Increased Incidence of juvenile onset systemic lupus erythematosus in atopic dermatitis cohort
Chang-Ching Wei, MD,a,b Cheng-Li Lin, MS,c,d Te-Chun Shen, MD,b,e Tsai-Chung Li,
PhDd, Fung-Chang Sung, PhD d
aDepartment of Pediatrics, China Medical University Hospital, Taichung, Taiwan; bCollege of Medicine, China Medical University, Taichung, Taiwan;
cManagement Office for Health Data, China Medical University Hospital, Taichung,
Taiwan;
dDepartment of Public Health, China Medical University, Taichung, Taiwan;
eDivision of Pulmonary and Critical Care Medicine, Department of Internal Medicine,
China Medical University Hospital, Taichung, Taiwan
fDepartment of Medical Research, China Medical University Hospital, Taichung,
Taiwan;
Address correspondence to: Fung-Chang Sung, PhD
Department of Public Health, China Medical University; #91 Hsueh-Shih Road, Taichung City 404, Taiwan; Tel: +886-4-2205-3366 ext. 6220; Fax: +886-4-2207-0429; E-mail: [email protected]
Short title: Juvenile onset systemic lupus erythematosus in atopic dermatitis Key words: atopic dermatitis, juvenile onset systemic lupus erythematosus Abstract words Text words Table Figure Abbreviations Atopic dermatitis: AD
Juvenile systemic lupus erythematous: JSLE Systemic lupus erythematous: SLE
T helper1 cells: Th1 T helper2 cells: Th2
DMR-100-076) from China Medical University Hospital, Taiwan Department of Health Clinical Trial and Research Center and for Excellence (DOH102-TD-B-111-004), Taiwan Department of Health Cancer Research Center for Excellence
(DOH102-TD-C-111-005), Bureau of Health Promotion, Department of Health, R.O.C. (Taiwan) (DOH99-HP-1205), and International Research-Intensive Centers of Excellence in Taiwan (I-RiCE) (NSC101-2911-I-002-303).
Financial Disclosure: The authors have indicated that they have no financial relationships relevant to this article to disclose.
Conflict of Interest: None. Contributor’s Statement:
Chang-Ching Wei, Te-Chun Shen: conceptualized and designed the study, drafted the initial manuscript, and approved the final manuscript as submitted.
Cheng-Li Lin, Tsai-Chung Li: carried out the initial analyses, reviewed and revised the manuscript, and approved the final manuscript as submitted.
Fung-Chang Sung: coordinated and supervised data collection, critically reviewed the manuscript, and approved the final manuscript as submitted.
ABSTRACT
Objective:Children with systemic lupus erythematosus (SLE) especially have a more aggressive course and a worse outcome. Previous reports have posed a possible link
between SLE and allergy. However, there have been relatively few epidemiologic
studies to explore the relationship between atopic dermatitis (AD) and SLE in
children. This population-based cohort study is to investigate the incidence and risk of
juvenile onset SLE (JSLE) among children with AD.
Methods: From 2000 to 2007, 192,357 children with newly diagnosed AD and 769,428 randomly selected non-AD controls were enrolled. A multivariate Cox
proportional hazard regression model was used to measure the incidence rate and risk
of JSLE in AD compared to non-AD cohorts.
Results: Overall, the SLE incidence was 2.92-fold greater in the AD cohort than in the non-AD cohort (3.25 vs. 1.12 per 100,000 person-years, 95%CI=1.85-4.60) in the
following 9 years and this pattern was similar in both gender. The incidence markedly
increased when AD children older than 12 years (22 per 100,000 person-years, HR
6.6, 95% CI = 2.88-13.1) compared to non-AD cohort. The HR of JSLE increased
when AD children with more related medical visits per year, from 1.55 (95% CI
=0.88-2.76) for those having 3 or fewer visits to 66.3 (95% CI =33.1-132.8) for those
patients with AD was highest within five year of follow-up after AD has been
diagnosed (HR=4.02, 95%CI=2.83-7.08).
