Kaohsiung J Med Sci August 2003 • Vol 19 • No 8 C.S Wang, K.B. Tsai, J.R. Tsai, et al
428
Received: February 21, 2003 Accepted: May 27, 2003 Address correspondence and reprint requests to: Dr. Ming-Shyan Huang, Division of Chest Medicine, Department of Internal Medicine, Kaohsiung Medical University Hospital, 100 Shih-Chuan 1st Road, Kaohsiung 807, Taiwan.
E-mail: [email protected]
Malignant fibrous histiocytoma (MFH) is the most common malignant soft tissue tumor in older adults, most frequently involving the extremities, retro-peritoneum, and trunk, but it is rare as a primary tumor of the lung [1–3]. Chest roentgenography, chest computerized tomography (CT), and magnetic reso-nance imaging (MRI) disclose a well-defined mass shadow that is not very lobulated [3–5]. Early diagnosis is very important because of the poor prognosis. Bronchoscopy and percutaneous needle aspiration are of limited value in differential diagnosis, and thoracotomy is warranted for definitive diagnosis [2,6]. Surgery is the primary mode of therapy [7].
We report a case of primary MFH of the lung illustrating the clinical, radiologic, histologic, immunohistochemical, and ultrastructural features, and the difficulty in treating such cases.
C
ASEP
RESENTATIONAn 86-year-old male was admitted to our hospital in February 2002 due to insidious onset of exertional dyspnea and poor appetite lasting for 1 month. He had previously been quite well and had no history of smoking. Physical examination revealed pale conjunctivae and decreased breath sounds over the left basal lung field. Laboratory examinations showed mild anemia, hyponatremia, hypoalbuminemia, and a high C-reactive protein concentration. Tumor markers, including carcinoembryonic antigen, tissue plasmin antigen, and squamous cell carcinoma antigen, were within normal limits. Chest roentgenography demonstrated a 9 × 15 cm, pleural-based opacity in the left lower lobe (Figure 1). Chest CT revealed a
well-© 2003 Elsevier. All rights reserved.
P
RIMARY
M
ALIGNANT
F
IBROUS
H
ISTIOCYTOMA
OF
THE
L
UNG
: A C
ASE
R
EPORT
Chuan-Sheng Wang, Kun-Bow Tsai,1 Jong-Rung Tsai, Chau-Chyun Sheu, Jen-Yu Hung, Te-Hung Hsu, and Ming-Shyan Huang
Division of Chest Medicine, Department of Internal Medicine, and 1Department of
Pathology, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan.
Malignant fibrous histiocytoma (MFH) is the most common soft tissue sarcoma in adults. However, primary MFH of the lung is rare, with only a few cases reported in the literature. Here, we report the case of an 86-year-old male who was admitted to our hospital with the chief complaint of exertional dyspnea and poor appetite. Chest roentgenography revealed a 9 × 15 cm, pleural-based opacity in the left lower lobe. Chest computerized tomography disclosed a well-defined mass with heterogeneous density in the left lower lung field. The diagnosis of MFH was confirmed by thoracoscopic lung biopsy and pathologic examination. Supportive care was given because of extreme old age and poor performance status (the patient’s Karnofsky performance status was 30). The patient died from respiratory failure 2 months later.
Key Words: malignant fibrous histiocytoma, sarcoma
Primary malignant fibrous histiocytoma of the lung
429 Kaohsiung J Med Sci August 2003 • Vol 19 • No 8
defined mass with heterogeneous density in the left lower lung field. Local extension to the left chest wall and right pleural effusion were noted (Figure 2). Gallium whole-body scan revealed intensively increased radioactivity in the anterolateral aspect of the left lower chest with a photopenic area in the adjacent middle portion and gradually increasing contrast throughout the serial 6-, 24- and 48-hour images.
