotals were calculated for internal (maximum 6) and external (maximum 6) validity separately.
Statistics Analysis
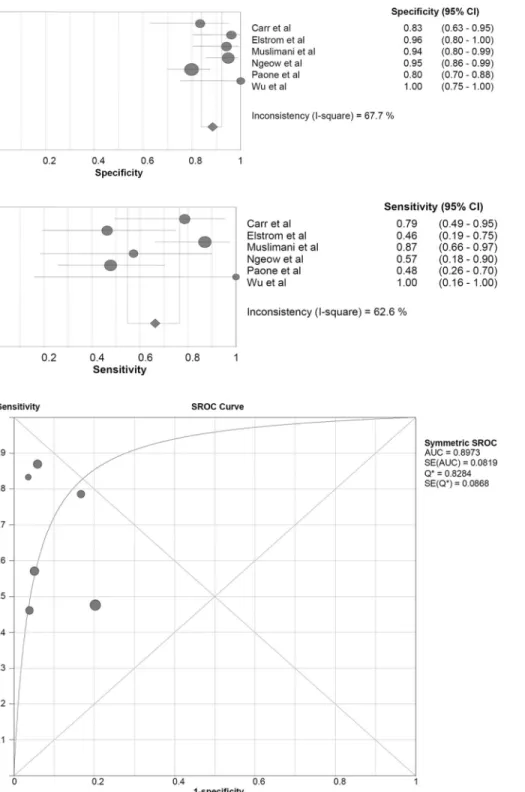
Data on sensitivity, specificity, positive predictive value, and negative predictive value of FDG PET or PET/CT in the detection of BM infiltration were calculated from the original numbers given in the publications. The datasets were pooled by adding the TP, FP, TN, and FN results from all relevant studies and finding the sensitivity and specificity for the combined data. A 95% confidence interval was constructed for these estimates by assuming that each of the sensitivity and specificity results was a simple proportion from a normal distribution. Overall weighted average for sensitivity and specificity was calculated for comparison with the results of the pooled data using random effect model. When estimation of sensi-tivities and specificities for an individual study was a least one zero cell, a correction of 1/2 was added to every cell for that study to make the estimators defined. Exploring heterogeneity other than threshold effect was performed using I-square which measures the degree of heterogeneity between studies. Figures 2 and 3 show the moderate inconsistency level of I-squares of sensitivities and spec-ificities in aggressive and indolent non-Hodgkin’s lymphoma, re-spectively. In addition, exploring heterogeneity due to threshold effect was performed using Spearman correlation coefficient. In aggressive non-Hodgkin’s studies, the threshold effect was not existent (P⫽ 0.872). There was a threshold effect among indolent group studies. We attempted to fit each set of data to a summary receiver operating characteristic (sROC) curve and the area under sROC curve was calculated. The maximum joint sensitivity and specificity (Q* index) that measured the overall diagnostic accuracy was estimated. Q* is the point where the sensitivity and specificity are equal. An sROC curve is used when the slope of the linear regression is within a prespecified range (⫺0.5–0.5). When appli-cable, the mean threshold for each group of studies was determined, and the sensitivity and specificity at that point on the curve were
FIGURE 1. Selection of studies. Inclusion
criteria: (1) lymphoma staging, non-Hodg-kin’s lymphoma, including aggressive and/or low grade (indolent) lymphoma, (2) bone involvement and/or BM infiltration, (3) FDG PET and/or PET/CT images. Exclu-sion criteria is as follows: (1) only Hodgkin’s lymphoma, (2) non-Hodgkin’s lymphoma, not further describe subtype, (3) totals of true positives, false positives, true negatives, and false negatives were not provided, and (4) no data from a subanalysis were pro-vided.