Conclusion: Children with AD have higher incidence and risk to develop JSLE than no-AD children regardless of gender. In the future, the mechanism of AD on JSLE
development should be better elucidated to establish innovative disease intervention
BACKGROUND
Children with systemic lupus erythematosus (SLE) have more serious organ
involvement, a more aggressive course and a worse outcome.1, 2The annual incidence
of juvenile onset SLE (JSLE) is less than one per 100,000 children per year. The low
incidence makes it hard to perform a study with a substantial number of patients.3 To
date, SLE has neither a specific treatment for disease healing nor a diagnostic tool for
disease prevention. Long-term immunosuppressive therapy is still the mainstay of
treatment, with multiple adverse side effects observed. Although great efforts have
put towards better understanding and developing treatment strategies for SLE over the
past 60 years, the etiology of SLE has not clearly established.4, 5
A possible link has been posed between SLE and allergic diseases, but the nature
between these disorders remain unclear. 6-10 More recently, patients with SLE were
noted to have elevated serum IgE which was associated with SLE disease activity.11-16
Atopic dermatitis (AD), an IgE mediated chronic skin inflammatory disease. AD is
mostly onset preceding other allergic disorders in infancy and early childhood.17
Interestinly, whether the Th2 related disease, AD, contribute to the development of
Th1 related autoimmune disease, JSLE has been unknown. In addition, human
epidemiologic studies that explore the association between AD and JSLE in children
hypothesis of childhood onset allergic disease, AD, may contribute to the
METHODS Data Sources
Our retrospective cohort study used research data from reimbursement claims of the
National Health Insurance (NHI) Program in Taiwan, which was implemented in
March 1995 and covers >99% of 23.74 million Taiwan residents. The National Health
Research Institutes (NHRI) is responsible to manage the insurance claims data that
records all beneficiaries’ medical services, including outpatient and inpatient
demographics, primary and second diagnoses, procedures, prescriptions, and medical
expenditures, for administrative and research uses
(http://www.nhi.gov.tw/english/index.aspx).18, 19 This study used a dataset consisting
of a randomly selected sample of half of all insured children in Taiwan. This study
was exempt from the Institutional Review Board because the NHIRD database
contains de-identified person identifiers and is publicly available through the proper
application process. The International Classification of Disease, Ninth Revision
(ICD-9), was used to define diagnostic disease codes, which had been reported with high
accuracy and validity for study using NHIRD database. 20,21
Study design and subjects
The atopic dermatitis (AD) cohort included patients younger than 18 years with AD
(ICD-9-CM 691) diagnosed from 2000 to 2007 with the date of AD diagnosis as the
in the same years frequency-matched without AD by sex, age, urbanization of
residence area, and parental occupation, and index year. For each child with AD, 4
comparison children were selected to increase the statistical power. We excluded
children who had missing data on date of birth, sex, or with preexisting systemic
lupus erythematosus (SLE) (ICD-9-CM 710.0) from the study cohorts. Each child was
followed from the index date until the developing SLE, insurance was withdrawal, or
until 31 December 2008, with estimated follow-up person-years. The SLE events
diagnosis was confirmed by the International Classification of Diseased, 9th Revision
of the Clinical Modification (ICD-9-CM), and the Registry for Catastrophic Illness
Patient Database (RCIPD), which includes selected major injuries or illnesses and is
published by the Department of Health, Executive Yuan. To register as SLE, the
diagnosis must be made by board-certified specialist and the application is further
reviewed and approved by the Bureau of NHI, which ensures the accuracy and
reliability of the diagnosis.
Statistical analysis
The sociodemographic variables in this study were sex, age, urbanization, and
parent’s occupation. The urbanization level was categorized by the population density
of the residential area into 4 levels, with level 1 as the most urbanized and level 4 as
(SAS institute Inc., Carey, NC), and the significance level was set at 0.05 in
two-tailed tests. The means and standard deviations (SDs) for continuous variables and
counts and percentages for categorical variables were used to demonstrate the
baseline distributions of the AD and non-AD cohorts. The differences were examined
using the Chi-square test for categorical variables and the t-test for continuous
variables. The Kaplan-Meier method was used to estimate proportions of the studies
subjects who did not suffer from SLE during the follow-up period in both cohorts.