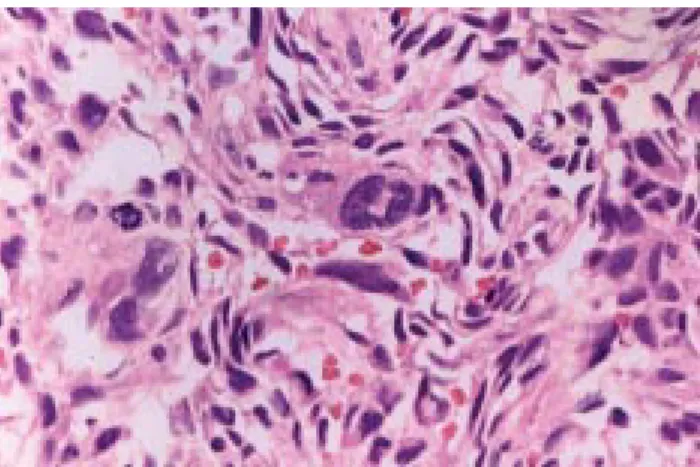
Thoracoscopic lung biopsy yielded eight tissue fragments, measuring up to 1.8 × 1.1 × 0.8 cm. Grossly, they were reddish, soft and elastic, or whitish, soft and jelly-like. A storiform pattern of spindle cells and multinucleated giant cancer cells with atypical mitotic figures were seen on microscopy (Figures 3 and 4). Hemorrhage and necrosis were noted. Immuno-histochemical studies were negative for cytokeratin, CK5/6, and calretinin, but positive for vimentin. Therefore, MFH was diagnosed. Because the patient was extremely old in age and had poor performance status (Karnofsky performance status = 30), he received supportive care. He died in April 2002 from respiratory failure.
D
ISCUSSIONMFH is the most common (10%) soft tissue sarcoma in adults and mostly occurs in males. It mainly arises from soft tissue in the extremities (68%), the retroperitoneum (16%), and lung (7.5%) [1]. Primary MFH comprises 0.04% of all pulmonary malignant tumors [2]. There must be no evidence of another primary site on careful physical examination and radiologic evaluation before MFH can be considered a primary rather than a metastatic lesion. The mean age of patients with primary lung MFH is 55 years (range, 10–80 years) [7,8]. There are no predisposing factors. The most common complaints are cough, dyspnea, fatigue, hemoptysis, weakness, headache, fever, chills, weight loss, and chest pain. Patients may be asymp-tomatic at presentation [7,9–11]. Our patient was older than usual (86 years old), and his initial presentation was exertional dyspnea and poor appetite.
Typically, lung MFH appears as a large, solitary, well-circumscribed, non-cavitating, non-calcified, peripheral lung mass with a slight preponderance in the middle and lower lobes. Approximately 20% of patients have associated pleural effusion [3,4]. CT and
Figure 1. Chest roentgenography shows a 9 × 15 cm, pleural-based opacity in the left lower lobe.
Figure 2. Chest computerized tomography reveals a well-defined mass with heterogeneous density in the left lower lung field. Local extension to the left chest wall and right pleural effusion are evident.
MRI can provide useful information to demonstrate the nature and extent of tumor invasion [5]. On CT, lung MFH appears to be of soft-tissue density, sometimes with central areas of low attenuation. The tumor displaces rather than invades local structures. In our case, imaging showed a huge, well-defined tumor in the left lower lobe with soft-tissue density
Kaohsiung J Med Sci August 2003 • Vol 19 • No 8 C.S Wang, K.B. Tsai, J.R. Tsai, et al
430
the storiform variety. No definite relationship between survival and histology has been identified because of the predominance of the storiform subtype. The most significant prognostic factors are the presence of metastases, local recurrence, and more than 15% necrosis [13]. In our case, histology revealed a storiform pattern in spindle cells and multinucleated giant cells. Hemorrhage and necrosis were noted. Immuno-histochemical studies were negative for cytokeratin, CK5/6, and calretinin, but positive for vimentin.
Bronchoscopy and percutaneous needle aspiration are of limited value in differential diagnosis, and thoracotomy is warranted for definitive diagnosis [2,6]. Mediastinoscopy is not useful because MFH usually disseminates hematogenously and does not commonly invade lymphatics [2,12]. The brain is a common site of metastasis [9,14–17].
Complete tumor resection is the treatment of choice, with high rates of local and distant recurrence reported. The roles of radiation and chemotherapy have not been clearly defined [7]. Systemic chemotherapy has been used largely for metastatic disease, but has yielded poor results [7,15,18,19]. In our case, the patient only received supportive care due to his extreme old age and poor performance status.
In conclusion, MFH of the lung is a rare clinical entity with variable outcome. Aggressive surgery is the mainstay of treatment. The role of adjuvant radiation and chemotherapy remains undefined.
R
EFERENCES1. Nascimento AG, Unni KK, Bematz PE. Sarcomas of the lung. Mayo Clin Proc 1982;57:355–9.
2. Janssen JP, Mulder JJ, Wagenaar SS, et al. Primary sarcoma of the lung: a clinical study with long-term follow-up. Ann Thorac Surg 1994;58:1151–5.