TABLE 1. Criteria List Used to Assess the Methodological Quality of the Studies
Criteria of Validity Positive Score
Internal validity
Valid reference test Histology, bone marrow biopsy
Blind measurement of FDG-PET without knowledge of reference test
Blind measurement of reference test without knowledge of FDG-PET
Avoidance of verification bias Assessment by reference test independent of FDG-PET results
FDG-PET interpreted independently of all clinical information
Mentioned in publication
Prospective study Mentioned in publication
External validity
Spectrum of disease Primary stage of disease
Demographic information Age and gender information
given
Inclusion criteria Mentioned in publication
Exclusion criteria Mentioned in publication
Avoidance of selection bias Consecutive series of patients Standard execution of FDG-PET Type of camera, dose FDG,
time interval, reconstruction
FDG indicates 18F Fluorodeoxyglucose; PET, positron emission tomography.
T1
AQ:2
provided. Overall values were also obtained by pooling of datasets, along with determining weighted averages for each of these sets of data. Statistical analyses were executed using Meta-Disc, a free statistical software package, version 1.4 (Unit of Clinical Biostatis-tics, Ramo´n y Cajal Hospital, Madrid, Spain).
RESULTS
Literature Search
A total of 163 studies about initial staging of lymphoma with FDG PET and associated with bone involvement were identified (Fig.
1). After reviewing the titles and abstracts, 155 studies were excluded. These studies included Hodgkin’s lymphoma, reviews, case reports, studies reporting on the use of FDG PET for response evaluation to chemotherapy. Of the remaining 12 studies, data of one study did not differentiate between Hodgkin’s and non-Hodgkin’s lymphoma, data of 2 studies did not classify non-Hodgkin’s lymphoma into high grade and low grade, and 1 study was excluded because of insufficient informa-tion to construct a 2⫻ 2 table. Eight studies met the inclusion criteria (Table 1). The characteristics of the included studies are presented in Table 2.
FIGURE 2. Individual study estimates
of sensitivity and specificity of aggres-sive non-Hodgkin’s lymphoma.
FIGURE 3. Summary ROC curves and
95% confidence intervals of aggres-sive non-Hodgkin’s lymphoma.
Methodological Quality Assessment
Methodological quality was assessed by 12 items for each of the 12 selected studies. There was disagreement in 40 of 144 scores with a Cohen’s of 0.70. Main disagreement was in the questions IV3 and IV5. Disagreements were caused by reading errors and differences in interpretation. The scores for internal and external validity of the 12 selected studies are presented in Table 2. All studies had a valid reference test, but some studies (37.5%) did not describe whether the reference test was interpreted without knowl-edge of the FDG PET findings. In 6 (75%) of the 8 studies, verification bias was avoided because patients were selected for assessment by the reference test independently of the FDG PET results (IV4). Four studies were prospective (50%), and in 4 studies (50%), patients entered the study consecutively. In all of the selected studies (100%), primary stage of disease was in-cluded. In all studies (100%), the inclusion criteria were de-scribed, and only in a minority of studies were the exclusion (25%) criteria described. The total score for the combined inter-nal and exterinter-nal validity, expressed as a fraction of the maximum score, ranged from 58% to 75%, with a median of 68.9%. Seven of the 8 studies had a total score above 60%.
