Community Dental Health (2009) 26, 183–187 © BASCD 2009
Received 15 March 2007; Accepted 14 September 2007 doi:10.1922/CDH_2322Chang05
Higher-order exploratory factor analysis of the Dental Subscale
of Children’s Fear Survey Schedule in a Taiwanese population.
Chen-Yi Lee; Yong-Yuan Chang and Shun-Te Huang
Kaohsiung Medical University, No.100, Shih-chuan 1st Rd., Sanmin District, Kaohsiung City 807, Taiwan
Objectives: The Dental Subscale of the Children’s Fear Survey Schedule (CFSS-DS) is extensively used to assess the level of child dental
anxiety. The present study aimed to explore the higher-order factor structure of the parental Chinese version of the CFSS-DS with a large sample of young children in Taiwan. Design: The parental CFSS-DS was used as a screening tool to survey the dental anxiety levels of 5 to 8- year-old children at kindergartens and elementary schools in Kaohsiung city, Taiwan. Subjects were selected by stratified random sampling. The stratification was done by geographic district, age group, and gender. Participants: The sample was 1,819 children aged 5 to 8 years old. Main outcome measures: A first-order factor analysis was performed using the principal components method with promax rotation, and a second-order factor was obtained by applying the Schmid-Leiman solution (SLS). Results: The present study found three first-order factors, defined as: (1) fear of dental aspects, (2) fear of medical aspects, and (3) fear of potential victimization. The second-order factor defined as “dental fear” accounted for most of the variance in the second-second-order factor structure. The results of higher-second-order factor analysis according to different gender or age levels were identical. Conclusions: A higher-order factor structure consisting of a single second-order factor and three first-order factors was extracted, giving a fuller understanding of the CFSS-DS. The second-order factor structure of Chinese version CFSS-DS was stable and reliable.
Key words: Dental fear, Dental Subscale of Children’s Fear Survey Schedule (CFSS-DS), exploratory factor analysis; higher-order factor analysis; Schmid-Leiman solution
Introduction
Cuthbert and Melamed (1982) developed the Dental Sub-scale of the Children’s Fear Survey Schedule (CFSS-DS), which has been extensively used to assess the level of dental anxiety of children in a number of studies (Alvesalo
et al., 1993; Chellappah et al., 1990; Klingberg, 1994;
Raadal et al., 1995; ten Berge et al., 2002; Wogelius et
al., 2003). The CFSS-DS has a parental and a children’s
version. For younger children unable to read and write, the parental CFSS-DS is filled out by their parents, who generally know their children’s concerns very well (Klingberg, 1994; Raadal et al., 1995; ten Berge et al., 2002; Wogelius et al., 2003). With older children who have learned to read, the researchers ask them to fill out the questionnaires by themselves (Chellappah et al., 1990). The psychometric characteristics of the scale have been reported in several studies in which the test-retest reliability and internal consistency coefficient were proved to be good (Alvesalo et al., 1993; Klingberg, 1994; ten Berge et al., 1998; Wogelius et al., 2003).
Factor analysis of the CFSS-DS has been performed in few studies (Alvesalo et al., 1993; Milgrom et al., 1994; ten Berge et al., 1998). A study in Finland (n=828, mean age=12.6 yr) found that three factors accounted for 54% of scale variance relating to “fear of highly invasive procedures,” “fear of potential victimization,” and “fear of less invasive procedures” (Alvesalo et al., 1993). Using a Dutch version of the CFSS-DS, a study in the Netherlands (n=150, 4-12 yrs) found that three
Correspondence to: Dr. Yong-Yuan Chang, Associate Professor, Graduate Institute of Public Health, Kaohsiung Medical University, No.100, Shih-chuan 1st Rd., Sanmin District, Kaohsiung City 807, Taiwan (R.O.C.). E-mail: yyc1948@mail2000.com.tw
factors relating to “highly invasive dental procedures,” “less invasive procedures and strangers,” and “general medical aspects of treatment” accounted for 65% of total scale variance (ten Berge et al., 1998). A cross-cultural study of Chinese, employed factor analyses of small sample sizes in Canada and the PRC; the PRC-Chinese responses (n=99, 3.7±0.7 yr) yielded three factors―“low invasive procedures,” “highly invasive procedures,” and “potential victimization” ―which in total accounted for 64.5% of scale variance; the Canadian-Chinese responses (n=70, 7.7±2.3 yr) yielded a similar factor structure (with a fourth factor of “having somebody look at you” and “being touched by a stranger”), explaining 67.6% of the scale variance (Milgrom et al., 1994).
