Evaluation the contribution of personalized Cyclin D1
genotype to triple negative breast cancer risk
Liang-Chih Liua,#
, Chen-Hsien Su
a,d,#, Hwei-Chung Wanga,#, Wen-Shin Chang
a,d, Chia-Wen Tsaia,b, Ming-Chei Maab, Chang-Hai Tsaia, Fuu-Jen Tsaic and Da-Tian Baua,b,d,*aTerry Fox Cancer Research Laboratory, China Medical University Hospital, Taichung,
Taiwan
bGraduate Institute of Basic Medical Science, China Medical University, Taichung, Taiwan
cDepartment of Medical Research, China Medical University Hospital, Taichung, Taiwan dGraduate Institute of Clinical Medical Science, China Medical University, Taichung,
Taiwan
# These authors contributed equally to this work
* Correspondence to: Da-Tian Bau, Terry Fox Cancer Research Lab, China Medical University Hospital, 2 Yuh-Der Road, Taichung, 404 Taiwan, R.O.C. E-mail address:
artbau 2 @ gmail .com
ABSTRACT
Aim: The cell cycle regulator cyclin D1 (CCND1) is an important regulator for G1/S phase transition and plays a critical part in initiation of carcinogenesis. Triple negative breast cancer comprises a very heterogeneous group of cancer cells, but little is known about what is wrong in the genome of these patients. The study aimed at investigating the contribution of CCND1 genotype to individual triple negative breast cancer susceptibility.
Materials: A total of 2464 native Taiwan subjects consist of 1232 breast cancer cases and 1232 controls were enrolled in this hospital-based case-control study, and
CCND1 A870G (rs9344) genotyping was analyzed by polymerase chain
reaction-restriction fragment length polymorphism (PCR-RFLP). We have also performed risk-stratified subgroup analyses to determine the association between the genotype and age-related characteristics of breast cancer subgroups.
Results: Although the results showed that there were no significant difference between breast cancer and control groups in the distribution of the genotypic and allelic frequencies in the CCND1 genotype, however, CCND1 A870G (rs9344) GG genotype was especially less prevalent in breast cancer patients who were younger than 55 years (OR=0.62, 95%CI=0.43–0.89, P=0.0362), with first menarche earlier than 12.2 years (OR=0.61, 95% CI=0.42–0.87, P=0.0241), with menopause earlier
than 49.0 years (OR=0.57, 95%CI=0.39–0.82, P=0.0093), or had triple-negative breast cancer (OR=0.28, 95%CI=0.13–0.62, P=0.0006). These valuable findings suggested that CCND1 A870G (rs9344) is a potential predictive marker for triple negative breast cancer in Taiwanese women and the authors sincerely hope these findings will help us to fight against the most tough subtype in clinical management.
1. Introduction
Breast cancer is one of the most common malignancies in women worldwide today, and the morbidity and mortality of breast cancer was not decreased as the development of anticancer drugs [1]. Breast cancer in Asia is characterized by a lower incidence than in Western populations, but is still the leading cancer in Asian women, and an issue of extraordinary public health concern. Asian breast cancer is characterized by early tumor onset, showing a relatively younger median age at diagnosis. In Taiwan, breast cancer is the second leading cancer, important for its high incidence, high mortality, and early onset [2,3]. Most of women are exposed to these well-known environmental risk factors for cancer, but only a portion of exposed individuals develop breast cancer, suggesting a wide variation in individual susceptibility to breast carcinogenesis.
Cyclin D1 (CCND1) plays a critical role in controlling the G1/S phase transition of the cell cycle [4], which accomplishes this gate-keeping role by forming a complex with its partners CDK 4 or CDK6 [4,5]. Some reports have demonstrated that CCND1 may involve in the development of some types of tumors in a CDK-independent pattern [6,7]. Dysregulation of CCND1 is a commonly observed character of human cancers, and frequently an overexpression of CCND1 has been reported as a potential biomarker in various types of human cancer [8-10]. However, the underlying
mechanisms of the CCND1 overexpression and its relationship to breast cancer progression are poorly understood. Previously, Terry fox Cancer Research Lab in China Medical University has found that CCND1 genotypes were positively associated with other types of cancer in Taiwan [11-15]. Currently, we are interested not only to reveal the contribution of genotypes to breast cancer, but to the toughest subtype of breast cancer in clinical treatment, the triple negative breast cancer.
