Suitability of the WHOQOL-BREF
for community-dwelling older
people in Taiwan
H
EI-F
ENH
WANG1, W
EN-M
IINL
IANG2, Y
UN-N
INGC
HIU3, M
AU-R
OUNGL
IN3 1Department of Nursing, National Taipei College of Nursing, Taipei, Taiwan, ROC 2Department of Public Health, China Medical College, Taichung, Taiwan, ROC3Institute of Injury Prevention and Control, College of Public Health and Nutrition, Taipei Medical University, Taipei, Taiwan, ROC
Address correspondence to: M.-R. Lin, Institute of Injury Prevention and Control, Taipei Medical University, 250 Wu-Hsing St., Taipei 110, Taiwan, ROC. Fax: (+886) 2 273 90387. Email: [email protected]
Abstract
Background: while life expectancy among older people has been lengthened due to improved public health and med-ical interventions, the importance of health-related quality of life in later life has also increased. However, the applica-tion of a generic health-related quality of life measure for older people needs to be carefully validated.
Objective: to evaluate the practicality, reliability, validity, and responsiveness of the use of the brief version of the World Health Organization Quality of Life for people aged 65 years or older.
Design: a prospective study.
Methods: for a baseline assessment, 1200 community-dwelling older people living in Shin-Sher Township of Taichung County, Taiwan, completed the brief version of World Health Organization Quality of Life at their residences either by themselves or with the assistance of an interviewer. Furthermore, score changes in each health-related quality of life domain after a fall were followed up for assessing its responsiveness.
Results: the average length of time required to complete the questionnaire was short (10.6 minutes for self-administration and 15.3 minutes for personal interview), and the score distribution in each domain was symmetrical with no Xoor or ceiling effect. Furthermore, all domain scores indicated excellent discriminant validity, construct validity, and responsiveness as well as good internal consistency and intra- and inter-observer test-retest reliabilities. Nevertheless, two items related to work capacity and sexual activity had higher missing values (4.5% and 16.5%) and poor inter-observer test-retest reliabilities (0.43 and 0.20). Suggested modiWcations to the two items for older people are discussed.
Conclusion: with a few modiWcations, the brief World Health Organization Quality of Life is a suitable health-related
quality of life instrument for older people.
Keywords: older people, health-related quality of life, psychometrics, Taiwan, WHOQOL-BREF
Introduction
While life expectancy among older people has been extended due to improved public health and medical interventions, the importance of the health-related qual-ity of life (HRQL) in later life has also increased. Health-related quality of life is a broad, multidimen-sional construct that includes at least the domains of physical, psychological, and social health, according to the World Health Organization (WHO) [1]. Since an ill-ness or some treatment often has an impact on multiple aspects of health among older people (e.g. hip fracture due to a fall may cause immobility, fear of falling, and
reduction of social activities), HRQL measures may help construct a comprehensive health proWle of older people after they experience an illness or undergo some treatment [2, 3].
However, several aspects of the measurement need to be considered when applying a generic HRQL measure to older people. First, compared with young people, the respondent’s burden in completing a questionnaire needs to be reduced for older people because of physical frailty, a higher proportion of illiteracy, or cognitive impairment in this population. Furthermore, even when readability is no problem, older people often take more time to complete a questionnaire. Second, the items and domains in a
at Taipei Medical University Lib. on March 22, 2011
ageing.oxfordjournals.org
HRQL measure should take into account the aspects of life identiWed as important by older people – for example, access to health services and environmental safety [4]. Although older people may consider similar HRQL aspects to be relevant and important to health as do younger people, the relative importance and deWnition of each domain or facet (e.g. role functioning may be deWned in terms of roles other than work) may differ substantially [5, 6]. Third, Xoor values of HRQL meas-ures may appear common among older people if the measures are directly used with no adaptation [7 ]. Floor effects can reduce the ability to detect distinguishing fea-tures, for instance, between ill and well people, and the ability to detect changes in HRQL scores over time or after a health intervention [8].
The brief version of the World Health Organization’s Quality of Life (WHOQOL-BREF), one of the generic HRQL measures, contains two items from the Overall Quality of Life and General Health facet and one item from each of the remaining 24 facets [9]. These facets are categorised into four major domains: Physical Capacity (7 items), Psychological Well-being (6 items), Social Rela-tionships (3 items), and Environment (8 items). The Taiwanese version of the WHOQOL-BREF was devel-oped in compliance with WHO guidelines [10, 11], and excellent reliability and validity of this version have been reported as well [12, 13]. In addition to comprising 26 items translated from the original WHOQOL-BREF, the Taiwanese version includes two additional items of local importance, i.e. being respected and food availability [12, 13]. The two local items are categorised into the Social relationships (being respected) and Environment (food availability) domains, respectively.
