Copyright © 2013 Inderscience Enterprises Ltd.
iPCA: an integration information system for patient
controlled analgesia using wireless techniques
Shu-Fen Yang and Tien-Hsiung Ku
Department of Anesthesia,Changhua Christian Hospital, Changhua, Taiwan
Email: [email protected] Email: [email protected]
Andy An-Kai Jeng, Rong-Hong Jan*,
Yu-Chee Tseng, Kuo-Chen Wang and
Yuh-Jyh Hu
Department of Computer Science, National Chiao Tung University, Hsinchu, Taiwan Email: [email protected] Email: [email protected] Email: [email protected] Email: [email protected] Email: [email protected] *Corresponding author
Abstract: Recently, pain management has become an important aspect of medical care. Patient
Controlled Analgesia (PCA) is a particularly effective and flexible treatment that allows patients to adjust the dosages of the analgesics that control their pain after surgery. However, PCA requires manual operation for sustained attention, and should be analysed with other pathology information for synergic usage. In this paper, we propose an integrated information system for pain management, called Integrated Patient Controlled Analgesia (iPCA). The system integrates various PCA-related devices by wireless techniques to provide real-time information for medial staffs, and offer more efficient and convenient pain control for both in-hospital and at-home patients. To evaluate our system, we have developed a prototype and conducted a series of field trails at a large private hospital in southern Taiwan. The results show that the iPCA system indeed works well with patients, and can provide better post-operative pain control by efficiently collecting PCA usage information.
Keywords: wireless sensor networks; network integration; patient controlled analgesia; home
healthcare; data mining.
Reference to this paper should be made as follows: Yang, S-F., Ku, T-H., Jeng, A.A-K., Jan,
R-H., Tseng, Y-C., Wang, K-C. and Hu, Y-J. (2013) ‘iPCA: an integration information system for patient controlled analgesia using wireless techniques’, Int. J. Ad Hoc and Ubiquitous Computing, Vol. 13, No. 1, pp.48–58.
Biographical notes: Shu-Fen Yang received the MD degree from China Medical University,
Taiwan in 1987. She joined the Department of Anesthesia, Changhua Christian Hospital in 1987, where she is currently an attending doctor. Her research interests include postoperative pain control, post-dural puncture headache treatments and painless labour.
Tien-Hsiung Ku is an Anaesthesiologist working at Changhua Christian Hospital, Taiwan since 1987. He got his master degree in Computer Science at Asia University in 2004. His research interests include medical informatics and bioinformatics. He recently finished the first complete genome analysis of bacteria Morganella morganii.
Andy An-Kai Jeng received the BS degree in Statistics from Tamkang University, Taiwan, in 2001, the MS degree in Management Information Systems from National Chi Nan University, Taiwan, in 2003, and PhD degree in Computer Science from National Chiao Tung University, Taiwan, in 2007, where is currently a post-doctoral researcher. His research interests include wireless networks, distributed algorithm design and analysis, scheduling theory, and operations research.
Rong-Hong Jan received the BS and MS degrees in Industrial Engineering, and the PhD degree in Computer Science from National Tsing Hua University, Taiwan, in 1979, 1983, and 1987, respectively. He joined the Department of Computer and Information Science, National Chiao Tung University, in 1987, where he is currently a Professor. During 1991–1992, he was a Visiting Associate Professor in the Department of Computer Science, University of Maryland, College Park, MD. His research interests include wireless networks, mobile computing, distributed systems, network reliability, and operations research.
Yu-Chee Tseng got his PhD in Computer and Information Science from the Ohio State University in January of 1994. He was/is Chairman (2005–2009), Chair Professor (2011– present), and Dean (2011–present), Department of Computer Science, National Chiao Tung University, Taiwan. His research interests include mobile computing, wireless communication, and sensor networks. He is an IEEE Fellow. He serves/served on the editorial boards of IEEE Trans. on Vehicular Technology (2005–2009), IEEE Trans. on Mobile Computing (2006–2011), and IEEE Trans. on Parallel and Distributed Systems (2008–present).
Kuo-Chen Wang received the BS degree in Control Engineering from the National Chiao Tung University, Taiwan, in 1978, and the MS and PhD degrees in Electrical Engineering from the University of Arizona in 1986 and 1991, respectively. He is currently a Professor in the Department of Computer Science, National Chiao Tung University. He was a Visiting Scholar in the Department of Electrical Engineering, University of Washington from July 2001 to February 2002. From 1980 to 1984, he was a Senior Engineer at the Directorate General of Telecommunications in Taiwan. His research interests include wireless (ad hoc/sensor/VANET) networks, mobile/cloud computing, and power management for multimedia portable devices. Yuh-Jyh Hu is currently an Associate Professor in the Department of Computer Science and also the Institute of Biomedical Engineering at National Chiao Tung University in Taiwan. His research interests include bioinformatics, medical informatics and machine learning. He obtained his Master degrees in Computer Science from University of Southern California in 1992, and from University of California, Irvine in 1994. He received the PhD degree from University of Southern California in 1999.
1 Introduction
The advances of information and network technologies have shifted the objectives of many innovations from improving hardware efficiency to providing better services. Medical care is one of the potential applications, which aims to create a safer, healthier and more comfortable environment where provides better treatment for patients and offer instant information or even decision support for health workers. Such as an on-line virtual clinic system developed by Chang et al. (2004), it enables remote diagnosis via video and voice devices; Yang et al. (2006) employed a radio system to trace each patient’s position. Similarly, a variety of remote medical treatment systems were studied by Reske et al. (2002), Fensli et al. (2004), Lin et al. (2004), Lee et al. (2007), Liu (2011) and Kahn et al. (2011). A survey of wireless-sensor-network-based healthcare systems can be found in Huo et al. (2011).