Therefore, in the study, we performed a genotyping work to determine the association between the CCND1 A870G (rs9344) polymorphism and breast cancer risk in Taiwanese women and additional analyses to evaluate the contribution of this SNP to breast cancer patients with specific clinicopathological features, such as those of triple negative breast cancer.
2. Materials and methods 2.1. Study population
One thousand two hundred and thirty two cancer patients diagnosed with breast cancer were recruited at the outpatient clinics of general surgery at the China Medical University Hospital, Taichung, Taiwan, Republic of China. The clinical characteristics of patients including histological details were all defined by expert surgeons. The slides were reviewed and scored by two independent pathologists. For ER, PR, and p53 immunoassaying, nuclear staining in 10% of neoplastic cells was
used as a positive cutoff. A Ki67-labelling index of >30% was considered positive. HER-2/neu results were determined according to the package insert and guidelines of the American Society of Clinical Oncology and College of American Pathologists [16]. All patients voluntarily participated, completed a self-administered questionnaire and provided peripheral blood samples. The same amounts of age-matched non-breast cancer healthy volunteers as controls were selected after initial random sampling from the Health Examination Cohort of the hospital. The exclusion criteria of the control group included previous malignancy, metastasized cancer from other or unknown origin, and any familial or genetic diseases. Both groups completed a short questionnaire which included habits. Our study was approved by the Institutional Review Board of the China Medical University Hospital (DMR96-IRB-240) and written-informed consent was obtained from all participants.
2.2. Genotyping conditions
Genomic DNA was prepared from peripheral blood leukocytes using a QIAamp Blood Mini Kit (Blossom, Taipei, Taiwan) and the genotyping processes were performed as our previous studies [11-15]. Briefly, the primers used for CCND1 A870G were: forward GTG AAG TTC ATT TCC AAT CCG C-3’, and reverse 5’-GGG ACA TCA CCC TCA CTT AC-3’, and polymerase chain reaction (PCR) cycling conditions were: one cycle at 94oC for 5 min; 35 cycles of 94oC for 30 s, 55oC
for 30 s, and 72oC for 30 s, and a final extension at 72oC for 10 min.
2.3. RFLP conditions
After the PCR procedure for the CCND1 A870G genotyping, the resultant 167 bp PCR product was mixed with 2 U Nci I and incubated for 3 h at 37C. The G form PCR products could be further digested while the A form could not. Two fragments 145 bp and 22 bp were present if the product was digestible G form. Then, 10 l of product was loaded into a 3% agarose gel containing ethidium bromide for electrophoresis. The genotype analysis was performed by two researchers independently and blindly. Ten percent of the samples were randomly selected for direct sequencing and the results were 100% concordant.
2.4. Statistical analyses
To ensure that the controls used were representative of the general population and to exclude the possibility of genotyping error, the deviation of the genotype frequencies of CCND1 single nucleotide polymorphisms in the control subjects from those expected under the Hardy-Weinberg equilibrium was assessed using the goodness-of-fit test. Pearson’s Chi-square test or Fisher’s exact test (when the expected number in any cell was less than five) was used to compare the distribution of the CCND1 genotypes between cases and controls. Data was recognized as significant when the statistical P-value was less than 0.05.
3. Results
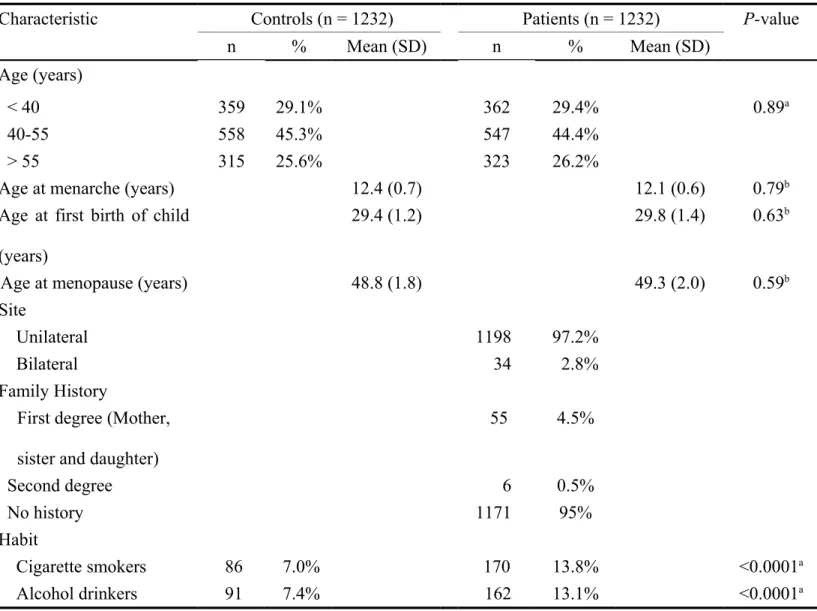
A total of 1232 patients diagnosed with breast cancer and the same amount of matched controls were included in this study, compared and summarized in Table 1. The ages of patients and controls are all well matched and no difference in age, age at menarche, age at first birth of child, among the subjects were observed (P>0.05) (Table 1). As for the individual behaviors, the cigarette smoking and alcoholism were both risk factors for breast cancer in this population (P<0.05) (Table 1).
