Kaohsiung J Med Sci August 2010 • Vol 26 • No 8 397 Quality of life (QOL) in patients with mental
disor-ders is an important issue when emphasizing a more consumer-oriented and holistic view of health care [1]. QOL is defined as the individuals’ perceptions of their life position in the context of the culture and value systems in which they live, and in relation to their goals, expectations, standards and concerns. QOL is a complex and broad-ranging concept, incorporating an individual’s physical health, psychological state, inde-pendence level, social relations, personal beliefs, and
relationship to salient features of the environment [2]. The concept of QOL differs from that of disability or impairment because different patients may react dif-ferently to similar levels of disability or impairment [3]. QOL has four uses in medicine: (1) for the plan-ning of clinical care of individual patients; (2) as an outcome measure in clinical trials and health services research; (3) to assess the health needs of populations; and (4) for resource allocation [4].
Obsessive-compulsive disorder (OCD) is a chronic illness associated with a high potential for disability [5,6]. OCD has a significant negative impact on pa-tients’ social and family relationships [7–9], marital relations [7,10], learning ability [9], occupational func-tion [7–9,11] and self-esteem [7,9], as well as increasing the risk of depression [8], suicidality [7], and alcohol and illicit drug abuse [7]. Previous studies have found Received: Jun 1, 2009 Accepted: Mar 2, 2010
Address correspondence and reprint requests to: Dr Yi-Chun Yeh, Department of Psychiatry, Kaohsiung Medical University Hospital, 100 Tzyou 1stRoad, Kaohsiung 80756, Taiwan. E-mail: [email protected]
Q
UALITY OF
L
IFE AND ITS
C
ORRELATES IN
P
ATIENTS
W
ITH
O
BSESSIVE
-
COMPULSIVE
D
ISORDER
Shu-Ying Hou,1Cheng-Fang Yen,2,3Mei-Feng Huang,4Peng-Wei Wang,4and Yi-Chun Yeh3
Departments of 1Nursing and 3Psychiatry, Kaohsiung Medical University Hospital, 2Department of Psychiatry, College of Medicine, Kaohsiung Medical University, and
4Department of Psychiatry, Kai-Suan Psychiatric Hospital, Kaohsiung, Taiwan.
The care of patients with obsessive-compulsive disorder (OCD) has raised quality of life (QOL) issues. The purpose of this study was to compare the level of QOL between patients with and without OCD, and to examine the associations between QOL and sociodemographic data, course of illness, psychopathology, perceived social support, and treatment characteristics. The QOL levels measured with the Taiwan version of the Short Form of the World Health Organization Questionnaire on Quality of Life were compared between 57 subjects with OCD and 106 subjects without OCD. The correlates of QOL were examined among subjects with OCD. The analysis revealed that QOL scores for the general, physical, psychological and social relationship domains were lower in the OCD group than in the control group; however, no difference in the environ-mental domain was found. Multiple factors were associated with poor QOL in subjects with OCD, including comorbid depression, severe obsession symptoms, perceived low social support, severe adverse effects of medication, combined use of mood stabilizers, and low social status. Different domains of QOL are differently affected by OCD. The QOL of subjects with OCD was correlated to multiple factors that were specific to individual subjects and influenced by interac-tions with treatment and the social environment.
Key Words:depression, obsessive–compulsive disorder, quality of life, social support (Kaohsiung J Med Sci 2010;26:397–407)
that QOL was worse among patients with OCD than in the general population [12], or patients with de-pressive disorders [12], heroin dependence [12], social phobia [13], panic disorder [13] and type 2 diabetes mellitus [8]. As assessing the impact of OCD on QOL is an important aid to make decisions on how aggres-sively the disorder should be treated for an outcome measure, for health needs assessments of patients and for resource allocation [4], further studies are needed to examine the correlates of QOL and to develop effective strategies to improve the QOL in patients with OCD.
