Title: Chinese medicine reduces the consumption of conventional medicine and medical cost in patients with uterine fibroids: a population-based retrospective
cohort study in Taiwan
Shan-Yu Su, Chih-Hsin Muo, and Donald E. Morisky
Shan-Yu Su ([email protected])
Department of Chinese Medicine, China Medical University Hospital, Taichung 40447, Taiwan
School of Post-baccalaureate Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung 40402, Taiwan
Chih-Hsin Muo ([email protected])
Department of Public Health, China Medical University, Taichung, 40402, Taiwan Management Office for Health Data, China Medical University Hospital, Taichung 40402, Taiwan
Donald E. Morisky ([email protected])
eDepartment of Community Health Sciences, UCLA Fielding School of Public Health,
Los Angeles, California 90095-1772, United States
Correspondence to: Shan-Yu Su. Department of Chinese Medicine, China Medical University Hospital. No. 2 Yuh-Der Road, Taichung, Taiwan 40447. Tel: 886-4-22052121ext.1675; Fax: 886-4-22365141; E-mail address: [email protected]
Abstract
Background: Chinese medicine is commonly used and covered by health insurance to
treat symptoms of uterine fibroids in Taiwan. This retrospective cohort study compared the consumption of conventional western medicine and medical cost between Chinese medicine (CM) users and nonusers among patients with uterine fibroids.
Methods: We extracted 44,122 patients diagnosed with uterine fibrosis between 1996
and 2010 from the National Health Insurance reimbursement database, which is a population-based database released by a government-run health insurance system. Multivariate linear regression models were used to find association between using Chinese medicine and the consumption of conventional medicine, and between using Chinese medicine and medical cost.
Results: The total fibroid-related conventional western medicine consumed by CM users
was less than that by nonusers (β = -10.49, P < 0.0001). Three categories of conventional medicines, including antianemics 3.50 days / year /patient, P < 0.0001), hemostatics (-1.89 days / year / patient, P < 0.0001), and hormone-related agents (-3.13 days / year / patient, P < 0.0001), were used less in patients who were CM users. Moreover, although using CM increased 16.9 USD per patient in CM users annually (P < 0.0001), the total annual medical cost for treating fibroid was 5610 USD less in CM users than in nonusers (P < 0.0001).
Conclusions: Our results suggested that CM reduced the consumption of conventional
medicine, and might be a potential therapeutic substitute for conventional western medicines to treat uterine fibroids with low cost.
Keywords: uterine fibroid; Chinese medicine; conventional western medicine;
Background
Uterine fibroids are the most common benign uterine tumors, which happens in 60% of reproductive aged women . The majority of fibroids are asymptomatic, while in 20% of patients it causes symptoms such as hypermenorrhea, dysmenorrhea, iron-deficiency anemia, and infertility . In symptomatic patients, the first-line treatment is surgery. However, since surgery often cause complications, conservative medical treatment to control symptoms related to fibroids are frequently adopted by patients and gynecologists . Available indicated medical treatments include antianemics (blood derivatives and iron preparations) to treat iron-deficient anemia, hemostatics (coagulants and anti-fibrinolytic agents) to reduce bleedings of hypermenorrhea, and non-steroid anti-inflammatory drugs (NSAIDs) to relief pain. As no currently validated medical treatment is capable of making fibroid disappear, there are no reason to consider medical treatment in case of asymptomatic fibroids .
The estimated direct cost related to uterine fibroids includes cost of surgery, hospital admission, outpatient visit, and medication. The annual cost of uterine fibroids is up to 4.1-9.4 billion US dollars (USD) in the United States , including 3.27 to 5.10 billion USD in nonsurgical management and 829 million to 4.3 billion USD annually in surgical management . If the indirect cost, including lost work-hour costs and obstetric outcomes cost, is taken into account, uterine fibroids are estimated to cost the United States 5.9 -34.4 billion USD annually . In European countries, the number of hospital admissions involving treatment for uterine fibroids ranges from 0.71 to 1.53 per 1000 women, and the estimated direct cost related to uterine fibroids ranges from two to five euros per woman .
Chinese medicine (CM) is an alternative and complementary medicine to treat gynecological diseases in Asian countries . Among fibroid patients, three fourth of them have the experience of utilizing CM, which are considered to be with fewer side effects, less expensive , less subsequent surgery rate , and higher life quality than conventional western medicine . Because of the high usage rate, the expense of CM in Taiwan has been covered by the government-run National Health Insurance (NHI) system since 1995 . Despite of the above-mentioned advantages, it is still unclear that whether use of CM decrease the consumption of conventional western medicine, in the case of that CM users usually have more symptoms than CM nonusers , and are supposed to use more medical resources. Moreover, as CM generates a new component of medical cost, whether the use of CM decreases the total medical cost also needed to be clarified.