The incidence densities were calculated for each cohort. Hazard ratios (HRs) and 95%
confidence interval (CI) were calculated using multivariable Cox proportional hazard
regression models, with the non-AD comparison cohort as the reference group, to
assess the association between AD and risk of developing a SLE. The Cox model was
also used to estimate the HRs of SLE associated with the annual average of medical
visits by AD, compared to the non-AD cohort. Further analysis was performed to
assess whether the association of SLE varied according to the length of the follow-up
RESULTS
This study evaluated 192,357 AD cases and 769,428 non-AD controls. The
majority of these children were aged ≤ 2 years (64.3%), living in higher urbanization
regions (61.5%) and most white collar of parent occupation (63.2%). The
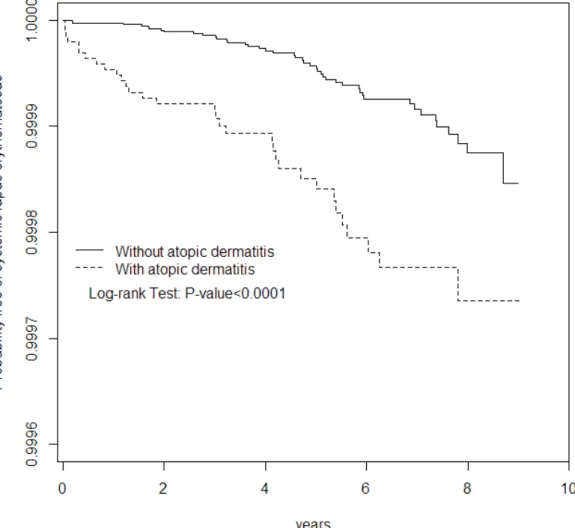
Kaplan-Meier survival analysis showed that the SLE-free rate was lower in the AD cohort
than non-AD cohort (long-rank p<0.0001; Figure 1). Table 2 presents the incidence
densities in the both cohorts and AD/non-AD hazard ratios of SLE by
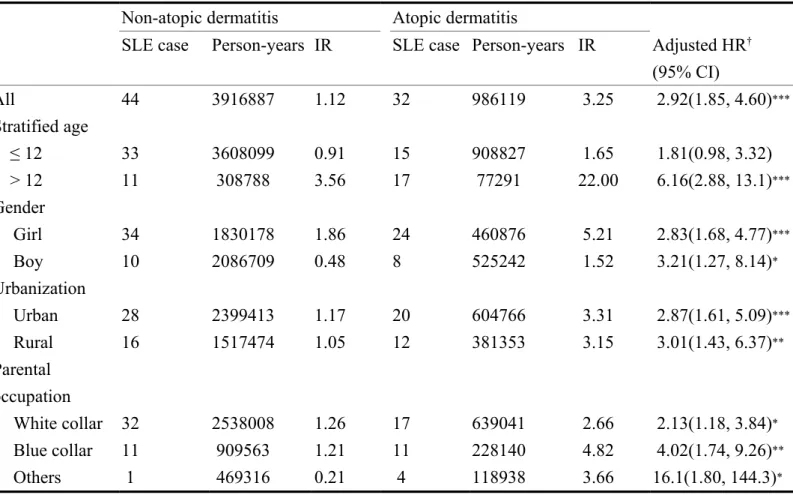
sociodemographic status. Overall, the SLE incidence was 2.92-fold greater in the AD
cohort than in the non-AD cohort (3.25 vs. 1.12 per 100,000 person-years, HR=2.92,
95%CI=1.85-4.60) in the following 9 years. When stratified by age, the incidence
density rates of SLE increase with age. The >12 year-old group had a 6.16-fold
relative risk of developing SLE (95% CI =2.88-13.1) in the AD cohort than in the
non-AD cohort. Generally, the incidence rate of JSLE was greater in girls in both
cohorts. For girls, the incidence density rates are 5.21 and 1.86 per 100,000
person-years in AD and non-AD cohorts, respectively. The gender specific HR for AD cohort
compared to non-AD cohort was approximately 3.0 in both genders. The urbanization
specific HR for AD cohort compared to non-AD cohort was also approximately 3.0
between different degree of urbanization. The incidence of SLE was the highest in the
was the lowest in the non-AD children whose parents are others (0.21 per100,000
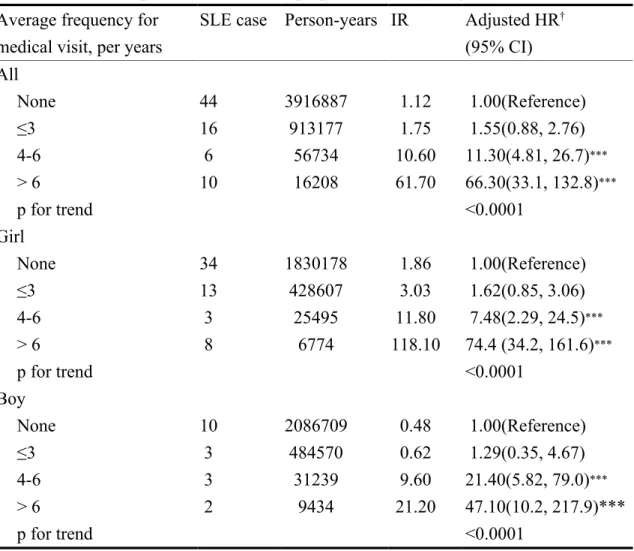
person-years). Compared to the non-AD cohort, the HR increased with the number of
medical visits because of AD, from 1.55 (95% CI =0.88-2.76) for those having 3 or
fewer visits, up to 66.3 (95% CI =33.1-132.8) for those having 6 and more visits (P
for trend < 0 .0001). The risk trend for both genders was similar. The risk of
developing SLE for patients with AD was highest within five year of follow-up after
AD has been diagnosed (HR=4.02, 95%CI=2.83-7.08), followed by follow-up of 5 or
DISCUSSION
By far, this is the first population-based cohort study to investigate the incidence of
JSLE in childhood with AD compared to a non-AD control group. The results show a
significantly increased incidence rate of JSLE in childhood among those with AD