Gorsuch (1983) suggested that the sample size for factor analysis should be greater than 100, and at least fivefold the number of measured variables. Guadagnoli and Velicer (1988) suggested that if the factors are each defined with ten or more structure coefficients each of around |0.4|, the sample size should not be less than 150. MacCallum et al. (1999) determined that if h2
val-ues were around 0.50, sample sizes of 100 to 200 were required. Among the previous studies, only the study in Finland had an ample sample size (Alvesalo et al., 1993), the sample size of the Dutch study was acceptable (ten Berge et al., 1998), and the sizes of the PRC sample and the Canadian–Chinese sample were obviously too small (Milgrom et al., 1994).
The previous studies all used the principal components method with varimax rotation in their factor analyses. They revealed three or four factor solutions with differ-ent factor structures, and all the studies found that many items loaded (≥0.4) on more than one factor, showing a possible correlation between the extracted factors. In these cases, the simple structure cannot be obtained using an orthogonal rotation like varimax since such factors are difficult to interpret. Oblique rotation, such as promax or direct oblimin, appears to be a better way to obtain the simple structure (Gorsuch, 1983; Kim J-O and Mueller, 1978; Thompson, 2004).
The factors extracted from intervariable correlations (or other statistics measuring associations) are called first-order factors. The factors then extracted from the interfactor correlations among the first-order factors are called second-order factors. If the second-order factors are correlated, then third-order factors can be extracted (Thompson, 2004). Second-order factor analysis does not seem to be widely known or understood at present. It is argued by some researchers, however, that these higher-order factors should be extracted whenever factors are correlated (Gorsuch, 1983; Kerlinger, 1984; Thompson, 2004). When higher-order factor analysis is conducted, the Schmid-Leiman solution (SLS) is a convenient tool for higher-order factor analysis (Schmid and Leiman, 1957; Thompson, 2004; Wolff H-G and Preising, 2005). It expresses the independent influence of first-order and higher-order factors in terms of the measured variables, and thus eases the interpretation of factors at different levels.
Since a higher-order factor analysis had not been carried out in a study of dental anxiety using the CFSS-DS, in this study we performed a higher-order factor analysis based on a large sample size using data from a previous epidemiological survey. The first-order factor structure was obtained using the principal components method with promax rotation, and the higher-order factors were extracted with the SLS.
Method
The data were obtained from a previous epidemiological survey of dental anxiety in Taiwanese children (Lee et
al., 2007). The Chinese parental version of the
CFSS-DS was used to survey 5-8 year-old children from 11 kindergartens and six elementary schools located in Kaohsiung city, Taiwan. The Kaohsiung City Bureau of Education gave us a list of all kindergartens and el-ementary schools and information about the distribution of kindergarten and elementary school children by age and geographic district within the city. Approval for the study was obtained from the local government.
The study population was recruited by stratified ran-domization, proportional to size. The stratification was done on age group, gender, and geographic district. Four districts (Sanmin, Yancheng, Lingya, and Qianjin) were randomly selected from 11 districts in Kaohsiung city, and then 11 kindergartens and six elementary schools were randomly selected from those districts. Finally, four age groups (5, 6, 7 and 8 years old) were randomly selected from those schools. The number of subjects required in each age group was in proportion to the number of the
whole population in each selected schools.
The observations with odd serial numbers were in-cluded in the analysis; the others were inin-cluded in another study not presented here. Therefore, the sample involved is 1,819 children. The informed consents were obtained from the participating parents, and the research protocol for this study was approved by the Human Experiment and Ethics Committee of the Chung-Ho Memorial Hos-pital, Kaohsiung Medical University.
The CFSS-DS consists of 15 items, each cover-ing different aspects of dental and medical situations, scored from 1(not afraid) to 5(very afraid) on a 5-point Likert-scale, with total scores ranging from 15 to 75. For young children unable to complete the questionnaire by themselves, the scale is usually completed by one of the parents.
Cronbach’s α was performed to estimate the internal consistency. The principal components method with promax rotation was performed to assess the first-order factor structure, and SLS was performed to obtain the higher-order factors. The higher-order factor applications are not included in most statistical programs. Even the popular packages such as SPSS and SAS do not provide routines for the calculation of the SLS. All of the analyses were done with SPSS for Windows 13.0 using syntax codes adapted from Thompson (2004) and Wolff and Preising (2005).
