腺相關病毒傳送第一介白質接受器拮抗蛋白基因應用於預防眼外肌炎; Prevention of Extraocular Myositis by Recombinant Adeno-asssociated Virus Vector With Delivary Of Interleukin-1 Receptor Antagonist
52
0
0
全文
(2) 摘 要 背景:甲狀腺眼疾及不明原因性眼肌發炎疾病的病人詳細機制尚不清楚,並 無完全有效的治療方法及好的預防方法。隨著分子生物學及細胞生物學的進 步,我們瞭解到人類細胞所分泌出第一介白質接受器拮抗蛋白 ( Interleukin-1 receptor antagonist protein) 是極有效力的抗發炎抑 制劑,重組的腺相關病毒(recombinant AAV)是將病毒本身約 96%的 DNA 序列皆移除,如此一來可防止病毒基因產生的病毒蛋白而誘發宿主強烈的免 疫反應。在我們的實驗中我們嚐試以腺相關病毒載體系統 (adeno-associated virus vector system)以基因傳送的方式,期使治療性 基因能被有效植入組織中而且能長期自然產生治療性的物質。. 目的:研究以腺相關病毒載體系統(adeno-associated virus vector system) 傳送第一介白質接受器拮抗蛋白基因,對預防 Phobol Ester 引發白兔眼外 肌炎動物模式組的預防效果。. 方法:實驗組為在左眼外上直肌注射 rAAV-IL-1Ra 劑量為 20 μl;對照組 於右眼外上直肌注射表現 Escherichia coli LacZ 的 AAV (rAAV-LacZ)。三星 期後,注射致炎物質 Porbol ester 0.1mg/mL 0.01ml 於上直肌以引發白兔 眼外肌炎動物模式。之後三星期後,以免疫化學染色及西方點默法確定第一 介白質接受器拮抗蛋白的產生,預防發炎的成效評估以測量肌肉張力及檢查 II.
(3) 病理組織切片之發炎細胞數來評估。. 結果:經由免疫化學染色及西方點默法確定第一介白質接受器拮抗蛋白的產 生。以肌肉內注射phobol ester誘發眼肌炎後7天,進行由病理組織切片之 發炎細胞數評估,發現注射rAAV- LacZ組有較多的發炎細胞,而注射rAAVIL-1Ra組發炎細胞較少(p<0.01)。肌肉張力測量發現於phobol ester誘發眼 肌炎後7天於注射rAAV- LacZ組增加150.4%;於注射rAAV- IL-1Ra組增加 69.4% (p<0.01)。此結果顯示先注射rAAV- IL-1Ra組較注射rAAV- LacZ組有 預防眼肌發炎的情形。 結論:以結合高效率又穩定的腺相關病毒載體系及有抗發炎效果的第一介白 質接受器拮抗蛋白提供一個有價值的預防眼外肌炎的方法。. 關鍵字:眼肌炎、第一介白質接受器拮抗蛋白﹑腺相關病毒﹑基因治療. III.
(4) Abstract Purpose: To evaluate the recombinant adeno-associated virus vector encoding interleukin-1 receptor antagonist (rAAV–IL-1Ra) complementary DNA for its potential in the prevention of phorbol ester–induced extraocular myositis.. Methods: Gene delivery to superior recturs muscle was achieved through intramuscular injections of rAAV-IL-1 Ra in the left eyes and AAV expressing Escherichia coli LacZ (rAAV-LacZ) in the right eyes of white rabbit. After 3 weeks, phorbol ester was used to induce myositis, and the severity of myositis was evaluated. The synthesis and accumulation of IL-1Ra within the muscle were determined using immunohistochemistry and western blot analysis three weeks after gene delivery. The preventive effects of IL-1Ra were evaluated by strain measurement, histologic changes of muscle and inflammatory cell counts one week after myositis induction.. Results: Gene expression of IL-1 Ra was demonstrated through immunohistochemistry and Western blot analysis. Histology revealed more inflammatory cells were retained in the rAAV- LacZ treated muscles (2594.386±319.933 cells/mm2; n=10) than in the rAAV- IL-1 Ra treated. IV.
(5) muscles (1369.479±228.509 cells/mm2; n=10). Strain measurement increased 150.4% 1 week after injection of phorbol ester in right eye, and increased 69.4% in the left eye with previous rAAV–IL-1Ra injection (p<0.01). The myositis in rAAV- IL-1 Ra treated muscles was less severe than that in the rAAV- LacZ treated muscles. Conclusion: This gene therapy, by combining highly efficient and stable rAAV gene delivery, and the anti-inflammatory effect of IL-1Ra, provides a valuable approach for prevention of extraoculor myositis.. Key words: recombinant adeno-asssociated Virus; interleukin-1 receptor antagonist; rabbit; myositis; phorbol ester. V.
(6) Tables of Contents Chapter 1 Introduction Session I Background. 1. Session II Purpose. 1. Session III Research Objectives. 2. Chapter 2 Literature review. 3. Session I Introduction of thyroid eye disesase. 3. Session II Introduction of idiopathic extraocular myositis. 10. Session III Interleukin-I Receptor Antagonist. 15. Session IV Recombinant Adeno-asssociated Virus Vector. 17. Chapter 3 Research Methods. 20. Session 1 Research Materials and Methods. 20. Session 2 Analytic Methods. 23. Chapter 4 Results. 24. Session 1 Expression of IL-1Ra in muscle cells after intramuscle injections of rAAV IL-1Ra. 24. Session 2 High level of IL-1Ra detected in rAAV-IL-1 Ra transduced muscles. 26. VI.
(7) Session 3 Morphology and inflammatory cell count of the muscles 28 Session 4 rAAV-IL-1 Ra treatment prevents myositis in the method of strain measurement Chapter 5 Discussion. 33 35. Session 1 Discussion of results. 35. Session 2 Other Related Discussion. 37. Session 3 Research Limitation. 38. Chapter 6 Conclusions and recommendations. 39. References. 40. VII.
(8) List of Tables and Figures Figure 2-1. Idiopathic orbital myositis with severe muscle destruction. 12. Figure 2-2. Treatment strategy for idiopathic orbital inflammation. 13. Figure 2-3. Mechanisms of interleukin-1 receptor antagonist. 16. Figure 4-1. Immunohistochemistry of IL1-Ra expression three weeks after injection of rAAV-LacZ or rAAV-IL1-Ra in extraocular muscles. 24. Figure 4-2. Representative western blotting of IL1-Ra expression in rabbit extraocular muscle.. 27. Figure 4-3. Effect of IL1-Ra on the muscle after myositis induction in pathology finding one week after phobal ester injection. 29. Figure 4-4. Effect of IL1-Ra on the muscle after myositis induction in pathology finding 12 week after phobal ester injection.. 31. Figure 4-5. Preventing myositis after rAAV-IL1-Ra treatment in strain gauge measurement 1 week after phobol ester injection. VIII. 34.
(9) Chaper 1 Introduction Session I Background Orbital myositis occurs in various diseases, like including thyroid eye disease, and idiopathic myositis. Severe myositis could result in strabismus and proptosis even under current treatment. The detailed pathophysiology and management of either idiopathic or thyroidal orbital myositis is not very clear. Moreover, there is no very effective therapy or preventive method in this field for these disease. Generally, anti-hyperthyroidism medication, oral steroid and pulse therapy are given; radiotherapy is also performed in some hospitals. However, severe and persistent proptosis and strabismus can only be corrected by orbital decompression and muscle surgery.. Session II Purpose In recent studies, increased expression of proinflammatory cytokines particularly interleukin-1 alpha and interleukin-1 beta, tumor necrosis factor-alpha and macrophage inflammatory protein-1 alpha, was observed in muscle of idiopathic inflammatory myopathies. The cytokine interleukin-1 stimulates cell proliferation, glycoaminoglycan synthesis, and prostaglandin production in orbital fibroblasts. There was no difference in cytokine and chemokine patterns between polymyositis, dermatomyositis, and inclusion body myositis, which could indicate that similar pathogenetic mechanisms are involved in these subsets of myositis. Interleukin-1 receptor antagonist (IL-1 Ra) is a naturally occurring protein that binds to IL-1 receptor and blocks the binding of both IL-1α and. 1.