The suitability of neither the original nor the Taiwanese version of the WHOQOL-BREF has been evaluated for older people, and therefore, this study was conducted to examine its use with community-dwelling people aged 65 years or over in Taiwan.
Materials and methods
Study subjects
This study is a part of a fall-related prospective study (Effect-iveness of Tai-Chi Chuan on Reduction of Elderly Falls). Shin-Sher Township, located in Taichung County in west-central Taiwan, is a residential area with a high pro-portion of older people, so it is suitable place to conduct a community intervention study of older people. The percentage of residents aged 65 or older in Shin-Sher Township was 11.9% in 1999, compared to 8.6% for Taiwan as a whole [14]. Out of 13 villages in the town-ship, the six villages with the largest elderly populations were selected. All people in Taiwan are required to regis-ter as residents at a local Household Registration OfWce, and the household registration programme is designed to
collate and to supply demographic information and ofW-cially to recognise personal status and relations. There-fore, based on records in the Shin-Sher Household Registration OfWce, 2072 people aged 65 or older in the six villages, with information on name, address, birth date, gender, and education, were identiWed at the begin-ning of the study.
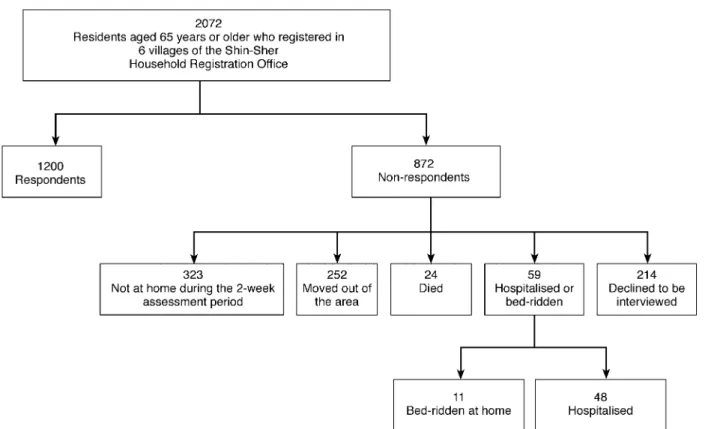
During a 2-week assessment period, 1200 eligible subjects agreed to participate in the study. Of the 872 subjects who did not participate, 24 had died, 59 were hospitalised or bed-ridden, 252 had moved out of the area, 323 were not at home during the assessment period, and 214 declined to be interviewed. A diagram of the study population is shown in Figure 1. Furthermore, compared with non-respondents, the respondents had similar distributions of gender and educational level, but tended to be younger (P = 0.073).
Procedures
Trained interviewers conducted personal interviews with structured questionnaires at a subject’s residence to col-lect related information. Interview procedures and inter-viewer attitudes were standardised through participation in a 4-hour training course. Postcards were mailed to these older people in order to describe the study purpose and to notify them of our visits to the community. Each sub-ject was Wrst asked whether he/she was willing to self-administer the Taiwan version of the WHOQOL-BREF, and if not, a personal interview was carried out. As a result, only 86 subjects self-administered the WHOQOL-BREF. The length of each interview was timed regardless of whether it was self- or interviewer-administered.
In addition, information on age, gender, educational level, chronic co-morbid conditions, depression, and cognitive status was collected as well. Co-morbidity was assessed in more detail using a list of 24 chronic co-morbid conditions that are likely to affect the elderly. The level of depression was assessed using a short form of the 15-item Geriatric Depression Scale (GDS) [15, 16], with a GDS score of higher than 10 being indicative of depression [17]. Cognitive status was assessed using the Mini-Mental State Examination (MMSE) [18, 19]. Commonly used in epidemiological studies, this ques-tionnaire assesses the cognitive status of subjects with respect to orientation, registration, recall of information, attention and calculation, language, and visuospatial construction. MMSE scores were categorised by scoring conventions applied in the Epidemiologic Catchment Area Study, with scores of 0–17 indicating cognitive impairment [20].
Fall status was used as an external indicator to assess the responsiveness of the WHOQOL-BREF. During the 3-month follow-up period, 24 subjects experienced a fall. For comparison, 200 subjects were randomly selected from those who had not fallen in the 3-month follow-up period. The WHOQOL-BREF was re-administered to these subjects 3 months after the above assessment.
at Taipei Medical University Lib. on March 22, 2011
ageing.oxfordjournals.org
Ten non-fallers did not complete the re-administration due to hospitalisation, death, or not being at home.