regardless of gender. During the first 5 years after AD diagnosis, the clinic physicians
should pay close attention to the expression of SLE-related biomarkers.
JSLE is rare disease with an estimated annual incidence of 0.36-0.9 per 100,000
children per year, with a significantly higher incidence among non-Caucasian
children, especially Asians, and African Americans.5, 22 The current study revealed an
incidence rate of 1.12 per 100,000 person per year in non-AD Han Chinese children,
which is similar to previous study population. Interestingly, a significantly increased
incidence rate of 3.25 per 100,000 persons per year was observed in AD children. In
addition, the incidence rate further increased in children with AD older than 12 (22
per 100,000 person per year) and those with female gender (5.21 per 100,000 person
per year). More medical visits for AD with increased risk for incidence rate of JSLE
indicated the risk of JSLE increasing with more serious or uncontrolled skin
inflammation of AD.
It is well recognized that the pathogenesis of SLE is from loss of self-tolerance due to
contributors to development or severity of disease are evident but their roles are
poorly understood to date. Only a few studies with limited numbers of patients
investigating the association between allergic diseases and SLE have produced
inconsistent results.6-9 Most of these studies were cross sectional in nature, mainly
focusing on adult patients.6-9 The causality between allergic disease and SLE in
children has not been clearly established. The strength of this study is that it is the
first cohort study to investigate the precise quantification of the incidence of JSLE in
children with AD. Our results, contrary to the Th1/Th2 paradigm, 23-25 revealed
increased incidence rate and risk of JSLE in AD children cohort and the risk further
increased with severity of AD symptoms. Second, the current study is a
population-based study which minimizes the selection bias in other case-control studies. Third,
the diagnosis of AD by physicians other than using questionnaires which minimizes
the selection bias and recall bias. SLE was defined using ICD-9-CM, and RCIPD,
which ensures better diagnosis validity. Fourth, we adjusted the possible confounding
factors, including age, gender, urbanization of residence area, parental occupation,
and baseline year. Ethic influence was not considered to be adjusted because most of
the population in Taiwan is ethnic Chinese.
Elevated total serum IgE has also been described in SLE patients.11-16 Some studies
study, in a mouse model of SLE and in human SLE subjects, reported that the
activation of the basophil by autoreactive IgE-containing immune complexes serves to
amplify the production of autoantibodies and contributes to the pathogenesis of
disease15, 16 The above research advances support our finding of Th2 environment in
contributing to the development of SLE.