Diagnostic Accuracy of FDG PET or PET/CT
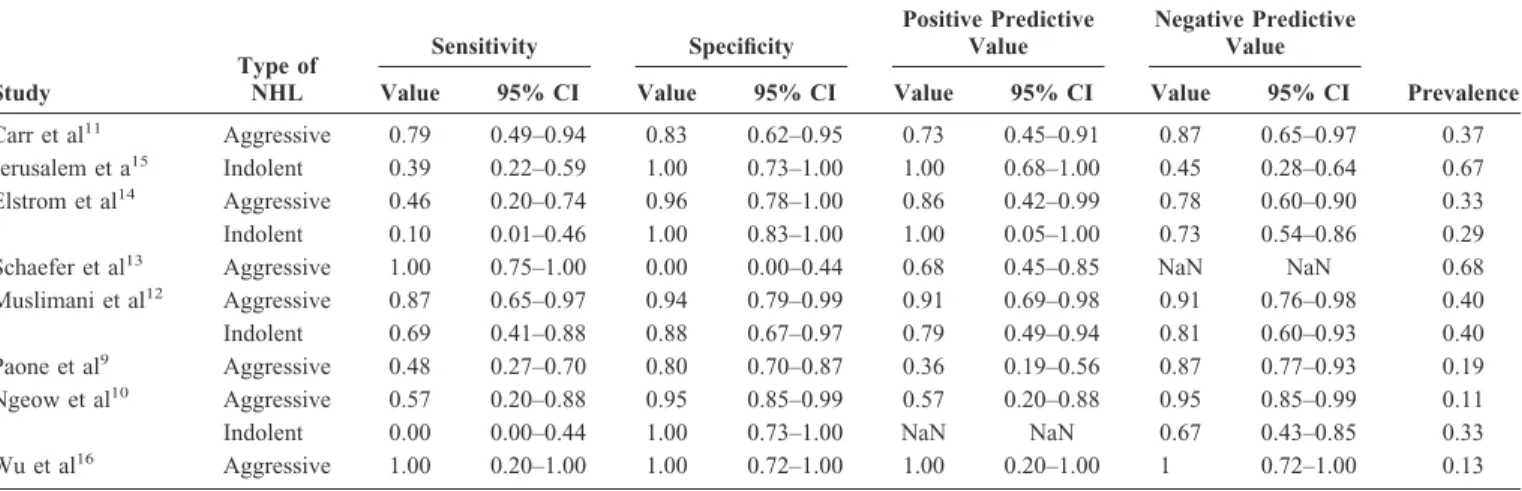
The data of each study and the results of the statistical pooling are presented in Table 3. Among the studies with patient-based data of aggressive non-Hodgkin’s lymphoma, the median sensitivity was
79% (range, 46%–100%) and the median specificity was 94% (range, 0%–100%) (Table 3). The summary (pooled) true-positive rate (sensitivity) was 74% (Table 4) and the summary of false-positive rate was 11.2%. The maximum joint sensitivity and speci-ficity, a global measure of diagnostic accuracy, was 81.3%. Among the studies with patient-based data of indolent non-Hodgkin’s lym-phoma, the median sensitivity was 24.5% (range, 0%– 69%) and the median specificity was 100% (range, 88%–100%) (Table 3). The summary (pooled) true-positive rate (sensitivity) was 46% (Table 4) and the summary false-positive rate was 4.5%. The maximum joint sensitivity and specificity, a global measure of diagnostic accuracy, was 75.6%.
DISCUSSION
The results of this meta-analysis indicate that FDG PET or PET/CT has a high diagnostic accuracy for the evaluation of BM involvement in non-Hodgkin’s aggressive lymphoma patients. The summary sensitivity was 74% and the summary specificity was 84%. The summary sensitivity was found to be higher in patients with non-Hodgkin’s aggressive lymphoma compared with patients with non-Hodgkin’s indolent lymphoma. The summary specificity was found to be slightly higher in patients with non-Hodgkin’s indolent lymphoma compared with patients with non-Hodgkin’s aggressive lymphoma.