Scoring of the WHOQOL-BREF
As with the original WHOQOL-BREF (the WHOQOL group), the Taiwanese version of the WHOQOL-BREF was scored over four domains: Physical Capacity (7 items), Psychological Well-being (6 items), Social Relationship (4 items), and Environment (9 items). All items were rated on a 5-point scale with a higher score indicating a higher quality of life. A sample of Wve items is listed in the Appendix. Domain scores were calculated by mul-tiplying the mean of all facet scores included in each domain by a factor of 4, and accordingly, potential scores for each domain ranged from 4–20.
Responses from the two items of the Overall Quality of Life and General Health facet were calculated as a single score with a range of 4–20, as with the scoring method for the four domain scores. However, this single facet score was not used by the WHOQOOL group.
Practicality
The length of time required to complete the WHOQOL-BREF, the percentage of respondents with missing val-ues for each item, and the distributions of minimum and maximum possible domain or facet scores (i.e. Xoor and ceiling values) were used to evaluate the respondent bur-den, difWculty of completion, and a problematic score
distribution, respectively. Furthermore, differences in the time length, missing values, and score distributions were also examined among different age and gender groups.
Internal consistency and test-retest reliability
Cronbach’s alpha [21] was used to examine the internal consistency of the four domains in the WHOQOL-BREF. In addition, a random stratiWed sample by village of 60 subjects was selected to assess their original res-ponses within 2 weeks. One-half of the sample was retested for estimating intra-observer reliability and the other for inter-observer reliability. Intraclass correlation coefW-cients [22] were calculated for both types of test-retest reliability.
Discriminant validity
The ability of each domain score in the WHOQOL-BREF to distinguish healthy and unhealthy people as well as three common co-morbid statuses, including falls, depression, and cognitive impairment, was evaluated by Student’s t-test after controlling for age. Lower domain scores among subjects who had had a fall, depression, or cognitive impairment were expected.
Construct validity
A four-domain solution for both the original WHOQOL-BREF and the Taiwanese version of the
Figure 1. A diagram of older people in the six villages of the Shin-Sher Township, Taichung Country, Taiwan
at Taipei Medical University Lib. on March 22, 2011
ageing.oxfordjournals.org
WHOQOL-BREF has been suggested [9, 11], with items relating to each domain loading onto that particular domain (see Table 1). ConWrmatory factor analysis was applied to validate whether the four-domain structure is suited to older people, and a Bentler’s comparative Wt index of 0.9 or higher indicates an acceptable level of suitability for that solution [23].
In addition, a focus group session of eight elderly sub-jects with higher educational levels such as a senior high school diploma or a college degree was conducted to dis-cuss the meaningfulness of all items in the WHOQOL-BREF to older people. In addition, they were encouraged to list additional items speciWcally for older people.
Responsiveness
The WHOQOL-BREF was administered again to these subjects 3 months after the initial assessment. The respon-sive statistics for the four domains and the overall quality of life and general health facet were calculated by the mean change in scores for that domain over the 3-month period among the 24 people who had fallen, divided by the standard deviation of score changes among the 190 subjects who had not fallen during that period [24, 25]. Furthermore, a meaningful responsiveness of 0.2–0.5 was considered small effect, 0.5–0.8 moderate effect, and >0.8 large effect [26].
SAS (Statistical Analysis Software) version 6.12 and LISREL version 8 were used for statistical analyses.
Results
The ages of these 1200 subjects ranged from 65 to 103 years with an average of 73.4. Furthermore, 709 (59%) of the subjects were males, 766 (66%) lived with a spouse, and 387 (37%) had no formal education. Of 821 subjects who reported having physician-diagnosed chronic co-morbid conditions, 353 (43%) had one chronic condition, 225 (27%) had two chronic conditions, and 243 (30%) had at least three chronic conditions. Furthermore, of the 127 (11%) subjects reported to have had at least one fall in the past year, 181 (15%) of the GDS scores were higher than 10 points, and 220 (18%) of the MMSE scores were lower than 18 points.
For the 86 subjects who were willing to self-administer the WHOQOL-BREF, the average time for completing it was 11 minutes (i.e. three items per minute) with a range of 4–20 minutes. On the other hand, for those who received a personal interview, the average time taken to complete it was 15 minutes (i.e. two items per minute) with a range of from 8 to 32 minutes. Furthermore, no signiWcant differences in the length of time of the interview were detected among different age groups (data not shown).
