Effective Reduction of Gastric Cancer Risk With Regular
Use of Nonsteroidal Anti-Inflammatory Drugs in
Helicobacter Pylori–Infected Patients
Chun-Ying Wu, Ming-Shiang Wu, Ken N. Kuo, Chang-Bi Wang, Yi-Ju Chen, and Jaw-Town Lin From the Division of Gastroenterology,
Taichung Veterans General Hospital; College of Public Health, China Medical University, Taichung; Faculty of Medi-cine, School of MediMedi-cine, National Yang-Ming University; Division of Gastroenterology, National Taiwan University Hospital, Taipei; Center for Health Policy Research and Develop-ment, National Health Research Insti-tutes, Miaoli; and the E-Da Hospital and I-Shou University, Kaohsiung County, Taiwan.
Submitted September 8, 2009; accepted March 11, 2010; published online ahead of print at www.jco.org on May 17, 2010.
Supported by Grant No. PH-098-PP-26 from Taiwan’s National Health Research Institutes.
C.-Y.W. and J.-T.L. contributed equally to this work.
Authors’ disclosures of potential con-flicts of interest and author contribu-tions are found at the end of this article.
Corresponding author: Jaw-Town Lin, MD, PhD, Department of Internal Medicine, E-Da Hospital and I-Shou University, No.1, E-Da Rd., Jiau-Shu Tsuen, Yan-Chau Shiang, Kaohsiung County 824, Taiwan; e-mail: [email protected].
© 2010 by American Society of Clinical Oncology
0732-183X/10/2818-2952/$20.00 DOI: 10.1200/JCO.2009.26.0695
A B S T R A C T
Purpose
Nonsteroidal anti-inflammatory drugs (NSAIDs) play protective roles in gastric carcinogenesis. However, the interaction between NSAIDs and Helicobacter pylori (H pylori) infection and the number needed to treat to prevent gastric cancer remains unclear.
Patients and Methods
We conducted a nationwide retrospective cohort study based on data from the Taiwan National Health Insurance Database. Hospitalized patients with a primary diagnosis of peptic ulcer disease were selected. Overall, 52,161 patients were divided into non-NSAID user and regular NSAID user cohorts. Standardized incidence ratios (SIRs), cumulative incidences, and hazard ratios (HRs) were calculated.
Results
Patients with peptic ulcers who never used NSAIDs had higher risk of gastric cancer compared with the general population (SIR, 2.11; 95% CI, 2.07 to 2.15), but regular NSAID use conferred lower risk (SIR, 0.79; 95% CI, 0.77 to 0.81). The protective role of NSAID use was observed in patients with gastric ulcer, but not in patients with non–H pylori-associated duodenal ulcer. On multivariate analysis, regular NSAID use was an independent protective factor for gastric cancer development (HR, 0.79 for each incremental year; P ⬍ .001), especially in H pylori-associated patients (HR, 0.52 for each incremental year; P⬍ .001). Among patients with H pylori-infected gastric ulcers, the NNT to prevent a gastric cancer was 50.
Conclusion
Regular NSAID use may be a feasible way to prevent gastric cancer, at least in patients with gastric ulcers, and especially in H pylori-infected subjects.
J Clin Oncol 28:2952-2957. © 2010 by American Society of Clinical Oncology
INTRODUCTION
Despite the declining trend in both incidence and mortality worldwide, gastric cancer remains the fourth most common cancer and the second lead-ing cause of cancer mortality.1Gastric carcinogen-esis is a multifactorial process, involving complex interactions between host and environmental fac-tors. Among these factors, chronic inflammation plays an important role in the development of gas-tric cancer.2,3 Inflammation-induced injury may compromise tissue integrity and drive the multi-stage process of carcinogenesis by altering targets and pathways crucial to normal tissue homeostasis.4 In addition, inflammatory conditions stimulate the formation and expansion of blood and lymphatic vessels within tumor, thus promoting tumor growth and invasion.5A prime example is Helicobacter
py-lori (H pypy-lori) infection, which has been known to
induce chronic gastric inflammation that leads to atrophy, metaplasia, dysplasia, and gastric cancer.2,6 After eradicating H pylori, precancerous lesions may regress.7,8Testing and treating for the H
py-lori infection earlier rather than later in life is
sug-gested to be the more beneficial approach.9In our recent population-based study, early H pylori eradi-cation was found to be associated with decreased risk of gastric cancer.10
Elucidation of inflammation-based carcino-genesis offers new opportunities for gastric cancer chemoprevention.11Aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) have been suggested to prevent gastric cancer by inhibiting production of cyclooxygenase (COX) -1 and COX-2 through both prostaglandin-dependent and -independent pathways.12In a meta-analysis pooling of the results of clinical studies, NSAID use was found to be asso-ciated with a reduced risk of gastric cancer, with
similar magnitudes of risk reduction for aspirin and nonaspirin NSAID users. Regular users of NSAIDs were found to have a lower risk of gastric cancer compared with nonusers and irregular users.13 An-other meta-analysis also reported similar protective effect of NSAIDs in gastric cancer.14
Previous studies have provided important evidence of the protective roles of NSAIDs in gastric carcinogenesis. However, the interaction between NSAID use and H pylori infection and the subpopulation for which benefits of chemoprevention outweigh the risks gastrointestinal bleeding and the number needed to treat (NNT) remain unclear.11,13
PATIENTS AND METHODS
Study Population
In this population-based retrospective cohort study, data were obtained from Taiwan’s National Health Insurance Research Database (NHIRD). The NHIRD has been described in detail in our previous study.10,15In brief, this database consists of health care data from more than 99% of the entire popu-lation of 23.72 million and comprises comprehensive health care informa-tion.15,16International Classification of Diseases-9 codes were used to define diseases. Gastric cancer diagnosis was defined according to the Registry for Catastrophic Illness Patient Database, which is a separate subpart of the NHIRD. Histological confirmation is required for the diagnosis of gastric cancer to be entered into this registry. This study has been approved by the National Health Research Institutes.
