Childhood Overweight or Obesity Predicts Subclinical Atherosclerosis in Young Adults
Ta-Chen Su1, Chien-Chang Liao2, Kuo-Liong Chien1,3, Sandy Huey-Jen Hsu4,
Fung-Chang Sung5
1Department of Internal Medicine and Cardiovascular Center, National Taiwan
University Hospital, Taipei, Taiwan
2Health Policy Research Center, Taipei Medical University, Taipei, Taiwan 3Institute of Epidemiology and Preventive Medicine, College of Public Health,
National Taiwan University, Taipei, Taiwan
4Department of Laboratory Medicine, National Taiwan University Hospital, Taipei,
Taiwan
5China Medical University Institute of Clinical Medical Science and Management
Office for Health Data, Taichung, Taiwan Corresponding Author:
Ta-Chen Su, MD, PhD
Department of Internal Medicine and Cardiovascular Center, National Taiwan University Hospital
Address: No. 7, Chung-Shan South Road, Taipei 100, Taiwan Tel: +886-2-23123456 ext 66719; Fax: +886-2-23712361, E-mail: tachensu@ntu.edu.tw
Co-corresponding Author Fung-Chang Sung, PhD, MPH
Professor, Institute of Clinical Medical Science China Medical University 91 Hsueh-Shih Road Taichung 404, Taiwan
Tel: 886-4-2206-2295; Fax: 886-4-2201-9901 E-mail: fcsung@mail.cmu.edu.tw
Abstract:
Aims: To investigate the relationship between childhood overweight and obesity and young adulthood preclinical atherosclerosis, including carotid intima-media thickness (CIMT) and prehypertension or hypertension, we conducted the YOung TAiwanese Cohort (YOTA) Study in Taiwan.
Methods: From children who participated in the 1992–2000 mass urine screening program in Taiwan, we recruited 303 subjects with elevated blood pressure (EBP) and 486 subjects with normal BP in their childhood, in 2006-2008. These 789 young adult participants received a health check-up for cardiovascular health, including blood and urine examines, anthropometrics, BP, and subclinical cardiovascular risk examines index by CIMT. Data analyses evaluated the associated risks in both childhood and young adulthood.
Results: School students with childhood overweight had a higher risk of prehypertension or hypertension with a relative risk of 3.32 (1.44-7.68) for
overweight and 5.58 (2.70-11.54) for obese in young adulthood with an average age of 21. Childhood overweight also predicted a higher risk of thicker CIMT with relative risks of 2.99 (1.37-6.52) and 3.33 (1.65-6.74) for overweight and obese, respectively, in adulthood after a mean follow-up of 8.5 years. The childhood body mass index had a well track from childhood to adulthood with an adjusted R square of
0.551. The participants who were not overweight in childhood could also have a higher risk of hypertension or pre-hypertension if they became obese in adulthood. Conclusions: This study highlights the importance of prevention and management of overweight or obesity in childhood for primary prevention of cardiovascular disease in adulthood.
Introduction
Cardiovascular disease (CVD) is the leading cause of mortality and a major health burden worldwide including many Asian populations, such as in Taiwan, China, and India1-3).The progression of atherosclerotic begins in early life may modify increased
risk of CVD, depending on predisposing genetic and environmental factors4-6). With
an aging population, as is the case in Taiwan, early detection of atherosclerosis and its associated risk factors is an important step to prevent stroke and heart disease in later life.
The worldwide increasing incidence and prevalence of childhood overweight and metabolic syndrome would further increase the cardiovascular burden in later life7, 8).
The Bogalusa Study4, 9)and the Pathobiological Determinants of Atherosclerosis in
Youth (PDAY)Study10) have shown that the atherosclerosis process starts in early
childhood. These autopsy studies have demonstrated that the intimal surfaces covered with atherosclerotic lesions was significantly associated with abnormal lipid profile and cardiovascular risk factors, such as hypertension and obesity11).The Bogalusa
Study reported that the fatty streak is the early atherosclerosis, presenting in 50% of the children and increasing to 85% of adults9). The Cardiovascular Risk in Young
Finns Study also reported, carotid intima-media thickness (CIMT) measured in young adults aged 33-39 years are directly related to low-density lipoprotein cholesterol
(LDL-C), systolic blood pressure, and cigarette smoking in 12-18 years old12). The
Bogalusa Study indicated that childhood measures of LDL-C level and BMI may predict carotid IMT in young adults13). Several other studies have further linked
childhood adiposity and obesity to premature deaths from cardiovascular diseases14-17).
