Effect of Antiretroviral Therapy on the Incidence of Cervical Neoplasia among HIV-infected Women: A population-based cohort study in Taiwan
Yen-Chin Chena, MS, Chung-Yi Lib,d, PhD, Hsiao-Ying Liua, MS, Nan-Yao Leec, MD, Wen-Chien Koc, MD, Nai-Ying Koa,b, PhD
Departments of aNursing, bPublic Health, and cMedicine, College of Medicine, National Cheng Kung University & Hospital, Tainan, Taiwan & dDepartment of Public Health, College of Public Health, China Medical University, Taichung, Taiwan
Running head: Incidence of cervical neoplasia in HIV There are no conflicts of interest.
This finding were presented in part at the 7th IAS conference on HIV pathogenesis, treatment and prevention.
This study was supported by the National Science Council (NSC 100-2629-B-006 -002), Taiwan.
Word counts: abstract = 237; text = 2412 Number of tables: 3
Reprint requests and correspondence: Nai-Ying Ko, Ph.D. Address: No.1, Ta-Hsueh Road, Tainan 701, Taiwan Tel: 886-6-235-3535 ext. 5838; Fax: 886-6-2377550 E-mail: [email protected] Introduction 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Cervical cancer has been recognized as one of the AIDS-defining cancers since 1993, and is the second most common cancer in Asian females with >530,000 new cases in 2012. In Taiwan, cervical cancer is the fifth most common cancer in women and was the most frequently-diagnosed gynecologic neoplasm in 2009. In that year, 1,797 women were diagnosed with new cases of invasive carcinoma, and 657 died as a result of this disease. It is well established that human papilloma virus (HPV) is a precursor lesion for cervical cancer. Studies have shown that HPV is more prevalent and persistent in HIV-infected women, particularly among those with a lower CD4 count, >40 years old at AIDS diagnosis, intercourse at an early age, multiple sexual partners, and low socioeconomic level. These factors explain the higher risk for both cervical cancer and cervical intraepithelial neoplasia associated with HIV infection. Compared with the general population, HIV-infected women have a 2.9-fold risk of cervical cancer. However, studies of the incidence of cervical cancer in Asia are frequently limited to persons with HIV.
In Taiwan, all HIV-infected patients were provided free access to inpatient or outpatient care and antiretroviral therapy at designated hospitals since the early 1990s. In 1997, HAART was introduced in Taiwan, and the mortality rate has declined dramatically from 148.4 per 100 person-years (PY) in 1995 to 6.5 per 100 PY after 2000 . Followed by Taiwan Center of Diseases Control Guidelines for diagnosis and
2 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 5
treatment of HIV/AIDS in 2008, HAART is recommended for all HIV-infected
person with CD4 counts of <350 cell/mm or presenting AIDS-related opportunistic3 infection or tumor; or severe clinical signs; or pregnant women. Since then, HIV-infected women are experiencing an increased life expectancy as deaths from opportunistic infections decline. HIV infection has been transformed from a fatal disease to a chronic, manageable disease. HAART use has been shown to reduce the risk of opportunistic malignancies such as Kaposi sarcoma and some lymphomas. However, reports on the effects of HAART on cervical neoplasia and cervical cytological changes have been inconsistent, with some studies showing a positive effect with HAART and others showing no change. With increasing age, cervical cancer poses a greater problem for HIV-infected women.
At present, little information is available concerning cervical cancer in HIV-infected women and the effect of HAART therapy in Asia. Therefore, this study aimed to determine the effect of HAART on the incidence of cervical cancer using a population-based longitudinal data of women living with HIV.
Methods
Data source
A secondary analysis of data was conducted using the National Health Insurance 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57
longitudinal databases that covers ~99% of the 23 million people living in Taiwan, and includes 99% of the hospitals and clinics under a mandatory single-payer health insurance system. The NHIRD includes the original medical and pharmacy records for all patients. Studies have systematically validated the accuracy and reliability of the NHIRD data. A recent report has further validated the utility of the database for identifying HIV-related diseases.
Data for HIV-infected women and women in the general population were obtained using claim files from 2000 to 2008. Data for HIV-infected women were identified by the ICD-9 code (042, V08) on the original claim. Data for the general population were obtained from the Longitudinal Health Insurance Database 2000 (LHID, 2000) of the NHIRD claims data. The LHID2000 contains original claims data for 1,000,000 subjects, a random sample of the National Health Insurance (NHI) program. The study was exempt from full review by the Institutional Review Board of National Cheng Kung University Hospital, as the database consisted of de-identified data released for research purposes.