In comparing fibroid patients who were CM users with CM nonusers, we sought to determine: (1) if the use of CM correlates with the consumption of conventional western medicines that is specifically for symptoms related to fibroids, and, (2) if the use of CM changes he Nation’s health care cost for uterine fibroids.
Methods
Subjects
Patients with uterine fibroids were identified according to the International
Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) code 218
from 1996 to 2010 in the Longitudinal Health Insurance Database 2000 (LHID2000). The LHID2000 was set up by Taiwan’s National Health Research Institute and it contains chronological information about one million randomly selected individuals who were beneficiaries from 1996 to 2000. This study was approved by the Research Ethics Committee of the CMUH (CMU-REC-101-012).
Study designs
The date of the first diagnosis was used as the entry date, and the endpoint date was December 31th 2010, the date of death, withdrawal from the insurance program, or underwent uterine surgery. The follow-up time was defined as the period from the diagnosis date to the endpoint date. CM users were defined as subjects who had received a mean orally administered CM treatment for more than fifteen days per year. The total fibroid - related consumption of western medicines was estimated by summarizing the number of days for which western medicines have been prescribed with a ICD-9-CM code of 218 from the diagnosis date to the endpoint date. Medical costs included insurance claim for the NHI reimbursement for outpatients (OPD), inpatients (IPD), emergency room (ER), and CM treatments that was related to uterine fibroid.
The examined variables included socio-demographic factors, including age (< 20, 20 – 29, 30 -39, 40-49, and > 50 years), income level (< 520, 520 -639, 640 – 759, and ≥ 759
USD, based on quartile), and occupation status (white collar, blue collar, and others), and endometriosis-related co-morbidities, including hypermenorrhea (ICD-9-CM 626.2), iron-deficiency anemia (ICD-9-CM 280), dysmenorrhea (ICD-9-CM 625.3), and infertility (ICD-9-CM 628 and 628.3).
Statistical analysis
In terms of categorical and ordinal variables, CM users and CM nonusers were compared using chi-square tests and Wilcoxon rank sum test, respectively. Multivariate linear regression models were performed to identify the independent factors associated to the consumption of western medicines, and to assess annual costs in OPD, IPD, ER, and CM, as well as total annual medical cost. These adjusted models were controlled for age, occupation, income, and co-morbidities (hypermenorrhea, iron-deficiency anemia, dysmenorrhea, and infertility). Continuous data are expressed as mean ± SD and categorical data are expressed as number and percentage. All statistical analyses were performed using SAS software, version 9.1 (SAS Institute Inc., Carey, NC), and the significance level was set at a two-tailed P value of less than 0.05.
Results
Study subjects
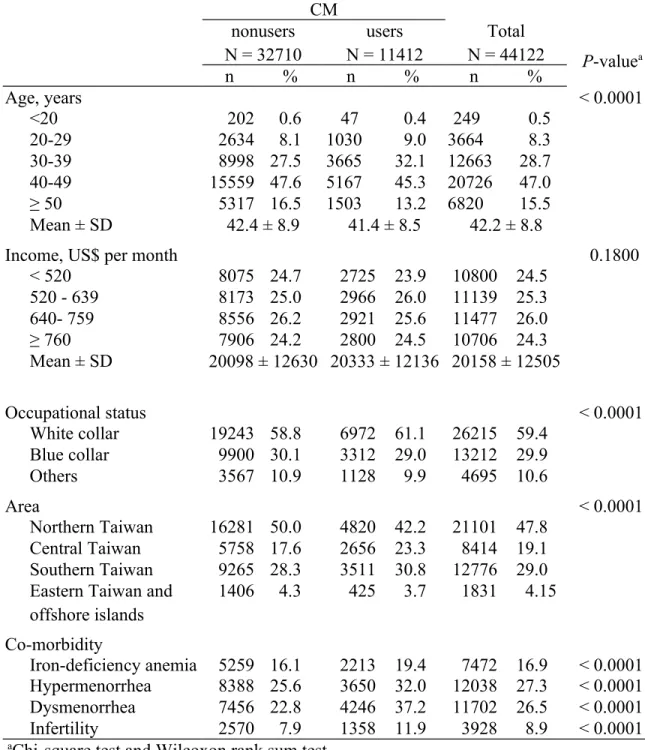
A total of 44,122 women diagnosed with uterine fibrosis between 1996 and 2010 were extracted from the LHID2000 database with a mean follow-up time of 4.6 years. Among them, 11,412 patients were identified as CM users, and 32,710 patients were identified as CM nonusers. The mean age of CM users (41.4 years) was younger than CM nonusers (42.4 years) (Table 1). The proportions of patients among CM users who were white collar, and registered their insurance in Central Taiwan were higher than that among CM nonusers. Moreover, the proportions of patients who were co-morbid with iron-deficiency anemia, hypermenorrhea, dysmenorrhea, and infertility were all higher among CM users than they were among CM nonusers.