In particular, pain management is a critical segment in modern medical care. Constant pain may both physically and mentally affect our life and make people feel more intolerable than the illness itself, especially for those who have undergone surgeries. Intramuscular (IM) opioid injection is a commonly used treatment for postoperative pain relief (Ballantyne et al., 1993). It takes roughly 10 to 20 minutes to take effect. But different surgeries cause
different degrees of pain and pain endurance varies among people. Without the correct analgesic dosage beforehand, it is hard to meet the patient’s need by this method.
Patient Controlled Analgesia (PCA) is an electronic analgesic delivery system that makes direct and flexible pain treatment by allowing patients to administer their own pain relief (Walder et al., 2001; Dolin et al., 2002). PCA also allows caregivers to regulate the patient’s operation by configuring, such as, the delivery rate, delivery limit, concentration units, bolus volume and loading dose of the device. It has been widely used in hospitals and considered the most effective way for postoperative analgesia, especially for major surgery.
However, there are still several reasons making PCA inconvenient for the users: First, the medical staff has to constantly monitor the patients for at least the first two to twenty four hours so as to ensure PCA devices were properly used (Taber and Venes, 2009). It involves several manual operations, e.g. collecting patient’s PCA data, printing out analgesia usage, entering readings into appropriate databases, and etc. Second, PCA data are usually exploited with pathology information obtained from other devices. For instance, whether the current PCA control requires a readjustment after the initial setting is based on the patient’s physical states (e.g. heartbeat rate, blood pressure, and SpO2) and discomfort symptoms (e.g. vomiting,
dizziness, fever and weakness). Such information should be quickly and correctly collected from the corresponding device as needed. Moreover, it is awkward for medical staffs if they have to frequently add or remove different devices using cable lines. The wired connections also restrict patients from walking freely in wards and hospital.
Recently, pain management also plays a vital role in home healthcare. Home healthcare, as opposed to in-hospital care, is a prevalent tendency that provides healthcare, including medication, for patients at homes as if they remain at hospital. Providing pain management in-home can not only assist the post-hospitalisation recovery process during the initial weeks after discharge but also improve the quality of life for chronic pain patients.
In this paper, we propose an integrated information system for pain management, called Integrated Patient Controlled Analgesia (iPCA). The system integrates various PCA-related devices by wireless techniques to provide real-time information for medial staffs, and offer more efficient and convenient pain control for both in-hospital and at-home patients. We have implemented a prototype and conducted a series of field trails at a large private hospital in southern Taiwan. The results show that our system can significantly reduce the time required for collecting PCA-related information.
The rest of this paper is organised as follows: In Section 2, we overview the architecture and application scenarios of the iPCA system. The major designs of the proposed system are presented in Section 3. In section 4, we detail the implementation information. Section 5 presents the on-site field trials, and the concluding remarks are given in Section 6.
2 System overview
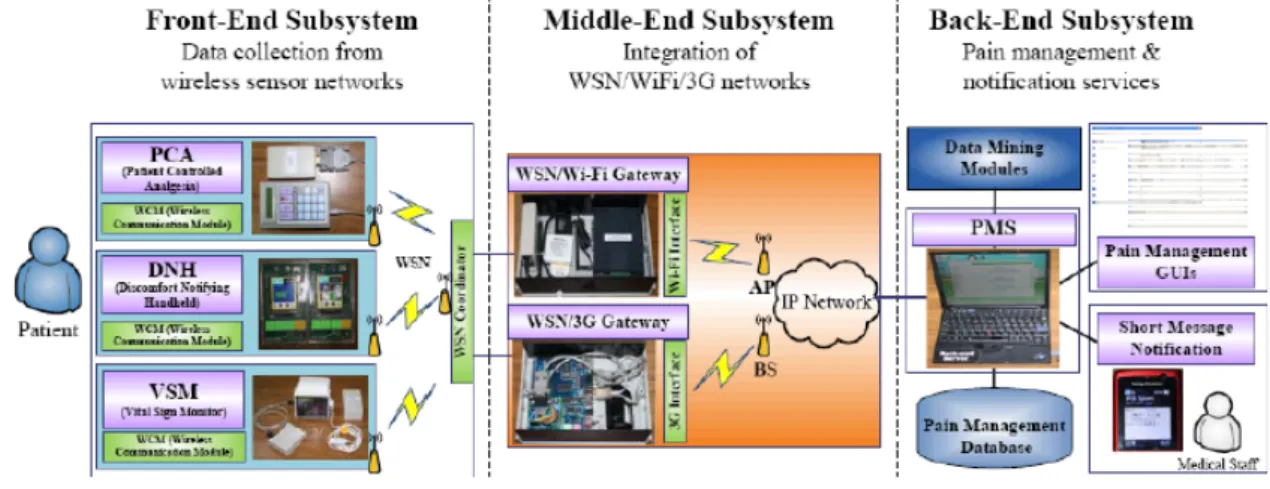
The iPCA system can be divided into the front-end, the middle-end and the back-end subsystems, as shown in Figure 1. The front end is a WSN-based monitoring system that collects health-related data from the patients. The back end provides monitoring, management and notification
services as well as data mining modules of PCA control prediction. The middle end is an information integration network that bridges the front and the back ends.