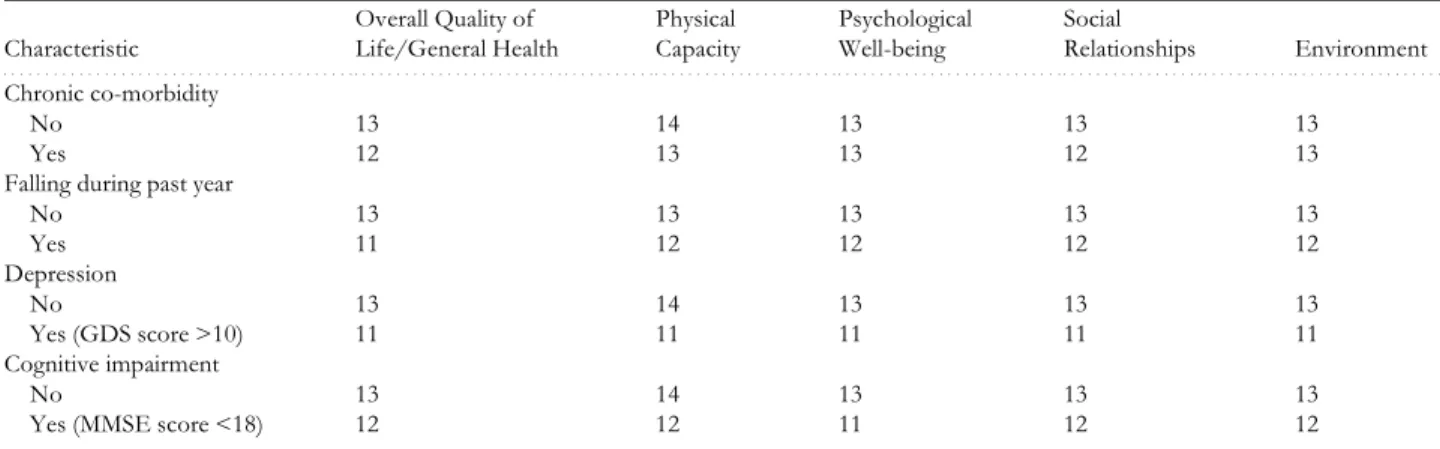
Table 2 presents score distributions for the four domains and the Overall Quality of Life and General Health facet of the WHOQOL-BREF. The average domain scores were 13 for Physical Capacity, 13 for Psy-chological Well-being, 13 for Social Relationships, and 13 for Environment. For each domain score, the median was close to the mean, indicating that the distributions of Table 1. Discriminative validity analysis: means of age-adjusted domain or facet scores by characteristica
aBased on Student’s t-test; all P-values are smaller than 0.01.
Characteristic Overall Quality of Life/General Health Physical Capacity Psychological Well-being Social Relationships Environment . . . . Chronic co-morbidity No 13 14 13 13 13 Yes 12 13 13 12 13
Falling during past year
No 13 13 13 13 13 Yes 11 12 12 12 12 Depression No 13 14 13 13 13 Yes (GDS score >10) 11 11 11 11 11 Cognitive impairment No 13 14 13 13 13
Yes (MMSE score <18) 12 12 11 12 12
Table 2. Score distributions of four domains and the Overall Quality of Life and General Health facet of the WHOQOL-BREF among 1200 older people in Taiwan
aStandard deviation.
Domain or facet Mean ± SDa Median % of Xoor value % of ceiling value % of missing range
. . . .. . . .
Overall Quality of Life/General Health 13 ± 3 12 0.2 0.8 0.50–0.75
Physical Capacity 13 ± 2 13 0.1 0.2 0.08–2.50
Psychological Well-being 13 ± 2 13 0.3 0.3 0.08–0.83
Social Relationships 13 ± 2 12 0.1 0.1 0.50–16.5
Environment 13 ± 2 13 0.0 0.0 0.25–0.83
at Taipei Medical University Lib. on March 22, 2011
ageing.oxfordjournals.org
these domain scores were nearly symmetrical (although the Shapiro-Wilk test for normality produced a P-value of <0.05 for all domain scores). The percentage of the ceiling or Xoor value in each domain score was very low, ranging from 0 to 0.8%. However, percentages of the ceiling values for items 3, 4, and 26 in the WHOQOL-BREF were 31%, 21%, and 18%, respectively, while it was 3% for the remaining 25 items (data not shown). Those three items were framed in an opposite manner compared to the others. While the missing percentages for most items were lower than 1%, it was 17% for the Sexual Activity facet (item 21) and 3% for the Work Capacity facet (item 18). Older subjects had more missing values in these two facets, and females had more in the Sexual Activity facet. Furthermore, a lower number of missing values was observed in self-administered forms than in the personal interviews with the exception of the Sexual Activity facet (21% versus 16%).