TABLE 2. Quality Assessment of the 8 Diagnostic Studies Included in the Present Review
Study IV EV Total IV Score Total EV Score % of Maximum Score IV1 IV2 IV3 IV4 IV5 IV6 EV1 EV2 EV3 EV4 EV5 EV6
Carr et al11 ⫹ ⫹ ⫹ ⫹ ⫺ ⫹ ⫹ ⫺ ⫹ ⫺ ⫹ ⫹ 5 4 75 Jerusalem et al15 ⫹ ⫹ ⫹ ⫹ ⫺ ⫹ ⫹ ⫺ ⫹ ⫺ ⫹ ⫹ 5 4 75 Elstrom et al14 ⫹ ⫹ ⫹ ⫹ ⫺ ⫺ ⫹ ⫺ ⫹ ⫹ ⫺ ⫹ 4 4 67 Schaefer et al13 ⫹ ⫹ ⫺ ⫺ ⫹ ⫺ ⫹ ⫹ ⫹ ⫺ ⫹ ⫹ 3 5 67 Muslimani et al12 ⫹ ⫹ ⫺ ⫺ ⫺ ⫺ ⫹ ⫹ ⫹ ⫹ ⫺ ⫹ 2 5 58 Paone et al9 ⫹ ⫹ ⫺ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫺ ⫺ ⫹ 5 4 75 Ngeow et al10 ⫹ ⫹ ⫹ ⫹ ⫺ ⫹ ⫹ ⫹ ⫹ ⫺ ⫺ ⫺ 5 3 67 Wu et al16 ⫹ ⫹ ⫹ ⫹ ⫺ ⫺ ⫹ ⫹ ⫹ ⫺ ⫺ ⫹ 4 4 67
NOTE. IV1-IV6, 6 criteria for internal validity (IV; see Table 1); EV1-EV6, 6 criteria for external validity (EV; see Table 1).
TABLE 3. Parameters of Diagnostic Accuracy of18F FDG PET or PET/CT for the Detection of Bone Marrow Infiltration
Study Type of NHL Sensitivity Specificity Positive Predictive Value Negative Predictive Value Prevalence Value 95% CI Value 95% CI Value 95% CI Value 95% CI
Carr et al11 Aggressive 0.79 0.49–0.94 0.83 0.62–0.95 0.73 0.45–0.91 0.87 0.65–0.97 0.37
Jerusalem et a15 Indolent 0.39 0.22–0.59 1.00 0.73–1.00 1.00 0.68–1.00 0.45 0.28–0.64 0.67
Elstrom et al14 Aggressive 0.46 0.20–0.74 0.96 0.78–1.00 0.86 0.42–0.99 0.78 0.60–0.90 0.33
Indolent 0.10 0.01–0.46 1.00 0.83–1.00 1.00 0.05–1.00 0.73 0.54–0.86 0.29
Schaefer et al13 Aggressive 1.00 0.75–1.00 0.00 0.00–0.44 0.68 0.45–0.85 NaN NaN 0.68
Muslimani et al12 Aggressive 0.87 0.65–0.97 0.94 0.79–0.99 0.91 0.69–0.98 0.91 0.76–0.98 0.40
Indolent 0.69 0.41–0.88 0.88 0.67–0.97 0.79 0.49–0.94 0.81 0.60–0.93 0.40
Paone et al9 Aggressive 0.48 0.27–0.70 0.80 0.70–0.87 0.36 0.19–0.56 0.87 0.77–0.93 0.19
Ngeow et al10 Aggressive 0.57 0.20–0.88 0.95 0.85–0.99 0.57 0.20–0.88 0.95 0.85–0.99 0.11
Indolent 0.00 0.00–0.44 1.00 0.73–1.00 NaN NaN 0.67 0.43–0.85 0.33
Wu et al16 Aggressive 1.00 0.20–1.00 1.00 0.72–1.00 1.00 0.20–1.00 1 0.72–1.00 0.13
NaN (Not a Number) is a value of numeric data type representing an undefined or unrepresentable value, especially in floating-point calculations.