Results
The Cronbach’s α in this study was 0.90, achieving high internal consistency. The scree plot suggested three fac-tors, and the first solution of our principal components analysis gave three factors with eigenvalues above 1.0 (6.445, 1.380, and 1.097). After comparing the factor structure of one factor, two factors and three factors, the three-factor structure was determined the simplest one.
Unlike orthogonal rotation, a factor structure produced through oblique rotation will obtain pattern and structure coefficients that are not identical. The promax-rotated factor pattern and structure coefficients are both presented in Table 1. All of the pattern coefficients (factor load-ings) of each factor were above 0.4. The communality coefficients (h2) were 0.320~0.745. The first factor from
the first solution of our principal components analysis consisted of items related to “the situations that may hap-pen in the dental setting,” including both the highly and less invasive dental procedures, except for “injection,” all items were specific to the dental setting. The second factor consisted of items related to “the situations that may happen in general medical settings, not specific to the dental setting.” The third factor consisted of items related to “these situations that may happen in other settings not specific to medical or dental settings, which involve potential victimization.” The three first-order fac-tors were correlated as expected, and such a result implies the presence of one or more higher-order factors.
Only one second-order factor was extracted from the first-order factor correlation matrix, with an eigenvalue of above 1.0 (1.856). The three second-order factor pat-tern/structure coefficients were 0.855, 0.843, and 0.644, respectively.
Table 1. First-order promax-rotated pattern and structure coefficients
*The items with factor loading ≥0.4 are in bold type.
Item Pattern Structure
Factor1 Factor2 Factor3 Factor1 Factor2 Factor3
8 The dentist drilling 0.951* -0.145 -0.018 0.855 0.441 0.255
9 The sight of the dentist drilling 0.891 -0.061 -0.004 0.851 0.491 0.274
10 The noise of the dentist drilling 0.823 0.026 -0.007 0.837 0.535 0.274
11 Having somebody put instruments in your mouth 0.727 0.031 0.134 0.791 0.522 0.385
15 Having the dentist clean your teeth 0.627 0.219 -0.090 0.733 0.582 0.183
12 Choking 0.622 0.009 0.199 0.694 0.454 0.408
1 Dentists 0.539 0.330 -0.186 0.682 0.610 0.090
3 Injections 0.537 -0.065 0.150 0.547 0.313 0.206
2 Doctors -0.057 0.763 -0.012 0.412 0.724 0.309
14 People in white uniforms -0.219 0.749 0.225 0.321 0.679 0.373
5 Having to open your mouth 0.148 0.717 -0.081 0.405 0.785 0.179
4 Having somebody examine your mouth 0.209 0.666 -0.078 0.450 0.773 0.187
6 Having a stranger touch you 0.116 -0.125 0.820 0.311 0.188 0.822
7 Having somebody look at you -0.022 0.083 0.803 0.296 0.305 0.820
13 Having to go to the hospital 0.077 0.348 0.448 0.442 0.527 0.576
Factor correlation matrix
Factor1 1.000
Factor2 0.621 1.000
Factor3 0.332 0.294 1.000
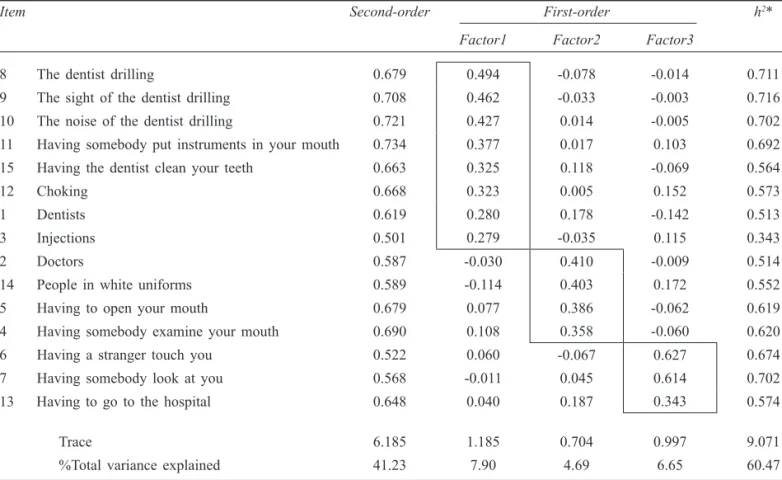
Table 2. Results of the Schmid-Leiman solution
Item Second-order First-order h2*
Factor1 Factor2 Factor3
8 The dentist drilling 0.679 0.494 -0.078 -0.014 0.711
9 The sight of the dentist drilling 0.708 0.462 -0.033 -0.003 0.716
10 The noise of the dentist drilling 0.721 0.427 0.014 -0.005 0.702
11 Having somebody put instruments in your mouth 0.734 0.377 0.017 0.103 0.692
15 Having the dentist clean your teeth 0.663 0.325 0.118 -0.069 0.564
12 Choking 0.668 0.323 0.005 0.152 0.573
1 Dentists 0.619 0.280 0.178 -0.142 0.513
3 Injections 0.501 0.279 -0.035 0.115 0.343
2 Doctors 0.587 -0.030 0.410 -0.009 0.514
14 People in white uniforms 0.589 -0.114 0.403 0.172 0.552
5 Having to open your mouth 0.679 0.077 0.386 -0.062 0.619
4 Having somebody examine your mouth 0.690 0.108 0.358 -0.060 0.620
6 Having a stranger touch you 0.522 0.060 -0.067 0.627 0.674