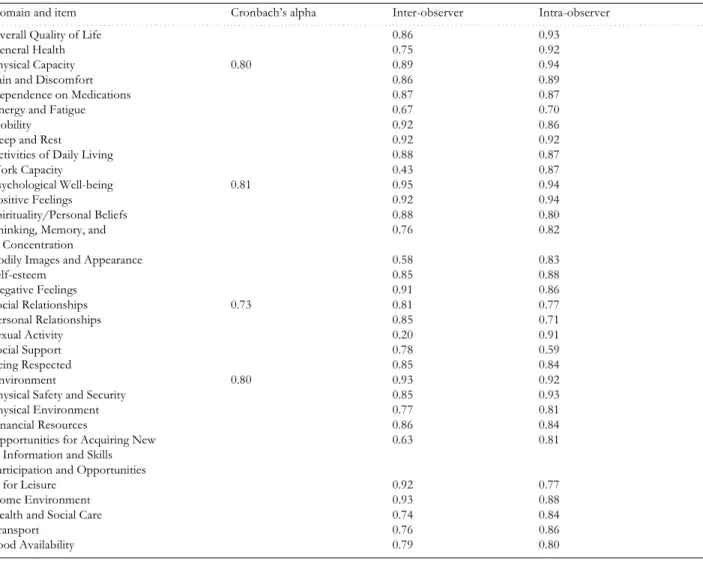
As shown in Table 3, Cronbach’s alpha coefWcients ranged from 0.73 to 0.81, indicating good internal con-sistency among these particular items within a domain. While the intraclass correlation coefWcients of inter- or
intra-observer reliability for most items were equal to or higher than 0.58, the coefWcient of the inter-observer reliability was 0.20 for the Sexual Activity facet and 0.43 for the Work Capacity facet. Differences between inter-and intra-observer reliabilities indicate that an interviewer effect may have appeared in the subject’s responses to these two items.
Table 1 presents the results of the discriminant valid-ity analysis. After adjusting for age, scores in all four domains and the Overall Quality of Life and General Health facet among older people who had a chronic co-mor-bid condition, a fall, depression, or cognitive impairment were signiWcantly lower than those who did not.
The initial conWrmatory factor analysis of testing a structure of four independent domains shows that Bentler’s comparative Wt index was 0.85, indicating that the four independent domains with particular items was not adequately Wt for older people. The index increased to 0.90 when three pairs of error variances were allowed to covary (i.e. Pain and Discomfort, and Dependence on Medications; Mobility, and Participation and Opportunities for Leisure; Home and Social Care, and Transport) and Table 3. Cronbach’s alpha coefWcients for internal consistency and intraclass correlation coefWcients for inter- and intra-observer test-retest reliabilities of the WHOQOL-BREF among 1200 older people in Taiwan
Domain and item Cronbach’s alpha Inter-observer Intra-observer
. . . .. . . .
Overall Quality of Life 0.86 0.93
General Health 0.75 0.92
Physical Capacity 0.80 0.89 0.94
Pain and Discomfort 0.86 0.89
Dependence on Medications 0.87 0.87
Energy and Fatigue 0.67 0.70
Mobility 0.92 0.86
Sleep and Rest 0.92 0.92
Activities of Daily Living 0.88 0.87
Work Capacity 0.43 0.87
Psychological Well-being 0.81 0.95 0.94
Positive Feelings 0.92 0.94
Spirituality/Personal Beliefs 0.88 0.80
Thinking, Memory, and
Concentration
0.76 0.82
Bodily Images and Appearance 0.58 0.83
Self-esteem 0.85 0.88 Negative Feelings 0.91 0.86 Social Relationships 0.73 0.81 0.77 Personal Relationships 0.85 0.71 Sexual Activity 0.20 0.91 Social Support 0.78 0.59 Being Respected 0.85 0.84 Environment 0.80 0.93 0.92
Physical Safety and Security 0.85 0.93
Physical Environment 0.77 0.81
Financial Resources 0.86 0.84
Opportunities for Acquiring New Information and Skills
0.63 0.81 Participation and Opportunities
for Leisure 0.92 0.77
Home Environment 0.93 0.88
Health and Social Care 0.74 0.84
Transport 0.76 0.86
Food Availability 0.79 0.80
at Taipei Medical University Lib. on March 22, 2011
ageing.oxfordjournals.org
two items were allowed to cross-load on other domains (i.e. Self-esteem on Social Relationships and Energy and Fatigue on Psychological Well-being). Therefore, the four-domain solution was also Wt for older subjects.
In the focus group discussion, subjects self-interpreted the meaning for most items similarly to the deWnitions of the WHOQOL. However, they perceived sexual activi-ties as ‘sexual intercourse activiactivi-ties’. Furthermore, most of these subjects perceived work activities as ‘doing things in daily living’, even though they did not have paid employment.
Based on Guyatt’s method, the responsiveness effect sizes were –1.42 for Physical Capacity, –0.80 for Psycho-logical Well-being, –0.46 for Social Relationships, and –0.71 for Environment [24, 25]. Furthermore, the effect size for the Overall Quality of Life and General Health facet was –0.56. Therefore, according to Cohen’s criteria [26], the responsiveness was large in the Physical Capacity and Psychological Well-being domains and moderate in the Social Relationships and Environment domains as well as in the Overall Quality of Life and General Health facet.