Factors associated with the consumption of conventional western medicine
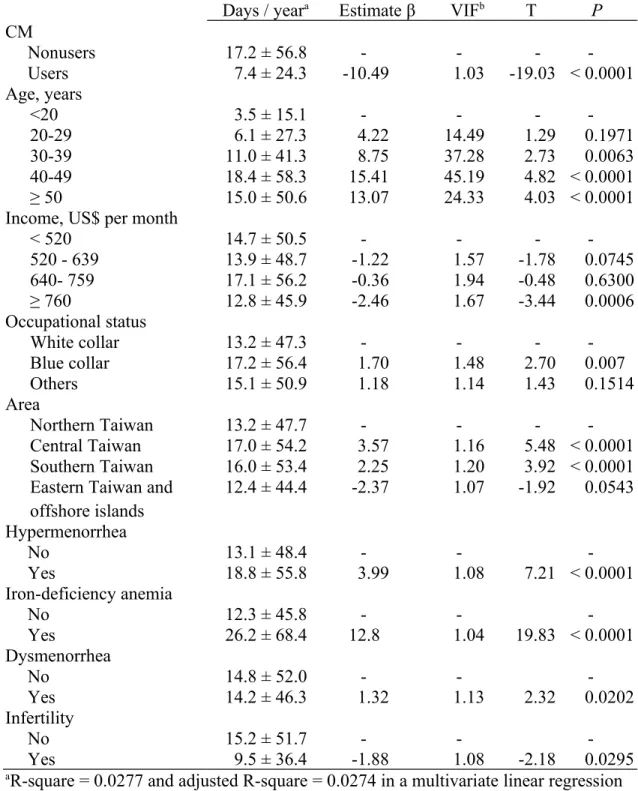
The mean number of days of fibroid-related western medicine taking was 14.6 ± 50.6 days per year. After adjusting for socio-demographic factors (age, income, occupation, and area), and co-morbid covariates (hypermenorrhea, iron-deficiency anemia, dysmenorrhea, and infertility) in a multivariate linear regression model, CM users consumed less western medicine than CM nonusers (-10.5 days / year / patient, P < 0.0001). Patients who aged higher than 40 years, who were blue collar, who registered their insurance in Central Taiwan, and whose income were less than 520 USD / month tended to consume more conventional western medicine. Patients whose diseases were co-morbid with hypermenorrhea, iron-deficiency anemia (both P < 0.0001), and dysmenorrhea (P = 0.0202) also consumed more western medicine than who were not
co-morbid with these illnesses. However, patients whose diseases were co-morbid with infertility tended to consumed less western medicine than whose diseases were not co-morbid with infertility (P = 0.0295) (Table 2).
Difference in the consumption of antianemics, hemostastics, analgesics, and hormone-related agents between CM users and nonusers
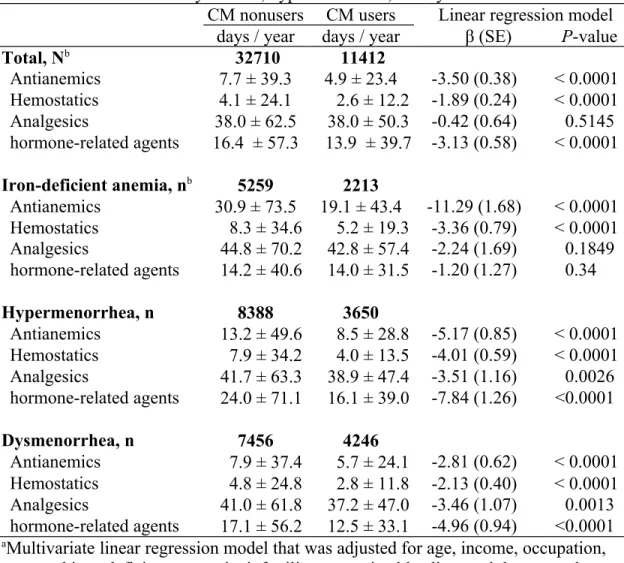
Taking all the subjects as a whole, multivariate linear regression revealed that CM users consumed less antianemics 3.50 days / year /patient, P < 0.0001), hemostatics (-1.89 days / year / patient, P < 0.0001), and hormone-related agents (-3.13 days / year / patient, P < 0.0001) than CM nonusers (table 3). Stratification analysis showed that differences between CM users and nonusers in the consumption of antianemics substantially enlarged in patients with iron-deficiency anemia (-11.29 days / year / patient, P < 0.0001), that of hemostatics enlarged in patients with dysmenorrhea (-4.01 days / year / patient, P < 0.0001), and that of hormone-related agents enlarged in patients with hypermenorrhea (-7.84 days / year / patient, P < 0.0001). Moreover, the consumption of analgesics became significantly different between CM users and nonusers in fibroid patients with dysmenorrhea (-3.46 days / year / patient, P = 0.0013).