HIV-infected women
A review of the database identified 17,277 patients who had visited ambulatory care facilities with a principal diagnosis of HIV infection. After excluding 13,153 (89.9%) male patients, and 53 (0.4%) who lacked gender information, 1,419 women
4 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 11
who were diagnosed with HIV between 2000 and 2008 were identified. Tests of goodness-of-fit between the study HIV population and annual statistics of HIV/AIDS from the Taiwan CDC from 2000-2008 showed no difference (χ2 = 6.66, p = 0.25) in age composition. For the purposes of this study, records were excluded if the women reported a history of cervical cancer (n = 9), or had undergone a hysterectomy prior to HIV diagnosis (n = 9). Ten records had incomplete information were also excluded. Data analyzed in the present study were 1,360 HIV-infected women.
General Population
A sample of general population (n = 475,626) was identified from the LHID2000 who were registered in the NHI program in 2000. Women aged <15 years (n = 100,373), diagnosed with cervical cancer (n = 899), infected with HIV (n = 107), or deceased prior to 2000 (n = 16,114) were excluded. A total of 358,141 HIV-negative women retrieved from the LHID2000 serving as the control group were analyzed and followed to 2008.
Research Variable The endpoint of cervical neoplasia (CIS, cervical cancer in situ or ICC, invasive cervical cancer) occurred in the catastrophic illness claim data, in which the NHI captures 30 categories (including cancers along with pathology or cytology documentation). The endpoint was reached if the diagnosis appeared at least twice in 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96
period. Under the NHI program, physicians and hospitals apply for reimbursement after providing care for cervical neoplasia, allowing cervical neoplasia codes to be reliably identified from the NHIRD medical claims data. Demographic and risk factor data were also retrieved from the claims data, including age at HIV diagnosis, urbanization level (according to the classification scheme proposed by Liu et al.), monthly income, occupation (blue-collar versus white-collar; white collar was defined as indoor working for more than 12 hours, i.e., public servant, technician and professional staff, others were recorded as blue collar), opioid dependence (based on the ICD-9 codes 3040, 3055, 3047), number of Pap tests after HIV diagnosis, history of sexually-transmitted diseases (STDs) (ICD-9: 0541, 0781, 0788, 091-099, 131, 6149) and treated opportunistic infections (OIs) (ICD-9: 4829, 112, 3210, 0074, 0785, 054, 1369, 0088, 0312, 1179, 1363, 130, 010-018, 0030, 0539, 7994) after HIV diagnosis.
Based on the participant’s pharmacy refill record, each antiretroviral drug code number and prescription dates were retrieved from outpatient medical visit claim data. Receipt of HAART therapy was categorized as ≤0.5 year (including non users) versus >0.5 year. Duration of HAART therapy was referred to the duration from the first date ART was prescribed to the occurrence of cancer, withdrawal from the program, or the end of 2008. For those received HAART therapy at least once, duration of
6 98 99 100 101 102 103 104 105 106 107 108 109 110 111 112 113 114 115 116 17
HAART therapy was further classified into 4 groups: ≤0.5, 0.5-2, 2-3 and >3 years. Additionally, a A ccording to individual’s pharmacy refill records, pattern of HAART use were classified into 3 groups: ≤0.5 year less than 6 months , >0.5 year and adherence (≥95%) , as well as >0.5 year but and non-adherence. To address the appropriateness of using ≥95% as a cut-off point in determining adherence, we also performed a sensitivity analysis by using ≥85% as a cut-off point.
Data Analysis
The calculated incidence rates were expressed per 1,000 prospective person-years of observation during the 9-year study period. Person-years varied slightly for each cervical cancer type due to the exclusion of prevalent cases. Person-years at risk for cervical cancer after HIV diagnosis were calculated from the date of enrollment. Cancer incidence rates for the general population were determined using data from the LHID2000. Cox proportional hazards models were used to assess the effect of
HAART therapy on the incidence of cervical cancer among women living with HIV after controlling for age at HIV diagnosis, monthly income, urbanization level, occupation, drug dependence, treated OIs, history of STDs and frequency of Pap tests after HIV diagnosis. The level of significance was set at P <0.05. Analyses were conducted with the SPSS (17.0) and SAS (9.3) statistical packages.