To date, few studies have examined the factors that influence QOL in patients with OCD. Previous studies have found that severe OCD symptoms and comorbid depression were associated with poor QOL in patients with OCD [8,13]. Antidepressant treatment was also found to improve the QOL of OCD patients [8,14]. However, patients with anxiety disorders might per-ceive the adverse effects of antidepressants, which can result in low medical adherence [15]. Furthermore, the adverse effects of medications negatively impact on some QOL domains of patients with panic disor-ders [16], depressive disordisor-ders [17], bipolar disorder [18] and schizophrenia [18]. However, little is known about the impact of adverse effects of pharmacother-apy on QOL in patients with OCD. Although selective serotonin reuptake inhibitors are first-line medications and other antidepressants, e.g. clomipramine, seroto-nin norepinephrine reuptake inhibitors and mono-amine oxidase inhibitors are second-line medications for OCD, patients who have been unsuccessfully treated with several antidepressants are often asked to consider augmentation of selective serotonin reuptake inhibitors with an antipsychotic or a mood stabilizer [19]. The influence of augmentation by antipsychotics or mood stabilizers on the QOL of patients with OCD needs further studies.
Previous studies have found that social support can reduce the impact of chronic stress on psychological well-being [20] and improved QOL in patients with severe mental [21–23] and chronic medical illnesses [24,25]. However, the relationship between QOL and social support in patients with OCD is still unknown. Further studies are needed to examine the impact of sociodemographic characteristics and course of illness on QOL in patients with OCD.
The aims of this study were (1) to examine whether different domains of QOL are differently affected by
OCD by comparing the QOL of subjects with and without OCD; and (2) to examine the association of QOL with sociodemographic characteristics (sex, age, education level, marriage status, social status and attending religious activities), course of illness (onset age and duration of illness), psychopathology (sever-ities of depression, obsession and compulsion), per-ceived social support, and treatment characteristics (adverse effects of medication and variety of medica-tion) among subjects with OCD.
M
ETHODSSubjects
From February to November 2008, 65 patients with OCD were consecutively recruited from the outpatient psychiatric clinics at a medical center and a regional teaching hospital in Southern Taiwan. Of these, five patients (3 men and 2 women) refused to participate in this study. Of the 60 patients who agreed to join the study, 57 patients who had received medication for OCD in the preceding 2 weeks were included in the study; the three patients who did not receive medica-tion were not included. A psychiatrist systematically assessed all patients to confirm the diagnosis of OCD using the structured Mini-International Neuropsychia-tric Interview [26] based on the diagnostic schemes of the 4thedition of the Diagnostic and Statistical Manual of Mental Disorders [27].
To recruit subjects for the control group, we posted an advertisement in the hospital and in newspapers to invite participation. A total of 157 persons responded to the advertisement. A psychiatrist assessed all res-ponders systematically to determine whether they had any mood or psychotic disorders using the Mini-International Neuropsychiatric Interview [26]. Those who had OCD, mood disorders, psychotic disorders, drank alcohol more than once per month, used any illicit drugs or had low mentality were excluded. A total of 106 subjects conformed to the criteria and were recruited as the control group [18].
Survey instruments
World Health Organization Questionnaire on Quality of Life: Short Form–Taiwan version (the WHOQOL-BREF Taiwan version)
The WHOQOL-BREF Taiwan version assessed the overall rating of QOL (2 items) and four QOL domains,
including physical health (7 items), psychological (6 items), social relations (4 items) and environment (9 items) [28]. The transformed scores of the four QOL domains ranged from 4 to 20, and Cronbach’s α ranged from 0.69 to 0.84 in the present study. Higher scores on the WHOQOL-BREF Taiwan version indicate a higher perceived QOL in the preceding 2 weeks.
Yale-Brown Obsessive Compulsive Scale (Y-BOCS) Subjects underwent a semi-structured interview based on the 10-item Y-BOCS [29] to evaluate the severity of OCD symptoms in the preceding 2 weeks. Every item was rated on a 0–4 scale (0= none, 4 = extreme). Higher total scores of the first five and second five items indicate more severe obsessions and compul-sions, respectively. The Cronbach’s α was 0.86 for obsessions and 0.94 for compulsions in the present study.