(10) IL-1βwithout inducing a signal of its own and thus is a very effective inhibitor of inflammation. The balance between IL-1 and IL-1Ra in local tissues plays an important role in the susceptibility to and severity of many diseases. In 1990 IL-1Ra was cloned and later on, a large numbers of studies led to disclosure of the crucial importance of the imbalance between IL-1 and IL-1Ra in the pathogenesis of rheumatoid arthritis. Due to the short half life of protein, long term oral medication or repeat injection was used in former experiment.. Session III Research Objectives With the recent advances in gene therapy, the IL-1Ra gene has been delivered by retrovirus-based, adenovirus-based, and adeno-associated virus vectors into synoviocytes to achieve antiinflammatory effects both in vivo and in vitro with varying success. Adenovirus-associated virus vector with a microdystrophin gene was inserted in the muscle tissue and the protein synthesized successfully in a mouse of Duchenne muscular dystrophy. In this study, to establish potential of rAAV in myositis gene therapy, rAAV-delivered IL-1Ra gene was introduced into extraocular muscles. The purpose of this study is to evaluate the recombinant adeno-associated virus vector encoding interleukin-1 receptor antagonist (rAAV–IL-1Ra) complementary DNA for its potential in the prevention of phorbol ester–induced extraocular myositis.. 2.
(11) Chapter 2 Literature review There are four components to be discussed in the literature review. Thyroid eye disease and idiopathic myositis are included in the disease of orbital myositis. Furthermore, the anti-inflammation cytokine, IL-1 Ra, and vector, recombinant adeno-associated virus, are also discussed in details.. Session I Introduction of thyroid eye disease Orbital myositis occurs in various diseases, like including thyroid eye disease, and idiopathic myositis. Severe myositis could result in strabismus and proptosis even under current treatment. The detailed pathophysiology and management of either idiopathic or thyroidal orbital myositis is not very clear. Moreover, there is no very effective therapy or preventive method in this field for these diseases. Generally, anti-hyperthyroidism medication, oral steroid and pulse therapy are given; radiotherapy is also performed in some hospitals. However, severe and persistent proptosis and strabismus can only be corrected by orbital decompression and muscle surgery. There are many different names you might find for the autoimmune eye condition that is often seen with thyroid disease, including: •. Thyroid Eye Disease (TED). •. Graves' Opthamolopathy (GO) Thyroid Eye Disease is an autoimmune eye condition that, while separate from thyroid disease, is often seen in conjunction with Graves' Disease. The condition, however, is seen in people with no other evidence of thyroid dysfunction, and occasionally in patients who have Hashimoto's Disease. Most 3.
(12) thyroid patients, however, will not develop thyroid eye disease, and if so, only mildly so. Graves’ ophthalmopathy continues to be a challenge for the ophthalmologist. The lymphocytic infiltration of orbital tissues are highly suggestive of an autoimmune pathogenesis. The majority of the symptoms can be explained by the increase in volume of the orbital contents due to hyperplasia of the adipose tissue and enlargement of the extraocular muscles following fibroblast stimulation to proliferate and secrete glycosaminoglycan. The cytokines stimulate the espression in orbital fibroblasts of immunomodulatory proteins, but the nature of the autoantigen responsible for the lymphocytic homing and the link with the thyroid gland remain controversial. Thyroid eye disease is characterised by a period of inflammation and engorgement of these tissues, followed by a healing response. Among patinets with thyroid eye disease in the incidence cohort, approximately 90% had Graves hyperthyroidesm, 1% had primaty hypothyroidism, 3% had Hashimoto thyroiditis, and 6% were euthyroid. There was a close temporal relationship between the development of hyperthyroidism and Graves ophthalmolopathy: in about 20% of patinets the diagnoses are made at the same time whereas in approximately 60% of patinets the eye disease occurred within 1 year of onset the thyroid disease. Cytokines are key regulators and mediators of normal and pathologic immune responses. The main cytokines are interferon-gamma, which is the product of activated T cells, and interleukin-1 and tumor necrosis factor-alpha, which are mainly secreted by macrophages. In addition, human fibroblasts 4.
(13) express a number of regulatory molecules that influence immune mechanisms, and treatment with the proinflammatory cytokine interleukin-1 can lead to their upregulation. The cytokine interleukin-1 stimulates cell proliferation, glycosaminoglycans synthesis, and prostaglandin production, along with induction of adhesion molecules, immunomodulatory proteins, and metalloproteinases in orbital fibroblasts. Interleukin-1 receptor antagonist is a naturally occurring inhibitor of interleukin-1 that inhibits interleukin-1-induced stimulation of orbital fibroblast GAG synthesis in vitro. In vitro expression of interleukin-1 receptor antagonist mRNA and protein has been shown to be significantly lower in thyroid eye disease when compared with normal orbital fibroblasts. This suggests an imbalance between interleukin-1 receptor agonist and antagonist, which may facilitate interleukin-1 receptor–mediated proinflammatory and fibrogenic actions in GO. GO patients who respond well to orbital radiotherapy have increased serum interleukin-1 receptor antagonist, leading the authors to hypothesize that glucocorticoid and radiotherapy may influence agonist stimulation of the interleukin-1 receptor by altering interleukin-1 receptor antagonist expression in human orbital fibroblasts. Low doses of ultraviolet and ionizing irradiation, but not dexamethasone, were shown to stimulate interleukin-1 receptor antagonist RNA and protein expression in Graves and normal orbital fibroblasts. In contrast, interleukin-1 beta induced transcription of two of the three hyaluronan synthase genes in GO orbital fibroblasts, and this could be attenuated by dexamethasone. Hyaluronan is one of the three main glycoaminoglycans found in GO. An increase in chondroitin sulfate in GO orbits in vivo and in 5.
(14) particular a shift to more highly sulfated, negatively charged compounds, with an increased water binding capacity, has been reported. (1) Epidemiology of Thyroid Eye Disease GO affected women approximately six times more frequently than men. The peak incidence rates occurred in the age groups 40-44 years and 60-64 years in women and 45-49 years and 65-69 years in men. The median age at the time of diagnosis of GO was 43 years. Although GO typically is associated with hyperthyroidism, and some cases arise in the setting of primary hypothyroidism, a small portion of patients with GOare euthyroid. Previous studies estimated the prevalence of euthyroid GO to be 6 to 21% in patients with GO. A recent study, however, indicates that more sensitive assays for thyroid hormone concentrations may be able to detect hyperthyroidism in the vast majority of patients with GO. Only 0.7% of patients in this study of 1020 Asian patients with GO were found to be euthyroid. In contrast to the low level of euthyroidism detected in this Asian study, a European group reported a 12.9% prevalence of euthyroid GO in patients with myasthenia gravis, compared with a 3.1% prevalence of euthyroid GO in patients without myasthenia. Although the results obtained in this university clinic-based study may have been influenced in part by referral bias, they may prompt future population-based studies to address more rigorously whether euthyroidism is more prevalent in myasthenic patients with GO than in patients with GO who do not have myasthenia gravis. The prevalence of open-angle glaucoma in patients with hyperthyroidism or GO recently was reported to be higher than previously considered. Clinicians should consider GO a possible risk factor for ocular hypertension and open 6.
(15) angle glaucoma, and should monitor patients' intraocular pressure, optic nerve appearance, and visual fields accordingly. (2) Clinical Features of Thyroid Eye Disease Signs and symptoms include: Pain in the eyes, pain when looking up, down or sideways •. Dryness, itching, dry eyes, difficulty wearing contact lenses. •. Inflammation and swelling of the eye, and its surrounding tissues. •. Swelling in the orbital tissues which causes the eye to be pushed forward. -- referred to as exophthalmos -- which can make Thyroid Eye Disease sufferers appear to have a wide-eyed or bulging stare. •. Bloodshot appearance to eyes. •. diplopia. •. Impaired vision. Thyroid Eye Disease is known to go through varying degrees of severity, and can go into periods of remission as well. When it has been inactive for a period of around a half a year, it's less likely to recur.. (3)Treatment of Thyroid Eye Disease 1. Medical treatment Although corticosteroids commonly are prescribed for clinically active GO, their many side effects limit their long-term usefulness. Patients with mild symptoms can often be successfully treated with frequent application of lubricating eye drops and eye covers at night. Humidification of room air can. 7.