There are several limitations to this study that are worth noting. Period of follow-up
was about 10 years, which may not be enough to see the long-term relationship
between AD and SLE. However, the prominent positive effect of AD on JSLE was
still observed. Even though the current study is the largest population to investigate
the incidence of JSLE in an AD cohort, JSLE is a very rare disease and subsequent
risk analysis of more frequently occurring presentations of JSLE, such as lupus
nephritis, thrombocytopenia, encephalopathy and so on cannot be performed due to
insufficient patient numbers. In addition, a number of possible confounding variables,
including body mass index and family history of allergic diseases, which are
associated with allergic diseases were not included in our database. Another limitation
is the lack of data for the study group on genetic and behavioral factors which might
affect the risks JSLE and allergic diseases.
In conclusion, this population-based cohort study revealed a significantly increased
research should look to explore the role of Th2 mediated allergic disease contributing
to the development of Th1 mediated autoimmune disease, and provide a potential
ACKNOWLEDGEMENTS
The study was supported in part by the study projects (DMR-101-061 and DMR-100-076) in our hospital; Taiwan Department of Health Clinical Trial and Research Center and for Excellence (DOH102-TD-B-111-004), Taiwan Department of Health Cancer Research Center for Excellence (DOH102-TD-C-111-005); Bureau of Health
Promotion, Department of Health, R.O.C. (Taiwan) (DOH99-HP-1205); and
International Research-Intensive Centers of Excellence in Taiwan (I-RiCE) (NSC101-2911-I-002-303).
REFERENCES
1. Brunner HI, Gladman DD, Ibanez D, Urowitz MD, Silverman ED. Difference in disease features between childhood-onset and adult-onset systemic lupus erythematosus. Arthritis and Rheumatism 2008; 58:556-62.
2. Tucker LB, Uribe AG, Fernandez M, Vila LM, McGwin G, Apte M, et al. Adolescent onset of lupus results in more aggressive disease and worse outcomes: results of a nested matched case-control study within LUMINA, a multiethnic US cohort (LUMINA LVII). Lupus 2008; 17:314-22.
3. Gardner-Medwin JM, Dolezalova P, CummJSLE C, Southwood TR. Incidence of Henoch-Schonlein purpura, Kawasaki disease, and rare vasculitides in children of different ethnic origJSLE. Lancet 2002; 360:1197-202.
4. Rahman A, Isenberg DA. Systemic lupus erythematosus. N Engl J Med 2008; 358:929-39.
5. Lipsky PE. Systemic lupus erythematosus: an autoimmune disease of B cell hyperactivity. Nat Immunol 2001; 2:764-6.
6. Sequeira JF, Cesic D, Keser G, Bukelica M, Karanagnostis S, Khamashta MA, et al. Allergic disorders in systemic lupus erythematosus. Lupus 1993; 2:187-91.
7. Sekigawa I, Yoshiike T, Iida N, Hashimoto H, Ogawa H. Allergic disorders in systemic lupus erythematosus: prevalence and family history. Lupus 2002; 11:426-9.
8. Cooper GS, Dooley MA, Treadwell EL, St Clair EW, Gilkeson GS. Risk factors for development of systemic lupus erythematosus: allergies, infections, and family history. J Clin Epidemiol 2002; 55:982-9.
9. Sekigawa I, Yoshiike T, Iida N, Hashimoto H, Ogawa H. Allergic diseases in systemic lupus erythematosus: prevalence and immunological considerations. Clin Exp Rheumatol 2003; 21:117-21.
10. Wozniacka A, Sysa-Jedrzejowska A, Robak E, Samochocki Z, Zak-Prelich M. Allergic diseases, drug adverse reactions and total immunoglobulin E levels in lupus erythematosus patients. Mediators Inflamm 2003; 12:95-9.
11. Laurent J, Lagrue G, Sobel A. Increased serum IgE levels in patients with lupus nephritis. Am J Nephrol 1986; 6:413-4.
12. Elkayam O, Tamir R, Pick AI, Wysenbeek A. Serum Ige Concentrations, Disease-Activity, and Atopic Disorders in Systemic Lupus-Erythematosus. Allergy 1995; 50:94-6.