Uterine fibroid-related medical cost between CM users and CM nonusers
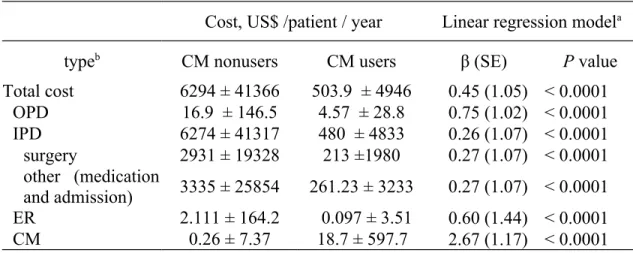
The mean total medical cost of CM users was 503.9 USD, and that of nonusers was 6294 USD per patients. After adjusting for age, income, occupation, area, iron-deficiency anemia, infertility, hypermenorrhea, and dysmenorrhea, the total annual medical cost for treating CM users was 0.45-fold as much as that for treating CM nonusers (Table 4).
Among the total medical cost, although the annual cost of Chinese medicine was 16.9 USD higher for CM users than that for CM nonusers, the annual cost of OPD (-13 USD / year, P < 0.0001), IPD (-5611 USD / year, P < 0.0001), and ER (-2.23 USD / year, P < 0.0001) for CM users were lower than that for CM nonusers.
Discussion
CM is used by patients with uterine fibroids as an alternative to conventional western medicine. This study compared the consumption of conventional western medicine and the exact medical cost between CM users and nonusers in fibroid patients. Although more CM users were co-morbid with iron-deficiency anemia, hypermenorrhea, dysmenorrhea, and infertility, they consumed less fibroid-related western medicines than CM nonusers. The difference in western medicine consumption between the two groups enlarged in patients with co-morbidities. Moreover, the utilization of CM did generate an extra medical cost, however, the total NHI-reimbursed annual health care fee per patient in CM users was substantially lower than that in CM nonusers.
Social-demographic trends regarding CM users in this study, which were extracted from a population-based database from 1996 to 2010, found that CM users in fibroid patients were more likely to be younger and white collar than nonusers. These trends was coincident with a previous study that extract patients from 2000 to 2003 , and also with studies on female-specific diseases, including gynecological and breast cancer and endometriosis . In terms of co-morbidities, including iron-deficiency anemia, hypermenorrhea, dysmenorrhea, and infertility, this study showed that fibroid patients with co-morbidities tended to use CM, implying severe patients with symptoms were more likely to seek for alternative treatments. Several studies have also reported that most alternative users are with poor health status and chronic diseases , and “suffering from disease” is considered one of an important factors that triggers patients to use CM .
Similar to those being associated to CM, high frequencies of taking conventional western medicine were associated with co-morbidities of hypermenorrhea,
deficiency anemia, and dysmenorrhea were associated with. However, patients who were co-morbid with infertility consumed less conventional western medicine than patients who were not co-morbid with infertility. Other social-demographic factors that associated with high consumption of conventional western medicine included age higher than 40, being blue collar, income less than 520 USD / month, and registration of the insurance in Central and Southern Taiwan. In terms of using CM, CM users were less likely to consume conventional medicine, indicating that CM users reduced the use of conventional western medicine when they chose CM to treat diseases.
Antianemics, hemostatics, analgesics, and hormone-related agents are commonly suggested medicines to control fibroid-related symptoms, i.e., iron-deficient anemia, hypermenorrhea, and dysmenorrhea . As medications are only used in patients with well-defined signs or symptoms, among patients with a specific co-morbidity, the difference in the consumption of a co-morbidity-specific medicine implied that CM substituted traditional western medicine to treat this co-morbidity for CM users. For example, among patients co-morbid with hypermenorrhea, the low consumption of hemostatics in CM users implied CM substituted hemostatics to control symptoms of hypermenorrhea. Our data implied that CM might be useful to control symptoms caused by uterine fibroid. Animal studies and clinical studies have reported that CM might have two beneficial effects on uterine fibroid. First, CM is able to treat the symptoms related to uterine fibroid. Second, CM is able to reduce the size of fibroids. An animal study has shown that Shao-fu-zhu-yu decoction, a commonly used CM formula for dysmenorrhea, has been shown to relieve uterine contraction pain by its peripheral analgesic activities . Other two animal studies reported that Bak-foong pills are able to directly down-regulate
mouse uterine tone , and Toki-shakuyaku-san is able to elevate hemoglobin levels in iron-deficiency anemic rats . A clinical trial also showed that Toki-shakuyaku-san improve symptoms of hypermenorrhea, dysmenorrhea, and anemia in fibroid patients . Another clinical trial reported that Nona Roguy made fibroids to shrink in a randomized controlled trial . The present study provided epidemiological evidence showing difference in consumption of conventional western medicine between CM users and nonusers among fibroid patients, implying therapeutic effects to release symptoms caused by fibroids.