(16) prevent drying of the eyes, and wrap-around polarizing sunglasses can also help relieve glare. Diplopia can be alleviated with prism lenses while awaiting either spontaneous improvement or surgical correction. Temporary plastic prisms are available which are applied to glasses and changed as needed. Prednisone, a steroid medication, may be taken orally to provide temporary relief from pain, swelling and redness, although side effects of the medication may limit the use of prednisone and related drugs. Overall, it is important to keep in mind that eye disease associated with Graves' disease will only improve gradually. 2. Radiation treatment Orbital radiation is used to treat the compressive optic neuropathy and the orbital inflammatory signs associated with GO. Radiotherapy decreased orbital congestion by interrupting the immunologic processes that promote inflammation in the retrobulbar tissue. A recent study confirms prior case series data by reporting good efficacy of orbital radiation in treating compressive optic neuropathy. In this retrospective, uncontrolled case series with four months of follow-up, the authors report that 8 of 10 GO patients treated with 2000 cGy showed improved optic nerve function after radiation therapy. Although the authors did not provide statistical analysis, their descriptive data indicate that mean visual acuity improved modestly from 20/30 before treatment to 20/20 after treatment. Color vision and peripheral visual field measures also improved. The efficacy of orbital radiation in treating GO-associated orbital edema, myopathy, and proptosis was evaluated in two retrospective case series, with conflicting results.. 8.
(17) 3. Surgical treatment Ophthalmopathy may contimue to progress even after a euthyroid state has been achieved. In most patients, the eye disease tends to stabilize over a course of weeks to monthes. If the eye condition does not improve or deteriorates despite treatment, surgery may be required. The enlargement of tissue behind the eye may sometimes cause significant exophthalmos, which produces the disfigurement, worsens the symptoms, and causes ocular exposure. Swelling in the orbit may actually contribute to vision loss as pressure increases on the optic nerve. Surgical procedures to relieve pressure on the optic nerve improve vision and allow the eye to settle back to a more normal position. Orbital decompression, although typically indicated to treat optic neuropathy, severe orbital congestion, or advanced proptosis, has been used increasingly in recent years as an elective procedure to enhance cosmesis in patients without sight-threatening ophthalmopathy. If intractable diplopia in primary gaze or in the teading position persistd, then strabismus surery may be helpful in restoring single vision. This surgery entails detaching and repositioning the eye movement muscles on the eyeball to improve ocular alignment and minimize double-vision. Retracted and puffy eyelids can alter a person's appearance and increase the risk of cornea drying. Similarly, procedures to correct eyelid retraction may improve ocular comfort and help to restore a more normal appearance. Corrective eyelid surgery can alleviate the problem through adjustable loosening of the eyelid muscles, as well as removal of scar tissue, excessive fatty tissue and. 9.
(18) skin to place the eyelids into a more normal position. Elective orbital decompression, strabismus surgery and eyelid retraction repair ususlly are not considered until a euthroid state has been maintained for several months and the ophthalmic signs have been confirmed to be stable. Patients with eye disease who have had their hyperthyroidism treated previously should also be examined at regular intervals to make certain that thyroid function remains normal since recurrence of hyperthyroidism, or development of hypothyroidism, may cause the eye disease to flare up.. Session II Introduction of Idiopathic orbital myositis Both children and adults may be afflicated by idiopathic inflammation of the orbital tissue. Idiopathic orbital inflammation is often subclassified on the basis of the anatomic target area within the orbit. Idiopathic orbital myositis is a subtype of nonspecific orbital inflammation primarily involving the extraocular muscles. It occurs most frequently in young to middle-aged adults with a 2 to 1 female predominance. Typically, patients present with acute onset of orbital pain, restreicted eye movement, and proptosis. Conjunctival vascular injection and chemosis are common, as are eyelid erythema and soft-tissue swelling. The classic patient presents with an abrupt onset of edema, erythema, chemosis, and pain and shows exquisite sensitivity to oral corticosteroids, often reporting subjective improvement within one or two days. In the ideal case, there is no flare-up as steroids are tapered. Myositis may affect one or multiple extraocular muscles. IOI may be unilateral or bilateral, and both sides may be involved either simultaneously or at varied intervals 10.
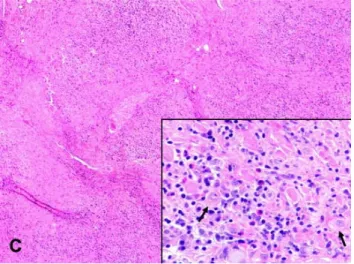
(19) (1.) Pathogenesis In recent studies, increased expression of proinflammatory cytokines particularly interleukin-1 alpha and interleukin-1 beta, tumor necrosis factor-alpha and macrophage inflammatory protein-1 alpha, was observed in muscle of idiopathic inflammatory myopathies. The cytokine interleukin-1 stimulates cell proliferation, glycoaminoglycan synthesis, and prostaglandin production in orbital fibroblasts. There were no difference in cytokine and chemokine patterns between polymyositis, dermatomyositis, and inclusion body myositis, which could indicate that similar pathogenetic mechanisms are involved in these subsets of myositis.. (2.) Histopathlogy Histopathologically, the extaocular myositis ic characterized by a pleomorphic cellular infiltrate consisting of lymphocytes, plasma cells, and histiocytes within the edematous with variable degrees of reactive fibrosis, but preserved architecture of affected tissue. There may be extensive destruction of the background extraocular muscle fibers (Figure 2-1), or other affected tissues. Granulomas, including giant cells, require exclusion of mycobacterial and fungal infections, sarcoidosis and Wegener granulomatosis.. 11.
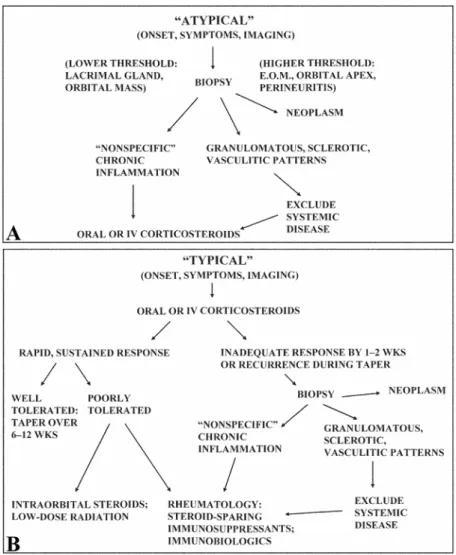
(20) Source: Ophthalmic Plastic and Reconstructive Surgery, Inc. Volume 22(2), March/April 2006, pp 79-86. FIG. 2-1. Idiopathic orbital myositis with severe muscle destruction (hematoxylin and eosin stain, original magnification ×40). Inset, Dense mixed inflammatory cell infiltrate among swollen, degenerating muscle fibers (arrows) (hematoxylin and eosin stain, original magnification ×400).. (3.) Treatment Strategy Initial therapy consists of systemic corticosteroids in doses adjusted to the individual patinet’s need in typical cases. Atypical clinical or imaging findings should prompt biopsy (Figure 2-2A). The threshold for biopsy should be lower for lacrimal gland lesions, since aggressive malignancies can present with inflammatory signs. If the biopsy reveals nonspecific inflammation, or if there are specific patterns of inflammation and systemic disease is excluded, treatment with steroids can begin.. 12.
(21) Source: Idiopathic Orbital Inflammation: A Pathogenetic Construct and Treatment Strategy: The 2005 ASOPRS Foundation Lecture. FIG. 2-2. Treatment strategy for idiopathic orbital inflammation. A, For atypical cases. B, For cases with the abrupt onset of inflammatory signs and symptoms, and with imaging compatible with a topographical variant of IOI. If the findings are typical, systemic corticosteroids should be beginned (Figure 2-2B). Acute cases generally responde rapidly. With a rapid response that is sustained and well-tolerated, dosage should be slowly tapered. Because many other orbital pathologic processes may be masked by steroids, incomplete therapeutic response suggests the need for orbial biopsy for histopathlogic 13.
(22) confirmation after 1 to 2 weeks at the higher doses, biopsy should then be performed. If the results are consistent with idiopathic inflammation, alternative therapy will be needed, and a rheumatologist should be enlisted at that point. (4.) Therapeutic Options Therapeutic approaches to idiopathic extraocular myositis have included observation, nonsteroidal antiinflammatory drugs, radiation therapy, “therapeutic” surgery, intravenous immunoglobulin, plasmapheresis, corticosteroids, immunosuppressants, and immunobiologic agents. In very mild cases, simple observation or nonsteroidal agents may suffice. Radiation may be effective in some patients who are steroid-responsive but steroid-intolerant. Rarely, orbital decompression or surgical debulking may have value for large sclerotic masses. Corticosteroids remain the first-line treatment in most cases. Depending on severity and response, beginning dose with oral prednisolone at 1.0 to 1.5 mg/kg/d (60-80 mg/d) for 1 to 2 weeks and then taper dosage very slowly below about 40 mg per day, generally over a period of several months. If a biopsy is performed prior to treatment, intraoperative corticosteroids (intravenous methylprednisolone, 125 to 250 mg) can be administered after frozen-section confirmation of the diagnosis. Intravenous corticosteroids at higher doses (methylprednisolone, 1.0 g/d for 1 to 3 days) can be given to patients with atypical involvement and vision loss. Intraorbital triamcinolone (40 mg/ml) is useful during surgery, especially in sclerosing inflammation, and can be considered for outpatients with steroid-responsive but steroid-intolerant disease.. 14.