Discussion
This study demonstrates that the WHOQOL-BREF is a suitable HRQL instrument for older people in terms of small respondent burden, ease of use, and nearly sym-metrical distribution of domain scores, even though a few modiWcations, discussed below, are needed. In add-ition, several psychometric properties such as validity, reliability, and responsiveness were sufWciently satisfac-tory for this population as well.
Although the high missing rates for items 21 and 18 somewhat reXect problems related to sexual and work activities among older people, statements for the two items (‘How satisWed are you with your sex life?’ and ‘How satisWed are you with your capacity for work?’) may need to be modiWed in order to improve the applicability of the WHOQOL-BREF for older people. To avoid a misunderstanding or an incorrect perception by older persons and even interviewers, the statement for item 21 could be revised to explicitly reXect its deWnition con-cerning a person’s urges and desires for sex. For instance, ‘How satisWed are you with your sex life, including
inti-mate behaviour other than sexual intercourse?’ Alterna-tively, the item could be replaced by another item in the Social Relationships domain of the full version of the WHOQOL questionnaire. Some reasons for using an alternative include: a substantial proportion of older people who live without a spouse (e.g. 34% in this study) may be unable or unwilling to answer the item. In add-ition, despite older Taiwanese being extremely reluctant to express their sexual desires [10] possibly because the cultures of Confucianism, Taoism, and Buddhism all dis-courage older people from having such desires. Also, reluctance or difWculty in answering the item might not speciWcally occur only for older Taiwanese. It was found that a substantial proportion of cancer patients in the United Kingdom (19%) and patients with chronic liver disease in the Netherlands (12–21.9%) did not answer items about sexuality either, while the missing value rates in remaining items were <5% [27, 28].
As for item 18, despite many older people possibly automatically self-interpreting work-related activities as ‘doing things in daily living’, perhaps due to multiple connotations of the Chinese characters, a modiWcation to the original question such as ‘How satisWed are you with your capacity for engaging in daily activities?’ is suggested. Only a few existing generic quality of life measures explicitly include the environment as a dimension of health-related quality of life. However, the importance of the environment for the quality of life in older people has been identiWed and recognised for a long time. For instance, the environment is strongly associated with life quality among older people with respect to fall prevention, social interaction, activity involvement, independence, safety and security, and psychological well-being [29–33]. Furthermore, adequate environmental modiWcations can maximise the capacities of older people and compensate for the decline in function that occurs with the ageing process or with chronic co-morbidity [34]; for example, a higher ambient temperature may prevent hypothermia among sedentary elderly people [35].
Several results deserve further discussion. First, self-administered forms might be less costly and/or more valid than interviewer-administered ones [36, 37], but problems with vision, comprehension, and writing may cause older people to be less willing or unwilling to Table 4. Responsiveness statistics calculated by the mean change in scores for a domain or a facet from the prior to the present assessment among 24 persons who had fallen over a 3-month follow-up period divided by the standard devia-tion of score changes among 190 persons who had not fallen in the period
aStandard deviation.
Domain or facet
Fallers
Score change ± SDa
Non-fallers
Score change ± SDa Effect size . . . .. . . .. . . .. . . .
Overall Quality of Life/General Health −1.25 ± 2.83 −0.71 ± 2.97 −0.56
Physical Capacity −3.52 ± 2.96 −3.36 ± 2.49 −1.42
Psychological Well-being −2.25 ± 2.26 −1.22 ± 2.81 −0.80
Social Relationships −1.41 ± 2.61 −0.25 ± 3.06 −0.46
Environment −1.70 ± 1.93 −1.95 ± 2.38 −0.71
at Taipei Medical University Lib. on March 22, 2011
ageing.oxfordjournals.org
self-complete a questionnaire. Therefore the use of the interviewer-administered WHOQOL-BREF for older people is recommended. Second, the higher percentage of ceiling values for WHOQOL items framed in a nega-tive manner may also exist in other populations. The framing effect on the responses to questions has been reported in preference measures [38, 39]; however, it has seldom been examined in psychometric HRQL measures and needs to be explored in future research. Third, com-pared with a single item for describing the overall HRQL, the two-item Overall Quality of Life and General Health facet is more likely to have better discriminant validity and responsiveness. Therefore, our scoring method for obtaining an overall quality of life score for each individ-ual could also be applied to the full version of the WHO-QOL which includes four items in the facet. Finally, although falls are supposed to simultaneously be related to changes in the four domain scores of the WHOQOL-BRE for assessing responsiveness, differences in the magnitude of the effect size might have resulted not only from the sensitivity of the four WHOQOL-BREF domain scores but also from the different effects of falls on the health domains of older people.