Study Subjects
From this database, we selected patients who were admitted to a hospital for the first time between January 1, 1998, and December 31, 2004, with a primary diagnosis of peptic ulcer disease (International Classification of Diseases-9 codes: 531, 532, and 533 for gastric ulcer, duodenal ulcer, and nonspecific peptic ulcer, respectively). Patients younger than 20 years and those with previous gastric cancer were excluded. Patients who underwent gastric resection or vagotomy before index hospitalization discharge were also excluded. Comorbidities were defined as diseases diagnosed on previous ad-mission before the index hospitalization.
Gastric Cancer Risk Analysis
The observation period started on the discharge day of the index hospi-talization until the end of 2006, death, or development of gastric cancer. The selected patients were divided into two cohorts according to their NSAID exposure status. Since gastric cancer developing in the first 2 years of the index hospitalization is difficult to differentiate from gastric cancer mimicking gas-tric ulcer, we excluded patients with a diagnosis of gasgas-tric cancer registered in this period. Each subject was observed for a minimum of 2 years and a maximum of 9 years. Standardized incidence ratios (SIRs), cumulative incidences, and hazards ratios (HRs) of gastric cancer were analyzed. To exclude the potential influence of competitive mortality, we also analyzed cumulative incidence of gastric cancer by excluding patients who died during the observation period.
Exposure to Aspirin and NSAIDs
NHIRD contains details of every prescription for nearly entire popula-tion of Taiwan between 1997 through 2006, including dose, frequency, starting and ending days, and administration routes. All information on aspirin and NSAID use for individual patients was obtained from NHIRD. NSAIDs in-cluded high-dose aspirin (⬎ 100 mg/d), low-dose aspirin (50 to 100 mg/d), COX-2 specific inhibitors, and traditional NSAIDs (excluding COX-2 specific inhibitors). All analyzed NSAIDs are shown in Appendix Table A1 (online only). During the observation period, patients taking NSAIDs regularly (more than 28 days monthly) and continuously for more than 6 months were defined as regular NSAID users. Non-NSAID users were defined as those who had not used NSAIDs during the observation period. Because NSAID use changes after the index hospitalization, we also analyzed the results by treating NSAID use as a time-dependent covariate.17
H pylori-Associated Peptic Ulcer
Those who received H pylori eradication therapy were defined as H pylori-associated peptic ulcer patients. H pylori eradication was defined as proton pump inhibitor (PPI) or H2 receptor antagonist (H2RA), plus clarithromycin or metro-nidazole, plus amoxicillin or tetracycline, with or without bismuth (details of all eligible H pylori eradication regimens are shown in Appendix Table A2, online only). These drug combinations were prescribed within the same pre-scription order and the duration of therapy was between 7 and 14 days.