In order to collect various health-related data from the patients, the front end integrates different medical devices, including PCA, Vital Sign Monitor (VSM), and Discomfort Notifying Handheld (DNH). The VSM is a portable device used to collect the periodic data of SpO2, heartbeat rate and
blood pressure from the patient. The DNH is a handheld device that can help the patient to express his (or her) pain level, e.g. a scale from 1 to 10, or discomfort symptoms, e.g. vomiting, dizziness, fever and weakness, to the doctor or medical staff in a more intuitive way. The iPCA connects the three kinds of medical devices using Zigbee nodes to form a wireless sensor network (WSN). The WSN provides wireless, light-weight and low-power connections (Sheu et al., 2010), which has been widely deployed for many usages, such intrusion detection (Farooqi and Farrukh, 2012). With the features of a WSN, medical staff can easily add or remove a medical device for the patient by associating the attached Zigbee node with a nearby WSN controller. Then, each medical device can transmit the sensing data through its Zigbee node.
Any PCA-related data collected by the WSN controller will be delivered to a back-end server for monitoring and controlling purposes. However, due to the short-range character of WSNs, it is often unable to transmit data directly to the back end server that could be far away from the ward (usually installed at the information centre of the hospital). Thus, we developed a WSN/Wi-Fi wireless gateway that bridges the WSN and IEEE 802.11 Wi-Fi networks. The gateway is connected with a (or multiple) WSN coordinator(s) and, on the other side, associated with a Wi-Fi access point (AP). The collected data will be forwarded through a Wi-Fi connection over the backbone IP network. As shown in Figure 2(a), with a pack that carries PCA and related devices, the in-hospital patient was no longer restricted by the wired connection allowing walking freely in the ward.
Figure 2 The front-end scenarios: (a) In-hospital Scenario,
(b) and (c) In-home Scenarios (see online version for colours)
(a) (b) (c)
On the other hand, for patients who need medical care in-home, we developed a WSN/3G wireless gateway, also called home gateway, to bridge the wireless sensor and 3G networks. The 3G transmitter has much larger coverage than the Wi-Fi transmitter. Similarly, the wireless gateway collects the sensing data from medical devices via a WSN coordinator placed in the patient’s house and associates with a 3G base station (BS). Any sensing data can be transmitted to the remote information centre of the hospital via the home gateway. As shown in Figure 2(b) and (c), chronic patients are now capable of controlling their pain in-home, making the quality of life better.
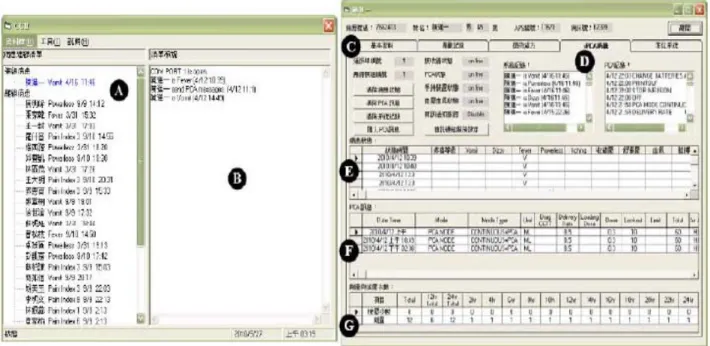
At the back end, we set up a Pain Management Server (PMS). The PMS was connected with the WSN/Wi-Fi and WSN/3G gateways to collect data from both in-hospital and in-home patients at the front end. All received data were decoded, parsed and stored into the Pain Management Database (PMD). We developed a set of user-friendly management interfaces on PMS.
Two snapshots are given in Figure 3. Area A provides a list of on-line and off-line lists patients registered in the iPAC system. For each patient, the staff can monitor the connection statues in Area B, conditions of devices in Area C and PCA usages in Areas D and F. The VSM and DNH records were merged in Area E, and the PCA pressing counts per 2 hours were listed in Area G.
On the other hand, for patients who need an instant aid, e.g. irregular heart rate, the iPCA provides a real-time notification service. The service integrates the PMS with the 3G Short Message Service (SMS) (Peersman et al., 2000). As shown Figure 4, when a patient feels uncomfortable, he (or she) can choose one of the buttons on the DNH to triggers a notification to the PMS. The PMS then execute a SMS AT-command set that pushes a SMS message into a 3G transmitter and sends it to the mobile phones of the staffs. The message includes, for instance, the current status of the patient, emergency level and doctor’s phone number. Finally, the staff can be aware of the patient’s status by reading the SMS on the screen.
Lastly, the data stored in PMD can be used for mining meaningful information for advanced patient care. As our recent study (Hu et al., 2010), we proposed applying data mining algorithms to predict the anaesthetic dose totally taken in 24 hours, and to decide whether PCA controls requires readjustment after the initial setting based on the patient’s physical states, e.g. heart rate, and the early-stage PCA usage, e.g. frequency of PCA demands for the first 6 hours. An accurate predictor could predict the amount of the analgesics injected at different periods of time and provide an early warning for anaesthesiologists to make necessary adjustments of PCA control.
Figure 4 Pain notification service (see online version for colours)
3 System designs
In this section, we present the design of major parts in our system. The implementation of each device is detailed in the next section.