There are several limitations to the study. One is that the representativeness of the study sample was somewhat limited. A comparison of demographics of age, gender, and education between the study sample, older people in Taichung County, and those in Taiwan showed that the present study had a similar age distribution but a greater number of males and lower educational levels compared to Taichung County or Taiwan. Nevertheless, further subgroup analysis showed that the score distributions and psychometric properties in the study remained robust across age groups, gender groups, and educational levels. Second, the exclusion of 59 people who were hos-pitalised or bed-ridden at home during the assessment period may partly explain the lack of Xoor effect of the WHOQOL-BREF in this study. Information on whether the effect appears in older people who are hospitalised or who are suffering a serious illness is needed. Finally, despite the focus group of the study not being able to come up with additional meaningful items speciWc to older people, that existing items in the original or Taiwanese versions of the WHOQOL-BREF may, in fact, not be sufWcient to adequately proWle the health of older people is worthy of further exploration.
Key points
• In each domain of the WHOQOL-BREF, score distributions were nearly symmetrical with no Xoor or ceiling effects.
• The WHOQOL-BREF had excellent validity and responsiveness as well as good internal consistency and test-retest reliability.
• Statements in the Sexual Activity and Work Capacity facets need to be modiWed.
• The WHOQOL-BREF is a suitable HRQL instrument for older people.
Funding
This work was supported by the National Science Council (grant NSC 91-2320-B-038-011), Taiwan, Republic of China.
References
1. World Health Organization. WHO Constitution. Geneva: WHO, 1948.
2. Stewart AL, GreenWeld S, Hays RD et al. Functional status and well-being of patients with chronic conditions – results from the Medical Outcomes Study. JAMA 1989; 262: 907–13.
3. Kaplan RM. ProWle versus utility based measures of
out-come for clinical trials. In Staquet MJ, Hays RD, Fayers PM eds. Quality of Life Assessment in Clinical Trials – Methods and Practice. New York: Oxford University Press, 1998: 69–90.
4. Lawton MP, Windley PG, Byerts TO. Aging and the Envi-ronment: Theoretical Approaches. New York: Springer, 1982.
5. Pearlman RA, Uhlmann RF. Quality of life in chronic dis-eases: perceptions of elderly patients. J Gerontol 1988; 43: M25–30.
6. Stewart AL, Sherbourne CD, Brod M. Measuring health-related quality of older and demented populations. In Spiker B ed. Quality of Life and Pharmacoeconomics in Clinical Trials. 2nd edn. Philadelphia: Lippincott-Raven Publishers, 1996: 819–30.
7. McHorney CA, Ware JE, Lu JFR, Sherbourne CD. The MOS 36-item Short-Form Health Survey (SF-36): III Tests of data quality. Scaling assumptions, and reliability across diverse patient groups. Med Care 1994; 32: 40–66.
8. Bindman AB, Keane D, Lurie N. Measuring health changes among severely ill patients: the Xoor phenomenon. Med Care 1990; 28: 1142–51.
9. The WHOQOL group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med 1998; 28: 551–8.
10. World Health Organization. WHOQOL Study Protocol. Geneva: WHO (MNH/PSF/93.9), 1993.
11. World Health Organization. WHOQOL Protocol for New Centers. Geneva: WHO (MNH/PSF/94.4), 1994.
12. The WHOQOL-Taiwan Group. Manual of the Taiwanese Version of WHOQOL-BREF. Taipei: Taiwan WHOQOL Group, 2000.
13. The WHOQOL-Taiwan Group. Introduction to the development of the WHOQOL-Taiwan version. Chin J Public Health (Taipei): 2000; 19: 315–24.
14. Department of Health (R.O.C.). Vital Statistics in 1999. Taipei: Department of Health, Executive Yuan, Taiwan, Republic of China, 2000.
15. Sheikh JA, Yessavage JA. Geriatric Depression Scale (GDS): recent Wndings and development of a shorter version.
at Taipei Medical University Lib. on March 22, 2011
ageing.oxfordjournals.org
In Brink TL ed. Clinical Gerontology: A Guide to Assessment and Intervention. New York: Howarth Press, 1986.
16. Liao YC, Yeh TL, Ko HC et al. Geriatric Depression Scale – validity and reliability of the Chinese-translated version: a preliminary study. R.O.C.: Med J Changhua Christian Hospital, 1995: 11–17.
17. Lyness JM, Noel TK, Cox C etal. Screening for depression in elderly primary care patients. A comparison of the Center for Epidemiologic Studies-Depression Scale and the Geriatric Depression Scale. Arch Intern Med 1997; 157: 449–54.