7 Having somebody look at you 0.568 -0.011 0.045 0.614 0.702
13 Having to go to the hospital 0.648 0.040 0.187 0.343 0.574
Trace 6.185 1.185 0.704 0.997 9.071
%Total variance explained 41.23 7.90 4.69 6.65 60.47
Interpretations of the second-order factors should not only rely on the first-order factors (Gorsuch, 1983; Cook and Thompson, 2000). Some researchers have suggested postmultiplying the first-order factor pattern matrix by the second-order factor pattern matrix. The SLS calculates the direct relations between higher-order factors and measured variables, and provides informa-tion about the independent contribuinforma-tion of the factors of different levels to the variables. This is, the optimal analytical strategy for the interpretation of higher-order factors (Gorsuch, 1983; Kim and Mueller, 1978; Wolff and Preising, 2005; Cook and Thompson, 2000). The SLS solution is presented in Table 2.
In this study, the variance in the first-order factors also present in the second-order factor was removed, so that the three first-order factors contained the residualized vari-ance. The factor loadings of the second-order factor ranged from 0.501 to 0.734, indicating that a generic higher-order dimension of child dental anxiety existed. The next three columns indicate the residualized first-order factors, all of which still retained a total variance of above 4%.
Items 1 and 3 did not have first-order factor loadings above 0.3 in the SLS, although their original loadings from promax rotation in Factor 1 were above this criterion (see Table 1). These items seem to reflect the second-order factor to the extent that they should not be considered “good” measures of Factor 1. Therefore, interpretations of Factor 1 should rely on items 8~12 and 15. All items have higher loadings on the second-order factor than on the first-order factors, except for items 6 and 7, which reflect purer measures of Factor 3.
Discussion
As in the earlier factor analyses of CFSS-DS data (Al-vesalo et al., 1993; Milgrom et al., 1994; ten Berge et
al., 1998), three first-order factors were obtained in the
present study. Factor 1 related to the situations mainly happening in the dental setting, and these may be defined as “fear of aspects of dental setting.” Factor 2 related to the situations about general medical setting, and these may be defined as “fear of aspects of medical setting.” Factor 3 related to the situations not specific to dental or medical settings and may be defined as “fear of aspects of potential victimization.” The single, second-order factor obtained from higher-order factor analysis can be defined as “dental fear.”
As presented in Table 2, with all coefficients ranging from 0.501 to 0.734, the 15 questions can be construed to represent a generic higher-order dimension of dental fear. Except for item 6 “Having a stranger touch you” and the item 7 “Having somebody look at you,” all the other items having higher loadings on the second-order factor were associated with dental and medical situations. Apart from the high loadings on one factor, these items also possessed some loadings on additional factors. The residualized first-order factor 1 still contained 7.90% of the total variance, items 8~12 and 15 contributing most to the remaining variance in Factor 1; the residualized factor 2 contained 4.69% of the total variance, contributed to most by items 2, 4, 5 and 14; the residualized factor 3 contained 6.65% of the total variance, contributed to most by items 6, 7, and 13.
As ten Berge et al. (1998) noted, all the previous studies found that many items load (≥0.4) on more than one factor, which implies that the CFSS-DS may essentially measure a one-dimensional concept of dental fear. In the revision of the scale, items 6 and 7 could be deleted because, in our study, they loaded more on the first-order factor than on the second-order factor, which resulted in a different factor structure.