3.1 WSN management protocol
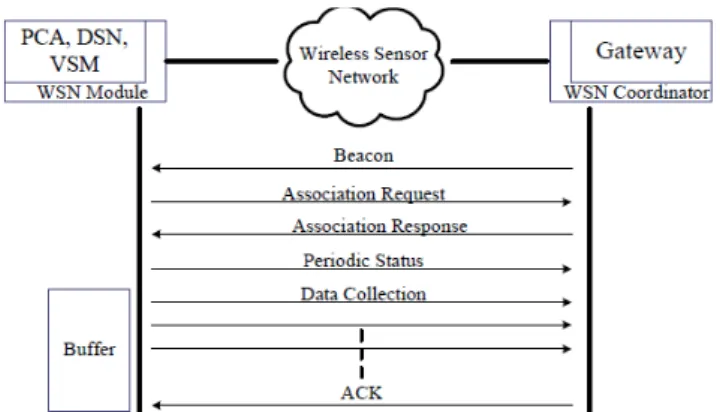
In order to collect data from patients, we propose a WSN management protocol. The protocol coordinates between each WSN module (i.e. Zigbee node) attached on a device and the WSN coordinator. As shown in Figure 5, the WSN coordinator periodically broadcasts a beacon to announce the gateway’ information. When a WSN module received the beacon, it sends a request to be associated with the WSN coordinator. Next, the WSN coordinator replies with an association response to assign the WSN module a short address. Then, the WSN module will periodically send the statuses gathered from the device it is connected with. Besides, the WSN module will send a data collection message if any operation of the device is triggered by the patient or medical staff. In either way, the WSN coordinator will forward the received message to the PMS.
Figure 5 WSN coordination with buffer-ACK mechanism
The above process can work well if no data loss occurs. However, in our practical deployment on site (as introduced in Section 5), we found that the data transmitted from devices in the wards suffered serious loss due to the obstacles in the hospital (e.g. doors, distance, and the limitations of deployment), especially when the size of the
data was large (e.g. the PCA data is about 3k~17k bytes). So, we incorporated a Buffer-ACK mechanism into the protocol to ensure the integrity of the collected data. As shown in Figure 5, the WSN module will buffer any data in its memory when it transmits data collection messages to the WSN coordinator. Besides, the WSN module counts the number of messages it has transmitted and appends this variable to the last message. When the last message is transmitted, the WSN module starts a timer to begin the retransmission procedure. Then, the WSN coordinator checks the variable appended in the last message with the number of messages it has received. If it is equal, the WSN coordinator will send back an ACK message to stop the retransmission procedure of the WSN module; otherwise, the WSN module will retransmit the data after the timeout period. In this way, the data transmission is more reliable.
On the other hand, if the PMS cannot receive data from a registered device over a period of time, e.g. 10 seconds, the management interface will show an “off-line” status for the derive, as shown in Area C of Figure 3. So, the staff can be aware of the disconnection event and do some thoroughgoing process, e.g. remove obstacles or relocate the WSN coordinator, immediately.
The format of the message sent from the WSN module is shown in Figure 6 (a); “Type” specifies whether a periodic status or data collection message. “Device” identifies to which medical device the message belongs (e.g. PCA, DNH, and VSM). “ID” is the unique identity for the patient in this system. ”Data” is the medical information generated by the device. The format of the status report sent from the WSN coordinator is shown in Figure 6 (b); its format is the same as that of the message mentioned above except for the data field which is replaced by the status of each device in order to indicate the on/off line status of the device. The field P, D or V represents whether the status is for the PCA, DNH or VSM device.
Figure 6 Message formats of management protocol
To protect patient privacy, we also apply a Character-based Cipher Chain Block Encryption in our protocol. The algorithm takes each character of the plaintext as a block for encryption. Every block does XOR with a sequence number and a secret key. The result of the first block then does XOR with an initialisation value (IV) to generate a ciphertext. Any result of the subsequent block does XOR with the ciphertext of the previous block. In this way, we can obtain a different ciphertext even if the same plaintext appears several times.
3.2 Network integration
The PMS connects to the wireless gateway for remotely accessing, monitoring, and controlling the PCA-related devices in the WSN network. On the other hand, any data
collected by the WSN coordinator will be forwarded to the PMS through the wireless gateway. The middle-end subsystem is responsible for integrating heterogeneous networking in the iPCA system.
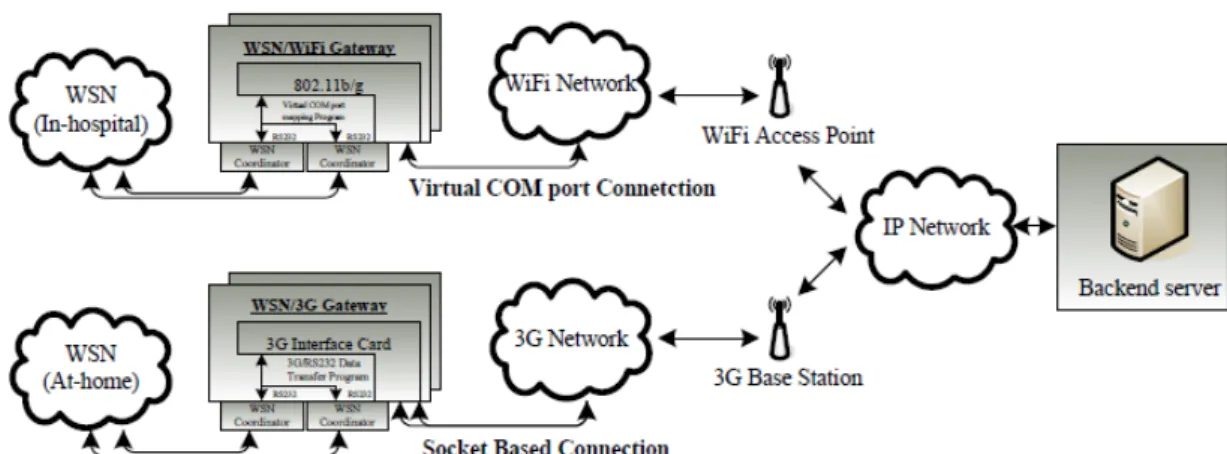
As shown in Figure 7, we integrate the WSN, Wi-Fi and 3G networks using the two types of wireless gateways: WSN/Wi-Fi and WSN/3G wireless gateways, respectively, for in-hospital and at-home scenarios. Both types of gateways can be connected with two or more WSN coordinators to disperse the loading from the WSN modules via the RS232 ports via the RS-232 serial port.