The frequencies of the genotypes and alleles of the CCND1 A870G in the breast cancer and control groups are shown in Table 2. First, the results of genotyping analysis revealed the distribution of CCND1 A870G genotype was not significantly different between breast cancer and control groups (P=0.1949) (Table 2). The odds ratios of the AG and GG were 0.95 and 0.80 (95%CI=0.79-1.15 and 0.62-1.03) compared to the AA wild-type genotype. Second, we have performed the dominant and recessive comparison, finding that the odds ratios of GG versus AA+AG and AG+GG versus AA were 0.82 and 0.92 (95%CI=0.66-1.03 and 0.77-1.10, P=0.0931 and 0.3793). Last, there was neither significant difference between breast cancer and control groups in the distribution of allelic frequency (OR=0.92, 95%CI=0.82-1.03, P=0.1442). To sum up, individuals who carried G allele (AG and GG) had only a
slightly but not statistically protective effect of developing breast cancer compared to those who carried the AA wild type genotype (Table 2).
We are interested in the association of clinicopathologic characteristics with CCND1 A870G genotypes. Given that distinct subtypes of breast cancer have different mechanisms of carcinogenesis, we analyzed the association among CCND1 A870G genotypes with age-related and clinicopathologic characteristics of breast cancer patients (Tables 3 and 4). The data showed that GG genotype at CCND1 A870G was less prevalent in breast cancer patients who were younger than 55 years (OR=0.62, 95%CI=0.43–0.89, P=0.0362), with first menarche earlier than 12.2 years (OR=0.61, 95% CI=0.42–0.87, P=0.0241), with menopause earlier than 49.0 years (OR=0.57, 95%CI=0.39–0.82, P=0.0093), or had triple-negative breast cancer (OR=0.28, 95%CI=0.13–0.62, P=0.0006) (Tables 3 and 4). The difference in the distribution of the genotype among breast cancer patients stratified by other factors, including first full pregnant (Table 3) and Ki67 status (Table 4), was not statistically significant.
4. Discussion
For years, Terry Fox Cancer Research Lab in China Medical University has keeping on the anticancer task via the translational circle from genomic biomarker revealing,
anticancer drug discovery, cell and animal model establishment for drug efficacy and genotype-phenotype correlation investigation, and clinical personalized application. In this hospital-based case-control study, our team has genotyped a famous SNP CCND1 A870G studying its association with Taiwanese breast cancer risk in central Taiwan. With a collection of samples from a quite large population, we have found that the GG genotype in CCND1 A870G plays a protective role for triple-negative breast cancer, and in early onset (< 55 years), early menarche (<12.2 years) and premenopausal (<49 years) Taiwanese women.