(23) Immunosuppressants have been used for patients who do not fully respond to corticosteroids, or cannot tolerate side effect. Orbital radiation, antimetabolites, T-cell inhibitors and alkylating agents (e.g., cyclophosphamide) may be useful in controlling the disease.. Session III Interleukin-I Receptor Antagonist Interleukin-1 receptor antagonist (IL-1 Ra) is a naturally occurring protein that binds to IL-1 receptor and blocks the binding of both IL-1α and IL-1β without inducing a signal of its own and thus is a very effective inhibitor of inflammation. The balance between IL-1 and IL-1Ra in local tissues plays an important role in the susceptibility to and severity of many diseases. In 1990 IL-1Ra was cloned and later on, a large numbers of studies led to disclosure of the crucial importance of the imbalance between IL-1 and IL-1Ra in the pathogenesis of rheumatoid arthritis. Due to the short half life of protein, long term oral medication or repeat injection was used in former experiment.. 1.) Endogenous Interleukin-I Receptor Antagonist IL-1Ra, discovered in the 1980s, inhibits the proinflammatory effects of IL-1 by functioning as a competitive inhibitor for receptor binding of IL-1. Restoring the balance between IL-1Ra and IL-1 with the administration of exogenous recombinant IL-lra is one therapeutic approach that has been investigated in recent years.. 2.) Human Recombinant Interleukin-1 Receptor Antagonist (ANAKINRA) 15.
(24) Endogenous IL-1Ra has been purified, sequenced, cloned as a cDNA, and expressed in Escherichia coli. Anakinra has a molecular weight of 17 kDa and binds to IL-1 receptors with an affinity nearly equal to that of IL-1. The mechanism is required of a second cell membrane molecule termed IL-1 accessory protein (IL-1AcP). When IL-1 binds to the IL-1RI, IL-1AcP interacts with the receptor-ligand complex and initiates cell stimulation. Anakinra, when bound to the IL-1RI, prevents IL-1AcP from interacting with the receptor, resulting in no response. Figure 2-3 illustrates the mechanism of action of endogenous IL-1Ra, which operates in the same manner as anakinra. The antagonistic effects of anakinra on IL-1- induced PGE 2 secretion, production of metalloproteinases, and proteoglycan degradation have been demonstrated in vitro. Anakinra blocked IL-1-induced T-cell proliferation and PGE 2 as well as collagenase production in cultured synovial cells.. Source: Clinical Therapeutics. 2004;26:1960-1975). 16.
(25) Session IV Recombinant Adeno-asssociated Virus Vector. With the recent advances in gene therapy, the IL-1Ra gene has been delivered by retrovirus-based, adenovirus-based, and adeno-associated virus vectors into synoviocytes to achieve antiinflammatory effects both in vivo and in vitro with varying success. Adenovirus-associated virus vector with a microdystrophin gene was inserted in the muscle tissue and the protein synthesized successfully in a mouse of Duchenne muscular dystrophy. In this study, to establish potential of rAAV in myositis gene therapy, rAAV-delivered IL-1Ra gene was introduced into extraocular muscles.. (1.) AAV and Recombinatn AAV Vectors AAV is one of a relatively small group of viruses that have been successfully modified for use as gene transfer agents in human trials. AAV is a 20-nm diameter replication-deficient parvovirus native to humans and nonhuman primates and exists in nature in over 100 distinct variants, including both those defined serologically as serotypes and those defined by DNA sequence as genomovars. There is no consistent indication of AAV infection being associated with human disease. The life cycle of AAV has been studied in detail. Cells infected with AAV require a helper virus, such as an adenovirus, herpesvirus, or vaccinia virus, to replicate efficiently in cell culture. Recombinant adeno-associated virus (rAAV) has proven to be a promising gene delivery vector for human gene therapy. Recombinant AAV vectors based 17.
(26) on the most frequently studied serotype, AAV2, were produced in the mid-1980s by creating ITR-deleted helper plasmids to supply rep and cap functionsm. Recombinant AAV2 vector plasmids were also constructed in which ITR-sequences flanked the therapeutic gene of interest, along with an appropriate promoter and polyadenylation signal. When helper plasmids and vector plasmids were co-transfected into permissive cells (usually human embryonic kidney 293 cells) that were also infected with a helper adenovirus, those cells packaged rAAV2 virions containing only the therapeutic vector genomes. Vector particles, thus produced, could be purified using CsCl density gradient ultacentrifugation. Over time, rAAV2 packaging and purification technology has improved, and helper plasmids now most frequenly encode both adenovirus and AAV helper genes. Recombinant vector particles are often purified using column chromatography methods and/or nonionic gradient media, resulting in a higher level of infectivity of recombinant virus as well as higher overall titers. Preclinical studies demonstrated that rAAV vectors were capable of long-term gene transfer and expression in the bronchial epithelium of rabbits and nonhuman primates. Importantly, studies also demonstrated no increase in inflammatory cells, or pro-inflammatory cytokines after rAAV delivery to the lower airways of nonhuman primates. Likewise, there were no adverse changes in chest x-rays, arterial blood gases, or pulmonary function tests in these animals after rAAV delivery. Based on this information, a number or phase I and phase II clinical trials of rAAV2-CFTR were performed.. (2.) Future Directions 18.
(27) rAAV is characterized by excellent safety profiles, wide host range, and the ability to transduce differentiated cells. Numerous rAAV-based vectors providing efficient and sustained expression of transgenes in target tissues have been developed for preclinical studies. Interest in rAAV has been driven by advances in production methods originally developed for rAAV serotype 2 vectors and expanded to include alternative serotypes. Recent years have also witnessed an extensive expansion of the use of these vectors to other diseases, particularly genetic and metabolic disorders involving the muscle, liver, and CNS. Recombinant AAV vectors have also been used to model and complement important animal models that better mimic the human phenotypes of these disorders. The combination of better animal models and improved biologic efficacy support the concept that in the future, safe and effective rAAV-mediated gene transfer methods will be devised.. 19.
(28) Chapter 3 Research Methods Session 1 Research Materials and Methods Vector construction and rAAV production Human IL-1Ra complementary DNA (cDNA) was obtained by reverse transcriptase–polymerase chain reaction (RT-PCR) from RNA prepared from U937 cells which were treated with phorbol ester for 48 hours. The forward primer used in the PCR reaction was 59-TAgcggccgcATGGAAATCTGC-39, which not only spans the region covering the initiation codon (underlined) and its flanking sequences but also contains a NotI site (the lower-case letter) at the 59 end. The PCR product was sequenced by the dideoxynucleotide termination method and found to be identical to the IL-1Ra sequences reported in GeneBank. The IL-1Ra gene was cloned between the 2 Not I sites of pXX-UF1 to replace green fluorescent protein gene, and was thus placed under the transcription regulation of human cytomegalovirus (CMV) immediate early promoter. The rAAV encoding IL-1Ra and E coli lac Z gene were produced by a 3-plasmid cotransfection system as previously described. The rAAVs were purified twice by cesium chloride ultracentrifugation as described. Titers of rAAV–lac Z and rAAV–IL-1Ra were determined by dot-blot hybridization using lac Z DNA and IL-1Ra cDNA, respectively, as probes.. Rabbit and vector administration Male New Zealand white rabbits weighing 2-3 kg were used after review and approval of the protocol by the animal experimentation committee at our institution. Animals were anesthetized with intramuscular thiazine hydrochloride(1 mg/kg) and ketamine hydrochloride (30 to 35 mg/kg). Topical anesthesia was obtained with two drops of 0.5% proparacaine hydrochloride. 20.