In the WSN/Wi-Fi gateway, we use the virtual COM port technique to enable any serial device (i.e. WSN coordinator) to be remotely accessed, controlled, monitored, and shared on the 802.11b/g wireless network. More precisely, it provides a serial COM port redirector that creates a virtual COM port on the remote machine (e.g. the PMS) for any serial device connected to the wireless gateway (e.g. WSN coordinator). Each virtual COM port works like a standard serial COM port. The remote machine can see no difference between a local serial device and one which connects to the serial port of the wireless gateway.
When receiving a serial operation call from the remote machine, the corresponding serial data will be encapsulated and transmitted using the wireless interface. In other words, the technique allows virtual serial links over an IP (TCP/IP, UDP/IP) network. Thus, the PMS can just read and write the virtual COM port to communicate with the WSN coordinator. Moreover, serial operation calls are transparent to the remote machine, guaranteeing compatibility with legacy serial devices and enabling backward compatibility with existing software.
For the WSN/3G gateway, we design a socket-based program that will establish an RS232/3G tunnel between the PMS and each WSN coordinator. To improve the reliability, if any data was received before the construction of the socket connection, the wireless gateway will buffer the data in its memory and send the buffered data when the socket to the PMS is successfully constructed.
Besides, any data being sent is recorded in a log file. If the connection to the PMS is corrupted, the data will be retransmitted when the connection is reconstructed.
3.3 PCA control predictor
In this part, we briefly introduce the PCA control predictors, as a part of the iPCA system developed in our recent study (Hu et al., 2010). Prediction methods can be evaluated according to accuracy and comprehensibility. The accuracy of a predictor refers to its ability to correctly predict the value of the target attribute, e.g. total anaesthetic dose, for previously unseen data; the comprehensibility of a predictor refers to the level of ease with which humans can interpret the predictions. However, for any prediction method available, there exist some tradeoffs between these two criteria due to inductive bias (Mitchell, 1982). It is often difficult or even unlikely to find one that can make the most accurate, and in the meantime, the most comprehensible predictions. So, we must examine the application domain of the predictor, and realise what information the users expect the predictor to deliver.
To maintain sufficient comprehensibility, the proposed predictors are based on an ensemble of decision trees to develop. Decision tree learning is among the most widely used and practical methods for inductive inference. It approximates the function for the target attribute by learning a decision tree from the examples. An ensemble of decision trees are often more accurate than any single tree in the ensemble (Bauer and Kohavi, 1999). In order to deal with the noise in medical data, the decision trees are created based on the Bagging (Freund and Schapire, 1996). Bagging is popular method for generating multiple versions of a predictor and combining them to form an aggregated predictor. It is prone to avoid over fitting the training data in the presence of noise.
The idea of Bagging can be illustrated by an intuitive example. Suppose that a patient wants a diagnosis made based on the symptoms. He (or she) would rather choose to consult with several than ask only one doctor. The most frequent diagnosis is more likely the correct diagnosis because intuitively, a majority vote made by a large group of doctors may be more reliable. If we substitute one version of a predictor for each doctor, we get the Bagging predictor. The detailed design of the proposed predictor can be found in Hu et al. (2010).
Figure 7 Integration of the WSN, Wi-Fi and 3G networks (see online version for colours)
4 Implementations
In this section, we present the implementations of the WSN module, connection to each medical device and the two wireless gateways.
4.1 WSN module
We used the Jennic-HSCC WSN module designed by the NCTU High-Speed Communication & Computing Lab. The Jennic-HSCC is based on the Jennic JN-5139 (http://www.jennic.com/) which is a power and low-price wireless chip that integrates with a 32-bit RISC microprocessor and is completely compatible with the 2.4GHz IEEE 802.15.4 specification. The Jennic-HSCC WSN module is also equipped with a 192k ROM and 8k~96 KB RAM (according to the chip type) and is able to be integrated with other digital and analogue peripheral hardware.
In order to connect PCA-related devices (including PCA, VSM, and DNH) with the WSN module, we have integrated the Jennic JN-5139 chip with a standard RS-232 serial port. As shown in Figure 8, the JN-5139 chip can send and receive sensing data from the device through the serial port. The Jennic-HSCC also provides the Jennic environment system and SDK so that we can easily program our WSN management protocol (introduced later) on the chip.