T3
The meta-analysis by Pakos et al5
reported 13 eligible non-overlapping studies: 4 studies recruited patients with HD, 3 studies had patients with NHL, and 6 studies had mixed populations. The weighted rates showed significantly better sensitivity in studies with HD than in those with NHL patients. However, in NHL, there was a clear difference in sensitivity depending on the histologic type. On the basis of the available data, 18
F-FDG PET identified 16 of 21 cases of BM involvement (76.2%) from large lymphocytic, large B-cell, Burkitt, and centroblastic lymphocytic lymphomas, whereas it detected only 16 of 53 cases with BM involvement (30.2%) from less aggressive histologic types (follicular, mantle cell, marginal zone, small lymphocytic lymphomas, and mucosa-associated lym-phoid tissue). Otherwise, the study of Paone et al9
revealed that 21 patients with diffuse large B-cell lymphoma had BM involvement. Only 10 patients (48%) had abnormal BM FDG uptake, 6 of the 7 with a prominent component of large transformed lymphoid cells, and 4 of the 14 with lymphoid infiltrates composed of small cells. The study of Ngeow et al10
showed maximum standardized uptake value⬎10 may predict for an aggressive histology. In a patient with an indolent lymphoma, sites with standardized uptake value⬎10 suggest the possibility of transformation or the possibility of pres-ence an aggressive component in addition to what is suggested by the histology. Except for indolent B-NHL, PET scans have a good overall negative predictive value in excluding lymphomatous BM involvement.
Unilateral BMB is the standard approach in the staging of the bone marrow. It has been recognized as an imperfect tool for a long time. Several large studies have consistently shown that a unilateral iliac crest trephine biopsy is an unreliable method of detecting marrow lymphoma, especially in high-grade NHL.11
Studies exam-ining the yield of a bilateral biopsy have shown that a unilateral biopsy would miss 20% of cases compared with a bilateral bi-opsy.7,17
BMB removes a small core of marrow and, therefore, is subject to sampling errors. It is clear proof of the limitations of BMB as a proposed gold standard. Cases with BM infiltration missed by unilateral biopsies might be mostly those with less extensive BM infiltration. In their study, Muslimani et alstudies12
revealed that PET scan for detecting BM involvement specificity may be spuri-ously low, as a result of the fact that of the 11 PET⫹/BMB⫺ patients, 5 patients did not have directed biopsy to the site of involvement detected by the 18
F-FDG PET scan, whereas the 6 patients who had directed biopsy were positive. In addition, the study of Schaefer et al13
revealed 50 (28 NHL) patients, 18 (36%) had direct biopsy of FDG-avid lesion in the bone. All direct bone biopsies of FDG-avid lesions revealed lymphomatous infiltration. Therefore,18
F-FDG PET can be used to direct the site of the biopsy, and image-guided repeat BMB should be considered in patients with negative initial iliac crest BMB, whose PET demonstrates BM involvement in a different site.12
BMB is generally safe but should not be thought of as a risk-free procedure. Adverse events (hemor-rhage, infection, etc) are reported in about 0.12% of cases.18
It is also a painful and stressful procedure even with good local anesthe-sia and sedation.
False-positive BM involvement on the 18
F-FDG PET scan due to chemotherapy, granulocyte colony-stimulating factor admin-istration,19
infection/inflammation, and hyperplastic marrow must be excluded as they may increase the18
F-FDG uptake and lead to a false-positive 18
F-FDG PET scan.12
False-negative BM involve-ment on the18
F-FDG PET scan may be due to relatively low FDG uptake per cell or to diffuse, low-density marrow involvement by tumor.14
In patients with diffuse large B-cell lymphoma, the lack of FDG uptake in patients with lymphoid infiltrates composed of small cells can be attributed to a lack of uptake by the cells of these infiltrates which are small atypical lymphocytes with only rare large transformed lymphoid cells.9
Routine reading of CT provided the correct anatomic local-ization of FDG-avid lesion and has a low yield in depicting bone/ born marrow lesions, because criteria for disease involvement by CT scan are usually based on the size of a lesion.14