(29) Each rabbit received an injection of 40 µl of rAAV-lac Z virus (109 particles /20μl phosphate buffered solution (PBS)) into the right superior rectus muscle and the same injected amount of rAAV-IL1-Ra virus in the left superior rectus muscle. Three weeks later, the 12-0-tetradecanoyl-phorbol-13-acetate (TPA; Sigma, St. Louis, MO, USA ) was diluted to 0.1 mg/mL with oliver oil in a sterile manner, and 0.01 mL of solution (1µg) was injected for induction of myositis in both eyes.. Strain measurement of rabbit superior rectus muscle A wire lid speculum was spread to 25 mm. A superior 1800 limbal peritomy was performed and the superior rectus complex was isolated with a muscle hook and then slung with a precut 2-0 cotton suture. The muscle was then carefully cleaned of all attachment to Tenon’s capsule until the muscle belly could be seen to exit the capsule posteriorly. The 2-0 cotton suture was tied to a previously zeroed 250-strain gauze. The globe was rotated opposite the muscle’s primary direction of action by pulling on the strain gauge until 50µg of pull was measured. The direction of pull on the muscle was kept parallel to the tangent of the muscle’s insertion. The lower lid was permanently marked with 6-0 prolene where the inferior corneal limbus intersected the lower lid margin at 50µg of pull. After an initial strain measurement, intramuscular injections were given into the superior rectus muscle 3mm posterior to its insertion using a 30-gauge needle. The needle tip was advanced into the muscle belly under direct visualization. After the injection was complete, the conjuctiva was then loosely approximated without sutures and a topical antibiotic was applied. 21.
(30) Immunohistochemistry staining Immunohistochemical analysis was performed on formalin-fixed, paraffin-embedded tissue sections (5 µm) using an ImmunoCruz Staining System kit (Santa Cruz Biotechnology, Santa Cruz, CA, USA). Briefly, the dewaxed, rehydrated sections were treated with 0.3% hydrogen peroxide in methanol. The sections were incubated with blocking serum (normal donkey serum), and then with the primary goat anti-human IL-1ra antibody (1:50 dilution; R&D Systems, Minneapolis, MN, USA) for 1 hour. After washing, membranes were incubated with a Rabbit anti-goat immunoglobulin (1:250 dilution; Santa Cruz Biotechnology, Santa Cruz, CA) as a secondary antibody for 1 hour. Finally, bound antibody complexes were stained with 0.05% diaminobenzidine. Sections then were counterstained with methyl green, dehydrated, and mounted.. Western blot analysis Six tissue samples of muscles treated with rAAV-IL1-Ra, three of muscles treated with rAAV-LacZ and three of normal muscles were used for determination of the expression of variant forms of the IL-1ra by Western blotting. The tissue samples were stored at −80°C until assay. Frozen tissues were homogenized in Triton lysis buffer. The procedures for treatment were carried out at 0–4°C. After sonication, the insoluble material was removed by centrifugation at 15,000g for 60 min. The total protein concentration of the supernatant was measured by the method of Bradford. The extracts were treated with SDS sample buffer and boiled for 3 min. Fifty micrograms of these protein samples were subjected to SDS–PAGE in 12% acrylamide and then 22.
(31) electrophoretically transferred to a nitrocellulose membrane (Amersham Pharmacia Biotech, Bucks, UK). After incubating the membrane in 4.5% skimmed milk–Tris-buffered saline overnight at 4°C, the membrane was incubated for 1 h at room temperature with the goat IL-1ra antibody (1:1000; R&D Systems). After washing, membranes were incubated with a anti-goat immunoglobulin (1:10000; PerkinElmer life sciences, Wellesley, MA ) as a secondary antibody for 1 h. After washing, the membrane was developed using a chemiluminescence system (ECL plus Western blotting detection system, Amersham Pharmacia Biotech) and exposed to film (Fuji Medical X-ray Film, Nakanuma, Japan).. Histoogy For histologic analysis, tissue harvested from dissected muscle was fixed in 4% paraformaldehyde for 24 hours. The fixed tissues were embedded in paraffin, cut into 5-mm sections, and stained with hematoxylin and eosin. The number of inflammatory cells in muscle in the sections was counted.. Session 2 Analytic Methods One-way analysis of variance (ANOVA) was used to determine the statistical differences in the inflammatory cell counts and strain measurement among the 3 protocols of the muscular tissue between normal muscles, muscles injected with rAAV-LacZ, and rAAV-IL-1 Ra. The data were obtained by statistical software (SPSS version 11.0; SPSS Inc., Chicago, IL) and are expressed as the mean in terms of the standard deviation with p<0.01 considered to be significant. A post hoc test using LSD test was performed. 23.
(32) Chapter 4 Results Session 1 Expression of IL-1Ra in muscle cells after intramuscle injections of rAAV IL-1Ra To determine whether three weeks after gene delivery, the muscles were resected for immunohistochemistry study. A majority of the myofibers stained positive for IL-1Ra in cytoplasm (Figure 4-1A), whereas no expression of IL-1Ra was identified in the control muscles (Figure 4-1B). These results confirmed that IL-1Ra was expressed in rAAV- IL-1Ra transduced muscle cells.. 24.
(33) Figure 4-1. Immunohistochemistry of IL1-Ra expression three weeks after injection of rAAV-LacZ or rAAV-IL1-Ra in extraocular muscles. A: The left superior rectus muscles of rabbits were transduced with rAAV-IL1-Ra. Cells possessing IL1-Ra protein appear brown particles in cytoplasm. B: The right superior rectus muscles were transduced with rAAV-LacZ. The cells stained with hemotoxylin appear light blue. (Immunohistochemistry; original magnification, X200). 25.
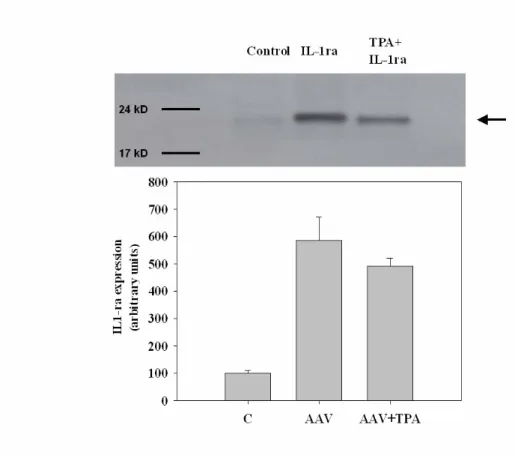
(34) Session 2 High level of IL-1Ra detected in rAAV-IL-1 Ra transduced muscles Western blot analysis of muscles transduced with rAAV-IL-1 Ra showed a dense level of IL-1 Ra expression at 23 KD. (Figure 4-2, line 2) A very faint band was noted comparable to that of the untreated muscles. (Figure 4-2, line 1) This indicated that cells transduced with rAAV-IL-1 Ra synthesized significant levels of IL-1 Ra in the muscle. Muscles treated with rAAV-IL1 Ra vector and TPA injections showed moderate staining, but it was lighter than that of muscle, which was only injected with rAAV-IL1-Ra. (Figure 4-2, line 3) The IL-1 Ra level in muscles transduced with rAAV-IL-1 Ra was 6 times higher than that in the untreated muscles. The muscles treated with rAAV-IL1 Ra vector and TPA injections showed a slight lower amount of IL-1 Ra than the muscles transduced with rAAV-IL-1 Ra.. 26.
(35) Figure 4-2. Representative western blotting of IL1-Ra expression in rabbit extraocular muscle. Muscle sample, which received a rAAV-IL1-Ra vector injection 3 weeks previously, exhibits IL1-Ra gene expression with expected molecular weight 23kD (middle line). Muscle treated with rAAV-LacZ injection reveals very slight band. Muscle treated with rAAV-IL1-Ra vector and TPA injection shows moderate stain and is lighter than muscle, which was only injected with rAAV-IL1-Ra only. (C: control group with no treatment). 27.