Figure 8 WSN module – Jennic-HSCC (see online version
for colours)
4.2 WSN connections and medical devices
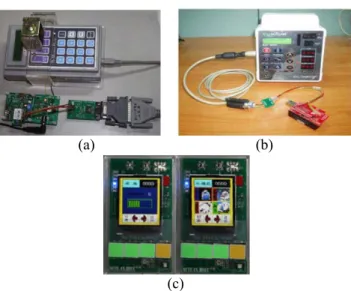
Then, we connect the WSN module with each medical device at the front-end subsystem, including the PCA, VSM and DNH devices, via a standard serial port. The PCA device manufactured by Abbott (http://www.abbott.com/) was connected with the Jennic HSCC through an RS-232 serial port. The Abbott PCA is an ambulatory pump designed to deliver analgesic to patients in hospitals, outpatient treatment centres, or at home. Delivery mode, concentration units (mg, lg or ml), delivery rate, bolus operation, bolus volume, 4-hour delivery limit and loading dose can all be programmed. As presented in Figure 9 (a), installed above the PCA device was the solenoid valve that pressed the “Print” button on the PCA when triggered by the
pain management applications. It transmitted the analgesic usage data to the WSN module. Likewise, we connected the vital sign monitor of Criticare (http://www.csiusa.com/) with a WSN module by a RS-232 serial port as shown in Figure 9(b). It periodically collected the data of Sp02, heart rate and blood pressure from the patient. Lastly, we implemented the DNH on an ATmega-128-CPU-based board (http://www.atmel.com/), see Figure 9(c). The DNH device consists of four buttons and an LCD displayer in two modes: the pain scale mode (right-hand side) and the discomfort symptom mode (left-hand side). In the former, a patient can select a scale between 1 and 10 according to the pain level. In the latter, the patient can acknowledge different symptoms, including vomiting, dizziness, fever and weakness. In either mode, a message will be sent to the WSN module via the serial port. Any data collected from these devices will be passed to the WSN module through an RS-232 serial port, and in turn, forwarded to the PMS through the wireless gateway. Note that although VSM is much heavy (1~2 kilograms depending on its type), with the WSN module, it can be easily added to or removed from a patient, making the deployment process easier
Figure 9 Connection of (a) PCA, (b) VSM, and (c) DNH with
the WSN module (see online version for colours)
(a) (b)
(c)
4.3 WSN/Wi-Fi and WSN/3G gateways
As shown in Figure 10(a), we connect the WSN coordinator (right-hand side) with the Advantech Eki-1352 wireless gateway (http://www.kaise.com.tw/, left-hand side) via the virtual COM port by a serial link. The Advantech Eki-1352 is then associated with an access point through the 802.11b/g interface and starts a virtual COM port mapping program to connect the WSN coordinator with the PMS over the IP network.
We implemented the WSN/3G gateway on the Kaise KS_2410 development board (http://www.kaise.com.tw/). As shown in Figure 10(b), the Kaise KS_2410 is a Linux-based embedded system providing USB and RS-232 ports (left-hand side). To access the internet, we connect the board with a 3G access module (right-hand side) through the USB port.
Figure 10 Wireless gateways: (a) WSN/Wi-Fi (b) WSN/3G
(see online version for colours)
(a) (b)
Then, we use the embedded Linux system with the ARM-Linux kernel version above 2.4 to bridge the WSN and 3G network. The bridging procedure consists of two parts. First, it mounts the USB-based 3G network module on the embedded development board via a shell program that consists of the USB library (libusb), USB mode switch (usb_modeswitch), and internet point to point protocol (PPP) source codes. When the 3G network module is successfully mounted, the gateway uses AT-command sets to communicate with the 3G access module, and dials up the 3G network through the PPP protocol to connect the internet. The second part is a socket-based client program that can forward data from the WSN coordinator (i.e. RS-232 serial port) to the PMS through the 3G network. When getting started, the program actively constructs a tunnel (i.e. a socket connection) to the PMS and waits for the data from the WSN coordinator. When receiving data, the signal is converted into the 3G network and transmitted using the 3G interface.
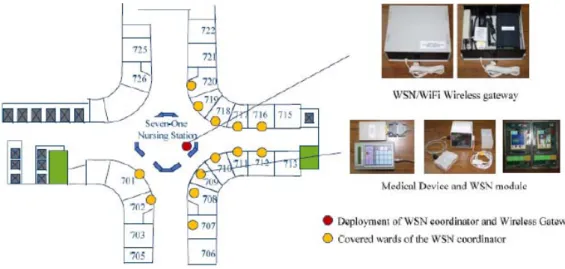
5 Field trials
We have conducted a series of field trials at the Changhua Christian Hospital (CCH) in Taiwan to verify the iPCA system. As shown in Figure 11, our prototype was set up on the 7th floor of CCH. We connected the WSN modules with medical devices in wards 702, 709, 716, and 717. The WSN/Wi-Fi gateway was placed at the nursing station to coordinate the WSN modules in the four wards. The gateway was associated with an access point in the WLAN
infrastructure, called E-care built by CCH, to access IP network. Note that for safety reasons the hospital has strict restrictions on the power usage and electromagnetic disturbance from extra electronic equipment, especially in the wards. Thus, the gateway, including the WSN coordinator, should be kept away from the wards. The PMS was installed in the Department of Anaesthesiology on the 3rd floor and is connected to IP network to receive and analyse data from the gateway. All data were collected from postoperative patients who needed analgesic care to control their pain after surgery.