Results 117 118 119 120 121 122 123 124 125 126 127 128 129 130 131 132 133 134 135
Study population
The files of 1,360 HIV-infected women and 358,141 HIV-negative women provided the data for analysis, representing 4,377 and 3,066,196 person-years of observation. The median age of the HIV-infected population at diagnosis was 31.6 years (range 15.7 to 89.0) which is significantly younger than the general population was 37.4 years (range 15 to 105.7) (t = 18.57, p < 0.001). The mean age (± SD) at the time of diagnosis of cervical cancer was 47.9 ± 11.58 years for the HIV group with no different comparing to 52.4 ± 14.54 years for the general population group (t = 0.99, p = 0.33). Almost one third (n = 509, 37.4%) of the HIV-infected women were
receiving HAART therapy. The mean duration (± SD) of HAART therapy was 3.3 ± 8.8 years.
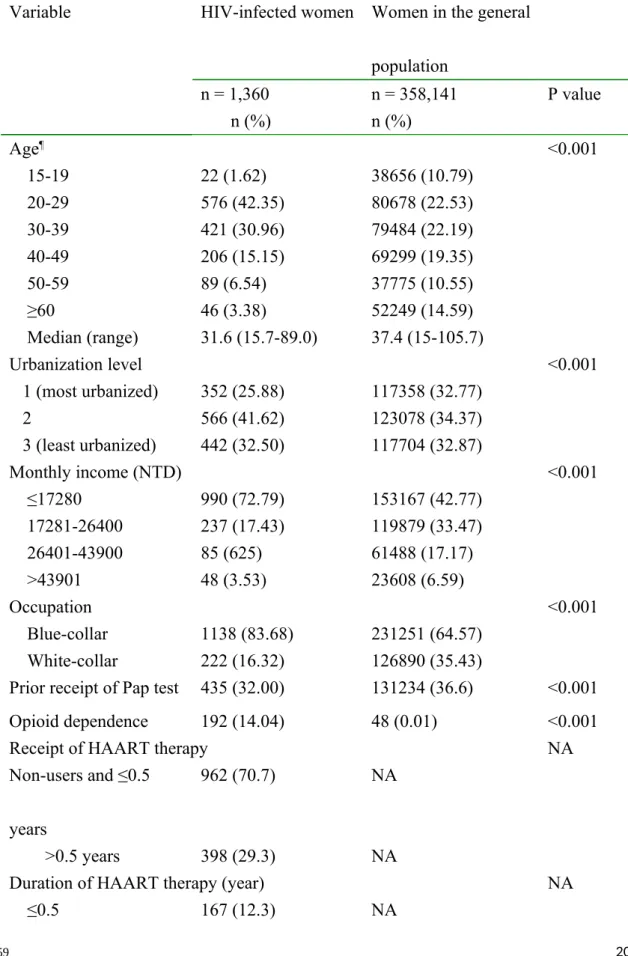
The populations differed in baseline demographics: HIV-infected persons were more likely to be younger (75% aged between 15 and 39 years), live in a less urbanized city (26%), have a low monthly salary (73%), be blue-collar workers (84%), have a low Pap test rate (32%; receiving at least one test during the study period), be drug-dependent (14%), have a history of STDs (15%), and have OIs treated after HIV diagnosis (23%) (Table 1).
Incidence and risk factors of cervical cancer
During the 9-year study period, 32.0% (n = 435) of the HIV-infected women had obtained a Pap test versus 36.6% (n = 131,234) of the general population. Thirteen
8 136 137 138 139 140 141 142 143 144 145 146 147 148 149 150 151 152 153 154 155 23
(1%) HIV-infected women had a diagnosis of cervical cancer versus 0.6% (n = 2,258) of the general population. The mean (SD) age at diagnosis of ICC was similar in the HIV-infected women [50.99 (12.62) years] and in the general population [56.65 (14.33) years] (t = 1.04; P = 0.3). The incidence was 3.2 (13/4376.5) per 1,000 person-years among the HIV-infected women and 0.7 (2258/3066196.4) per 1,000 person-years for the general population. The incidence of cervical neoplasia was significantly higher in the HIV-infected women than in the control group: CIS (SIR, 4.0 [95% CI, 1.47-8.70]), ICC (4.1 [95% CI, 1.66-8.48]), overall (4.0 [95% CI, 2.16-6.95]). The SIR for cervical neoplasia was greater for HIV-infected women between 40 and 59 years of age (Table 2).
Effect of HAART on cervical cancer incidence
The risk factors of for developing cervical cancer based on Cox proportional hazards models was significantly increased ing with age at HIV diagnosis (HRadj = 1.07 [95% CI: 1.02 to 1.11] ) , a highermore frequenc y of Pap tests after HIV ies
diagnosis (HRadj = 1.25 [95% CI: 1.15 to 1.35] ) and receipt of HAART therapy ≤0.5years (HRadj = 0.20 [95% CI: 0.05 to 0.77] ) after adjusting for confounding variables ( only the later was shown in Table 3 ) . We further to examine the effectd s of HAART on risk of cervical neoplasia according to specific duration and pattern risk after adjusting for confounding variables. Model 2 showed that the HAART use for 156 157 158 159 160 161 162 163 164 165 166 167 168 169 170 171 172 173 174
>
3 years showed had a significantly protective effect ( HRadj = 0.03 [95% CI: 0.01 to
0.