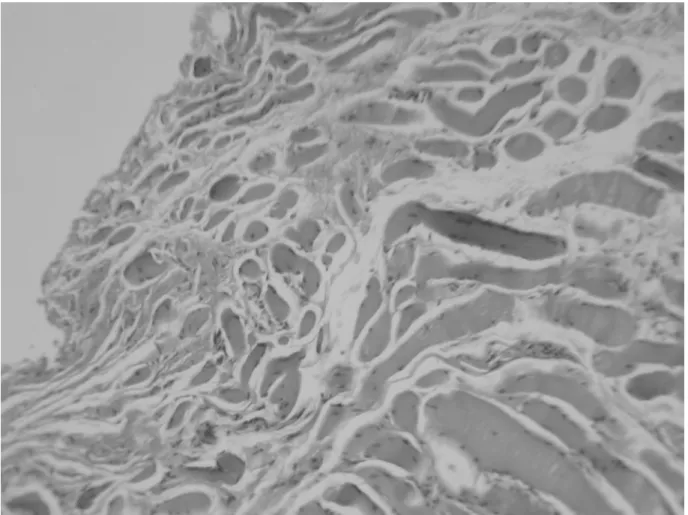
(36) Session 3 Morphology and inflammatory cell count of the muscles The right superior rectus muscles of the rabbits were previously injected with rAAV-LacZ and the left with rAAV-IL-1 Ra (n=10) and then with TPA 3 weeks later. A separate group of non-pretreated rabbits that received only TPA injection served as controls (n=10). Myositis was induced three weeks after viral transduction. When compared with the myositis pretreated with rAAV-IL-1 Ra, the myositis pretreated with rAAV-LacZ injection showed signs of severe inflammation such as muscular engorgement, edema, vascular injection and increase of muscle thickness. Myositis pretreated with rAAV-IL-1Ra showed milder inflammation. .. Figure 3 shows the histologic morphology 1 week after TPA injection. When. compared with the normal muscles (Figure 4-3A), the inflammatory muscles with rAAV-LacZ injection (Figure 4-3B) showed severe signs of muscular coagulation necrosis and many inflammatory cells such as lymphocytes. Muscles treated with rAAV-IL-1 Ra (Figure 4-3C) showed better preservation of muscle cells and fewer inflammatory cells. To further document the anti-inflammatory effect of IL-1 Ra gene delivery, we compared the inflammatory cell count of the muscular tissue between normal muscles, muscles injected with rAAV-LacZ, and muscles injected with rAAV- IL-1 Ra. The number of inflammatory cells in muscle was counted in the central area of 0.25 mm2 in the sections. In the normal muscle, the mean number of inflammatory cell count was 2.274±1.810 cells/mm2 (n=10). One week after myositis induction, more inflammatory cells were retained in the rAAV- LacZ treated muscles (2594.386±319.933 cells/mm2; n=10) than in the rAAV- IL-1 Ra treated muscles (1369.479±228.509 cells/mm2; n=10) or in the normal muscles. These results were statistically significant (p<0.01 and p<0.01, respectively). 28.
(37) 29.
(38) Figure 4-3. Effect of IL1-Ra on the muscle after myositis induction in pathology finding one week after phobal ester injection.. A: Normal muscles without any. treatment. B: muscles treated with rAAV-LacZ previously C: Muscles treated with rAAV-IL1-Ra previously. Better preservation of the muscle structure (arrow head), less muscle cell necrosis and fewer lymphocytes (arrow) are noted in muscles pre-treated with rAAV-IL1-Ra than in the group pre-treated with rAAV-LacZ. (Hematoxylin-eosin; original magnification, X100).. 30.
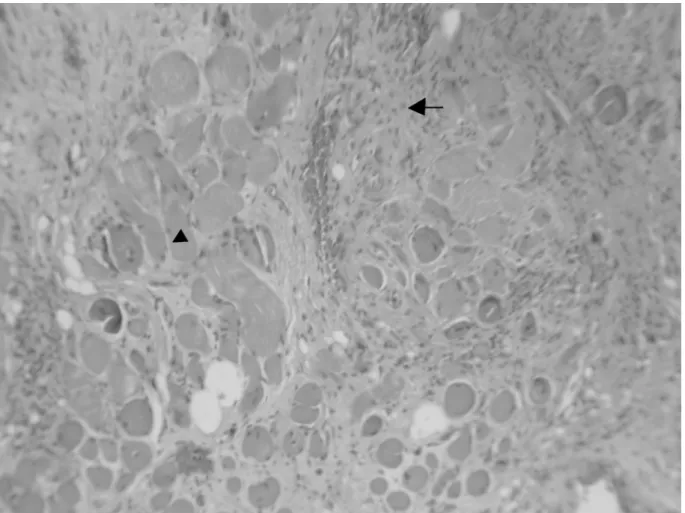
(39) At 12 weeks, muscles treated with rAAV-LacZ injection showed dense fibrotic tissue and few intact muscle bundles. (Figure 4-4A) Better preservation of muscle tissue and less fibrosis was noted in the muscles treated with rAAV-IL-1Ra. (Figure 4-4B). 31.
(40) Figure 4-4. Effect of IL1-Ra on the muscle after myositis induction in pathology finding 12 week after phobal ester injection. A: Mixture of densely packed fibrous connective tissue (arrow) and muscle cells is revealed in the histology of the muscle treated with rAAV-LacZ injection. B: In the muscles pre-treated with rAAV-IL-1 Ra, less fibrous tissue and better preservation of muscle structure are noted. (Hematoxylin-eosin; original magnification, X100).. 32.
(41) Session 4 rAAV-IL-1 Ra treatment prevents myositis in the method of strain measurement With the method of strain measurement of superior rectus muscle, the lid margin where rotate opposite the muscle’s primary direction of action by pulling on the strain gauge 50 g of pull was marked. Repeated strain measurements to previous marked lid margin 7 days after myositis induction revealed 125.20±6.75 g in rAAV-LacZ treated muscles, 124.60±9.477 g in non pre-treated muscles, and 81.90±7.09g g in rAAV-IL-1 Ra treated muscles. (Figure 4-5) The lower strain gauze measurement in rAAV-IL-1 Ra-treated group indicated that rAAV-IL1-Ra treatment (n=10) was significantly better at preventing TPA induced myositis than rAAV-LacZ treatment (n=10) or no pre-treatment (n=10).These data thus demonstrated that rAAR-IL-1 Ra prevented the development of severe inflammation in muscles (p<0.01).. 33.
(42) Figure 4-5. Preventing myositis after rAAV-IL1-Ra treatment in strain gauge measurement 1 week after phobol ester injecction. rAAV-IL1-Ra treated muscles (n=10) significantly prevent muscle from phobol ester induced myositis than rAAV-LacZ treated muscles (n=10) and in untreated muscles (n=10). Groups marked with an asterisk ( ) were significantly different from the rAAV- IL1-Ra transfected group ( p<0.001). In the event of a significant ANOVA, a post hoc test using Scheffe’s multiple comparison was performed.. 34.
(43) Chapter 4 Discussion Session 1 Discussion of results By immunohistochemistry, we confirmed that intramascular injections of rAAV- IL-1 Ra resulted in IL-1 Ra protein expression. Results from Western blot confirmed that high levels of IL-1 Ra were produced in the muscle. The appearance and histological analysis revealed milder inflammation of the muscle injected with rAAV- IL-1 Ra after myositis induction. Functionally, strain measurement confirmed moderate prevention of severe myositis in muscle tissue. Our results thus demonstrate the possibility of using gene therapy to prevent extraocular myositis. In this study, intramuscular injection of TPA was used to induce the animal models of extraocular myositis. TPA can produce inflammation or promote tumor development. The most potent is TPA, also known as phorbol myristate acetate. When rabbit alveolar macrophages were treated with TPA phorbol-12-myristate-13-acetate and lipopolysaccharide, the synthesis of interleukin-1, as well as tumor necrosis factor, was greatly increased. Whether or not rAAV vector itself will result in viral myositis is very important for gene therapy. In this study, we used rAAV–Lac Z and PBS in attempts to generate nonspecific inflammation in the muscle. One week after intramuscular injection, the histologic analysis of extraocular muscle revealed mild inflammation after PBS or rAAV-lac Z injection, and the degrees of inflammation were similar in these two samples (data not shown). Three weeks after injection, no more inflammation was noted in either group. We concluded that rAAV-lac Z and PBS would induce only mild inflammation. rAAV vectors did not induce severe inflammation following intramuscular injections in the 35.