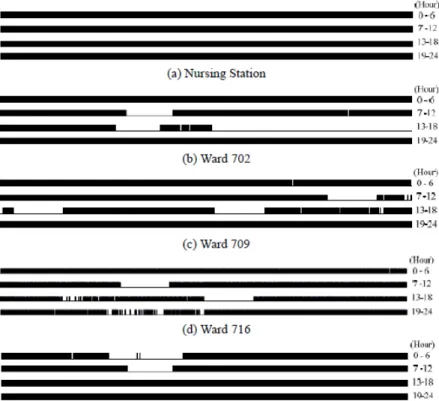
First, we turned on each device for 24 hours and recorded the on-line/off-line status detected by the PMS every 1 minute. Figure 12 shows the connection time of the WSN coordinator at the nursing station and the WSN module of the PCA device in each ward. A black segment represents that the device was connected during the period of time. We can see that the WSN coordinator is constantly on-line. This means that the Wi-Fi connection between the gateway and the PMS is stable. On the contrary, the WSN modules are frequently off-line or even disconnected for certain periods of time, and some data sent from the PCA devices were lost during the unstable intervals. This is because of the fact that many obstacles (e.g. doors, walls, and trolleys) were between the wards and the nursing station. Besides, the signals from the WSN modules may interfere with each other if two or more PCA devices transmit data at the same time.
Table 1 presents the reception ratio and the maximum disconnection time, summarised from the results shown in Figure 12. We can observe that the unstable status gets worse for those wards farther from the nursing station (e.g. wards 702 and 716), because the distance between the WSN module and WSN coordinator may further deteriorate the quality (i.e. signal-to-noise ratio, SINR) of the received signals. Besides, the farther the distance between the ward and the nursing station implies more obstacles existing between them. Thus, the Buffer-ACK mechanism in Section 3.1 is necessary for retransmitting lost data. With this mechanism, the PCA device can transmit data to the coordinator in a reliable way.
Figure 12 Connection time of the WSN coordinator and WSN modules
Table 1 Reception ratio and maximum disconnect time in different wards
WARD 702 709 716 717
RECEPTION RATIO 76.9% 77.9% 79.6% 86.3%
MAX DISCONNECT TIME (MIN) 174.6 43.8 43.8 38.2
In Figure 13, we compare the average time required to collect the PCA and vital sign data from patients using the traditional printer, personal computer and iPCA system. In the traditional way, if a medical staff needs the PCA data, he or she needs to bring the PCA device to a printer to print out the log file. That takes much time and wastes paper resources; otherwise, the staff member must manually connect the PCA device to a PC and use some software to collect the log file via the line print terminal port. It still wastes much time. By using the iPCA system, we can just press the “Print” button on the PCA device. Then, the PCA data will be immediately transmitted, parsed, and stored into the database in the PMS. Thus, the system provides a more
efficientwaytocollectthePCAdata.AsshowninFigure13(a), the iPCA system needs less than 20 seconds to collect the PCA data. In contrast, it takes over 10 minutes before the data is collected in the traditional ways.
On the other hand, if doctors need a patient’s vital signs (SpO2, heart rate and blood pressure), traditionally, they
must wait until nurses have finished recorded daily room check and mutually typed results into the PC. This procedure obviously wastes much time. To improve it, we have also developed a PDA-based method to record the information. In this way, a nurse just needs to record the information in the PDA. The data will be transmitted to the PMS via the 3G network. Although the PDA-based method requires less time for sending data, the data collection can still only be done during the daily room check. In contrast, the iPCA system can automatically collect and transmit the vital sign data to the PMS via the WSN network. As shown in Figure 13(b), vital sign data collection is more efficient when using the iPCA system.
On the other hand, with the assistance of Acute Pain Service at CCH, we have retrospectively collected a significant number of patient records from 2005 to 2008 to evaluate our PCA control predictors in Hu et al. (2010). We predicted the total anaesthetic dose taken in later hours, and decide if any PCA control, e.g. lockout time or PCA dosage, should be readjusted. The results show that the Bagging method with majority voting achieves almost 80% and 70% of accuracy, respectively, for the two prediction tasks. The outcomes also identify the important attributes that most affected the prediction results according to the frequencies of the attributes (i.e. attributes at the top 5 levels in the Bagging trees), e.g. continuous dose in 3rd hr, dose setting in 6th hr, successful demands in 5th hr and etc. We also noticed that the delivery of analgesics by PCA on the patient’s demands seemed like a stronger factor that could have affected the total anaesthetic dose, and the continuous doses were always selected as the root in the decision trees. Besides, the results indicate that whether the patient is diabetic could be a significant factor in the need for later PCA control readjustment. Readers can refer to Hu et al. (2010) for detail results.
6 Conclusion
In this paper, we have proposed an integrated pain control system (iPCA) that integrates various pain control devices using the wireless sensor, Wi-Fi, and 3G networks, which to provide real-time information for medial staffs, and offer more efficient and convenient pain control for both in-hospital and at-home patients. We have also developed tree-learning based predictors to predict the total anaesthetic does and to make the readjustment decision. Through a series of field trials in CCH, we have examined that our iPCA system can work well with patients and significantly reduce the collection time of PCA data.
In the future research, we plan to extend the work in the following directions. First, we will integrate other medical instruments with iPCA to collect a wider variety of vital health signs, and use them as additional descriptive attributes that can provide the medical staff with more accurate predictions. Second, we will incorporate authentication and encryption into iPCA to address the issues of privacy and security. With the architecture of the integrated system proposed in this paper, we hope not only to improve its performance and expand its applicability, but also to link the research on sensor networks with real-world applications.