Taiwanese version of the Beck Depression Inventory-II (BDI-II)
The BDI-II assesses the severity of depression [30], with a total score higher than 17 indicates a depres-sive tendency [31]. The Cronbach’s α of the Taiwanese version of the BDI-II in the present study was 0.92. Social Support Scale (SSS)
We used the SSS, as modified by Wang [32] from the Inventory of Socially Supportive Behavior developed by Barrera and Sandler [33]. Cronbach’s α for the SSS in the present study was 0.95 and the 1-week test–retest reliability was 0.92 (p< 0.001). Higher SSS scores indicate higher levels of perceived social support.
Questionnaire on Adverse Effects of Medication for Depression and Anxiety (QAEM-DA)
We developed the QAEM-DA, which contains 16 items, to evaluate the patients’ perceived adverse effects in-duced by antidepressants used to treat OCD in the preceding 2 weeks [34]. The positive items were summed to represent the total severity of adverse effects of medication. Cronbach’s α of the QAEM-DA in the present study was 0.79 and the 1-week test– retest reliability was 0.91 (p< 0.001). The QAEM-DA has been used to assess the adverse effects of antide-pressants in previous studies on patients with panic disorder [16] or depressive disorders [17] with satis-factory validity [16].
Social Status Rating Scale (SSRS)
The SSRS classifies subjects’ social status into classes I–V according to their education level and occupa-tion [35]. A high category on the SSRS indicates low social status.
Subject characteristics
We recorded the sex, age, education level and marital status of participants in the OCD and control groups. Religious observation, duration of illness, age at onset of OCD, clinical diagnosis of mood disorders recorded in medical charts, and type and dose of medication were also recorded for participants in the OCD group. Based on the results of the review by Fineberg and Craig [36], participants were divided into two groups. Subjects who received 60 mg/day of fluoxetine, 60 mg/ day of paroxetine, 150 mg/day of sertraline, 20 mg/day of escitalopram, 200 mg/day of fluvoxamine, 100 mg/ day of clomipramine, or 300 mg/day of venlafaxine, or more, were classified as the high-dose group, while subjects who received doses of these antidepressants lower than those stated above were classified as the low-dose group.
Protocol and statistical analysis
The protocol was approved by the Institutional Review Board of Kaohsiung Medical University. Informed consents were obtained from all subjects before start-ing the study. A researcher explained the methods to complete the questionnaires to each participant, and then the participants completed the questionnaires by themselves. Participants also underwent a semi-structured interview based on the Y-BOCS to evaluate the severity of OCD symptoms in preceding 2 weeks. Among subjects in the OCD and control groups, the influences of the diagnosis of OCD on the five QOL domains on the WHOQOL-BREF Taiwan version were examined using stepwise multiple linear regres-sion analyses controlling for sex, age, education level and marriage. The relationships between the five QOL domains on the WHOQOL-BREF Taiwan version and subjects’ sociodemographic data, current severity of OCD symptoms, BDI-II depression scores, perceived social support, clinical diagnosis of mood disorders, the type and doses of medications, and adverse effects of medications, were analyzed with t tests, analysis of variance and Pearson’s correlation. Because multi-ple comparisons were conducted, a two-tailed p value of < 0.005 was considered statistically significant.
The predictive potential of variables that were signifi-cantly associated with QOL in bivariate analyses was further examined using forward stepwise multiple linear regression analysis, and a two-tailed p value of < 0.05 was considered statistically significant.