16 ] as compared to those who used HARRT for <=0.5 year. to reduce the risk of cervical neoplasia among women who received HAART therapy at least once (Table 3)
. Further, we performed sensitivity analyses on different adherence cutoff
parameters. Also cC ompared to those used HARRT <=0.5 year6 months, Model 3 we
found that shows HIV-infected women who used HARRT for >0.5 year reduced in the risk of cervical neoplasia were significantly associated with a reduced risk of cervical neoplasm regardless of level of adherence ( adherence >=95%, H Radj=0.09 [95% CI: 0.02 to 0.36] ; adherence <95%, HRadj=0. 13 [95% CI: 0.0 1 to 0. 89 ] adherence to HAART (Model 3 of Table 3). We alternatively used varied the per-patient >=85% as a adherence cut - off point and came up with from 85 % to the maximum efficacy of 95%, and also adjusted confounding factors , the data show similar results effects of varying adherence cutoff from 85 % to 95% to HAART on reducing risk of cervical neoplasia for HIV-infected women who initiated with HAART therapy (data not shown). Model 4 showed a dose-response relationship, whereas this risk changed with the duration of HAART use (p for trend = 0.002) and HAART use >3 year (HRadj = 0.
01 [95% CI: 0.0 0 to 0. 34 ] ) was associated with an significantly decre ased risk of cervical neoplasia when we put two variables as pattern of HAART use and duration of HAART therapy together into Cox-regression after adjusted confounding factors .
10 175 176 177 178 179 180 181 182 183 184 185 186 187 188 189 190 191 192 193 29
(Table 3) [建議不要放 model 4] Discussion
In the largest population-based analysis of cervical neoplasia incidence in HIV-infected women in Asia; the overall incidence was 9.6 per 1,000 persons (the ICC incidence was 1.6 per 1,000 persons) during our 9-year study period, and they had a 4-fold at greater risk than the general population adjusted for age and calendar years. This study was among the first to show that the strong association between HIV and cervical cancer risk shown in Europe and the United States also occurred in Asia. Our results are similar to previous reports that cervical cancer incidence is increased among women with HIV infection, such as 1.2/1,000 person-years and 4.2 to 5.3-fold SIR for ICC in the United States. However, they contrast with those of Kadhel et al. in France, who showed no significantly increased risk of ICC association with HIV. A partial explanation for this difference could be the relatively low rate of Pap tests among HIV-infected women in Taiwan. The coverage of annual screening for cervical cancer in HIV-infected women in Taiwan (11.9-24.4%) was lower than in France (28%). Consequently, this may account for the lower frequency of cervical neoplasia discovery, which may have been underestimated in Taiwan.
Data on the impact of HAART on cervical neoplasia has so far been equivocal. Our study showed that women who adherence to HAART and increasing duration of 194 195 196 197 198 199 200 201 202 203 204 205 206 207 208 209 210 211 212
HAART were significantly protected from cervical neoplasia, especially when the therapy extended over 3 years. The findings we present here are consistent with prior clinical studies reporting that adherent to HAART appear to have significantly increased immune function (CD4 counts) and a reduced prevalence of oncogenic HPV, which are likely to delay the onset of cervical lesions. Our study is in contrast to registry-based studies from the United States and Europe that suggest the risk of ICC among HIV-infected women has not decreased in the HAART era. The variation in findings generated by the registry-based studies may in part be due to survival bias, along with the coverage of antiretroviral therapy among women with HIV and the length of exposure to HAART. In Taiwan, all HIV-infected patients have been provided free antiretroviral therapy and medical care at AIDS-designated hospitals since the early 1990s. The NHIRD used for analysis covered almost all HIV-infected patients and their claim records for Pap smears and medical services in Taiwan. Furthermore, we found that HAART use for >3 years reduced the risk of cervical cancer to levels lower than those of HAART use for ≤3 years, and the immune system may be as good as that initial HAART users. Our results add significant weight to the growing body of research supporting the increased likelihood of protective effects on cervical cancer in HIV-infected women afforded by HAART.