Schaefer et al examined a selected population of 50 lymphoma patients (28 NHL) with FDG-avid bone lesions on PET/CT. On CT, only 32 of the 193 lesions (16.6%) were detected without the PET information. In 161 lesions (83.4%), only focal increased FDG uptake in the bone was observed on PET/CT, without morphologic alteration of osseous structures on CT images.13
In patients with positive FDG PET/CT and negative BMB, CT-guided BMBs at the involvement sites detected by the FDG PET/CT scan were recommended.12
There are several potential limitations to conducting a meta-analysis of diagnostic tests. The presence of clinical heterogeneity (heterogeneity originated by the inclusion of patients at different stages of disease and other clinical characteristics) affects the gen-eralizability of the results and it is not necessarily ruled out by the lack of statistical heterogeneity. It is important to note that the majority of the studies included a mix of patients with Hodgkin disease, non-Hodgkin lymphoma, and non-Hodgkin lymphoma with different cell types. Studies reported on B/BM lesions together and did not try to make a clear-cut distinction between bony involvement and BMI in every patient and for each lesion.6
Furthermore, due to the nature of this disease, biopsy results were available in only a few studies; the majority had to rely on clinical follow-up, including a variety of imaging modalities and clinical examinations, not all of which were performed in the same manner in all the studies. The use of an imperfect reference standard, together with variability in the quality of the primary studies, introduces important limitations for the interpretation of this meta-analysis. In addition, the verification bias potentially present in the primary studies cannot be fully addressed in a meta-analysis. Nevertheless, despite these limitations, meta-analytic techniques have been very useful for demonstrating the significant role of FDG PET or PET/CT imaging in the diagnosis and staging of several malignancies.
The results from this literature review and meta-analysis suggest that the diagnostic accuracy of FDG PET or PET/CT is slightly higher but without significantly statistical difference (P⫽ 0.1507) in patients with non-Hodgkin’s aggressive lymphoma (ac-curacy: 81%) than in those with non-Hodgkin’s indolent lymphoma (accuracy: 76%) (Table 4). The overall high specificity of FDG PET
TABLE 4. Meta-analysis of Sensitivity and Specificity Data
Type of Scan Type of NHL No. TP FP TN FN
Pooled Sensitivity (95% CI) Pooled Specificity (95% CI) Accuracy (95% CI) PET Aggressive 134 37 7 77 13 0.74 (0.62–0.86) 0.92 (0.86–0.98) 0.85 (0.79–0.91) PET/CT Aggressive 237 67 29 117 24 0.74 (0.65–0.83) 0.80 (0.74–0.87) 0.78 (0.72–0.83)
PET or PET/CT Aggressive 321 67 36 194 24 0.74 (0.65–0.83) 0.84 (0.80–0.89) 0.81 (0.77–0.86)
PET or PET/CT Indolent 156 26 7 92 31 0.46 (0.33–0.59) 0.93 (0.88–0.98) 0.76 (0.69–0.82)
or PET/CT in patients with non-Hodgkin’s aggressive lymphoma and indolent lymphoma were 84% and 93%, respectively. FDG PET or PET/CT scan shows potential to detect BM involvement in non-Hodgkin’s aggressive lymphoma, which would otherwise be missed by iliac crest BMB. Furthermore, FDG PET or PET/CT can be used to directly guide the site of the biopsy, when PET demon-strates BM involvement in a different site. However, the overall sensitivity of FDG PET or PET/CT in patients with non-Hodgkin’s indolent lymphoma was only 46%. In FDG-negative cases of indo-lent lymphoma, a BMB is probably still warranted.
REFERENCES
1. Lee MY, Tan TD, Feng AC, Liu MC. Clinicopathological analysis of malignant lymphoma in Taiwan, defined according to the World Health Organization classification. Haematologica. 2005;90:1703–1705.
2. Weiler-Sagie M, Bushelev O, Epelbaum R, et al. 18
F-FDG avidity in lymphoma readdressed: a study of 766 patients. J Nucl Med. 2010;51: 25–30.
3. McKenna RW. The bone marrow manifestations of Hodgkin’s disease, the non-Hodgkin lymphomas, and lymphoma-like disorders. In: Knowles DM, ed. Neoplastic Hematopathology. Baltimore, MD: Williams & Wilkins; 1992:1135.