(44) absence of TPA treatment. This indicated that rAAV is a safe gene-delivery tool for myositis therapy. In addition, we evaluated the adjacent tissues such as cornea, anterior chamber, lens, vitreous and retina; no obvious adverse morphologic effects like retinitis, vitritis or keratopathy were noted. This means that rAAV will not induce obviously adverse morphologic effects in neighboring tissues. Gene therapy researchers have been generally concerned about the diffusion of the vector to the major organs. In a previous study, rAAV-IL1 Ra was injected into the knees of rats. No rAAV DNA has yet been found in tissues such as the brain, lung, liver, spleen, and gonads under conditions that can detect 10 copies of vector DNA in 1mg of cellular DNA. This indicates that the diffusion of rAAV vectors to major organs may not be a problem. In short conclusion, rAAV is an efficient and safe vector for the transduction of muscle tissues. rAAV vectors are based on a non-pathogenic human parvovirus (AAV) that is unique in its ability to persist in human cells without causing any pathologic effects. The result of western blotting showed significant production of IL-1 Ra after muscles were transduced with rAAV-IL-1 Ra. In this study, TPA was used to induce myositis three weeks after rAAV-IL-1 Ra injection. The high level of IL-1 Ra mildly decreased after TPA injection. This may be ascribed to the use of IL-1 Ra after induction of inflammation or the decreased production of IL-1 Ra after myositis induction. In this study, the intramuscular injection of rAAV-IL-1 Ra had a partially preventive effect in the myositis model. It is well-known that several proinflammatory cytokines, including interleukin-1 alpha, interleukin-1beta, tumor necrosis factor -alpha and macrophage inflammatory protein-1alpha have been observed in idiopathic inflammatory myopathies. Interleukin -1 is only one 36.
(45) among several inflammatory factors. Furthermore, not all of the muscular cells could be transferred the IL1-Ra gene by local injection of this vector successfully. This could account for the only partially preventive effect.. Session 2 Other Related Discussion Increased expression of proinflammatory cytokines particularly interleukin -1alpha and IL-1beta, tumor necrosis factor-alpha and macrophage inflammatory protein-1alpha, was observed in muscle of idiopathic inflammatory myopathies. In Graves’ ophthalmopathy, the main cytokines are interoeukin-1, tumor necrosis factor-alpha, and interferon-gamma. In the inflammatory process, macrophages then are stimulated to synthesize and release a variety of cytokines, primarily interleukin -1 and tumor necrosis factor-alpha. IL-I also participates in the mechanisms of tissue destruction through the induction of fibroblast proliferation. Collectively, these data indicate that Interleukin-1 is one of the most important proinflammatory cytokine. Three structurally related ligands for IL-1receptors have been described. These include two agonists, IL-1 α and IL-1 β, and a specific receptor antagonist, IL-1Ra. Interleukin-1 receptor antagonist is a naturally occurring inhibitor of interleukin-1. Elevation of both IL-1Ra mRNA and protein in serum of patients with active-stage polymyositis and dermatomyositis suggests that higher levels of serum IL-1 Ra may reflect increased IL-1 Ra production in myositis, and that IL-1Ra may regulate IL-1-mediated muscle fiber damage. Furthermore, radiotherapy is indicated in active Graves ophthalmopathy. Recent data have indicated that low doses of UV and ionizing irradiation dose dependently up-regulated IL-1RA-specific transcripts in Graves Ophthalmopathy 37.
(46) and control orbital fibroblasts. IL-1 Ra represents an important new biologic approach to treating patients with rheumatoid arthritis. Therapy and prevention of arthritis by recombinant adeno-associated virus vector with delivery of interleukin-1 receptor antagonist has also been documented. The balance between IL-1 and IL-1Ra in local tissues plays an important role in the susceptibility to and severity of many diseases. It is possible that the endogenous upregulation of IL1-Ra alone is not sufficient to produce an anti-inflammatory effect. We speculate that sustained expression of IL-1Ra will provide the additional anti-inflammatory effect needed to combat myositis. The observations described here support this postulation.. Session 3 Research Limitation There were certainly some limitations in this study. First, this animal study provided the results of prevention of extraocular myositis by rAAV-IL-1 Ra. Further human studies are needed to determine the effect in human being. Second, the main inflammatory-related cytokines are interoeukin-1, tumor necrosis factor-alpha, and interferon-gamma in Graves’ ophthalmopathy. Besides interleukin-1, further studies of other antagonist of pro-inflammatory cytokines could be used for the prevetion of inflammation additionally.. 38.
(47) Chaper 5 Conclusion and Recommendations. In our study, the suppression of myositis and inducible expression of transduced gene were observed in a model of TPA induced extraocular myositis. The regulation of gene expression and other suppressive factors of myositis remain to be determined in further myositis experiments. So this study recommends that: 1. This gene therapy, by combining highly efficient and stable rAAV gene delivery, and the anti-inflammatory effect of IL-1Ra, provides a valuable approach for prevention of extraoculor myositis in this animal model. The effect of using rAAV-IL-1 Ra in the extraocular myositis of human is worth further study. 2. The result revealed the preventive effect of extraocular myositis by rAAV-IL-1 Ra. In this study, IL-1Ra gene has been delivered by adeno-associated virus vectors into muscular cells successfully. More anti-inflmmatory cytokines could be tried to be delivered into muscular cells in further studies. The anti-inflammation results by the different cytokines are expected.. 39.
(48) References Wegrowski J, Bellon G, Haye B, Borel JP. Effects of thyroid-stimulating hormone and phorbol ester on glycoaminoglycan synthesis in porcine thyroid epithelial cells in primary culture. Cell Biol Int Rep. 1989;13:881-890. Ludgate M, Starkey K. Prognosis in our understanding of the pathogenesis of Graves ophthalmopathy. Curr Ther Endocrinol Metab. 2000;7:270-274. Bahn RS, Heufelder AE. Pathogenesis of Graves’ ophthalmopathy. N Engl J Med. 1993;329:1468. Reed AM. Immunogenetic associations in childhood dermatomyositis. Curr Rheumatol Rep. 2000;2:212-215. Lumdberg IE. The role of cytokines, chemokines, and adhesion molecules in the pathogenesis of idiopathic inflammatory myopathies. Curr Rheumatol Reps. 2000;2:216-224. Natt N, Bahn RS. Cytokines in the evolutions of Graves’ ophthalmopathy. Autoimmunity. 1997;26:129-136. Bahn RS, Heufelder AE. Pathogenesis of Graves’ ophthalmopathy. N Engl J Med. 1993,329:1468. Arend WP. The balance between IL-1 and IL-1Ra in disease. Cytokine Growth Factor Rev. 2002;13:323-340. Fleischmann R, Stern R, I qbal I. Anakinra: an inhibitor of IL-1 for the treatment of rheumatoid arthritis. Expert Opin Biol Ther. 2004;4:1333-1344. Watchko J, O’day T, Wang B, Zhou L, Tang Y, Li J, Xiao X. Adeno-associated virus vector-mediated minidystropin gene therapy improves dystrophic muscle contractile function in mdx mice. Humen Gene therapy. 2002;13:1451-1460. Wang B, Li J, Xiao X. Adeno-associated virus vector carrying human minidystrophin genes effectively ameliorates muscular dystrophy in mdx mouse model. Proc Natl Acad Sci. 2000;97:13714-13719. Pruchnic R, Cao B, Peterson ZQ, Xiao X, Li J, Samulski RJ, Epperly M, Huard J. The use of 40.
(49) adeno-associated virus to circumvent the maturation-dependent viral transduction of muscle fibers. Humen Gene therapy. 2000;11:521-536. Takeda S. Current status and perspective of gene therapy on dystrophic animal model. Rinsho Shinkeigaku. 2004;44:911-913. Athanansopoulos T, Graham IR, Foster H, Dickson G. Recombinant adeno-associated viral (rAAV) vectors as therapeutic tools for Duchenne muscular dystrophy (DMD). Gene Ther 2004;11 Suppl 1;S109-121. Carter DB, Deibel MR, Dunn CJ, Tomich CS, Sun FF, McEwan RN. Purification, cloning, expression and biological characterization of an interleukin-1 receptor antagonist protein. Nature. 1990;344:633–638. Li J, Dressman D, Tsao YP, Sakamoto A, Hoffman EP, Xiao X. rAAV vector-mediated sarcoglycan gene transfer in a hamster model for limb girdle muscular dystrophy. Gene Ther. 1999;6:74–82. Xiao X, Li J, Samulski RJ. Production of high-titer recombinant adeno-associated virus vectors in the absence of helper adenovirus. J Virol. 1998;72:2224–2232. Xiao X, Li J, McCown TJ, Samulski RJ. Gene transfer by adeno-associated virus vectors into the central nervous system. Exp Neurol. 1997;144:113–124. Furst DE. Anakinra: review of recombinant human interleukin-I receptor antagonist in the treatment in the treatment of rheumatoid arthritis. Clin Ther. 2004;26:1960-1975. Arend WP, Malyak M, Smith MF, Whisenand TD, Slack JL, Sims JE, Giri JG, Dower SK. Binding of IL-1α, IL-1β and IL-1 receptor antagonist by soluble IL-1 receptors and levels of soluble IL-1 receptors in synovial fluids. J Immunol. 1994;153: 4766-4774. Son K, Tomita Y, Shimizu T, Nishinarita S, Sawada S, Horie T. Abnormal IL-1 receptor antagonist production in patients with polymyositis and dermatomyositis. Inter Med. 2000;39:128-135. Muhlberg T, Joba W, Spitzweg C. Interleukin-1 receptor antagonist ribonucleic acid and protein expression by cultured Graves’ and normal orbital fibroblasts is differentially modulated by dexamethasone and irradiation, J Clin Endocrinal Metab. 2000;85:734-742. 41.