3. Ros PR, Viamonte M Jr, Rywlin AM. Malignant fibrous histiocytoma: mesenchymal tumor of ubiquitous origin. AJR Am J Roentgenol 1984;142:753–9.
4. Reifsnyder AC, Smith HJ, Mullhollan TJ, Lee EL. Malignant fibrous histiocytoma of the lung in a patient with a history of asbestos exposure. AJR Am J Roentgenol 1990;154: 65–6.
5. Dai J, Jiang L, Zhang Y. Imaging findings of malignant fibrous histiocytoma in the lung. Chung-Hua Chung Liu Tsa Chih 1997;19:130–3. (In Chinese)
6. Pui MH, Yu SP, Chen JD. Primary intrathoracic malignant fibrous histiocytoma and angiosarcoma. Australas Radiol 1999;43:3–6.
Figure 3. Histopathology of a thoracoscopic biopsy shows a storiform pattern of spindle cells and scattered multinucleated giant cancer cells. (Hematoxylin & eosin, × 20)
Figure 4. Histopathology of a thoracoscopic biopsy shows spindle cells and multinucleated giant cancer cells with mitotic figures. (Hematoxylin & eosin, × 80)
and no mediastinal or hilar lymph node involvement. The tumor had local extension to the left chest wall and right pleural effusion was also noted.
Immunohistochemical examination permits the line of differentiation to be established in a number of primary or metastatic sarcomas of the lung. Mesenchymal neoplasms are positive for vimentin and negative for cytokeratin. Both leiomyosarcoma and rhabdomyosarcoma contain myoglobin. S-100 protein is a marker for neurogenic sarcoma. MFH tumor cells show positive reactions for vimentin, α1
-antitrypsin and α1-antichymotrypsin, but are negative
for cytokeratin, desmin, myoglobin, smooth muscle actin, and S-100 protein [8]. Enzinger and Weiss described four histologic types of soft-tissue MFH: storiform pleomorphic; myxoid; giant cell; and inflammatory [12]. Most primary lung tumors are of
Primary malignant fibrous histiocytoma of the lung
431 Kaohsiung J Med Sci August 2003 • Vol 19 • No 8
7. Halyard MY, Camoriano JK, Culligan JA, et al. Malignant fibrous histiocytoma of the lung: report of four cases and review of the literature. Cancer 1996;78:2492–7.
8. McDonnell T, Kyriakos M, Roper C, Mazoujian G. Malignant fibrous histiocytoma of the lung. Cancer 1988;61:137–45. 9. Misra DP, Sunderrajan EV, Rosenholtz MJ, Hurst DJ. Malignant
fibrous histiocytoma in the lung masquerading as recurrent pulmonary thromboembolism. Cancer 1983;51:538–61. 10. Lessel W, Erbstosser E. Malignant fibrous histiocytoma of the
lung. Z Erkr Atmungsorgane 1984;163:70–4. (In German) 11. Casey TC, Peddle LM. Primary pulmonary fibrous
histiocytoma: report of three cases. Can J Surg 1988;31: 251–3.
12. Enzinger FM, Weiss SW. Malignant fibrohistiocytic tumors. In: Enzinger FM, Weiss SW, eds. Soft Tissue Tumors, 3rd
ed. St. Louis: CV Mosby Co, 1995:351–80.
13. Gal AA, Koss MN, McCarthy WF, Hochholzer L. Prognostic
factors in pulmonary fibrohistiocytic lesions. Cancer 1994;73: 1817–24.
14. Kern WH, Hughes RK, Meyer BW, Harley DP. Malignant fibrous histiocytoma of the lung. Cancer 1979;44:1793–801. 15. Sajjad SM, Begin LR, Dail DH, Lukeman JM. Fibrous
histiocytoma of the lung: a clinicopathologic study of two cases. Histopathology 1981;5:325–34.
16. Ismailer I, Khan A, Leonidas JC, et al. Computed tomography of primary malignant fibrohistiocytoma of the lung. Comput Radiol 1987;11:37–40.
17. Palmer AS, Passman JM, Vega JG. Malignant fibrous histiocytoma of the lung. Illinois Med J 1988;174:290–1. 18. Lee JT, Shelburne JD, Linder J. Primary malignant fibrous
histiocytoma of the lung: a clinicopathologic and ultra-structural study of five cases. Cancer 1984;53:1124–30. 19. Yousem SA, Hochholzer L. Malignant fibrous histiocytoma of