Aging was the other factor contributing to the increased risk of cervical neoplasia
12 213 214 215 216 217 218 219 220 221 222 223 224 225 226 227 228 229 230 231 35
among women with HIV. Moreover, our finding is consistent with earlier reports showing that HIV-infected women have ICC earlier; they are ~10 years younger than in their seronegative counterparts This finding is consistent with the suggestion that the overall public health burden of cervical cancer in HIV-infected women is still likely to increase as HAART prolongs their lives; it also allows more time for HPV progression and the opportunity for cervical cancer to develop. In Taiwan, increasing age was significantly associated with having at least one Pap smear after HIV
diagnosis due to the national Pap smear screening policy, which targets women aged 30 or over . O ur findings suggest that healthcare professionals should remind
conducting Pap smear screening annually, especially for older HIV-infected women, to allow early detection and treatment of cervical intraepithelial neoplasia.
This study had some limitations. First, ascertainment of cervical cancer was based on the registry of patients with a critical illness; but in an administrative database, inaccuracies such as coding errors or loss are inevitable. Second, by the same token, the general population cohort may contain some subjects with HIV infection that had not yet been diagnosed that might compromise our findings. Third, on our finding of low Pap test usage, some patients with cancer might not have been detected and therefore not visited a clinic, a situation which could not be identified in this study. Finally, the study was limited by the nature of its retrospective design, which relied on 232 233 234 235 236 237 238 239 240 241 242 243 244 245 246 247 248 249 250
existing data sources. Potentially important clinical or laboratory parameters were not available, such as CD4 counts, viral load, and lifestyle-related information.
We found that women with HIV aged 40-59 years were at significantly increased risk of cervical cancer, more than 4-fold that of their counterparts in the general population during 2000-2008. Among the factor associated with a low risk of cervical cancer were adherence and prolonged HAART uses for at least 3 years. Our data suggest a potential benefit of adherence and HAART use over 3 years in HIV-infected women. Efforts to monitor pattern of HARRT toward the adherence and persistence HAART over 3 years of the goals will require healthcare providers to enhance. Integrating cervical cancer screening programmes into HIV care is a compulsory mission in Taiwan.
Acknowledgements
The authors thank Drs Susan Fetzer and IC Bruce for helpful editing and review. All authors participated in conception of the analysis . Detail a ssignments information below: S tudy design: Y.C.C. and N.Y.K. ; Data analysis: C.Y.L. and Y.C.C.
Interpretation of the results: Y.C.C., H.Y.L., N.Y.L., W.C.K., and N.Y.K. , Manuscript writing: Y.C.C., H.Y.L., and N.Y.K.
Approval of the text: All the authors have read and approved the text as submitted to AIDS. 14 251 252 253 254 255 256 257 258 259 260 261 262 263 264 265 266 267 268 269 41
Our study was supported by grants from the National Science Council, The
Executive Yuan of Taiwan (NSC 100-2629-B-006-002). This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health, and managed by the National Health Research Institutes. The interpretations and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
Conflicts of interest None. 270 271 272 273 274 275 276 277 278
References
1. Maiman M, Fruchter RG, Clark M, Arrastia CD, Matthews R, Gates EJ. Cervical Cancer as an AIDS-Defining Illness. Obstetrics & Gynecology 1997,89:76-80.
2. Webinars CCA. Ending Cervical Cancer in Asia. In; 2013.
3. Department of Health EY. Cancer Registry Annual Report. In; 2009.
4. Ellerbrock TV, Chiasson MA, Bush TJ, Sun XW, Sawo D, Brudney K, et al. Incidence of cervical squamous intraepithelial lesions in HIV-infected women. JAMA 2000,283:1031-1037.
5. Holmes RS, Hawes SE, Toure P, Dem A, Feng Q, Weiss NS, et al. HIV infection as a risk factor for cervical cancer and cervical intraepithelial
neoplasia in Senegal. Cancer Epidemiol Biomarkers Prev 2009,18:2442-2446. 6. Pinto VM, Golub JE, Tancredi MV, Alencar RS, Miranda AE. Cervical
Cytology and Histopathologic Abnormalities in Women living with AIDS in Sao Paulo, Brazil. Jaids-Journal of Acquired Immune Deficiency Syndromes 2011,57:S212-S216.
7. Chalermchockcharoenkit A, Chayachinda C, Thamkhantho M, Komoltri C. Prevalence and cumulative incidence of abnormal cervical cytology among HIV-infected Thai women: a 5.5-year retrospective cohort study. Bmc Infectious Diseases 2011,11.
8. Adewuyi SA, Shittu SO, Rafindadi AH. Sociodemographic and
clinicopathologic characterization of cervical cancers in northern Nigeria. European Journal of Gynaecological Oncology 2008,29:61-64.