13. Sekigawa I, Tokano Y, Yoshiike T, Iida N, Hashimoto H, Ogawa H. Relationship between serum IgE and autoantibody levels in SLE patients.
Clinical and Experimental Rheumatology 2003; 21:683-.
14. Rebhun J, Quismorio F, Dubois E, Heiner DC. Systemic Lupus-Erythematosus Activity and Ige. Annals of Allergy 1983; 50:34-6.
15. Charles N, Hardwick D, Daugas E, Illei GG, Rivera J. Basophils and the T helper 2 environment can promote the development of lupus nephritis. Nat Med 2010; 16:701-7.
16. Charles N, Rivera J. Basophils and Autoreactive IgE in the Pathogenesis of Systemic Lupus Erythematosus. Current Allergy and AD Reports 2011; 11:378-87.
17. Spergel JM, Paller AS. Atopic dermatitis and the atopic march. J Allergy Clin Immunol 2003; 112: S118-S127.
18. Davis K, Huang AT. Learning from Taiwan: experience with universal health JSLEurance. Ann Intern Med 2008; 148:313-4.
19. Cheng TM. Taiwan’s National Health JSLEurance system: high value for the dollar. In Okma KGHaC, L.ed. Six Countries, Six Reform Models: The Health Reform Experience of Israel, the Netherlands, New Zealand, Singapore, Switzerland and Taiwan. 2009:71-204.
20. Cheng CL, Kao YHY, Lin SJ, Lee CH, Lai ML. Validation of the National Health JSLEurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiology and Drug Safety 2011; 20:236-42.
21. Wei CC, Yu IW, Lin HW, Tsai AC. Occurrence of infection among children with nephrotic syndrome during hospitalizations. Nephrology 2012; 178: 681-688.
22. Levy DM, Peschken CA, Tucker LB, Chedeville G, Huber AM, Pope JE, et al. Influence of ethnicity on childhood-onset systemic lupus erythematosus: results from a multiethnic multicenter Canadian cohort. Arthritis Care Res (Hoboken) 2013; 65:152-60.
23. Bach JF. The effect of infections on susceptibility to autoimmune and allergic diseases. N Engl J Med 2002; 347:911-20.
24. Okada H, Kuhn C, Feillet H, Bach JF. The 'hygiene hypothesis' for
autoimmune and allergic diseases: an update. Clin Exp Immunol 2010; 160:1-9.
25. Romagnani S. The increased prevalence of allergy and the hygiene hypothesis: missing immune deviation, reduced immune suppression, or both?
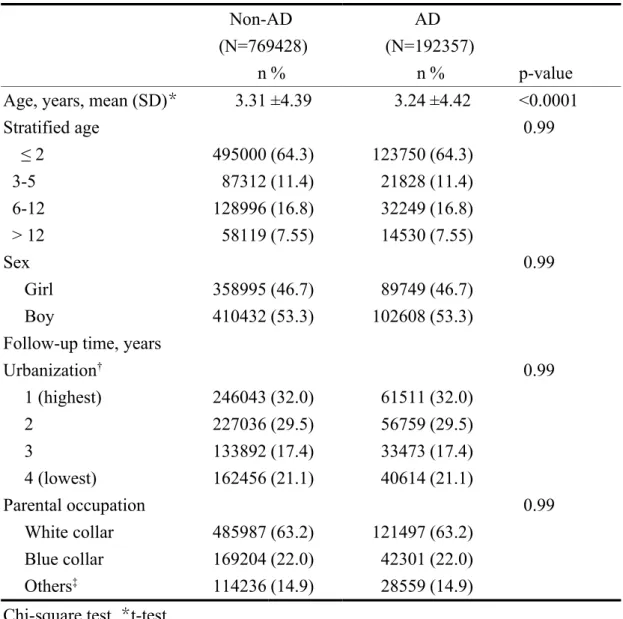
Table 1. Demographics between children with and without atopic dermatitis (AD) Non-AD (N=769428) AD (N=192357) n % n % p-value
Age, years, mean (SD)* 3.31 ±4.39 3.24 ±4.42 <0.0001
Stratified age 0.99 ≤ 2 495000 (64.3) 123750 (64.3) 3-5 87312 (11.4) 21828 (11.4) 6-12 128996 (16.8) 32249 (16.8) > 12 58119 (7.55) 14530 (7.55) Sex 0.99 Girl 358995 (46.7) 89749 (46.7) Boy 410432 (53.3) 102608 (53.3)
Follow-up time, years
Urbanization† 0.99 1 (highest) 246043 (32.0) 61511 (32.0) 2 227036 (29.5) 56759 (29.5) 3 133892 (17.4) 33473 (17.4) 4 (lowest) 162456 (21.1) 40614 (21.1) Parental occupation 0.99 White collar 485987 (63.2) 121497 (63.2) Blue collar 169204 (22.0) 42301 (22.0) Others‡ 114236 (14.9) 28559 (14.9)
Chi-square test, *t-test
‡Other occupations included primarily retired, unemployed, or low income
populations.