18. Folstein MF, Folstein SE, McHugh PR. Mini-Mental State: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975; 12: 189–98.
19. Guo NW, Liu HC, Wong PF et al. Chinese version and norms of the Mini-Mental State examination. J Rehab Med Assoc (R.O.C.) 1988; 16: 52–9.
20. George LK, Landerman R, Blazer DG, Anthony C. Cogni-tive impairment. In Robins LN, Regier DA eds. Psychometric Disorders in America: The Epidemiologic Catchment Area Study. New York: Free Press, 1991: 291–327.
21. Cronbach LJ. CoefWcient alpha and the internal structure
of tests. Psychometrika 1951; 16: 297–334.
22. Shrout PE, Fleiss JL. Intraclass correlations: uses in assess-ing rater reliability. Psychol Bull 1979; 86: 420–8.
23. Bentler P. Comparative Wt indexes in structural models.
Psychol Bull 1990; 107: 238–46.
24. Guyatt GH, Walter S, Norman G. Measuring change over time: assessing the usefulness of evaluative instruments. J Chronic Dis 1987; 40: 171–8.
25. Guyatt GH, Deyo RA, Charlson M, Levine MN, Mitchell A. Responsiveness and validity in health status measurement: a clariWcation. J Clin Epidemiol 1989; 42: 403–8.
26. Cohen J. Statistical Power Analysis for the Behavioral Sci-ences. 2nd edn. New York: Lawrence Erlbaum Associates, 1998.
27. Curran D, Fayers PM, Molenberghs G, Machin D. Analysis of incomplete quality of life data in clinical trials. In Staquet MJ, Hays RD, Fayers PM eds. Quality of Life Assessment in Clinical Trials – Methods and Practice. New York: Oxford Uni-versity Press, 1998: 249–80.
28. Ünal G, de Boer JB, Borsboom GJ et al. A psychometric comparison of health-related quality of life measures in chronic liver disease. J Clin Epidemiol 2001; 54: 587–96.
29. Lawton MP. The physical environment of the person with Alzheimer’s disease. Aging Mental Health 2001; Suppl 1: S56–64.
30. Connell BR. Role of the environment in falls prevention. Clin Geriatr Med 1996; 12: 859–90.
31. Lemke S, Moos RH. Personal and environmental determi-nants of activity involvement among elderly residents of con-gregate facilities. J Gerontol 1989; 44: S139–48.
32. Lawton MP. Environment and other determinants of well-being on older people. Gerontologist 1983; 23: 349–57.
33. Sundeen RA, Mathieu JT. The fear of crime and its conse-quences among elderly in three urban communities. Gerontol-ogist 1976; 16: 211–9.
34. Pastalan LA, Pawlson LG. Importance of the physical envi-ronment for older people. J Am Geriatr Soc 1985; 33: 874.
35. Reuler JA. Hypothermia: pathophysiology, clinical setting, and management. Ann Intern Med 1978; 89: 519–27.
36. McHorney CA. Measuring and monitoring general health status in elderly persons: practical and methodological issues in using the SF-36 health survey. Gerontologist 1996; 36: 571–83.
37. Cook DJ, Guyatt GH, Juniper E et al. Interviewer versus self-administered questionnaires in developing a disease-speciWc, health-related quality of life instrument for asthma. J Clin Epidemiol 1993; 46: 529–34.
38. McNeil BJ, Pauker SG, Sox HC, Tversky A. On the elicita-tion of preferences for alternative therapies. N Engl J Med 1982; 306: 1259–62.
39. Hershey JC, Kunreuther HC, Shoemaker PJH. Sources of bias in assessment procedures for utility functions. Manag Sci 1982; 28: 936–54.
Appendix
A sample of 5 items in the Taiwanese version of the WHOQOL-BREF
Q1. How would you rate your quality of life?
❏ Very poor ❏ Poor ❏ Neither poor nor good ❏ Good ❏ Very good
Q4. How much medical treatment do you need to function in your daily life?
❏ Not at all ❏ Slightly ❏ Moderately ❏ Very much ❏ Extremely
Q12. Do you have enough money to meet your needs? ❏ Not at all ❏ A little ❏ Moderately ❏ Mostly ❏ Completely
Q22. How satisWed are you with the support you get
from your friends?
❏ Very dissatisWed ❏ DissatisWed ❏ Neither satisWed nor dissatisWed ❏ SatisWed ❏ Very satisWed
Q28. Are you usually able to get the things you like to eat? ❏ Never ❏ Seldom ❏ Quite often ❏ Very often ❏ Always
Received 23 July 2002; accepted in revised form 25 March 2003
at Taipei Medical University Lib. on March 22, 2011
ageing.oxfordjournals.org