Thus, the study on adolescents and young adults may provide important information for early prevention of cardiovascular disease. However, there is limited study investigating this association in Asian population and lack of evidence if the tracking of overweight/obesity and subclinical cardiovascular disease was measured in young adults with an average age of 21 years-old. To investigate the effect of childhood elevated blood pressure (EBP) on later life, we conducted a follow-up study, the YOung TAiwanese Cohort (YOTA) Study from 2006 to 2008. This study examined how childhood and adolescent overweight/obesity predict atherosclerosis and prehypertension/hypertension in young adulthood, by measuring the CIMT and blood pressure in a cohort of young adult and adolescents.
Material and Methods Subjects
From 1992 to 2000, a nationwide mass urine screening on renal health was conducted for school children aged 6 to 18 years in Taiwan 8, 18-20). Anthropometric
status and blood pressure were also measured for each children who had been
examined with proteinuria or glucosuria positive for twice at the screening activity (N =103,756). Among them, 9227 students were found to have childhood EBP. Students who had participated in the screening program were contacted for the present YOTA Study. Figure 1 shows the flow chart of this study starting from the urinary screening program to the participant recruitment for the present study20). We sent invitation
letters to parents of eligible students in the Taipei area. After 3-5 days, 12 trained assistants and nurses conducted telephone interviews inviting these subjects with childhood EBP to come in for a follow up health examination. No telephone interview contact was made with normotensive students. Among the 707 subjects with EBP in childhood, 303 completed the follow-up health examinations, for a response rate of 42.9%. The detailed information is available in recent reports.
Among the 59,855 subjects of normal BP in childhood with address, 17,448 live in Taipei. We randomly contacted with 6390 living in Taipei by mail, 5886 did not respond, and 17 refused to
participate. Finally, 487 subjects with normal BP in childhood completed the follow-up health examinations, but one lacked the scheduled blood test and carotid duplex examination, resulting in a response rate of 7.6% (486/6390). The social background at that time didn’t favor the study because a great social anxiety when criminal syndicate had
flourished most inTaiwan. Thus, most of contact methods to them were considered as suspected criminal affairs in 2006-2008. Even though the very low response rate, the basic characteristics such as gender, fasting glucose levels, and cholesterol in childhood revealed no significant difference between responder and non-responders.
With consents, 303 with EBP and 486 with normal BP in childhood completed the follow-up study in Taipei area. Participants provided blood and urine specimens, and received subclinical atherosclerotic measures including carotid intima-media thickness (CIMT) and brachial-ankle aortic pulse wave velocity. All participants signed the inform
consents while they were recruited and this study was approved by institutional reviews at National Taiwan University and China Medical University.
Assessments of Vascular Risk Factors and Clinical Information
the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7), hypertension was defined as values 140/90 mmHg, or participants receiving anti-hypertension agents. The BP was measured with mercury
sphygmomanometer in a standardized fashion, cuff-size adjusted to the circumference of the arm. BP was recorded using the mean of two measurements taken after 5 minutes of rest in the seated position. Subjects' weight and height were also obtained.
The body mass index (BMI) of each participant was the weight in kilograms divided by the square of the height in meters. Overweight in childhood and adolescents was defined according to age and gender-specific criteria of BMI level ≥85th percentile from 2 to 18
years-old of age by Taiwan Department of Health
(http://www.ctaso.org.tw/news5.htm). Adult (age ≥18 years) with a BMI range 24-26.99 kg/m2 was defined as overweight, and a BMI of
27 kg/m2 and over as obesity. Prevalent diabetes mellitus (DM) was
defined as fasting glucose >6.99 mmol/L and/or a history of
managing DM. The lifestyle of each individual, including smoking, drinking and exercise, was obtained from a structured and
self-administered questionnaire. Dietary habits with a modified frequency scale of dietary questionnaire for hyperlipidemia in Taiwanese. Family history of CVD, hyperlipidemia, DM, and hypertension were also obtained.
Serum markers
All subjects with a fasting period for 10-14 h were asked to provide a venous blood sample of 20 ml from an antecubital vein for serum and plasma, and DNA extraction. Blood glucose, and serum total cholesterol, triglyceride, low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C) were
measured by an auto-analyzer (Hitachi 7250 Special; Hitachi, Tokyo, Japan) in central lab at the National Taiwan University Hospital. For the assays, blood samples were first centrifuged at 3000 rpm for 15 minutes within 30 minutes of collection, and then stored at -70 degree Celsius until assessment.