†: The urbanization level was categorized by the population density of the residential
area into 4 levels, with level 1 as the most urbanized and level 4 as the least urbanized.
Table 2. The risk of systemic lupus erythematosus compared to children without atopic dermatitis stratified by demographics in Cox proportional hazard regression
Non-atopic dermatitis Atopic dermatitis
SLE case Person-years IR SLE case Person-years IR Adjusted HR†
(95% CI) All 44 3916887 1.12 32 986119 3.25 2.92(1.85, 4.60)*** Stratified age ≤ 12 33 3608099 0.91 15 908827 1.65 1.81(0.98, 3.32) > 12 11 308788 3.56 17 77291 22.00 6.16(2.88, 13.1)*** Gender Girl 34 1830178 1.86 24 460876 5.21 2.83(1.68, 4.77)*** Boy 10 2086709 0.48 8 525242 1.52 3.21(1.27, 8.14)* Urbanization Urban 28 2399413 1.17 20 604766 3.31 2.87(1.61, 5.09)*** Rural 16 1517474 1.05 12 381353 3.15 3.01(1.43, 6.37)** Parental occupation White collar 32 2538008 1.26 17 639041 2.66 2.13(1.18, 3.84)* Blue collar 11 909563 1.21 11 228140 4.82 4.02(1.74, 9.26)** Others 1 469316 0.21 4 118938 3.66 16.1(1.80, 144.3)*
IR, incidence rate, per 100,000 person-years Adjusted HR†, adjusted for age and sex
Table 3. The risk of systemic lupus erythematosus among average frequency for medical visits of atopic dermatitis in Cox proportional hazard regression
Average frequency for medical visit, per years
SLE case Person-years IR Adjusted HR†
(95% CI) All None 44 3916887 1.12 1.00(Reference) ≤3 16 913177 1.75 1.55(0.88, 2.76) 4-6 6 56734 10.60 11.30(4.81, 26.7)*** > 6 10 16208 61.70 66.30(33.1, 132.8)*** p for trend <0.0001 Girl None 34 1830178 1.86 1.00(Reference) ≤3 13 428607 3.03 1.62(0.85, 3.06) 4-6 3 25495 11.80 7.48(2.29, 24.5)*** > 6 8 6774 118.10 74.4 (34.2, 161.6)*** p for trend <0.0001 Boy None 10 2086709 0.48 1.00(Reference) ≤3 3 484570 0.62 1.29(0.35, 4.67) 4-6 3 31239 9.60 21.40(5.82, 79.0)*** > 6 2 9434 21.20 47.10(10.2, 217.9)*** p for trend <0.0001
IR, incidence rate, per 100,000 person-years Adjusted HR†, adjusted for age and sex
Table 4 Trends of systemic lupus erythematosus event risk by stratified follow-up years
Non-atopic dermatitis Atopic dermatitis
Follow time SLE case Person-years IR SLE case Person-years IR Adjusted HR
†
(95% CI) SLE
≤5 years 24 3113134 0.77 24 782734 3.07 4.02(2.83, 7.08)*** >5 years 20 803752 2.49 8 203384 3.93 1.60(0.71, 3.63) IR, incidence rate, per 100,000 person-years
Crude HR, hazard ratio
Adjusted HR†, adjusted for age and sex
* p<0.05, ** p<0.01, *** p<0.001
Figure 1. Probability free systemic lupus erythematosus for patients with atopic dermatitis (dashed line) or without atopic dermatitis (solid line)