9. Engels EA, Biggar RJ, Hall HI, Cross H, Crutchfield A, Finch JL, et al. Cancer risk in people infected with human immunodeficiency virus in the United States. Int J Cancer 2008,123:187-194.
10. Hung CC, Chen MY, Hsieh SM, Sheng WH, Chang SC. Clinical spectrum, morbidity, and mortality of acquired immunodeficiency syndrome in Taiwan: a 5-year prospective study. J Acquir Immune Defic Syndr 2000,24:378-385. 11. Hung CC, Hsiao CF, Chen MY, Hsieh SM, Chang SY, Sheng WH, et al.
Improved survival of persons with human immunodeficiency virus type 1 infection in the era of highly active antiretroviral therapy in Taiwan. Jpn J Infect Dis 2006,59:222-228.
12. Chin-Hui Y, Mei-Yu C, Yen-Fang H, Hui-Rong L. Guidelines for diagnosis and treatment of HIV/AIDS. 2 nd ed: TCDC; 2008.
16 279 280 281 282 283 284 285 286 287 288 289 290 291 292 293 294 295 296 297 298 299 300 301 302 303 304 305 306 307 308 309 310 311 312 313 47
13. Yang CH, Yang SY, Shen MH, Kuo HS. The changing epidemiology of prevalent diagnosed HIV infections in Taiwan, 1984-2005. Int J Drug Policy 2008,19:317-323.
14. Engels EA, Pfeiffer RM, Goedert JJ, Virgo P, McNeel TS, Scoppa SM, et al. Trends in cancer risk among people with AIDS in the United States 1980-2002. AIDS 2006,20:1645-1654.
15. Bratcher LF, Sahasrabuddhe VV. The impact of antiretroviral therapy on HPV and cervical intraepithelial neoplasia: current evidence and directions for future research. Infect Agent Cancer 2010,5:8.
16. Firnhaber C, Westreich D, Schulze D, Williams S, Siminya M, Michelow P, et al. Highly active antiretroviral therapy and cervical dysplasia in HIV-positive women in South Africa. J Int AIDS Soc 2012,15:1-6.
17. Adler DH, Kakinami L, Modisenyane T, Tshabangu N, Mohapi L, De Bruyn G, et al. Increased regression and decreased incidence of HPV-related cervical lesions among HIV-infected women on HAART. AIDS 2012.
18. Minkoff H, Zhong Y, Burk RD, Palefsky JM, Xue X, Watts DH, et al. Influence of adherent and effective antiretroviral therapy use on human papillomavirus infection and squamous intraepithelial lesions in human immunodeficiency virus-positive women. J Infect Dis 2010,201:681-690. 19. Lillo FB, Ferrari D, Veglia F, Origoni M, Grasso MA, Lodini S, et al. Human
papillomavirus infection and associated cervical disease in human
immunodeficiency virus-infected women: effect of highly active antiretroviral therapy. J Infect Dis 2001,184:547-551.
20. Mwakigonja AR, Torres LM, Mwakyoma HA, Kaaya EE. Cervical cytological changes in HIV-infected patients attending care and treatment clinic at Muhimbili National Hospital, Dar es Salaam, Tanzania. Infect Agent Cancer 2012,7:3.
21. Chiang TL. Taiwan's 1995 health care reform. Health Policy 1997,39:225-239.
22. Cheng CL, Kao YH, Lin SJ, Lee CH, Lai ML. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol Drug Saf 2011,20:236-242.
23. Yu ST, Chang HY, Lin MC, Lin YH. Agreement between self-reported and health insurance claims on utilization of health care: A population study. J Clin Epidemiol 2009,62:1316-1322.
24. Chen MH, Su TP, Chen TJ, Cheng JY, Wei HT, Bai YM. Identification of psychiatric disorders among human immunodeficiency virus-infected 314 315 316 317 318 319 320 321 322 323 324 325 326 327 328 329 330 331 332 333 334 335 336 337 338 339 340 341 342 343 344 345 346 347 348 349 350
Care 2012.
25. NHI. Introduction to the National Health Insurance Research Database (NHIRD), Taiwan. In.
26. TCDC. Stastic data. 2010.
27. Liu CY, Hung YT, Chuang YL, Chen YJ, Weng WS, Liu JS. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Manag 2006, 4:e22.
28. Gay CL, Mayo AJ, Mfalila CK, Chu H, Barry AC, Kuruc JD, et al. Efficacy of NNRTI-Based Antiretroviral Therapy Initiated During Acute HIV Infection. AIDS 2011,25:941-949.