Statistical Analysis
To compare the risk of gastric cancer with the age- and sex-matched general population, SIR was calculated. The SIR was defined as the ratio of the observed to the expected gastric cancer incidences in the two cohorts. The expected incidence of cancer was calculated by adding up all person-time
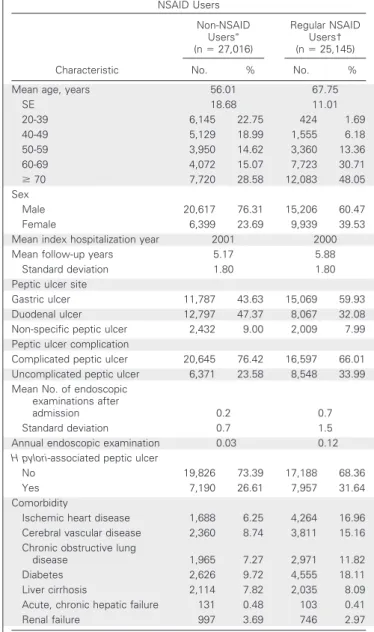
Table 1. Baseline Characteristics of Non-NSAID Users and Regular NSAID Users Characteristic Non-NSAID Usersⴱ (n⫽ 27,016) Regular NSAID Users† (n⫽ 25,145) No. % No. %
Mean age, years 56.01 67.75
SE 18.68 11.01 20-39 6,145 22.75 424 1.69 40-49 5,129 18.99 1,555 6.18 50-59 3,950 14.62 3,360 13.36 60-69 4,072 15.07 7,723 30.71 ⱖ 70 7,720 28.58 12,083 48.05 Sex Male 20,617 76.31 15,206 60.47 Female 6,399 23.69 9,939 39.53 Mean index hospitalization year 2001 2000 Mean follow-up years 5.17 5.88 Standard deviation 1.80 1.80 Peptic ulcer site
Gastric ulcer 11,787 43.63 15,069 59.93 Duodenal ulcer 12,797 47.37 8,067 32.08 Non-specific peptic ulcer 2,432 9.00 2,009 7.99 Peptic ulcer complication
Complicated peptic ulcer 20,645 76.42 16,597 66.01 Uncomplicated peptic ulcer 6,371 23.58 8,548 33.99 Mean No. of endoscopic
examinations after
admission 0.2 0.7
Standard deviation 0.7 1.5 Annual endoscopic examination 0.03 0.12
H pylori-associated peptic ulcer
No 19,826 73.39 17,188 68.36 Yes 7,190 26.61 7,957 31.64 Comorbidity
Ischemic heart disease 1,688 6.25 4,264 16.96 Cerebral vascular disease 2,360 8.74 3,811 15.16 Chronic obstructive lung
disease 1,965 7.27 2,971 11.82 Diabetes 2,626 9.72 4,555 18.11 Liver cirrhosis 2,114 7.82 2,035 8.09 Acute, chronic hepatic failure 131 0.48 103 0.41 Renal failure 997 3.69 746 2.97 Abbreviations: NSAID, nonsteroidal anti-inflammatory drug; H pylori,
Helico-bacter pylori.
ⴱPatients who did not take NSAIDs or aspirin were defined as
non-NSAID users.
†Patients who took NSAIDs or aspirin regularly (longer than 28 days monthly) and continuously for more than 6 months were defined as regular NSAID users.
experienced in the cohort divided into strata by age (in 10-year gradient intervals) andsex,andthenmultiplyingthestratum-specificperson-timebythecorrespond-ing stratum-specific incidence rates of the entire Taiwan population. The popula-tion of each age and sex strata and the corresponding stratum-specific incidence rates of gastric cancer for the entire Taiwan population were based on the popula-tion census in 2001 and cancer registry data in 2001, respectively.
Since cumulative incidence by log-rank analysis may be incorrectly esti-mated in the presence of competing risks, we directly model the cumulative incidences by a semiparametric proportional hazards model suggested by Fine and Gray.18,19The cumulative incidence is estimated in a two-step process to account for the informative nature censoring due to competing risk.20,21HRs were calculated using the Cox proportional hazards model, adjusted by the partial likelihood principle and weighting techniques.19The assumption of proportional hazards was confirmed by plotting the graph of the survival function versus the survival time and the graph of the log(⫺log(survival)) versus log of survival time. Variables in the model included age, sex, peptic ulcer site, peptic ulcer complications, NSAID use, and H pylori eradication. We also fit the model with interaction term between NSAID use and H pylori infection. Assess-ment of goodness-of-fit of the models with step-down method was used to analyze the independent prognostic factors. All data management and analyses were per-formed using SAS version 9.1 (SAS Institute, Cary, NC).
RESULTS
Demographic Data
Among the 52,161 subjects who were admitted for the first time with a primary diagnosis of peptic ulcer disease between 1998 and
2004, 27,016 were selected into the non-NSAID users group; 25,145 patients were defined as regular NSAID users. The average durations of follow-up for non-NSAID users and regular NSAID users were 5.17 and 5.88 years, respectively. Other demographic data, including age, sex, peptic ulcer site, with or without complications, numbers of endoscopic examinations, H pylori eradication, and comorbidities, are presented in Table 1.