Acknowledgements
The authors would like to thank Chia-Wei Tao and Tzu-Lin Chang for their helpful assistance in component design and experiment conduction. This research was supported in part by the National Science Council, Taiwan, ROC, under grants NSC99-2218-E-009-002 and NSC 100-2811-E-009-006.
References
Ballantyne, J-C., Carr, D-B. and Chalmers, T-C. (1993) ‘Postoperative patient-controlled analgesia: meta-analyses of initial randomized control trials’, Journal of Clinical Anesthesia, Vol. 5, No. 3, pp.182–193.
Bauer, E. and Kohavi, R. (1999) ‘An empirical comparison of voting classification algorithms: bagging, boosting, and variants’, Machine Learning, Vol. 36, pp.105–139.
Chang, T-C., Lee, J-D. and Wu, S-J. (2004) ‘The telemedicine and teleconsultation system application in clinical medicine’, Proceedings of the 26th Annual International Conference of the Engineering in Medicine and Biology Society, pp.3392–3395. Dolin, S-J., Cashman, J-N. and Bland, J-M. (2002) ‘Effectiveness of
acute postoperative pain management: evidence from published data’, British Journal of Anaesthesia, Vol. 89, No. 3, pp.409–423. Farooqi, A-H. and Farrukh, A-K. (2012) ‘A survey of intrusion
detection systems for wireless sensor networks’, International Journal of Ad Hoc and Ubiquitous Computing, Vol. 9, No.2, pp.69–83.
Fensli, R., Gunnarson, E. and Hejlesen, O. (2004) ‘A wireless ECG system for continuous event recording and communication to a clinical alarm station’, Proceedings of the 26th Annual International Conference of the Engineering in Medicine and Biology Society, pp.2208–2211.
Freund, Y. and Schapire, R. (1996) ‘Experiments with a new boosting algorithm’, Proceedings of the 13th International Conference on Machine Learning, pp.148–156.
Hu, Y-J., Jan, R-H., Wang, K., Tseng, Y-C., Ku, T-H., Yang, S-F. and Wu, H-S. (2010) ‘An application of sensor networks with data mining to patient controlled analgesia’, Proceedings of the 12th IEEE International Conference on e-Health Networking Applications and Services, pp.353–360.
Huo, H., Zhang, Y., Zhang, H., Chuang, Y-H. and Wu, T.C. (2011) ‘Wireless-sensor-networks-based healthcare system: a survey on the view of communication paradigms’, International Journal of Ad Hoc and Ubiquitous Computing, Vol. 8, No.3 pp.135–154. Kahn, C., Buono, C., Chan, T., Blair, P., Griswold, W., Johansson,
P., Chipara, O. and Plymoth, A-N. (2011) ‘Secure scalable disaster electronic medical record and tracking system’, Proceedings of the IEEE International Conference on Technologies for Homeland Security, pp.402–406.
Lee, Y-L., Wu, J-L., Wu, H-S., Yan, S-F., Hsu, S-C., Tsai, C-C. and Ku, T-H. (2007) ‘The use of portable computer for information acquirement during anesthesiologist’s ward round in acute pain service’, Acta Anaesthesiologica Taiwanica, Vol. 45, No. 2, pp.79–87.
Lin, Y-H., Jan, I-C., Ko, P-C-I., Chen, Y-Y., Wong, J-M. and Jan, G-J. (2004) ‘A wireless PDA-based physiological monitoring system for patient transport’, IEEE Transactions on Information Technology in Biomedicine, Vol. 8, No. 4, pp.439–448.
Liu, W. (2011) ‘Research on construction of smart medical system based on the social security card’, Proceedings of the International Conference on Electronic and Mechanical Engineering and Information Technology, Vol. 9, pp.4698–4790. Mitchell, T. (1982) ‘Generalization as search’, Artificial
Intelligence, Vol. 18, pp.203–226.
Peersman, G., Griffiths, P., Spear, H., Cvetkovic, S., Smythe, C. (2000) ‘A tutorial overview of the short message service within 3G’, Computing and Control Engineering Journal, Vol. 11, No. 2, pp.79–89.
Reske, D. and Moussavi, Z. (2002) ‘Design of a web-based remote heart monitor system’, Proceeding of the Biomedical Engineering Society BMES Conference, pp.1847–1848.
Walder, B., Schafer, M. and Henzi, H. (2001) ‘Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain’, Acta Anaesthesiol Scand, Vol. 45, No. 7, pp.795–804.
Yang, X., Shen, X., Sun B-O. and Cai, L. (2006) ‘Security and privacy in RFID and applications in telemedicine’, IEEE Communications Magazine, Vol. 44, No. 4, pp.64–73. Taber, C.W. and Venes, D. (2009) Taber’s Cyclopedic Medical
Dictionary, F.A. Davis Co., pp.108–109.
Sheu, J-P., Chang, C-C. and Yang W-S. (2010) ‘A distributed wireless sensor network testbed with energy consumption estimation’, International Journal of Ad Hoc and Ubiquitous Computing, Vol. 6, No. 2, pp.63–74.
Websites
Abbott Laboratories. Available online at: http://www.abbott.com/ Advantech Co., Ltd. Available online at: http://www.advantech.
com/
Atmel Co. Available online at: http://www.atmel.com/
Criticare Systems Inc. Available online at: http://www.csiusa.com/ Jennic Wireless Microcontrollers, Available online at: http://www.
jennic.com/
Kaise electronic technology. Available online at: http://www.kaise. com.tw/