R
ESULTSThe sociodemographic data, course of illness, psy-chopathology, perceived social support, level of QOL on the WHOQOL-BREF Taiwan version, and treat-ment characteristics are shown in Tables 1 and 2. After controlling for sex, age, education, and marriage, the OCD group had worse QOL in the general (β = –0.322, t = –4.097, p < 0.001), physical (β = –0.512, t=–7.350, p<0.001), psychological (β=–0.290, t=–3.704, p<0.001) and social relationships (β=–0.191, t=–2.495, p= 0.014) domains than the control group. However,
no difference was found between the two groups for the environmental domain (β=0.042, t = 0.517, p> 0.05). Tables 3 and 4 present the associations between the overall rating and the four QOL domains on the WHOQOL-BREF Taiwan version and subjects’ socio-demographic data, current severity of OCD symptoms, BDI-II depression scores, perceived social support, type and dose of medications, and adverse effects of medications analyzed with t tests, analysis of variance and Pearson’s correlation for the OCD group. The re-sults indicated that QOL was worse in the social rela-tionship and environment domains for subjects with low (class V) social status than those with higher social status (classes I–IV). Participants with significant de-pression (BDI-II≥ 17) had worse QOL in the general, physical, psychological, and environment domains compared with participants without significant de-pression (BDI-II < 17). Participants who received mood stabilizers had worse QOL in the psychological, social
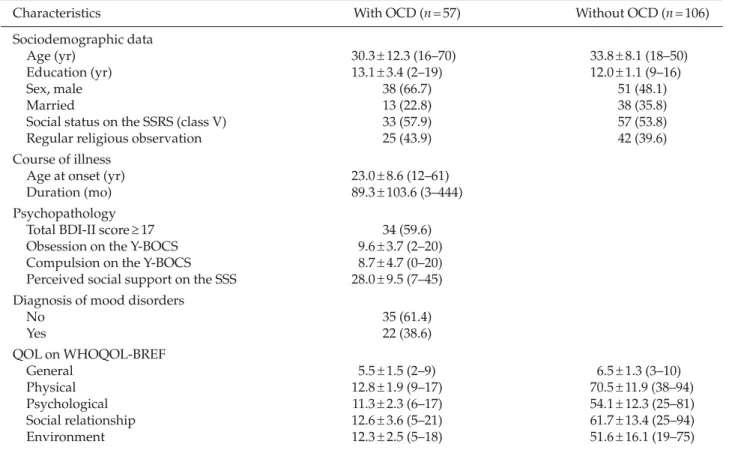
Table 1.Sociodemographic data, course of illness, psychopathology, perceived social support and the level of quality of life of OCD patients*
Characteristics With OCD (n= 57) Without OCD (n= 106)
Sociodemographic data
Age (yr) 30.3± 12.3 (16–70) 33.8± 8.1 (18–50)
Education (yr) 13.1± 3.4 (2–19) 12.0± 1.1 (9–16)
Sex, male 38 (66.7) 51 (48.1)
Married 13 (22.8) 38 (35.8)
Social status on the SSRS (class V) 33 (57.9) 57 (53.8)
Regular religious observation 25 (43.9) 42 (39.6)
Course of illness
Age at onset (yr) 23.0± 8.6 (12–61)
Duration (mo) 89.3± 103.6 (3–444)
Psychopathology
Total BDI-II score≥ 17 34 (59.6)
Obsession on the Y-BOCS 9.6± 3.7 (2–20)
Compulsion on the Y-BOCS 8.7± 4.7 (0–20)
Perceived social support on the SSS 28.0± 9.5 (7–45) Diagnosis of mood disorders
No 35 (61.4) Yes 22 (38.6) QOL on WHOQOL-BREF General 5.5± 1.5 (2–9) 6.5± 1.3 (3–10) Physical 12.8± 1.9 (9–17) 70.5± 11.9 (38–94) Psychological 11.3± 2.3 (6–17) 54.1± 12.3 (25–81) Social relationship 12.6± 3.6 (5–21) 61.7± 13.4 (25–94) Environment 12.3± 2.5 (5–18) 51.6± 16.1 (19–75)
*Data presented as mean± standard deviation (range) or n (%). OCD = Obsessive–compulsive disorder; SSRS = Social Status Rating Scale; BDI-II= Taiwanese version of the Beck Depression Inventory-II; Y-BOCS = Yale-Brown Obsessive–compulsive Scale; SSS= Social Support Scale; WHOQOL-BREF = World Health Organization Questionnaire on Quality of Life: Short Form–Taiwan Version; QOL= quality of life.
relationship and environment domains compared with participants who did not receive mood stabilizers. Severe obsession and compulsion symptoms and low social support were significantly associated with poor QOL in all five domains. Severe adverse effects of med-ications were significantly associated with poor QOL in the general, physical, psychological and environ-ment domains. Higher chlorpromazine equivalents of antipsychotics were significantly associated with poor QOL in the social relationship domains.