SIRs of Gastric Cancer
Patients with peptic ulcers who did not use NSAIDs had signifi-cantly higher risk of gastric cancer compared with the general popu-lation (SIR, 2.11; 95% CI, 2.07 to 2.15), but those with regular NSAID use showed significantly lower risk of gastric cancer compared with the general population (SIR, 0.79; 95% CI, 0.77 to 0.81). On stratified analysis, non-NSAID users had significantly higher risks of gastric cancer in nearly all stratified groups compared with the general pop-ulation. In contrast, regular NSAID users were associated with re-duced risk of gastric cancer for all stratified groups compared with the general population except for patients of female sex, with gastric ulcer and non-H pylori-associated gastric ulcer (Table 2).
Among patients with gastric ulcers, SIRs were 6.79 and 0.86 for H pylori-positive NSAID nonusers and regular users, respec-tively; 2.53 and 1.06 for H pylori-negative NSAID nonusers and regular users, respectively. For patients with duodenal ulcers, SIRs were 2.01 and 0.33 for H pylori-positive NSAID nonusers and regular
Table 2. Risk of Gastric Cancer for Non-NSAID Users and Regular NSAID Users
Variable
Non-NSAID Users (n⫽ 27,016) Regular NSAID Users (n⫽ 25,145)
GCAⴱ(No.) EXP† (No.) SIR‡ 95% CI GCAⴱ(No.) EXP† (No.) SIR‡ 95% CI Total 103 48.8 2.11 2.07 to 2.15 69 87.0 0.79 0.77 to 0.81 Age, years ⬍ 70 60 13.8 4.36 4.25 to 4.47 21 22.8 0.92 0.88 to 0.96 ⱖ 70 43 33.5 1.29 1.25 to 1.32 48 60.0 0.80 0.78 to 0.82 Sex Male 77 40.1 1.92 1.88 to 1.96 46 67.0 0.69 0.67 to 0.71 Female 26 8.9 2.93 2.82 to 3.05 23 20.3 1.13 1.08 to 1.18 Peptic ulcer site
Gastric 77 23.9 3.22 3.15 to 3.29 51 51.0 1.00 0.97 to 1.03 Duodenal 26 24.5 1.06 1.02 to 1.10 18 35.9 0.50 0.48 to 0.52 Ulcer complication Complicated 77 39.6 1.94 1.90 to 1.99 47 58.4 0.80 0.78 to 0.83 Noncomplicated 26 9.3 2.80 2.70 to 2.91 22 28.6 0.77 0.74 to 0.80 H pylori associated No 66 39.4 1.67 1.63 to 1.71 52 59.6 0.87 0.85 to 0.90 Yes 37 9.4 3.92 3.79 to 4.05 17 27.3 0.62 0.59 to 0.65 Gastric ulcer H pylori positive 26 3.8 6.79 6.53 to 7.05 13 15.2 0.86 0.81 to 0.90 H pylori negative 51 20.1 2.53 2.46 to 2.60 38 35.8 1.06 1.03 to 1.10 DU H pylori positive 11 5.5 2.01 1.89 to 2.12 4 12.1 0.33 0.30 to 0.36 H pylori negative 15 19.1 0.79 0.75 to 0.83 14 23.8 0.59 0.56 to 0.62
NOTE. The standardized incidence ratios after the second year of follow-up for non-NSAID users and regular NSAID users according to different demographic and ulcer characteristics.
Abbreviations: NSAID, nonsteroidal anti-inflammatory drug; GCA, gastric cancer; EXP, expected; SIR, standardized incidence rate; DU, duodenal ulcer; H pylori,
Helicobacter pylori.
ⴱNo. of patients with gastric cancer observed in each stratified group.
†No. of patients with gastric cancer expected in each stratified group according to the age- and sex-specific gastric cancer risk.
‡SIR was defined as the ratio of the observed to the expected gastric cancer incidences in the two cohorts. The expected incidence of cancer was calculated by adding up all person-time experienced in the cohort divided into strata by age (in 10-year gradient intervals) and sex, and then multiplying the stratum-specific person-time by the corresponding stratum-specific incidence rates of the entire Taiwan population.
users, respectively; 0.79 and 0.59 for H pylori-negative nonusers and regular users, respectively (Table 2).
Cumulative Incidences of Gastric Cancer
The cumulative incidence of gastric cancer in these 7 years for non-NSAID users was significantly higher than the cumulative inci-dence for regular NSAID users (6.4% v 4.7%; P⫽ .0051; Fig 1). The NNT to prevent a gastric cancer development in peptic ulcer patients was 589. Life expectancy in Taiwan in 2006 was 74.86 and 81.41 years for male and female, respectively. Overall, 7,693 people died without developing gastric cancer.