FIGURE 4. Individual study estimates
of sensitivity and specificity of indo-lent non-Hodgkin’s lymphoma.
FIGURE 5. Summary ROC curves and
95% confidence intervals of indolent non-Hodgkin’s lymphoma.
F4-5 AQ: 4
4. Isasi CR, Lu P, Blaufox MD. A metaanalysis of18
F-2-deoxy-2-fluoro-D-glucose positron emission tomography in the staging and restaging of patients with lymphoma. Cancer. 2005;104:1066 –1074.
5. Pakos EE, Fotopoulos AD, Ioannidis JP. 18F-FDG PET for evaluation of bone marrow infiltration in staging of lymphoma: a meta-analysis. J Nucl
Med. 2005;46:958 –963.
6. Pelosi E, Penna D, Deandreis D, et al. FDG-PET in the detection of bone marrow disease in Hodgkin’s disease and aggressive non-Hodgkin’s lym-phoma and its impact on clinical management. Q J Nucl Med Mol Imaging 2008;52:9 –16.
7. Moulin-Romsee G, Hindie´ E, Cuenca X, et al.18F-FDG PET/CT bone/bone
marrow findings in Hodgkin’s lymphoma may circumvent the use of bone marrow trephine biopsy at diagnosis staging. Eur J Nucl Med Mol Imaging 2010;37:1095–1105.
8. Brennan P, Silman A. Statistical methods for assessing observer variablility in clinical measures. BMJ. 1992;304:1491–1494.
9. Paone G, Itti E, Haioun C, et al. Bone marrow involvement in diffuse large B-cell lymphoma: correlation between FDG-PET uptake and type of cellular infiltrate. Eur J Nucl Med Mol Imaging. 2009;36:745–750.
10. Ngeow JY, Quek RH, Ng DC, et al. High SUV uptake on FDG-PET/CT predicts for an aggressive B-cell lymphoma in a prospective study of primary FDG-PET/CT staging in lymphoma. Ann Oncol. 2009;20:1543–1547. 11. Carr R, Barrington SF, Madan B, et al. Detection of lymphoma in bone
marrow by whole-body positron emission tomography. Blood. 1998;91: 3340 –3346.
12. Muslimani AA, Farag HL, Francis S, et al. The utility of 18-F-fluorodeoxy-glucose positron emission tomography in evaluation of bone marrow involve-ment by non-Hodgkin lymphoma. Am J Clin Oncol. 2008;31:409 – 412. 13. Schaefer NG, Strobel K, Taverna C, et al. Bone involvement in patients with
lymphoma: the role of FDG-PET/CT. Eur J Nucl Med Mol Imaging. 2007; 34:60 – 67.
14. Elstrom R, Guan L, Baker G, et al. Utility of FDG-PET scanning in lymphoma by WHO classification. Blood. 2003;101:3875–3876.
15. Jerusalem G, Beguin Y, Najjar F, et al. Positron emission tomography (PET) with 18F-fluorodeoxyglucose (18F-FDG) for the staging of low-grade non-Hodgkin’s lymphoma (NHL). Ann Oncol. 2001;12:825– 830.
16. Wu HB, Wang QS, Wang MF, et al. Utility of 18F-FDG PET/CT for staging NK/T-cell lymphomas. Nucl Med Commun. 2010;31:195–200.
17. Wang J, Weiss LM, Chang KL, et al. Diagnostic utility of bilateral bone marrow examination: significance of morphologic and ancillary technique study in malignancy. Cancer 2002;94:1522–1531.
18. Bain BJ. Bone marrow biopsy morbidity and mortality: 2002 data. Clin Lab
Haematol. 2004;26:315–318.
19. Moog F, Bangerter M, Kotzerke J, et al. 18-F-fluorodeoxyglucose-positron emission tomography as a new approach to detect lymphomatous bone marrow. J Clin Oncol 1998;16:603– 609.