We further examined the predictive potential of variables in the OCD group that were significantly associated with QOL in bivariate analyses using step-wise multiple linear regression analyses. Total BDI-II scores ≥ 17 and severe current obsession symptoms were significantly associated with poor QOL in the general and physical domains (Table 5). Total BDI-II scores ≥ 17 and combined use of mood stabilizers were significantly associated with poor QOL in the psy-chological domain. Low social status, perceived low social support and combined use of mood stabilizers were significantly associated with poor QOL in the
social relationship domain. Total BDI-II scores ≥ 17, severe current obsession symptoms, perceived low social support, perceived severe adverse effects of medications and combined use of mood stabilizers were significantly associated with poor QOL in the environmental domain.
D
ISCUSSIONThis study found that patients with OCD had worse QOL on the general, physical, psychological and so-cial relationship domains compared with the control group, which shows that OCD negatively influenced the conditions that are essential for maintaining good QOL in these three domains. A previous study found that the general domain of the WHOQOL-BREF was positively correlated with serotonin transporter avail-ability in male healthy controls [37]. It was speculated that the scope of global perception of QOL may over-lap with the daily sense of perceived joy or happiness [37]. However, no difference in the environmental QOL domain was found between these two groups. The results of this study indicate that different domains of QOL are differently affected by OCD.
The present study found that comorbid depression, symptoms of obsession, low social status, perceived lack of social support, adverse effects of medication, and combined use of mood stabilizers were associated with poor QOL in some domains on the WHOQOL-BREF Taiwan version among patients with OCD. The results indicate that the QOL of patients with OCD is associated with multiple factors that are specific to individual subjects and is influenced by interactions with treatment and the social environment. These re-sults should encourage clinicians to screen for these factors and, if present, intervene to improve QOL in patients with OCD.
Consistent with the results of previous studies [8,13], the present study found that severe obsession symptoms and comorbid depression were associated with poor QOL in patients with OCD. This indicates that adequate treatment of OCD and the comorbid depressive symptoms is an important step towards im-proving QOL. On the other hand, this study also found that adverse effects of medications predicted poor QOL in the environment domain. Because OCD has a chronic course [5], a long-term treatment is necessary for many patients with OCD. Although several types Table 2.Treatment characteristics*
OCD group (n= 57) Adverse effects of medications 4.9± 3.8 (0–15) Augmentation of antipsychotic 23 (40.4) or mood stabilizers Type of antidepressants SSRI 42 (73.7) TCA 3 (5.3) SNRI 7 (12.2) SSRI+ TCA 5 (8.8) Antidepressant dose Low-dose 34 (59.6) High-dose 23 (40.4) Types of antipsychotics No antipsychotic 36 (63.2) Atypical 12 (21.0) Typical 9 (15.8)
Combined use of mood stabilizers
No 50 (87.7)
Yes 7 (12.3)
Chlorpromazine equivalents of 39.8± 73.0 (0–300) antipsychotic (mg/day)
*Data presented as mean± standard deviation (range) or n (%). OCD= Obsessive–compulsive disorder; SSRI = selective sero-tonin reuptake inhibitor; TCA=tricyclic antidepressant; SNRI = serotonin-norepinephrine reuptake inhibitor.
T
able 3.