On stratified analysis, we observed the protective role of NSAIDs in gastric cancer in patients with gastric ulcer (cumulative incidence in 7 years: 11.6% for non-NSAID users versus 6.2% for regular NSAID users; P⬍ .001), but not in patients with duodenal ulcer. Among patients with gastric ulcers, the NNT to prevent a gastric cancer was 186. Also among patients with gastric ulcers, regular NSAID use had stronger prophylactic effect against gastric cancer development in H
pylori-associated patients (cumulative incidence in 7 years: 25.2% for
non-NSAID users v 5.0% for regular NSAID users; P⬍ .001) than in non-H pylori-associated patients (8.7% for non-NSAID users v 6.7% for regular NSAID users; P⫽ .0169). For H pylori-associated and noninfected gastric ulcer patients the NNTs to prevent a gastric cancer were 50 and 500, respectively (Appendix Fig A1, online only). Gastrointestinal Risk of NSAID Use
During the observation period, the annual incidences of read-mission due to peptic ulcer diseases were 0.09 and 0.05 for regular and non-NSAID users, respectively. For each hospitalization, the mean numbers of admission days for regular and non-NSAID users were 7.38 and 7.92, respectively. Consistent with the higher gastrointestinal
risk in regular NSAID users, more PPIs and H2Rs were prescribed for regular NSAID users when compared with non-NSAID users. Multivariate Analysis
On Cox multivariate proportional hazards analysis, older age (HR, 1.03 for each incremental year; P⬍ .001), gastric ulcer (HR, 2.85;
P⬍ .001), and H pylori-associated peptic ulcer (HR, 1.93; P ⬍ .001)
were independent risk factors for gastric cancer development. Regular NSAID use was independently associated with lower risk of gastric cancer (HR, 0.79 for each incremental year; P⬍ .005). Patients with both regular NSAID use (each incremental year) and positive H pylori status were associated with even lower risk of gastric cancer (HR, 0.69;
P ⬍ .001; Table 3). Among H pylori-associated patients, regular
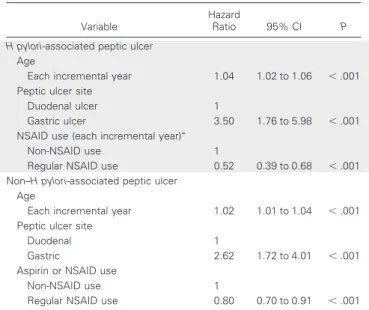
NSAID use was associated with significantly lower risk of gastric can-cer (HR, 0.52 for each incremental year; P⬍ .001). For those never receiving H pylori eradication therapy, regular NSAID use was also associated with reduced risk of gastric cancer (HR, 0.80 for each incremental year; P⬍ .001; Table 4).
DISCUSSION
This study was based on patients admitted to a hospital for the first time with a primary diagnosis of peptic ulcer disease. There are several reasons for choosing patients hospitalized for peptic ulcers as the study population. First, nearly all patients received endoscopic examination during the admission, which is helpful in confirming that these pa-tients were free from gastric cancer at the time of recruitment. Second, among patients with peptic ulcer diseases, a high proportion receive regular NSAIDs and H pylori eradication therapy simultaneously, which provides an excellent cohort to investigate the interaction be-tween NSAID use and H pylori infection in the development of gastric cancer. Third, the relative risks of gastric cancer compared with the general population were reported to be 1.8 and 0.6 for patients with gastric and duodenal ulcers, respectively.22There is an opportunity to examine how NSAID use differentially alters the risk of gastric cancer among patients with gastric or duodenal ulcer.
P = .0051 Death
Non-NSAIDs users Regular NSAIDs users
7 6 5 4 3 2 1 0 2 3 1 4 5 6 7 8 9
Cumulative Incidence of Gastric Cancer (%)
Follow-Up Time (years) 300
200
100
Fig 1. Cumulative incidences of gastric cancer and competing risk. The gold and blue lines show the cumulative incidences of gastric cancer for non–nonsteroidal anti-inflammatory drug (NSAID) users and regular users, respectively, after adjusting for competing risk. The gray line shows the cumulative incidence of the competing risk (ie, death as a result of causes other than gastric cancer). The cumulative incidences of gastric cancer for non-NSAID users were significantly higher than for regular NSAID users (P⬍ .001).