Assessment of IMT of carotid arteries
The protocol for the carotid atherosclerosis measurements, including CIMT and carotid atherosclerotic plaque, has been well documented18, 20-22). An experienced technician measured CIMT at
extracranial carotid arteries using a high-resolution B-mode ultrasonography (GE Vivid ultrasound system, Horten, Norway), equipping with a 3.5–10 MHz real-time B-mode scanner. A
quantification package was applied to do offline automatic
calculation for vascular ultrasound. The maximum and mean values of IMTs were calculated bilaterally for the common carotid artery (CCA) proximal to the carotid bifurcation, bulb, and internal carotid artery. CCA1 and CCA2 on the CCA distal were measured at 0–1 cm and 1–2 cm, respectively, from the carotid bifurcation. CIMT
measurement of the posterior wall of the distal CCA was made from the leading edge of the first echogenic line (interface between lumen and vascular intima) to the leading edge of the second line (interface between vascular media and adventitia)23).
The carotid IMT measures included RCCA1 (right CCA 1cm), RCCA2 (right CCA 2 cm), LCCA1 (left CCA 1 cm), LCCA2 (left CCA 2cm), right bulb, left bulb, right and left internal carotid artery. A digitalized memory system in the DICOM format recorded all measurements. We acquired a clipped moving-image for the carotid bulb and CCA for 5-secnds. A computer program was used to analyze the digitized M-mode and to
measure the CIMT between two successive R waves. This method was able to obtain a mean value of 150 CCA measurements on a 10-mm segment. The technician was required to conduct the reliability test by repeating measurements for 30 subjects in Two weeks. The reliability of CIMT measurement at bilateral CCA (mean of right and left CCA) was excellent. The intraobserver coefficients of correlation reliability of CIMT measurements were 98.8% for the right side CCA and 98.5% for the left side CCA20).
Statistical Analyses
Statistical analyses were performed using SAS software (Version 9.1.3; SAS Institute Inc., Cary, NC, USA). Data analysis first made comparisons between participants with and without childhood EBP for associations with childhood risks and adult risks measured in the follow-up period in males and females. The childhood risks included BMI, cholesterol, fasting glucose, systolic BP and diastolic BP, and the adult risks included BMI, cholesterol, glucose AC, systolic BP and diastolic BP, HDL-C, LDL-C, DM, hypertension, smoking, drinking, overweight and obesity. Simple correlation analysis measured the relationship between childhood BMI and adulthood BMI. The means of carotid IMT measures were calculated item by item in association with BMI trend for both men and women. Continuous variables were compared between group
means ± standard deviations (SD) using the Student’s two-tailed t-test, or the Mann– Whitney U-test if not in normal distribution. The Chi-square test was applied for categorical data. Multivariate logistic regression analyses measured the strength of association between childhood BMI overweight and adulthood overweight or obesity on the risk of adulthood thicker CIMT or pre-hypertension or hypertension. Odds ratios (ORs) and 95% confidence intervals (CIs) for participants with the carotid IMT at ≥ 75th percentile and with prehypertension or hypertension were obtained after
controlling for adulthood cardiovascular risk factors, including age, gender, systolic BP, fasting glucose, cholesterol level, smoking and alcohol habit, and household income.
Results
Participants in Table 1 shows male participants had higher mean BMI and prevalence of cardiovascular risk factors than female participants had. Participants with childhood EBP had higher childhood risks included BMI, cholesterol, fasting glucose, systolic BP and diastolic BP than those without childhood EBP, but not in cholesterol and glucose AC for males. Compared with participants without childhood EBP, participants with the childhood EBP were more likely to have metabolism syndromes, particularly overweight or obese (more than 2-fold in both men and women) and hypertension (12-fold in men and 7-fold in women). There was a strong correlation between the childhood BMI measures and the adulthood BMI measures (R2 = 0.551, p <0.001) (Figure 2).
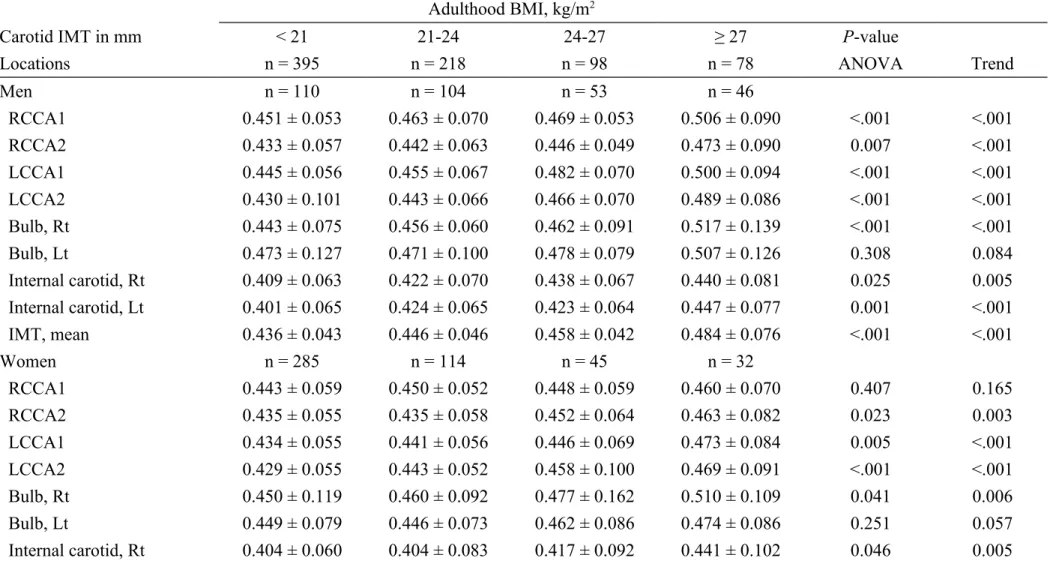
All carotid IMT measured in adulthood, including RCCA1, RCCA2, LCCA1, LCCA2, Bulb Rt, Bulb Lt, ICA Rt, and ICA Lt, increased with the increase of BMI in both men and women. The trends were not significant only for Bulb Lt in men and women and for RCCA1 in women (Table 2).