Associations between quality of life on the W
orld Health Or
ganization Questionnair
e on Quality of Life: Short Form–T
aiwan versi
on and sociodemographic
and tr
eatment characteristics, and psychopathology
General Physical Psychological Social r elationships Envir onment Mean ± SD t or F * Mean ± SD t or F * Mean ± SD t or F * Mean ± SD t or F * Mean ± SD t or F * Sex Male 5.5 ± 1.5 0.10 12.8 ± 2.1 −0.15 1 1.2 ± 2.4 −0.36 12.0 ± 3.3 −1.74 12.2 ± 2.8 −0.47 Female 5.5 ± 1.5 12.8 ± 1.7 11.5 ± 2.2 13.7 ± 3.9 12.5 ± 2.2 Married No 5.5 ± 1.6 0.14 12.9 ± 2.2 0.30 1 1.3 ± 2.3 0.04 12.2 ± 3.7 −0.47 12.3 ± 2.4 0.04 Y es 5.4 ± 1.3 12.7 ± 1.9 11.3 ± 2.4 12.8 ± 3.6 12.3 ± 2.6 Regular r eligious observation Y es 5.6 ± 1.8 −0.68 12.8 ± 1.6 0.14 11.4 ± 1.9 0.30 12.9 ± 4.1 0.42 12.3 ± 2.2 −0.09 No 5.3 ± 1.1 12.8 ± 2.1 11.2 ± 2.6 12.5 ± 3.2 12.3 ± 2.8
Social status Class I–IV
6.0 ± 1.4 −2.36 13.5 ± 1.8 −2.62 12.0 ± 2.3 −2.05 14.2 ± 3.4 −3.22 † 13.3 ± 2.6 −2.75 † Class V 5.1 ± 1.6 12.3 ± 1.8 10.8 ± 2.2 11.4 ± 3.3 11.5 ± 2.1 BDI-II ≥ 17 Y es 4.8 ± 1.4 4.03 ‡ 12.0 ± 1.6 −4.42 ‡ 10.4 ± 1.9 −4.1 1 ‡ 11.9 ± 4.0 −1.77 11.1 ± 2.5 −4.89 ‡ No 6.3 ± 1.3 13.9 ± 1.8 12.6 ± 2.3 13.6 ± 2.8 13.9 ± 1.7
Diagnosis of mood disor
ders Y es 4.6 ± 1.6 2.33 12.5 ± 1.9 −0.98 10.9 ± 2.2 −1.15 12.0 ± 3.2 −1.10 11.4 ± 2.2 −2.08 No 5.7 ± 1.5 13.0 ± 1.9 11.6 ± 2.5 13.1 ± 3.9 12.9 ± 2.7 T ype of antidepr essant
medication used SSRI
5.7 ± 1.5 1.36 13.2 ± 2.0 1.80 11.6 ± 2.4 1.63 13.1 ± 3.5 0.90 12.7 ± 2.5 1.40 TCA 4.3 ± 1.5 12.2 ± 1.4 9.8 ± 2.8 10.7 ± 3.2 11.1 ± 3.5 SNRI 4.7 ± 1.6 11.8 ± 1.1 11.9 ± 2.3 12.4 ± 4.4 11.6 ± 2.5 SSRI + TCA 5.6 ± 1.5 11.7 ± 1.8 9.6 ± 1.6 10.8 ± 4.1 10.7 ± 2.7 Antidepr essant dose Low-dose 5.1 ± 1.4 −2.18 12.4 ± 2.0 −1.99 11.4 ± 2.5 0.15 12.3 ± 3.8 −0.92 11.9 ± 2.5 −1.27 High-dose 6.0 ± 1.6 13.4 ± 1.8 11.3 ± 2.2 13.2 ± 3.5 12.8 ± 2.7 T
ype of antipsychotic medication No antipsychotic
5.6 ± 1.7 0.25 12.9 ± 2.0 2.48 11.8 ± 2.2 3.32 13.5 ± 3.7 3.59 12.8 ± 2.5 4.65 Atypical 5.3 ± 1.4 11.9 ± 1.1 9.8 ± 1.8 10.4 ± 3.2 10.4 ± 1.7 T ypical 5.3 ± 1.3 13.9 ± 2.3 11.6 ± 3.1 12.2 ± 2.9 12.7 ± 2.8
Combined use of mood stabilizers No
5.5 ± 1.5 0.60 12.9 ± 1.9 1.31 11.7 ± 2.3 3.18 † 13.2 ± 3.5 3.15 † 12.7 ± 2.4 3.39 † Y es 5.1 ± 1.7 11.9 ± 2.0 8.9 ± 1.6 8.9 ± 2.9 9.5 ± 1.9 *Results of t
tests and analysis of variance;
†p < 0.005; ‡p < 0.001. SD = Standar d deviation; BDI-II = T
aiwanese version of the Beck Depr
ession Inventory-II; SSRI
=
selective ser
otonin
reuptake inhibitor; TCA
= tricyclic antidepr essant; SNRI = ser otonin-nor epinephrine r euptake inhibitor .
of antidepressants can improve OCD symptoms, the antidepressants have different levels of adverse effects on several organs and systems [38], which may com-promise patients’ QOL and thus reduce adherence to treatment [15]. The findings of this study indicate that clinicians must help patients with OCD to identify and to manage the adverse effects of therapy. Frequent discussions with patients may encourage them to con-tinue treatment and to accept the balance between the benefits and adverse effects of treatment.