Complementary and alternative medicine is considered less expensive than conventional western medicine , and the mean cost per visit is lower for CM than for conventional western medicine . However, since the use of CM generates a component of medical cost, whether using CM decreases the total medical cost is controversial. A review article concludes that there is still a lack of cost-effectiveness research in CM . This study found that the use of CM did reduce total medical cost paid by nation’s health-care system for uterine fibroid. Although there was an extra expenditure in CM (18.7 USD / year / patient) spent by CM users, this extra expenditure was much less than the expenditure in conventional western medicine in both of the groups. Moreover, as CM users reduced the use of western medicine, the total medical reimbursement from NHI for CM users was 5610 UDS / year / patient less in CM users than in nonusers. The costs of uterine fibroids for OPD, IPD, and ER in CM users were all lower than that in CM nonusers. The major difference in medical cost between CM users and nonusers was the in-patient cost. CM users saved more than 2,622 dollars in the cost of surgery and 2,987 dollars in the cost of hospital admission and inpatient medication per patient annually,
indicating CM users underwent less surgery and less hospitalization than CM nonusers. The present group has reported that CM users were more unlikely to under uterine surgery, including hysterectomy and myomectomy, with a hazard ratio of 0.18 . This study confirmed that the decreased surgery rate in CM users reduced health care spending in uterine fibroid.
Using a database from the NHI, which is a government-run, single-payer national health insurance program that insures over 97% of citizens and over 99% of health-care institutes , this study provided epidemiological evidence showing different amount of conventional western medicine consumption and different medical cost between CM users and nonusers among patients with uterine fibroids. However, the first limitation of this study was that we could not verify whether patients underwent other forms of alternative medicines that are not covered by NHI, although the proportional of patients who took those alternative medicines was presumed small because of their high prices. The second limitation of this retrospective study was that it could not directly provide evidence for the efficacy of CM, but could only find a correlation between using CM and low consumption of western medicine and low cost. This correlation could also possibly come from the difference in healthcare seeking behavior between CM users and nonusers. Nevertheless, whatever the underlying reason was, this study highlighted that CM was associated with low consumption of conventional western medicine and low medical cost in fibroid patients. For practitioners, this study provided evidence that CM might be a potential therapeutic substitute for conventional western medicines to treat several symptoms of uterine fibroids. Moreover, for insurance policy makers, this study suggested that CM might be a proper area for health insurance to cover in fibroid
patients.
Conclusion
This study revealed that CM reduced the consumption of conventional medicine, including total fibroid-related conventional medicine and three categories of conventional medicines (antianemics, hemostatics, and hormone-related agents) that are commonly used to release symptoms of fibroids. Moreover, although using CM increased a small amount of medical cost, the total medical cost for treating fibroid was less in CM users than in nonusers. Our results implied that CM might be a potential therapeutic substitute for conventional medicines to treat uterine fibroids with low cost.
Abbreviations
CM, Chinese medicine; IPD, inpatient department; ER, emergency room; ICD-9-CM,
International Classification of Diseases, 9th Revision, Clinical Modification; LHID2000,
Longitudinal Health Insurance Database 2000; NHI, National Health Insurance; NSAID, non-steroid anti-inflammatory drugs; OPD, outpatient department; USD, US dollar.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SYS designed the study and wrote the manuscript. CHM carried out all of the statistical analyses. DEM refined the manuscript and performed English editing.
Acknowledgements
This study was supported by grants from Taiwan Department of Health Clinical Trial and Research Center and for Excellence (DOH102-TD-B-111-004), and Taiwan Department of Health Cancer Research Center for Excellence (DOH102-TD-C-111-005).
References
1. Marino JL, Eskenazi B, Warner M, Samuels S, Vercellini P, Gavoni N, Olive D:
Uterine leiomyoma and menstrual cycle characteristics in a population-based cohort study. Hum Reprod 2004, 19(10):2350-2355.
2. Levy G, Hill MJ, Beall S, Zarek SM, Segars JH, Catherino WH: Leiomyoma:
genetics, assisted reproduction, pregnancy and therapeutic advances. J Assist
Reprod Genet 2012, 29(8):703-712.
3. Chalermchockchareonkit A, Tekasakul P, Chaisilwattana P, Sirimai K, Wahab N:
Laparoscopic hysterectomy versus abdominal hysterectomy for severe pelvic endometriosis. Int J Gynaecol Obstet 2012, 116(2):109-111.