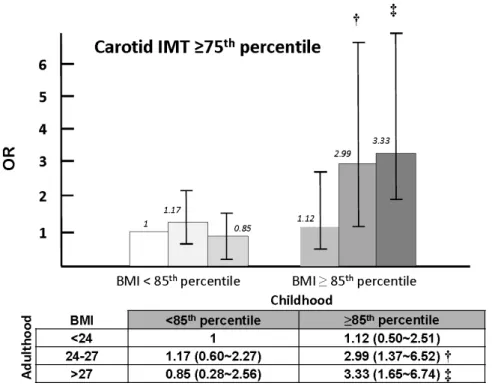
Figure 3 shows ORs of having adulthood carotid IMT measures at the highest 25 percentiles associating with participants BMI by their childhood BMI at < 85th
percentile and > 85percentiles. The risk of having high carotid IMT was not associated with adult BMI if their childhood BMIs were at < 85 percentile. The
adjusted OR increased with the increase of adulthood BMI, to 3.33 (95% CI 1.65~6.74) for those with the BMI of > 27 Kg/m2 and their childhood BMIs at >
85percentiles. Figure 4 shows the OR of having adult prehypertension or hypertension increased as increases of both adulthood BMIs and childhood BMIs. Compared to those with adulthood BMIs <24 Kg/m2 and childhood BMI < 85 percentiles, the
Discussions
Earlier atherosclerosis and hypertension are known risks leading to cardiovascular diseases in the later life. This study revealed that children with overweight/obesity are also more likely to remain obese and at a higher risk of pre-hypertension/ hypertension and thicker CIMT, 8.5 years later in the young adult with a mean age of 21.32 years-old. Participants who were not overweight in childhood would also have a higher risk of pre-hypertension or hypertension if they were obese in adulthood. This study provides the first line evidence to link childhood
overweight/obesity and risk for pre-hypertension/hypertension and subclinical atherosclerosis in adulthood in Asia.
The high tracking of BMI between childhood and adulthood is similar to previous findings, including in a society undergoing enormous changes in diet and activity, like in China25). The findings of our study are in agreement with previous
large cohort studies in the US and European populations that childhood
overweight/obesity is associated with adulthood atherosclerosis using the indicator of carotid IMT4, 5, 12, 13). However, the follow-up time from the childhood survey to the
adulthood survey in the present study is shorter than that studies in western countries. This study indicated that the pathogenesis of atherosclerosis could act through
insulin resistance, and etc., as early as from childhood to adolescents, and to young adult7, 10-11). Cardiovascular risk factors in childhood may act and promote
atherosclerosis if they are persistent across adolescents and young adults14, 16-17).
Childhood overweight/obesity is associated with higher risk of future pre-hypertension or pre-hypertension and high-risk subclinical atherosclerosis in young adulthood. However, as shown in this study, though, some children and adolescents with overweight or obesity become nonobese in their young adulthood and this change is associated with a reduction in cardiovascular risk, such as
prehypertension/hypertension and subclinical atherosclerosis. This finding also echoes the recent results of the Bogalusa heart and cardiovascular risk in young Finns
studies: the youth metabolic syndrome may have 3.4-time the high IMT risk in adulthood26). Clinical implication of this study is primarily for the prevention of
cardiovascular diseases and premature death should be focused on childhood
overweight/obesity. On the other hand, the educational program for healthy lifestyle to normalize body weight should be initiated as early as possible at elementary schools and middle schools. There is an urgent need to call for action for worldwide “obesity epidemic in childhood” in order to prevent cardiovascular diseases and premature death27-28).