This study also found that combined use of mood stabilizers was significantly associated with poor QOL in the psychological, social relationship and
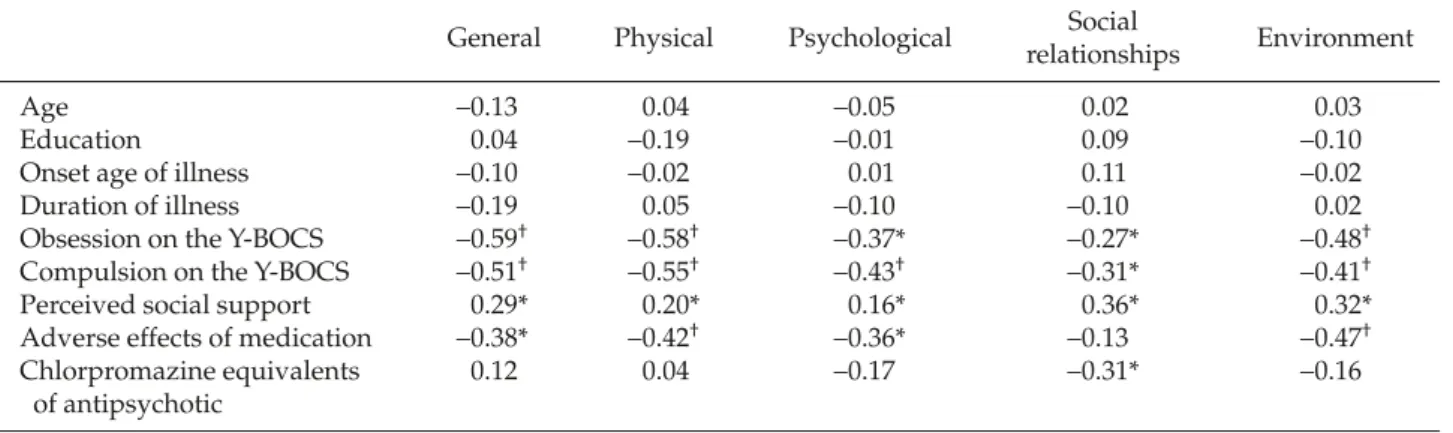
environmental domains. There are several possible explanations for these associations. First, mood stabi-lizers may be used for augmentation in patients with severe OCD symptoms and poor response to routine antidepressant treatment, and these severe OCD symptoms compromised their QOL. Second, mood stabilizers may be used to treat mood symptoms other than OCD symptoms. Although we did not find a difference in the level of QOL between those with and without a clinical diagnosis of mood disorders, it is possible that a diagnosis of mood disorders was not recorded in the patients’ charts and any unrecorded mood disorders may have compromised the level of Table 4.Pearson’s correlations analysis (r) between quality of life on the World Health Organization Questionnaire on Quality of Life: Short Form–Taiwan Version and sociodemographic and treatment characteristics, course of illness, psychopathology, and perceived social support
General Physical Psychological Social Environment
relationships
Age −0.13 0.04 −0.05 0.02 0.03
Education 0.04 −0.19 −0.01 0.09 −0.10
Onset age of illness −0.10 −0.02 0.01 0.11 −0.02
Duration of illness −0.19 0.05 −0.10 −0.10 0.02
Obsession on the Y-BOCS −0.59† −0.58† −0.37* −0.27* −0.48†
Compulsion on the Y-BOCS −0.51† −0.55† −0.43† −0.31* −0.41†
Perceived social support 0.29* 0.20* 0.16* 0.36* 0.32*
Adverse effects of medication −0.38* −0.42† −0.36* −0.13 −0.47†
Chlorpromazine equivalents 0.12 0.04 −0.17 −0.31* −0.16
of antipsychotic
*p< 0.005; †p< 0.001. Y-BOCS = Yale-Brown Obsessive–compulsive Scale.