Table 3. Multivariate Cox Proportional Hazards Model Analysis for Prediction of Occurrence of Gastric Cancer
Variable
Hazard
Ratio 95% CI P
Age
Each incremental year 1.03 1.02 to 1.04 ⬍ .001 Peptic ulcer site
Duodenal 1
Gastric 2.85 2.01 to 4.03 ⬍ .001
H pylori-associated peptic ulcer
Not 1
Yes 1.93 1.29 to 2.88 ⬍ .001 NSAID use (each incremental year)ⴱ
Non-NSAID user 1
Regular NSAID user 0.79 0.69 to 0.90 ⬍ .001 NSAID use and H pylori interactionⴱ
Other 1
Both regular NSAID use and H pylori 0.69 0.51 to 0.93 ⬍ .001 Abbreviations: NSAID, nonsteroidal anti-inflammatory drug; H pylori,
Helico-bacter pylori.
The roles of aspirin and NSAIDs in chemoprevention of gastro-intestinal tumors have been widely discussed. In a meta-analysis re-viewing epidemiologic studies, NSAID use was associated with a reduced risk of gastric cancer, with a summary odds ratio of 0.78.13In comparisons with non-NSAID users, regular NSAID users had a lower risk of gastric cancer than that of irregular NSAID users (odds ratio, 0.57 v 0.76 for regular and irregular users, respectively). The protective effect of NSAID use was only observed in patients with noncardia gastric cancer.13In Taiwan, noncardia gastric cancer com-prises 86% of all gastric cancers.23Another meta-analysis reported similar results with relative risks of 0.73 and 0.54 for aspirin use and NSAID use, respectively.14 In a recent study, NSAID users had a reduced risk of gastric cancer (odds ratio, 0.65).24These observations were compatible with our results in this study (HR, 0.79 for each incremental year).
In the cumulative incidence analysis, we found NSAIDs only decreased the risk of gastric cancer in those with gastric ulcer, but not in those with duodenal ulcer. The reason the risk of gastric cancer in those with duodenal ulcer was not significantly reduced was because the absolute risk was quite low to start with. This explanation was supported by the observation in this study that regular NSAID use actually significantly decreased the risk of gastric cancer in those in-fected with H pylori, but not in those without H pylori infection.
NSAIDs inhibit the replication and proliferation of H pylori and potentially increase H pylori clearance.25 NSAIDs also attenuate COX-2 expression and prostaglandin synthesis stimulated by H pylori, thus reducing the risk of H pylori-related gastric cancer.26,27But how H
pylori infection impacts the chemopreventive effect of NSAID use
remains unclear.28,29In a case-control study, NSAID use was found to be associated with a reduced risk of gastric cancer, but this prophylac-tic effect was not found in noninfected subjects.28In a Swedish study, NSAID use was associated with 40% and 20% gastric cancer risk
reductions among H pylori-positive and H pylori-negative subjects, respectively.29In this study, regular NSAID use for each incremental year was found to be associated with 48% and 20% gastric risk reduc-tion among H pylori-positive and H pylori-negative patients with peptic ulcer.
In this study, we defined the time frame for assessing NSAID exposure starting on the discharge day of the index hospitalization until the end of 2006, death, or development of gastric cancer. We also analyzed the relative risk of gastric cancer by limiting the time frame in the first 2 years after the index hospitalization. Patients taking NSAIDs regularly (more than 28 days monthly) and continuously for more than 6 months in the first 2 years after the index hospitalization were defined as regular NSAID users. Since patients tended to avoid NSAIDs after the index hospitalization and the shorter observation period, the number of regular NSAID users decreased from 25,145 to 8,749 after limiting the time frame to 2 years after the index hospital-ization. However, regular NSAID use was still associated with de-creased risk of gastric cancer after adjusting age, peptic ulcer site, and
H pylori status (HR, 0.49; P⫽ .021; Appendix Table A3, online only).
The gastrointestinal safety of NSAIDs in patients with peptic ulcer history is a major concern. In a meta-analysis of 24 randomized controlled trials, gastrointestinal bleeding was found to occur in 2.47% patients taking aspirin regularly compared with 1.42% taking placebo based on an average of 28 months’ therapy.30In another meta-analysis regarding the risk of endoscopic ulcers on treatment with NSAIDs, increasing age was found to be associated with both more frequent and more serious NSAIDs gastropathy.31In this study, the annual incidences of readmission due to peptic ulcer diseases were 9% and 5% for regular and non-NSAID users, respectively. Whether the chemopreventive effect of NSAIDs is offset by the increased gas-trointestinal complications depends on the risk of gastric cancer of the target populations.
Even if the risk-benefit profile for gastric cancer prevention can be justified, the role of NSAIDs as a measure to prevent gastric cancer development may be challenged by the large number of subjects need-ing treatment. A better approach is to apply the chemoprevention only to patients highly susceptible to gastric cancer. Age, lifestyle, diet, environment, family history, and genetic factors all contribute to identifying individuals with high risk of gastric cancer. In this study, gastric ulcer and H pylori were identified as independent risk factors. The enhanced prophylactic effect of NSAIDs in high-risk population was reflected by the decreasing NNT from 589 for all peptic ulcer patients to 50 for patients with H pylori-associated gastric ulcer. Fur-ther studies are needed to improve the identification of individuals highly susceptible to gastric cancer for implementation of chemopre-ventive strategies.