This study was limited with the recruited participants had been identified with proteinuria or glucouria positive in the urinary screening program. Thus, the findings may not be generalized to all young population. However, all participants were relative healthy in adulthood and similar with general population in Taiwan29). The
incident hypertension and diabetes identified in the participants are low in the 8.5-year follow-up as shown in Table 1. No serious illnesses have been identified. Thus, the abnormal urine screening in childhood does not exclude the clinical application of this study. The strength of this study was that the study subjects came from a large school children population in Taiwan during 1992-2000 and provided an important representative population for a long-term cohort study to investigate the
cardiovascular and endocrine/metabolic risk from childhood to adulthood14, 18, 20, 30).
In conclusion, this study demonstrates well a BMI track from childhood to adulthood and the persistent overweight or obesity contributes to the risk of preclinical atherosclerosis and high blood pressure in adulthood. More attention should be paid to the prevention and management of childhood overweight and obesity.
Acknowledgements:
Funding: This study was supported by grants from National Health Research Institute of Taiwan (NHRI-EX97-9721PC, EX98~9721PC, EX99~9721PC, EX100~9721PC; NHRI-EX95-9531PI, EX96~9531PI, EX97~9531PI).
Financial Disclosure: The authors have no financial relationships relevant to this article to disclose.
Potential Conflicts of Interest: The authors have no conflicts of interest relevant to this article to disclose.
This paper has been presented in学会ダイジェスト:第 44 回日本動脈硬化学会 2012年 7 月 19 日~20 日 福岡
Key messages
WHAT’S KNOWN ON THIS SUBJECT: Although childhood obesity has been linked to adulthood cardiovascular diseases, there is little evidence if the tracking of overweight/obesity and subclinical cardiovascular disease was measured in young adults with an average age of 21 years-old?
WHAT THIS STUDY ADDS: Tracking of body mass index from childhood to young adulthood in Taiwanese, a significant increase in subclinical carotid intima-media thickness and prehypertension/hypertension was clearly demonstrated in those persistent overweight/obesity.
References
1) Reddy KS. Cardiovascular disease in non-western countries. N Engl J Med 2004; 350: 2438-40
2) He J, Gu D, Wu X, Reynolds K, Duan X, Yao C, et al: Major causes of death among men and women in China. N Engl J Med, 2005; 353: 1124-34
3) Health and vital statistics II of the Republic of China, 2009, Department of Health, Executive Yuan, Taipei, Republic of China. Available at http://www.doh.gov.tw/EN2006/index_EN.aspx. Accessed March 4, 2011.
4) Berenson GS, Srinivasan SR, Bao W, Newman WP 3rd, Tracy RE, Wattigney WA: Association between multiple cardiovascular risk factors and the early development of atherosclerosis. Bogalusa Heart Study. N Engl J Med, 1998; 338: 1650-66
5) Davis PH, Dawson JD, Riley WA, Lauer RM: Carotid intimal medial thickness is related to cardiovascular risk factors measured from childhood through middle age: the Muscatine Study. Circulation, 2001; 104: 2815-19
6) McMahan BW, Gidding SS, Malcom GT et al: Pathobiological determinants of atherosclerosis in young risk scores are
associated with early and advanced atherosclerosis. Pediatrics, 2006; 118: 1447-55
7) Daniels SR, Arnett DK, Eckel RH, Gidding SS, Hayman LL, Kumanyika S, et al: Overweight in children and adolescents: pathophysiology, consequences, prevention, and treatment. Circulation, 2005; 111: 1999-2012
8) Liao CC, Su TC, Chien KL, Wang JK, Chiang CC, Lin CC, et al: Elevated blood pressure, obesity, and hyperlipidemia. J Pediatr, 2009; 155: 79-83, 83.e1
9) Newman WP 3rd, Freedman DS, Voors AW, Gard PD, Srinivasan SR, Cresanta JL, et al: Relation of serum lipoprotein levels and systolic blood pressure to early atherosclerosis: the Bogalusa Study. N Engl J Med, 1986; 314: 138-44
10) McGill HC Jr, McMahan CA, Zieske AW, Malcom GT, Tracy RE, Strong JP: Effect of nonlipid risk factors on the atherosclerosis in young with favorable lipoprotein profile. Pathobiological
1546-50
11) McGill HC Jr, McMahan CA, Malcom GT, Oalman MC, Strong JP: Effects of serum lipoproteins and smoking on the atherosclerosis in young men and women. The PDAY Research Group.