4. Marret H, Fritel X, Ouldamer L, Bendifallah S, Brun JL, De Jesus I, Derrien J, Giraudet G, Kahn V, Koskas M et al: Therapeutic management of uterine fibroid
tumors: updated French guidelines. Eur J Obstet Gynecol Reprod Biol 2012, 165(2):156-164.
5. Cardozo ER, Clark AD, Banks NK, Henne MB, Stegmann BJ, Segars JH: The
estimated annual cost of uterine leiomyomata in the United States. Am J Obstet
Gynecol 2012, 206(3):211 e211-219.
6. Sabry M, Al-Hendy A: Innovative oral treatments of uterine leiomyoma. Obstet
Gynecol Int 2012, 2012:943635.
7. Fernandez H, Farrugia M, Jones SE, Mauskopf JA, Oppelt P, Subramanian D: Rate,
type, and cost of invasive interventions for uterine myomas in Germany, France, and England. J Minim Invasive Gynecol 2009, 16(1):40-46.
8. Chang LC, Huang N, Chou YJ, Lee CH, Kao FY, Huang YT: Utilization patterns of
Chinese medicine and Western medicine under the National Health Insurance Program in Taiwan, a population-based study from 1997 to 2003. BMC Health
Serv Res 2008, 8:170.
9. Tu CC, Li CS, Liu CM, Liu CC: Comparative use of biomedicine and Chinese
medicine in Taiwan: using the NHI Research Database. J Altern Complement Med
2011, 17(4):339-346.
10. Shih CC, Liao CC, Su YC, Tsai CC, Lin JG: Gender Differences in Traditional
Chinese Medicine Use among Adults in Taiwan. PLoS One 2012, 7(4):e32540.
11. Maxion-Bergemann S, Wolf M, Bornhoft G, Matthiessen PF, Wolf U:
Complementary and alternative medicine costs - a systematic literature review.
Forsch Komplementmed 2006, 13 Suppl 2:42-45.
12. Hoenders HJ, Willgeroth FC, Appelo MT: Western and alternative medicine: a
comparison of paradigms and methods. J Altern Complement Med 2008, 14(8):894-896.
13. Su SY, Muo CH, Morisky DE: Use of chinese medicine and subsequent surgery in
women with uterine fibroid: a retrospective cohort study. Evid Based
Complement Alternat Med 2012, 2012:617918.
14. Wye L, Sharp D, Shaw A: The impact of NHS based primary care complementary
therapy services on health outcomes and NHS costs: a review of service audits and evaluations. BMC Complement Altern Med 2009, 9:5.
15. Hsieh SC, Lai JN, Lee CF, Hu FC, Tseng WL, Wang JD: The prescribing of
health insurance reimbursement database. Pharmacoepidemiol Drug Saf 2008, 17(6):609-619.
16. Lin YH, Chiu JH: Use of Chinese medicine by women with breast cancer: a
nationwide cross-sectional study in Taiwan. Complement Ther Med 2011, 19(3):137-143.
17. Navo MA, Phan J, Vaughan C, Palmer JL, Michaud L, Jones KL, Bodurka DC, Basen-Engquist K, Hortobagyi GN, Kavanagh JJ et al: An assessment of the
utilization of complementary and alternative medication in women with gynecologic or breast malignancies. J Clin Oncol 2004, 22(4):671-677.
18. Fang RC, Tsai YT, Lai JN, Yeh CH, Wu CT: The traditional chinese medicine
prescription pattern of endometriosis patients in taiwan: a population-based study. Evid Based Complement Alternat Med 2012, 2012:591391.
19. Liao HL, Ma TC, Chiu YL, Chen JT, Chang YS: Factors influencing the
purchasing behavior of TCM outpatients in Taiwan. J Altern Complement Med
2008, 14(6):741-748.
20. Wolsko P, Ware L, Kutner J, Lin CT, Albertson G, Cyran L, Schilling L, Anderson RJ: Alternative/complementary medicine: wider usage than generally
appreciated. J Altern Complement Med 2000, 6(4):321-326.
21. Blais R, Maiga A, Aboubacar A: How different are users and non-users of
alternative medicine? Can J Public Health 1997, 88(3):159-162.
22. Ma H, Su S, Duan J, Tang Y, Zhou J, Guo J, Zhan Z: Evaluation of the analgesic
activities of the crude aqueous extract and fractions of Shao Fu Zhu Yu decoction. Pharm Biol 2011, 49(2):137-145.
23. Rowlands DK, Cui YG, Wong HY, Gou YL, Chan HC: Traditional Chinese
medicine Bak Foong Pills alters uterine quiescence - possible role in alleviation of dysmenorrhoeal symptoms. Cell Biol Int 2009, 33(12):1207-1211.