At the first step, we performed the genotype work routinely but the results showed that CCND1 A870G genotype was not associated with breast cancer susceptibility. Since we have almost collected the largest breast cancer population in Taiwan, 1232 cases and age-matched controls, the strategy of enlargement investigated subjects is not in urgent need. It is well believed that estrogen exposure is closely related to breast cancer risk, and there is no denying that age is the strongest demographic risk factor for most malignancies; 75% of malignancies occur in patients older than 55 years [17]. With the large enough sample size, we were confident to evaluate the contribution of this SNP to breast cancer patients with specific clinicopathological features by stratification analysis. The estrogen- and age-related factors included onset age, age at menarche, age at first birth of child, and age at
menopause (Table 3). In addition, we are interested in evaluating the contribution of this SNP to triple negative breast cancer. In the present study, 104 breast cancer patients was identified to be triple negative breast cancer patients, so named because of its negative expression of ER, PR, and HER-2/neu [18], is characterized by its aggressiveness and higher rates of recurrence and metastasis. It is of our interest since existing targeted therapies which are effective in other subtypes of breast cancer, were not effective in dealing with triple negative breast cancer patients. Typically, triple negative breast cancer occurs in young patients whose disease is associated with genetic variations on BRCA1 and other hereditary genes, such as hOGG1 and EGFR2 [16, 19, 20]. The cyclin D1 (coded by CCND1) plays as the first gatekeeper in cell cycle, and the copy number alterations of CCND1 was reported to be differentially more frequent in triple negative breast cancer samples than in those non-triple negative breast cancer ones [21]. However, there is no report investigating the association of SNPs on CCND1 with triple negative breast cancer risk. In this study, the results showed that the genotype of CCND1 A870G was not associated with breast cancer risk as in other cancers [11-15], but more valuable, the stratified analysis showed that the GG genotype of CCND1 A870G plays a protective role for triple-negative breast cancer (Table 4), and in early onset (<55 years), early menarche (<12.2 years) and premenopausal (<49 years) Taiwanese women (Table 3). It is also
found that the Ki67 status, which was reported to be a potential indicator to triple negative breast cancer [22], were not associated with CCND1 A870G genotype (Table 4).
In recent years, rapidly accumulated information in cancer genotyping indeed has done a great favor to translational medicine and personalized therapy. However, we still have a long way to go to make Taiwan cancer history. The first successful step seemed to be fulfilled by the cooperation between clinicians and basic scientists in Taiwan. Since heredity plays an important role in cancer susceptibility, we have to pay more attention to the genetic conservation and independency of Taiwan from Western countries, and respect the profound difference equally to globalization. The translational studies in Taiwan, together with the participation of experts in nutrition and care-taking, the cooperation of patients and relatives, should be strengthened and encouraged as much as possible in Taiwan. In this study, we demonstrated that the GG genotype of CCND1 A870G plays a protective role for triple-negative breast cancer, and in early onset, early menarche and premenopausal Taiwanese women. We sincerely hope each piece of our continue work can contribute to speeding the success of personalized therapy and medication, and the war against cancers, especially those in our loved Taiwan.
This work was supported by China Medical University Hospital (grant number: DMR-103-019) and the Terry Fox Cancer Research Foundation. The authors deeply appreciate the help from Tsai-Ping Ho, Chieh-Lun Hsiao, Lin-Lin Hou, Chao-Yi Lai, Chia-En Miao, Tzu-Chia Wang, Yun-Ru Syu and Tissue Bank.
REFERENCES
[1] Jemal A, Center MM, DeSantis C and Ward EM. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol Biomarkers Prev 2010;19:1893-907.
[2] Cheng SH, Tsou MH, Liu MC, Jian JJ, Cheng JC, Leu SY, et al. Unique features of breast cancer in Taiwan. Breast Cancer Res Treat 2000;63:213-23. [3] Kuo WH, Yen AM, Lee PH, Chen KM, Wang J, Chang KJ, et al. Cumulative
survival in early-onset unilateral and bilateral breast cancer: an analysis of 1907 Taiwanese women. Br J Cancer 2009;100:563-70.
[4] Sherr CJ. Cancer cell cycles. Science 1996;274:1672-7.
[5] Sherr CJ. D-type cyclins. Trends Biochem Sci 1995;20:187-90.
[6] Coqueret O. Linking cyclins to transcriptional control. Gene 2002;299:35-55. [7] Fu M, Wang C, Li Z, Sakamaki T and Pestell RG. Minireview: Cyclin D1:
normal and abnormal functions. Endocrinology 2004;145:5439-47.
[8] Jayasurya R, Sathyan KM, Lakshminarayanan K, Abraham T, Nalinakumari KR, Abraham EK, et al. Phenotypic alterations in Rb pathway have more prognostic influence than p53 pathway proteins in oral carcinoma. Mod Pathol 2005;18:1056-66.
[9] Bova RJ, Quinn DI, Nankervis JS, Cole IE, Sheridan BF, Jensen MJ, et al. Cyclin D1 and p16INK4A expression predict reduced survival in carcinoma of the anterior tongue. Clin Cancer Res 1999;5:2810-9.