There are several limitations to this study. First, our results were based on hospitalized patients with peptic ulcer diseases. Selection biases may exist, and caution must be taken in extrapolating our results. Second, we defined patients who received H pylori eradication therapy as patients with H pylori-associated peptic ulcer. Some pa-tients may be H pylori infected, but not given anti–H pylori therapy and thus may be inappropriately classified into the non–H pylori-associated group. Since H pylori infection increases the risk of gastric cancer, this misclassification would not bias the results. Third, regular NSAID users were significantly older with more comorbidities than non-NSAID users. However, older age in the regular NSAID user group should contribute to a higher incidence of gastric cancer, and to Table 4. Multivariate Analysis for Prediction of Gastric Cancer Development
According to H pylori Status
Variable
Hazard
Ratio 95% CI P H pylori-associated peptic ulcer
Age
Each incremental year 1.04 1.02 to 1.06 ⬍ .001 Peptic ulcer site
Duodenal ulcer 1
Gastric ulcer 3.50 1.76 to 5.98 ⬍ .001 NSAID use (each incremental year)ⴱ
Non-NSAID use 1
Regular NSAID use 0.52 0.39 to 0.68 ⬍ .001 Non–H pylori-associated peptic ulcer
Age
Each incremental year 1.02 1.01 to 1.04 ⬍ .001 Peptic ulcer site
Duodenal 1
Gastric 2.62 1.72 to 4.01 ⬍ .001 Aspirin or NSAID use
Non-NSAID use 1
Regular NSAID use 0.80 0.70 to 0.91 ⬍ .001 Abbreviations: NSAID, nonsteroidal anti-inflammatory drug; H pylori,
Helico-bacter pylori.
a less significant difference between regular and non-NSAID users. Fourth, although we have conducted multivariate analysis to examine whether NSAID use is an independent protective factor, many factors are not available for adjustment, such as precancerous lesions, and environmental factors, and so on.
In conclusion, our observations provide further support that NSAID use may be a feasible way to prevent gastric cancer, at least in patients with gastric ulcers, and especially in H pylori-infected subjects.
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
The author(s) indicated no potential conflicts of interest.
AUTHOR CONTRIBUTIONS
Conception and design: Chun-Ying Wu, Ming-Shiang Wu, Ken N. Kuo,
Chang-Bi Wang, Yi-Ju Chen, Jaw-Town Lin
Financial support: Ken N. Kuo
Administrative support: Ken N. Kuo, Yi-Ju Chen, Jaw-Town Lin Provision of study materials or patients: Ken N. Kuo
Collection and assembly of data: Chun-Ying Wu, Chang-Bi Wang Data analysis and interpretation: Chun-Ying Wu, Ming-Shiang Wu,
Chang-Bi Wang, Jaw-Town Lin
Manuscript writing: Chun-Ying Wu, Jaw-Town Lin
Final approval of manuscript: Chun-Ying Wu, Ming-Shiang Wu, Ken
N. Kuo, Chang-Bi Wang, Yi-Ju Chen, Jaw-Town Lin
REFERENCES
1. Parkin DM, Pisani P, Ferlay J: Global cancer statistics. CA Cancer J Clin 49:33-64, 1999
2. Fox JG, Wang TC: Inflammation, atrophy, and gastric cancer. J Clin Invest 117:60-69, 2007
3. Wu MS, Chen CJ, Lin JT: Host-environment interactions: Their impact on progression from gas-tric inflammation to carcinogenesis and on develop-ment of new approaches to prevent and treat gastric cancer. Cancer Epidemiol Biomarkers Prev 14:1878-1882, 2005
4. Coussens LM, Werb Z: Inflammation and cancer. Nature 420:860-867, 2002
5. Zumsteg A, Christofori G: Corrupt policemen: Inflammatory cells promote tumor angiogenesis. Curr Opin Oncol 21:60-70, 2009
6. Amieva MR, El-Omar EM: Host-bacterial in-teractions in Helicobacter pylori infection. Gastroen-terology 134:306-323, 2008
7. Leung WK, Lin SR, Ching JY, et al: Factors predicting progression of gastric intestinal metapla-sia: Results of a randomised trial on Helicobacter pylori eradication. Gut 53:1244-1249, 2004
8. Mera R, Fontham ET, Bravo LE, et al: Long term follow up of patients treated for Helicobacter pylori infection. Gut 54:1536-1540, 2005