24. Akase T, Onodera S, Matsushita R, Tashiro S: A comparative study of laboratory
parameters and symptoms effected by Toki-shakuyaku-san and an iron preparation in rats with iron-deficiency anemia. Biol Pharm Bull 2004,
27(6):871-878.
25. Akase T, Onodera S, Jobo T, Matsushita R, Kaneko M, Tashiro S: A comparative
study of the usefulness of toki-shakuyaku-san and an oral iron preparation in the treatment of hypochromic anemia in cases of uterine myoma. Yakugaku Zasshi
2003, 123(9):817-824.
26. Hazlina NNH, Pazudin MI, Nor Aliza AG, Mohsin Sahil SJ: Clinical Study to
Compare the Efficacy and Adverse Effects of Nona Roguy Herbal Formulation and Gonadotrophin Releasing Hormone Agonist (GnRH) in the Treatment of Uterine Fibroids. International Medical Journal 2005, 12(4):295-302.
27. Zhang F, Kong LL, Zhang YY, Li SC: Evaluation of impact on health-related
quality of life and cost effectiveness of Traditional Chinese Medicine: a systematic review of randomized clinical trials. J Altern Complement Med 2012, 18(12):1108-1120.
28. Lin MH, Chou MY, Liang CK, Peng LN, Chen LK: Population aging and its
impacts: strategies of the health-care system in Taipei. Ageing Res Rev 2010, 9 Suppl 1:S23-27.
29. Chi C, Lee JL, Tsai SL, Chen WY: Out-of-pocket payment for medical care under
Table 1 Comparison of socio-demographic factors and co-morbidities between Chinese medicine (CM) users and nonusers in patients with uterine fibroids.
CM nonusers N = 32710 users N = 11412 Total N = 44122 P-valuea n % n % n % Age, years < 0.0001 <20 202 0.6 47 0.4 249 0.5 20-29 2634 8.1 1030 9.0 3664 8.3 30-39 8998 27.5 3665 32.1 12663 28.7 40-49 15559 47.6 5167 45.3 20726 47.0 ≥ 50 5317 16.5 1503 13.2 6820 15.5 Mean ± SD 42.4 ± 8.9 41.4 ± 8.5 42.2 ± 8.8
Income, US$ per month 0.1800
< 520 8075 24.7 2725 23.9 10800 24.5 520 - 639 8173 25.0 2966 26.0 11139 25.3 640- 759 8556 26.2 2921 25.6 11477 26.0 ≥ 760 7906 24.2 2800 24.5 10706 24.3 Mean ± SD 20098 ± 12630 20333 ± 12136 20158 ± 12505 Occupational status < 0.0001 White collar 19243 58.8 6972 61.1 26215 59.4 Blue collar 9900 30.1 3312 29.0 13212 29.9 Others 3567 10.9 1128 9.9 4695 10.6 Area < 0.0001 Northern Taiwan 16281 50.0 4820 42.2 21101 47.8 Central Taiwan 5758 17.6 2656 23.3 8414 19.1 Southern Taiwan 9265 28.3 3511 30.8 12776 29.0
Eastern Taiwan and offshore islands 1406 4.3 425 3.7 1831 4.15 Co-morbidity Iron-deficiency anemia 5259 16.1 2213 19.4 7472 16.9 < 0.0001 Hypermenorrhea 8388 25.6 3650 32.0 12038 27.3 < 0.0001 Dysmenorrhea 7456 22.8 4246 37.2 11702 26.5 < 0.0001 Infertility 2570 7.9 1358 11.9 3928 8.9 < 0.0001
Table 2 Multivariate linear regression for number of days of fibroid-related treatment in patients with uterine fibroid.
Days / yeara Estimate β VIFb T P
CM Nonusers 17.2 ± 56.8 - - - -Users 7.4 ± 24.3 -10.49 1.03 -19.03 < 0.0001 Age, years <20 3.5 ± 15.1 - - - -20-29 6.1 ± 27.3 4.22 14.49 1.29 0.1971 30-39 11.0 ± 41.3 8.75 37.28 2.73 0.0063 40-49 18.4 ± 58.3 15.41 45.19 4.82 < 0.0001 ≥ 50 15.0 ± 50.6 13.07 24.33 4.03 < 0.0001
Income, US$ per month
< 520 14.7 ± 50.5 - - - -520 - 639 13.9 ± 48.7 -1.22 1.57 -1.78 0.0745 640- 759 17.1 ± 56.2 -0.36 1.94 -0.48 0.6300 ≥ 760 12.8 ± 45.9 -2.46 1.67 -3.44 0.0006 Occupational status White collar 13.2 ± 47.3 - - - -Blue collar 17.2 ± 56.4 1.70 1.48 2.70 0.007 Others 15.1 ± 50.9 1.18 1.14 1.43 0.1514 Area Northern Taiwan 13.2 ± 47.7 - - - -Central Taiwan 17.0 ± 54.2 3.57 1.16 5.48 < 0.0001 Southern Taiwan 16.0 ± 53.4 2.25 1.20 3.92 < 0.0001
Eastern Taiwan and offshore islands 12.4 ± 44.4 -2.37 1.07 -1.92 0.0543 Hypermenorrhea No 13.1 ± 48.4 - - -Yes 18.8 ± 55.8 3.99 1.08 7.21 < 0.0001 Iron-deficiency anemia No 12.3 ± 45.8 - - -Yes 26.2 ± 68.4 12.8 1.04 19.83 < 0.0001 Dysmenorrhea No 14.8 ± 52.0 - - -Yes 14.2 ± 46.3 1.32 1.13 2.32 0.0202 Infertility No 15.2 ± 51.7 - - -Yes 9.5 ± 36.4 -1.88 1.08 -2.18 0.0295
aR-square = 0.0277 and adjusted R-square = 0.0274 in a multivariate linear regression
model that was adjusted for age, income, occupation, area, and iron-deficiency anemia, infertility, excessive bleeding, and dysmenorrhea.