29. Wood E, Hogg RS, Yip B, Harrigan PR, O'Shaughnessy MV, Montaner JS. Effect of medication adherence on survival of HIV-infected adults who start highly active antiretroviral therapy when the CD4+ cell count is 0.200 to 0.350 x 10(9) cells/L. Ann Intern Med 2003,139:810-816.
30. Clifford GM, Polesel J, Rickenbach M, Dal Maso L, Keiser O, Kofler A, et al. Cancer risk in the Swiss HIV Cohort Study: associations with
immunodeficiency, smoking, and highly active antiretroviral therapy. J Natl Cancer Inst 2005,97:425-432.
31. Frisch M, Biggar RJ, Goedert JJ. Human papillomavirus-associated cancers in patients with human immunodeficiency virus infection and acquired
immunodeficiency syndrome. J Natl Cancer Inst 2000,92:1500-1510.
32. Phelps RM, Smith DK, Heilig CM, Gardner LI, Carpenter CCJ, Klein RS, et al. Cancer incidence in women with or at risk for HIV. International Journal of Cancer 2001,94:753-757.
33. Kadhel P, Multigner L, Bardinet F, Goerger-Sow M, Janky E. Cervical
intraepithelial neoplasia and invasive cancer risks in women infected with HIV in the French West Indies. HIV Med 2012,13:79-82.
34. Chen YC, Liu HY, Li CY, Lee NY, Ko WC, Chou CY, et al. Low Papanicolaou Smear Screening Rate of Women with HIV Infection: A
Nationwide Population-Based Study in Taiwan, 2000-2010. J Womens Health (Larchmt) 2013.
35. Dal Maso L, Polesel J, Serraino D, Lise M, Piselli P, Falcini F, et al. Pattern of cancer risk in persons with AIDS in Italy in the HAART era. Br J Cancer 2009,100:840-847.
36. Sekirime WK, Gray R. HIV infection among Uganda women with cervical cancer: a retrospective study. Gynecol Obstet Invest 2007,63:222-228. 37. van Bogaert LJ. Age at diagnosis of preinvasive and invasive cervical
neoplasia in South Africa: HIV-positive versus HIV-negative women. Int J 18 352 353 354 355 356 357 358 359 360 361 362 363 364 365 366 367 368 369 370 371 372 373 374 375 376 377 378 379 380 381 382 383 384 385 386 387 388 389 53
Gynecol Cancer 2011,21:363-366. 390
391 392
Table 1. Demographics of the study population, 2000-2008 (n = 359,501)
Variable HIV-infected women Women in the general population n = 1,360 n = 358,141 P value n (%) n (%) Age¶ <0.001 15-19 22 (1.62) 38656 (10.79) 20-29 576 (42.35) 80678 (22.53) 30-39 421 (30.96) 79484 (22.19) 40-49 206 (15.15) 69299 (19.35) 50-59 89 (6.54) 37775 (10.55) ≥60 46 (3.38) 52249 (14.59) Median (range) 31.6 (15.7-89.0) 37.4 (15-105.7) Urbanization level <0.001 1 (most urbanized) 352 (25.88) 117358 (32.77) 2 566 (41.62) 123078 (34.37) 3 (least urbanized) 442 (32.50) 117704 (32.87) Monthly income (NTD) <0.001 ≤17280 990 (72.79) 153167 (42.77) 17281-26400 237 (17.43) 119879 (33.47) 26401-43900 85 (625) 61488 (17.17) >43901 48 (3.53) 23608 (6.59) Occupation <0.001 Blue-collar 1138 (83.68) 231251 (64.57) White-collar 222 (16.32) 126890 (35.43)
Prior receipt of Pap test 435 (32.00) 131234 (36.6) <0.001
Opioid dependence 192 (14.04) 48 (0.01) <0.001
Receipt of HAART therapy NA
Non-users and ≤0.5 years
962 (70.7) NA
>0.5 years 398 (29.3) NA
Duration of HAART therapy (year) NA
≤0.5 167 (12.3) NA
20 393
>0.5-2 107 (7.9) NA 2-3 47 (3.5) NA >3 244 (17.9) NA Treated OIs 316 (23.2) 61782 (17.3) <0.001 Candidiasis 119 (37.7) 33652 (54.5) HSV 44 (13.9) 11824 (19.1) TB 50 (15.8) 30174 (4.9) VZV 72 (22.8) 8254 (13.4) Others 31 (9.8) 22122 (8.1) History of STDs 209 (15.37) 4 (<0.01) <0.001