In the present study, notably using a large sample size relative to the number of items and the sample sizes used in previous first-order factor analytic studies of CFSS-DS, we attempted to establish a higher-order factor solution for data from the Chinese version of the CFSS-DS and found a higher-order factor structure consisting of a single second-order factor and three first-order factors. The SLS gave further insight into the structural relations between first-order and second-order factors, as well as the rela-tions between items and second-order factors.
Acknowledgements
This research was based on a thesis submitted to the Col-lege of Dental Medicine, Kaohsiung Medical University, in partial fulfillment of the requirements for the Sc.D. degree. Support for the study came from the National Science Council of Taiwan.
The authors thank the Bureau of Education, Kaoshiung City Government, for permission to conduct a survey in those selected schools; the teachers and dentists who helped in this research; and, most importantly, the par-ticipating children and parents or guardians.
References
Alvesalo, I., Murtomaa, H., Milgrom, P., Honkanen, A., Karj-alainen, M., and Tay, K. M. (1993): The Dental Fear Sur-vey Schedule: a study with Finnish children. International journal of paediatric dentistry 3, 193-198.
Chellappah, N. K., Vignesha, H., Milgrom, P., and Lo, G. L. (1990): Prevalence of dental anxiety and fear in children in Singapore. Community Dentistry and Oral Epidemiol-ogy 18, 269-271.
Cook, C., and Thompson, B. (2000): Higher-order factor analytic perspectives on user’s perceptions of library service quality. Library and Information Science Research 22, 393-404. Cuthbert, M. I., and Melamed, B. G. (1982): A screening device:
children at risk for dental fears and management problems. ASDC Journal of Dentistry for Children 49, 432-436. Gorsuch, R. L. (1983): Factor analysis, 2nd edn. Hillsdale,
NJ: Erlbaum.
Guadagnoli, E., and Velicer, W. (1988): Relation of sample size to the stability of component patterns. Psychological Bulletin 103, 265-275.
Kerlinger, F. N. (1984): Liberalism and conservatism: The nature and structure of social attitudes. Hillsdale, NJ: Erlbaum. Kim, J-O., and Mueller, C. W. (1978): Introduction to factor
analysis: what it is and how to do it. Beverly Hills and London: Sage Pubns.
Klingberg, G. (1994): Reliability and validity of the Swedish version of the Dental Subscale of the Children’s Fear Sur-vey Schedule, CFSS-DS. Acta Odontologica Scandinavica 52, 255-256.
Lee CY, Chang YY, Huang ST. (2007): Prevalence of dental anxiety among 5~8 year-old Taiwanese children. Journal of Public Health Dentistry 67, 36-41.
MacCallum, R. C., Widaman, K. F., Zhang, S., and Hong, S. (1999): Sample size in factor analysis. Psychological Methods 4, 84-99.
Milgrom, P., Jie, Z., Yang, Z., and Tay, K. M. (1994): Cross-cultural validity of a parent’s version of the Dental Fear Survey Schedule for children in Chinese. Behaviour Re-search and Therapy 32, 131-135.
Raadal, M., Milgrom, P., Weinstein, P., Mancl, L., and Cauce, A. M. (1995): The prevalence of dental anxiety in children from low-income families and its relationship to personality traits. Journal of Dental Research 74, 1439-1443. Schmid, J., and Leiman, J. N. (1957): The development of
hierarchical factor solutions. Psychometrika 22, 53-61. ten Berge, M., Veerkamp, J. S. J., Hoogstraten, J., and Prins,
P. J. M. (2002): Childhood dental fear in the Netherlands: prevalence and normative data. Community Dentistry and Oral Epidemiology 30, 101-107.
ten Berge, M., Hoogstraten, J., Veerkamp, J. S. J., and Prins, P. J. M. (1998): The dental subscale of the children’s fear survey schedule: a factor analytic study in the Netherlands. Com-munity Dentistry and Oral Epidemiology 26, 340-343. Thompson, B. (2004): Exploratory and confirmatory factor
analysis: Understanding concepts and applications. Washington, DC: American Psychological Association. Wogelius, P., Poulsen, S., and Sørensen, H. T. (2003): Prevalence
of dental anxiety and behavior management problems among six to eight years old Danish children. Acta Odontologica Scandinavica 61, 178-183.
Wolff, H-G., and Preising, K. (2005): Exploring item and higher order factor structure with the Schmid-Leiman solution: Syntax codes for SPSS and SAS. Behavior Research and Methods 37, 48-58.