[10] Michalides R, van Veelen N, Hart A, Loftus B, Wientjens E and Balm A. Overexpression of cyclin D1 correlates with recurrence in a group of forty-seven operable squamous cell carcinomas of the head and neck. Cancer Res 1995;55:975-8.
[11] Shih LC, Tsai CW, Tsai MH, Tsou YA, Chang WS, Li FJ, et al. Association of cyclin D1 genotypes with nasopharyngeal carcinoma risk. Anticancer Res 2012;32:1093-8.
[12] Hsia TC, Liu CJ, Lin CH, Chang WS, Chu CC, Hang LW, et al. Interaction of CCND1 genotype and smoking habit in Taiwan lung cancer patients.
Anticancer Res 2011;31:3601-5.
[13] Lin HH, Ke HL, Hsiao KH, Tsai CW, Wu WJ, Bau DT, et al. Potential role of CCND1 G870A genotype as a predictor for urothelial carcinoma susceptibility and muscle-invasiveness in Taiwan. Chin J Physiol 2011;54:196-202.
[14] Lin HH, Ke HL, Hsiao KH, Tsai CW, Wu WJ, Bau DT, et al. CCND1 1722 polymorphism and potential relevance to upper tract urothelial cancer. Anticancer Res 2011;31:1043-7.
[15] Tsai MH, Tsai CW, Tsou YA, Hua CH, Hsu CF and Bau DT. Significant association of cyclin D1 single nucleotide polymorphisms with oral cancer in taiwan. Anticancer Res 2011;31:227-31.
[16] Wolff AC, Hammond ME, Schwartz JN, Hagerty KL, Allred DC, Cote RJ, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch Pathol Lab Med 2007;131:18-43.
[17] Edwards BK, Howe HL, Ries LA, Thun MJ, Rosenberg HM, Yancik R, et al. Annual report to the nation on the status of cancer, 1973-1999, featuring implications of age and aging on U.S. cancer burden. Cancer 2002;94:2766-92.
[18] Lee E, McKean-Cowdin R, Ma H, Spicer DV, Van Den Berg D, Bernstein L, et al. Characteristics of triple-negative breast cancer in patients with a BRCA1 mutation: results from a population-based study of young women. J Clin Oncol 2011;29:4373-80.
[19] Liu X, Xiao N, Guo W, Wu Y, Cai Z, He Q, et al. The hOGG1 gene 5'-UTR variant c.-53G>C contributes to the risk of gastric cancer but not colorectal cancer in the Chinese population: the functional variation of hOGG1 for gastric cancer risk. J Cancer Res Clin Oncol 2011;137:1477-85.
[20] Xie H, Xia K, Rong H and Chen X. Genetic polymorphism in hOGG1 is associated with triple-negative breast cancer risk in Chinese Han women. Breast 2013;22:707-12.
[21] Zhang S, Shao Y, Hou G, Bai J, Yuan W, Hu L, et al. QM-FISH analysis of the genes involved in the G1/S checkpoint signaling pathway in triple-negative breast cancer. Tumour Biol 2013.
[22] Li XR, Liu M, Zhang YJ, Wang JD, Zheng YQ, Li J, et al. CK5/6, EGFR, Ki-67, cyclin D1, and nm23-H1 protein expressions as predictors of pathological complete response to neoadjuvant chemotherapy in triple-negative breast cancer patients. Med Oncol 2011;28 Suppl 1:S129-34.
Table 1. Distributions of demographic and life-style of breast cancer patients and the matched controls.
Characteristic Controls (n = 1232) Patients (n = 1232) P-value
n % Mean (SD) n % Mean (SD)
Age (years)
< 40 359 29.1% 362 29.4% 0.89a
40-55 558 45.3% 547 44.4%
> 55 315 25.6% 323 26.2%
Age at menarche (years) 12.4 (0.7) 12.1 (0.6) 0.79b
Age at first birth of child (years)
29.4 (1.2) 29.8 (1.4) 0.63b
Age at menopause (years) 48.8 (1.8) 49.3 (2.0) 0.59b
Site
Unilateral 1198 97.2%
Bilateral 34 2.8%
Family History
First degree (Mother, sister and daughter)
55 4.5% Second degree 6 0.5% No history 1171 95% Habit Cigarette smokers 86 7.0% 170 13.8% <0.0001a Alcohol drinkers 91 7.4% 162 13.1% <0.0001a