9. Hunt RH: Will eradication of Helicobacter py-lori infection influence the risk of gastric cancer? Am J Med 117 Suppl 5A:86S–91S, 2004
10. Wu CY, Kuo KN, Wu MS, et al: Early Helico-bacter pylori eradication decreases risk of gastric cancer in patients with peptic ulcer disease. Gastro-enterology 137:1641-1648, 2009
11. Cuzick J, Otto F, Baron JA, et al: Aspirin and non-steroidal anti-inflammatory drugs for cancer pre-vention: An international consensus statement. Lan-cet Oncol 10:501-507, 2009
12. Shaheen NJ, Straus WL, Sandler RS: Chemo-prevention of gastrointestinal malignancies with nonsteroidal antiinflammatory drugs. Cancer 94: 950-963, 2002
13. Wang WH, Huang JQ, Zheng GF, et al: Non-steroidal anti-inflammatory drug use and the risk of gastric cancer: A systematic review and meta-analysis. J Natl Cancer Inst 95:1784-1791, 2003
14. Gonzalez-Perez A, Garcia Rodriguez LA, Lopez-Ridaura R: Effects of non-steroidal anti-inflammatory drugs on cancer sites other than the colon and rectum: A meta-analysis. BMC Cancer 3:28-39, 2003
15. Wu CY, Wu CH, Wu MS, et al: A nationwide population-based cohort study shows reduced hos-pitalization for peptic ulcer disease associated with H pylori eradication and proton pump inhibitor use. Clin Gastroenterol Hepatol 7:427-431, 2009
16. Cheng TM: Taiwan’s new national health in-surance program: Genesis and experience so far. Health Aff (Millwood) 22:61-76, 2003
17. Fisher LD, Lin DY: Time-dependent covariates in the Cox proportional-hazards regression model. Annu Rev Pulbic Health 20:145-157, 1999
18. Dignam JJ, Kocherginsky MN: Choice and interpretation of statistical tests used when compet-ing risks are present. J Clin Oncol 26:4027-4034, 2008
19. Fine JP, Gray RJ: A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 94:496-509, 1999
20. Satagopan JM, Ben-Porat L, Berwick M, et al: A note on competing risks in survival data analysis. Br J Cancer 91:1229-1235, 2004
21. Marubini E, Valsecchi MG: Analysing Survival Data From Clinical Trials and Observational Studies. New York, NY, John Wiley and Sons, 1995
22. Hansson LE, Nyren O, Hsing AW, et al: The risk of stomach cancer in patients with gastric or
duodenal ulcer disease. N Engl J Med 335:242-249, 1996
23. Wu CW, Hsieh MC, Lo SS, et al: Prognostic indicators for survival after curative resection for patients with carcinoma of the stomach. Dig Dis Sci 42:1265-1269, 1997
24. Lindblad M, Lagergren J, Garcia Rodriguez LA: Nonsteroidal anti-inflammatory drugs and risk of esophageal and gastric cancer. Cancer Epidemiol Biomarkers Prev 14:444-450, 2005
25. Wang WH, Wong WM, Dailidiene D, et al: Aspirin inhibits the growth of Helicobacter pylori and enhances its susceptibility to antimicrobial agents. Gut 52:490-495, 2003
26. Chang YJ, Wu MS, Lin JT, et al: Induction of cyclooxygenase-2 overexpression in human gastric epithelial cells by Helicobacter pylori involves TLR2/ TLR9 and c-Src-dependent nuclear factor-kappaB activation. Mol Pharmacol 66:1465-1477, 2004
27. Chang YJ, Wu MS, Lin JT, et al: Helicobacter pylori-Induced invasion and angiogenesis of gastric cells is mediated by cyclooxygenase-2 induction through TLR2/TLR9 and promoter regulation. J Im-munol 175:8242-8252, 2005
28. Zaridze D, Borisova E, Maximovitch D, et al: Aspirin protects against gastric cancer: Results of a case-control study from Moscow, Russia. Int J Can-cer 82:473-476, 1999
29. Akre K, Ekstrom AM, Signorello LB, et al: Aspirin and risk for gastric cancer: A population-based case-control study in Sweden. Br J Cancer 84:965-968, 2001
30. Derry S, Loke YK: Risk of gastrointestinal haemorrhage with long term use of aspirin: Meta-analysis. BMJ 321:1183-1187, 2000
31. Boers M, Tangelder MJ, van IH, et al: The rate of NSAID-induced endoscopic ulcers increases linearly but not exponentially with age: A pooled analysis of 12 randomised trials. Ann Rheum Dis 66:417-418, 2007 ■ ■ ■