Pathobiological Determinants of Atherosclerosis in Youth. Arterioscler Thromb Vasc Biol, 1997; 17: 95-106
12) Raitakari OT, Juonala M, Kähönen M, Taittonen L, Laitinen T, Mäki-Torkko N, et al: Cardiovascular risk factors in childhood and carotid artery intima-media thickness in adulthood: the
Cardiovascular Risk in Young Finns Study. JAMA, 2003; 290: 2277-83
13) Li S, Chen W, Srinivasan SR, Bond MG, Tang R, Urbina EM, Berenson GS: Childhood cardiovascular risk factors and carotid vascular changes in adulthood: the Bogalusa Heart Study. JAMA, 2003; 290: 2271-6. Erratum in: JAMA, 2003; 290: 2943
14) Juonala M, Magnussen CG, Berenson GS, Venn A, Burns TL, Sabin MA, et al: Childhood adiposity, adult adiposity, and cardiovascular risk factors. N Engl J Med, 2011; 365: 1876-85
15) Must A, Jacques PF, Dallal GE, Bajema CJ, Dietz WH: Long-term morbidity and mortality of overweight adolescents: a follow-up of the Harvard Growth Study of 1922 to 1935. N Engl J Med, 1992; 327: 1350-5
16) Baker JL, Olsen LW, Sørensen TI: Childhood body-mass index and the risk of coronary heart disease in adulthood. N Engl J Med, 2007; 357: 2329-37
17) Franks PW, Hanson RL, Knowler WC, Sievers ML, Bennett PH, Looker HC: Childhood obesity, other cardiovascular risk factors, and premature death. N Engl J Med, 2010; 362: 485-93
18) Tsai CW, Kuo CC, Wu CF, Chien KL, Wu VC, Chen MF, et al: Associations of renal vascular resistance with albuminuria in adolescents and young adults. Nephrol Dial Transplant, 2011; 26: 3943-9
19) Wei JN, Sung FC, Lin CC, Lin RS, Chiang CC, Chuang LM: National surveillance for type 2 diabetes mellitus in Taiwanese children. JAMA, 2003; 290: 1345-50
20) Lin CY, Lin LY, Wen TW, Lien GW, Chien KL, Hsu SH, et al: Association between levels of serum perfluorooctane sulfate and carotid artery intima-media thickness in adolescents and young adults. Int J Cardiol, 2013; 168: 3309-16 21) Su TC, Jeng JS, Chien KL, Sung FC, Hsu HC, Lee YT: Hypertension
community-based study in Taiwan. Stroke, 2001; 32: 2265-71 22) Su TC, Chien KL, Jeng JS, Chen MF, Hsu HC, Torng PL, et al: Age- and
gender-associated determinants of carotid intima–media thickness: a community-based study. J Atheroscler Thromb, 2012; 19: 872-80
23) Pignoli P, Tremoli E, Poli A, Oreste P, Paoletti R: Intimal plus medial thickness of the arterial wall: a direct measurement with ultrasound imaging. Circulation, 1986; 74: 1399-406
24) Wendelhag I, Liang Q, Gustavsson T, Wikstrand J: A new automated
computerized analyzing system simplifies readings and reduces the variability in ultrasound measurement of intima-media thickness. Stroke, 1997; 28: 2195-200 25) Wang Y, Ge K, Popkin BM: Tracking of body mass index from childhood to
adolescence: a 6-y follow-up study in China. Am J Clin Nutr, 2000; 72: 1018-24 26) Magnussen CG, Koskinen J, Juonala M, Chen W, Srinivasan SR, Sabin MA, et al:
A diagnosis of the metabolic syndrome in youth that resolves by adult life is associated with a normalization of high carotid intima-media thickness and type 2 diabetes mellitus risk: the Bogalusa heart and cardiovascular risk in young Finns studies. J Am Coll Cardiol, 2012; 60: 1631-9
27) Ebbeling CB, Pawlak DB, Ludwig DS: Childhood obesity: public-health crisis, common sense cure. Lancet, 2002; 360: 473-82
28) Wang Y, Beydoun MA: The obesity epidemic in the United States—gender, age, socioeconomic, racial/ethnic, and geographic characteristics: a systematic review and meta-regression analysis. Epidemiol Rev, 2007; 29; 6-28
29) Su TC, Bai CH, Chang HY, You SL, Chien KL, Chen HJ, et al: Evidence for improved control of hypertension in Taiwan: 1993-2002. J Hypertens, 2008; 26; 800-6
30) Lin CY, Lee HL, Chen YC, Lien GW, Lin LY, Wen LL, et al: Positive association between urinary levels of 8-hydroxydeoxyguanosine and the acrylamide metabolite N-acetyl-S-(propionamide)-cysteine in adolescents and young adults. J Hazard Mater, 2013; 261: 372-7
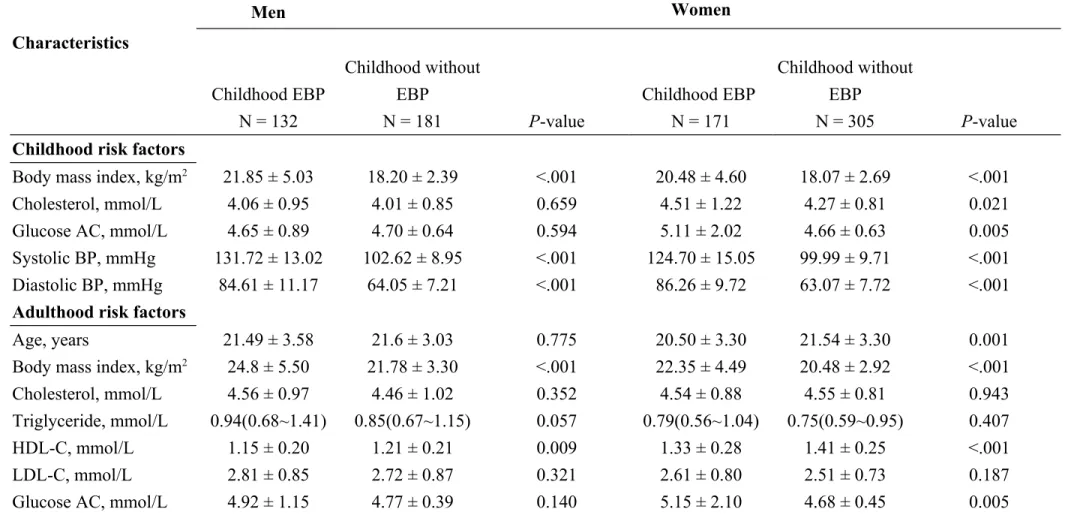
Table 1 Baseline characteristics between subjects with and without childhood elevated blood pressure (EBP) in the YOung Taiwanese Cohort (YOTA) study during 2006-2008
Men Women Characteristics Childhood EBP N = 132 Childhood without EBP N = 181 P-value Childhood EBP N = 171 Childhood without EBP N = 305 P-value
Childhood risk factors
Body mass index, kg/m2 21.85 ± 5.03 18.20 ± 2.39 <.001 20.48 ± 4.60 18.07 ± 2.69 <.001
Cholesterol, mmol/L 4.06 ± 0.95 4.01 ± 0.85 0.659 4.51 ± 1.22 4.27 ± 0.81 0.021
Glucose AC, mmol/L 4.65 ± 0.89 4.70 ± 0.64 0.594 5.11 ± 2.02 4.66 ± 0.63 0.005
Systolic BP, mmHg 131.72 ± 13.02 102.62 ± 8.95 <.001 124.70 ± 15.05 99.99 ± 9.71 <.001 Diastolic BP, mmHg 84.61 ± 11.17 64.05 ± 7.21 <.001 86.26 ± 9.72 63.07 ± 7.72 <.001 Adulthood risk factors
Age, years 21.49 ± 3.58 21.6 ± 3.03 0.775 20.50 ± 3.30 21.54 ± 3.30 0.001
Body mass index, kg/m2 24.8 ± 5.50 21.78 ± 3.30 <.001 22.35 ± 4.49 20.48 ± 2.92 <.001
Cholesterol, mmol/L 4.56 ± 0.97 4.46 ± 1.02 0.352 4.54 ± 0.88 4.55 ± 0.81 0.943
Triglyceride, mmol/L 0.94(0.68~1.41) 0.85(0.67~1.15) 0.057 0.79(0.56~1.04) 0.75(0.59~0.95) 0.407
HDL-C, mmol/L 1.15 ± 0.20 1.21 ± 0.21 0.009 1.33 ± 0.28 1.41 ± 0.25 <.001
LDL-C, mmol/L 2.81 ± 0.85 2.72 ± 0.87 0.321 2.61 ± 0.80 2.51 ± 0.73 0.187
Diabetes mellitus, % 1.52 0 0.097 3.51 0.66 0.020 Systolic BP, mmHg 120.45 ± 16.63 111.8 ± 11.88 <.001 105.56 ± 13.89 100.8 ± 10.13 <.001 Diastolic BP, mmHg 76.33 ± 13.13 68.17 ± 8.69 <.001 67.11 ± 11.30 62.08 ± 8.27 <.001 Hypertension, % 6.82 0.55 0.002 2.34 0.33 0.039 Smoking habit, % 18.94 26.52 0.117 4.68 7.54 0.225 Alcohol habit, % 8.33 18.78 0.009 4.68 5.57 0.674 Overweight, % 24.24 11.6 <.001 12.28 7.87 0.001 Obesity, % 24.24 7.73 <.001 12.28 3.61 <.001 Follow-up years 7.90 ± 1.95 8.54 ± 1.72 0.003 8.06 ± 2.08 9.00 ± 1.86 <.001
Data was presented with mean ± standard deviation for continuous variables and n (%) for binary variables. Level of triglycerides was presented with median (Q1-Q3)