Table 3 Consumption of antianemics, hemostatics, and analgesics in patients co-morbid with iron-deficiency anemia, hypermenorrhea, and dysmenorrhea.
CM nonusers CM users Linear regression model
days / year days / year β (SE) P-value
Total, Nb 32710 11412 Antianemics 7.7 ± 39.3 4.9 ± 23.4 -3.50 (0.38) < 0.0001 Hemostatics 4.1 ± 24.1 2.6 ± 12.2 -1.89 (0.24) < 0.0001 Analgesics 38.0 ± 62.5 38.0 ± 50.3 -0.42 (0.64) 0.5145 hormone-related agents 16.4 ± 57.3 13.9 ± 39.7 -3.13 (0.58) < 0.0001 Iron-deficient anemia, nb 5259 2213 Antianemics 30.9 ± 73.5 19.1 ± 43.4 -11.29 (1.68) < 0.0001 Hemostatics 8.3 ± 34.6 5.2 ± 19.3 -3.36 (0.79) < 0.0001 Analgesics 44.8 ± 70.2 42.8 ± 57.4 -2.24 (1.69) 0.1849 hormone-related agents 14.2 ± 40.6 14.0 ± 31.5 -1.20 (1.27) 0.34 Hypermenorrhea, n 8388 3650 Antianemics 13.2 ± 49.6 8.5 ± 28.8 -5.17 (0.85) < 0.0001 Hemostatics 7.9 ± 34.2 4.0 ± 13.5 -4.01 (0.59) < 0.0001 Analgesics 41.7 ± 63.3 38.9 ± 47.4 -3.51 (1.16) 0.0026 hormone-related agents 24.0 ± 71.1 16.1 ± 39.0 -7.84 (1.26) <0.0001 Dysmenorrhea, n 7456 4246 Antianemics 7.9 ± 37.4 5.7 ± 24.1 -2.81 (0.62) < 0.0001 Hemostatics 4.8 ± 24.8 2.8 ± 11.8 -2.13 (0.40) < 0.0001 Analgesics 41.0 ± 61.8 37.2 ± 47.0 -3.46 (1.07) 0.0013 hormone-related agents 17.1 ± 56.2 12.5 ± 33.1 -4.96 (0.94) <0.0001
aMultivariate linear regression model that was adjusted for age, income, occupation,
area, and iron-deficiency anemia, infertility, excessive bleeding, and dysmenorrhea
bN, subject number in a group; and n, subject number in a subgroup
cAntianemics, including blood derivatives and iron; hemostatics, including coagulants
and hemostatics; and analgesics, including non-steroid anti-inflammatory drugs and analgesics.
Table 4 Uterine fibroid-related cost in CM-users and nonusers.
Cost, US$ /patient / year Linear regression modela
typeb CM nonusers CM users β (SE) P value
Total cost 6294 ± 41366 503.9 ± 4946 0.45 (1.05) < 0.0001 OPD 16.9 ± 146.5 4.57 ± 28.8 0.75 (1.02) < 0.0001 IPD 6274 ± 41317 480 ± 4833 0.26 (1.07) < 0.0001 surgery 2931 ± 19328 213 ±1980 0.27 (1.07) < 0.0001 other (medication and admission) 3335 ± 25854 261.23 ± 3233 0.27 (1.07) < 0.0001 ER 2.111 ± 164.2 0.097 ± 3.51 0.60 (1.44) < 0.0001 CM 0.26 ± 7.37 18.7 ± 597.7 2.67 (1.17) < 0.0001
aMultivariate linear regression model for nature log transformation of cost and model
was adjusted for age, income, occupation, area, iron-deficiency anemia, infertility, excessive bleeding, and dysmenorrhea.