(50) Pan RY, Chen SL, Xiao X, Liu DW, Peng HJ, Tsao YP. Therapy and prevention of arthritis by recombinant adeno-associated virus vector with delivery of interleukin-1 receptor antagonist. Arthritis & Rheumatism. 2000;43:289–297. Fries PD, Fohrman DS, Char DH Phorbol ester-induced orbital myositis. Arch Ophthalmol. 1987;105:1273-1276. Conlon TJ, Floatte TR. Recombinant adeno-associated virus vectors for gene therapy. Expert Opin Biol Ther. 2004;4:1093-1101. Colotta, F., Re, F., Muzio, M., Bertini, R., Polentarutti, N., Sironi, N., Giri, J.G., Dower, S.K., Sims, J.E.,Mantovani, A., 1993. Interleukin-1 type II receptor: a decoy target for IL-1 that is regulated by IL-4. Science 261, 472–475. Cominelli, F., Bortolami, M., Pizarro, T.T., Monsacchi, L., Ferretti, M., Brewer, M.T., Eisenberg, S.P., Ng, R.K., 1994. Rabbit interleukin-1 receptor antagonist. Cloning, expression, functional characterization, and regulation during intestinal inflammation. J. Biol. Chem. 269, 6962–6971. Dinarello, C.A., 1991. Interleukin-1 and interleukin-1 antagonism. Blood 77, 1627–1652. Dinarello, C.A., Thompson, R.C., 1991. Blocking IL-1: interleukin 1 receptor antagonist in vivo and in vitro.Immunol. Today 12, 404–410. Eisenberg, S.P., Evans, R.J., Arend, W.P., Verderber, E., Brewer, M.T., Hannum, C.H., Thompson, R.C.,1990. Primary structure and functional expression from complementary DNA of a human interleukin-1 receptor antagonist. Nature 343, 341–346. Eisenberg, S.P., Brewer, M.T., Verderber, E., Heimdal, P., Brandhuber, B.J., Thompson, R.C., 1991. Interleukin 1 receptor antagonist is a member of the interleukin 1 gene family: evolution of a cytokine control mechanism. Proc. Natl. Acad. Sci. U.S.A. 88, 5232–5236. Evans, R.J., Bray, J., Childs, J.D., Vigers, G.P.A., Brandhuber, B.J., Skalicky, J.J., Thompson, R.C., Eisenberg, S.P., 1995. Mapping receptor binding sites in interleukin _IL.-1 receptor antagonist and IL-1b by site-directed mutagenesis. J. Biol. Chem. 270, 11477–11483.. 42.
(51) Ferretti, M., Casini-Raggi, V., Pizarro, T.T., Eisenberg, S.P., Nast, C.C., Cominelli, F., 1994. Neutralization of endogenous IL-1 receptor antagonist exacerbates and prolongs inflammation in rabbit immune colitis. J. Clin. Invest. 94, 449–453. Fisher, E., Van Zee, K.J., Marano, M.A., Rock, C.S., Kenney, J.S., Poutsiaka, D.D., Dinarello, C.A., Lowry, S.F., Moldawer, L.L., 1992. Interleukin-1 receptor antagonist circulates in experimental inflammation and in human disease. Blood 79, 2196–2200. Goto, F., Goto, K., Miyata, T., Ohkawara, S., Takao, T., Mori, S., Furukawa, S., Maeda, T., Iwanaga, S., Shimonishi, Y., Yoshinaga, M., 1992. Interleukin-1 receptor antagonist in inflammatory exudate cells of rabbits. Production, purification and determination of primary structure. Immunology 77, 235–244. Goto, M., Kirisawa, R., Tajima, M., Takahashi, K., Iwai, H., 1995. A bioassay for bovine interleukin-1 by the A375 cell growth inhibition. J. Vet. Med. Sci. 57, 523–525. Goto, M., Maruyama, M., Kitadate, K., Kirisawa, R., Obata, Y., Koiwa, M., Iwai, H., 1997. Detection of interleukin-1b in sera and colostrum of dairy cattle and in sera of neonates. J. Vet. Med. Sci. 59, 437–441. Granowitz, E.V., Santos, A.A., Poutsiaka, D.D., Cannon, J.G., Wilmore, D.W., Wolf, S.M., Dinarello, C.A., 1991. Production of interleukin-1 receptor antagonist during experimental endotoxaemia. Lancet 338, 1423–1424. Hannum, C.H., Wilcox, C.J., Arend, W.P., Joslin, F.G., Dripps, D.J., Heimdal, P.L., Armes, L.G., Sommer, A., Eisenberg, S.P., Thompson, R.C., 1990. Interleukin-1 receptor antagonist activity of a human interleukin-1 inhibitor. Nature 343, 336–340. Haskill, S., Martin, G., Van Le, L., Morris, J., Peace, A., Bigler, C.F., Jaffe, G.J., Hammerberg, C., Sporn, S.A., Fong, S., Arend, W.P., 1991. cDNA cloning of an intracellular form of the human interleukin-1 receptor antagonist associated with epithelium. Proc. Natl. Acad. Sci. U.S.A. 88, 3681–3685. Jenkins, J.K., Arend, W.P., 1993. Interleukin-1 receptor antagonist production in human monocytes is induced by IL-1a, IL-3, IL-4 and GM-CSF. Cytokine 5, 407–415. Kato, H., Ohashi, T., Matsushiro, H., Watari, T., Goitsuka, R., Tsujimoto, H., Hasegawa, A., 1997. Molecular cloning and functional expression of equine interleukin-1 receptor 43.
(52) antagonist. Vet. Immunol. Immunopathol. 56, 221–231. Sample, A.K., Czuprynski, C.J., 1994. Bovine neutrophil chemiluminescence is preferentially stimulated by homologous IL-1, but inhibited by the human IL-1 receptor antagonist. Vet. Immunol. Immunopathol. 41, 165–172. Schreuder, H.A., Rondeau, J.M., Tardif, C., Soffientini, A., Sarubbi, E., Akeson, A., Bowlin, T.L., Yanofsky, S., Barrett, R.W., 1995a. Refined crystal structure of the interleukin-1 receptor antagonist. Presence of a disulfide link and a cis-proline. Eur. J. Biochem. 227, 838–847. Schreuder, H., Tardif, C., Soffientini, A., Sarubbi, E., Akeson, A., Bowlin, T., Yanofsky, S., Barrett, R.W., 1995b. Crystals of soluble interleukin-1 receptor complexed with its natural antagonist reveal a 1:1 receptor–ligand complex. FEBS Lett. 373, 39–40. Shuster, D.E., Kehrli, M.E., 1995. Administration of recombinant human interleukin 1 receptor antagonist during endotoxin-induced mastitis in cows. Am. J. Vet. Res. 56, 313–320.. 44.
(53)
數據

+4

相關文件
Reading Task 6: Genre Structure and Language Features. • Now let’s look at how language features (e.g. sentence patterns) are connected to the structure
好了既然 Z[x] 中的 ideal 不一定是 principle ideal 那麼我們就不能學 Proposition 7.2.11 的方法得到 Z[x] 中的 irreducible element 就是 prime element 了..
volume suppressed mass: (TeV) 2 /M P ∼ 10 −4 eV → mm range can be experimentally tested for any number of extra dimensions - Light U(1) gauge bosons: no derivative couplings. =>
For pedagogical purposes, let us start consideration from a simple one-dimensional (1D) system, where electrons are confined to a chain parallel to the x axis. As it is well known
The observed small neutrino masses strongly suggest the presence of super heavy Majorana neutrinos N. Out-of-thermal equilibrium processes may be easily realized around the
incapable to extract any quantities from QCD, nor to tackle the most interesting physics, namely, the spontaneously chiral symmetry breaking and the color confinement..
(1) Determine a hypersurface on which matching condition is given.. (2) Determine a
• Formation of massive primordial stars as origin of objects in the early universe. • Supernova explosions might be visible to the most