Table 2 Carotid arteries intima-media thickness (IMT) according to adulthood body mass index (BMI) categories Adulthood BMI, kg/m2
Carotid IMT in mm < 21 21-24 24-27 ≥ 27 P-value
Locations n = 395 n = 218 n = 98 n = 78 ANOVA Trend
Men n = 110 n = 104 n = 53 n = 46 RCCA1 0.451 ± 0.053 0.463 ± 0.070 0.469 ± 0.053 0.506 ± 0.090 <.001 <.001 RCCA2 0.433 ± 0.057 0.442 ± 0.063 0.446 ± 0.049 0.473 ± 0.090 0.007 <.001 LCCA1 0.445 ± 0.056 0.455 ± 0.067 0.482 ± 0.070 0.500 ± 0.094 <.001 <.001 LCCA2 0.430 ± 0.101 0.443 ± 0.066 0.466 ± 0.070 0.489 ± 0.086 <.001 <.001 Bulb, Rt 0.443 ± 0.075 0.456 ± 0.060 0.462 ± 0.091 0.517 ± 0.139 <.001 <.001 Bulb, Lt 0.473 ± 0.127 0.471 ± 0.100 0.478 ± 0.079 0.507 ± 0.126 0.308 0.084 Internal carotid, Rt 0.409 ± 0.063 0.422 ± 0.070 0.438 ± 0.067 0.440 ± 0.081 0.025 0.005 Internal carotid, Lt 0.401 ± 0.065 0.424 ± 0.065 0.423 ± 0.064 0.447 ± 0.077 0.001 <.001 IMT, mean 0.436 ± 0.043 0.446 ± 0.046 0.458 ± 0.042 0.484 ± 0.076 <.001 <.001 Women n = 285 n = 114 n = 45 n = 32 RCCA1 0.443 ± 0.059 0.450 ± 0.052 0.448 ± 0.059 0.460 ± 0.070 0.407 0.165 RCCA2 0.435 ± 0.055 0.435 ± 0.058 0.452 ± 0.064 0.463 ± 0.082 0.023 0.003 LCCA1 0.434 ± 0.055 0.441 ± 0.056 0.446 ± 0.069 0.473 ± 0.084 0.005 <.001 LCCA2 0.429 ± 0.055 0.443 ± 0.052 0.458 ± 0.100 0.469 ± 0.091 <.001 <.001 Bulb, Rt 0.450 ± 0.119 0.460 ± 0.092 0.477 ± 0.162 0.510 ± 0.109 0.041 0.006 Bulb, Lt 0.449 ± 0.079 0.446 ± 0.073 0.462 ± 0.086 0.474 ± 0.086 0.251 0.057 Internal carotid, Rt 0.404 ± 0.060 0.404 ± 0.083 0.417 ± 0.092 0.441 ± 0.102 0.046 0.005
Internal carotid, Lt 0.387 ± 0.056 0.401 ± 0.070 0.405 ± 0.068 0.413 ± 0.056 0.024 0.028
IMT, mean 0.429 ± 0.041 0.435 ± 0.045 0.445 ± 0.067 0.460 ± 0.060 0.001 <.001
Abbreviations: CCA, common carotid artery; ICA, internal carotid artery; IMT mean = mean of IMT at 8 measured sites of carotid artery, include RCCA1, RCCA2, LCCA1, LCCA2, Bulb Rt, Bulb Lt, ICA Rt, and ICA Lt.
Figure Legends
Figure 1
Flowchart of participants’ recruitment based on with and without childhood elevated blood pressure (EBP) in the YOung TAiwanese Cohort (YOTA)Figure 2 Tracking of body mass index from childhood to adulthood with significant correlation with p value <.0001
Figure 3 Change of body mass index (BMI) between childhood and adulthood, and the risk for thicker carotid intima-media thickness
Data was shown by multivariate logistic regression analyses after controlling adulthood cardiovascular risk factors, including age, gender, systolic BP, fasting
glucose, cholesterol level, smoking and alcohol habit, and household income. P value: * <0.05, † <0.01, ‡ <0.001
Figure 4 Change of body mass index (BMI) between childhood and adulthood, and the risk for high blood pressure
Data was shown by multivariate logistic regression analyses after controlling adulthood cardiovascular risk factors, including age, gender, systolic BP, fasting
glucose, cholesterol level, smoking and alcohol habit, and household income. P value: * <0.05, † <0.01, ‡ <0.001