NTD, New Taiwan Dollars; OIs, opportunistic infections; STDs, sexually-transmitted diseases; herpes simplex virus, HSV; varicella-zoster virus, VZV; tuberculosis, TB; tuberculosis
¶ For the general population, the age was defined by the date of insurance. 394
395 396 397
Table 2. Age, calendar year, and cancer type incidence and SIR of cervical neoplasia in HIV-infected women and women in the general population (2000-2008)
Cancer type/Age (year) No. of PYs Incidence (1,000 PYs)
Observed Expected SIR 95% CI
CIS 4376.5 1.4 6 1.5 4.0 1.47-8.70 15-29 1769.6 0.6 1 0.2 4.3 0.13-27.86 30-49 2105.4 1.4 3 1.0 3.1 0.62-8.77 ≥50 531 3.8 2 0.2 9.0 1.21-36.12 ICC 4376.5 1.6 7 1.7 4.1 1.66-8.48 15-29 1774.4 0.6 1 0.1 11.4 0.25-55.72 30-49 2106.3 0.9 2 0.9 2.3 0.27-8.03 ≥50 527.5 7.6 4 0.4 8.9 2.73-25.60 Overall 4376.5 9.6 13 3.2 4.1 2.16-6.95 15-19 79.7 0.0 0 0.0 0 NA 20-29 1686.2 3.5 2 0.4 5.0 0.61-18.06 30-39 1355 2.4 1 1.0 1.0 0.03-5.57 40-49 739.5 19.4 4 0.8 5.0 1.36-12.8 50-59 320.7 56.2 5 0.3 16.7 5.41-38.89 ≥60 195.4 21.7 1 0.3 3.3 0.08-18.57
PYs, person-years; SIR, standardized incidence ratio; CIS, cervical cancer in situ; ICC, invasive cervical cancer
22 398 399 400 401 65
Table 3. Hazard ratio of cervical neoplasia (ICD-9: 2331, 180) in relation to receipt of HAART therapy in HIV-infected women
Variables Crude HR (95% CI) P §HR (95% CI) P Trend test§ P for trend
§Model 1:
Receipt of HAART therapy (n = 1,360)
Non- users orand ≤0.5 years(n = 962, 70.7%) Referent Referent
>0.5 years (n = 398, 29.3%) 0.62 (0.18-2.11) 0.44 0.20 (0.05-0.77) 0.02 §Model 2:
Duration of HAART therapy (year) (n = 565)#
≤0.5 (n = 167, 29.6%) Referent Referent
>0.5-2 (n = 107, 18.9%) 0.20 (0.02-1.59) 0.13 0.18 (0.02-1.62) 0.13
2-3 (n = 47, 8.3%) 0.39 (0.05-3.17) 0.38 0.29 (0.03-2.54) 0.26
>3 (n = 244, 43.2%) 0.08 (0.01-0.43) 0.003 0.03 (0.01-0.16) <0.001
§Model 3:
Pattern of HAART use (n = 565) #
≤<0.5 yearLess than 6 months (n = 167, Referent Referent 402
29.6%) >=0.5 years Adherence < 95% (n = 315, 55.8%) 0.23 (0.03-1.94) 0.13 0.10 (0.01-0.89) 0.04 Adherence ≥ 95% (n = 83, 14.7%) 0.19 (0.05-0.72) 0.01 0.09 (0.02-0.36) 0.001 §Model 4:
Pattern of HAART use (n = 565) #
≤<0.5 yearLess than 6 months (n = 167, 29.6%)
Referent Referent
Adherence < 95% (n = 315278, 55.8%) 0.74 (0.09-7.00) 0.79 1.91(0.15-24.52) 0.62 Adherence ≥ 95% (n = 83120, 14.7%) 0.63 (0.04-10.21) 0.75 0.81(0.04-15.15) 0.89 Duration of HAART therapy (year) (n = 565)# 我還是建議不要 model
4,因為雖是有 trend 但也是只有>3 年才有顯著,而且控制 duration 後,adherence 變得就不顯著了 -1.36 0.002 ≤0.5 (n = 167, 29.6%) Referent Referent >0.5-2 (n = 107, 18.9%) 9.00 (2.25-36.02) 0.002 0.84(0.11-6.37) 0.86 24 71
2-3 (n = 47, 8.3%) 6.26 (0.44-89.15) 0.38 0.27 (0.01-5.87) 0.40
>3 (n = 244, 43.2%) 0.50 (0.02-11.89) 0.67 0.01 (0.00-0.34) 0.01
HAART, highly active anti-retroviral therapy; HR, hazard ratio
§Adjusted for age at HIV diagnosis, monthly income, urbanization level, occupation, drug dependence, treated OIs, history of STDs and
frequency of Pap tests after HIV diagnosis
# Including those who received HAART therapy at least once 403
404 405 406
26 407