Table 5.Variables associated with quality of life on the World Health Organization Questionnaire on Quality of Life: Short Form–Taiwan Version in stepwise multiple linear regression
General Physical Psychological Social Environment
relationships β t β t β t β t β t BDI-II≥ 17 –0.261 –2.212* –0.371 –3.257† –0.448 –4.068‡ –0.326 –3.004† Obsession on the –0.472 –3.995‡ –0.410 –3.593† –0.224 2.027* Y-BOCS Social status –0.229 –1.946* (class V) Perceived social 0.381 3.394† 0.245 2.385* support Adverse effects –0.287 –2.645* of medication Combined use of –0.348 –3.162† –0.369 –3.144† –0.396 –4.048‡ mood stabilizers Adjusted R2 0.385 0.425 0.329 0.341 0.491 F value 18.325‡ 21.675‡ 14.750‡ 10.660‡ 14.485‡
*p< 0.05; †p< 0.01; ‡p< 0.001. BDI-II = Taiwanese version of the Beck Depression Inventory-II; Y-BOCS = Yale-Brown Obsessive– compulsive Scale.
QOL. Third, mood stabilizers may have adverse effects that exert a negative effect on QOL. Because this study only evaluated the adverse effects of antidepressants, the association between QOL and the adverse effects of mood stabilizers needs further study.
Some studies have found that the QOL of some patients with OCD did not improve even with an im-provement in OCD symptoms due to medication [14, 39]. This suggests that there are factors other than OCD symptoms that influence QOL. The findings of this study indicate that low social support was asso-ciated with poor QOL in the social relationship and environment domains in patients with OCD. Of note, patients with OCD may show dysfunction in the areas of work inside the home and functioning as a family unit [7,9], which, ironically, may reduce sup-port from their families. To enhance family supsup-port and improve patients’ QOL, it may be helpful, with the patients’ permission, for clinicians to explain the characteristics of OCD and teach family members the skills necessary to help patients managing their OCD symptoms.
This study found that low social status was signif-icantly associated with poor QOL in the social rela-tionship domain. Because OCD has a negative impact on work ability and economic independence [7–9,11], the social status of patients with OCD may deterio-rate in the course of illness, leading to impaired QOL. The WHOQOL-BREF includes domains on life function critical to health-related QOL [40] and, as a generic scale, provides information that is compa-rable across patient groups and populations with different languages and cultures. Meanwhile, the WHOQOL BREF is a transcultural instrument with high face and construct validity within the specific cultural setting [41].
However, our results needed to be interpreted in light of several study limitations. First, the cross-sectional design of this study limited our ability to draw conclusions about the causal relationship between QOL and the associated factors. Second, analysis of a small sample of patients from mental health clinics may limit generalizations to other clinical units or populations. Some patients with OCD may receive no treatment or even inappropriate treatment. Third, although we examined a broad range of individual and environmental factors, some factors that may affect QOL in patients with OCD remain unmeasured. For example, the personality or coping style of the
participants and whether they received psychother-apy were not explicitly assessed in this study. Fourth, while QOL is an inherently subjective phenomenon, psychopathology may affect the mental, emotional and social judgments on which the patients’ responses to the QOL instruments are based [42]. No information from family members, friends or professionals was used to confirm the participants’ self-evaluation of the level of QOL in this study. Fifth, the psychological domain of the WHOQOL-BREF contains an item that inquires about negative feelings, including anxiety. For patients with OCD, it is difficult to find out whether a specific score on the psychological domain is due to a high level of anxiety or to poor QOL [43]. Several items of the WHOQOL-BREF inquire about depressive symptoms, which increases the association between QOL and total BDI-II scores.
In conclusion, the present study found that multi-ple factors, including adverse effects of medication, type of medication, social support, severity of obses-sion and depressive symptoms, and social status were associated with QOL in patients with OCD. The re-sults should encourage clinicians to screen for these factors and, if present, intervene to improve the QOL in patients with OCD.
A
CKNOWLEDGMENTSThis study was supported by a grant (KMUH 96-6G57) from Kaohsiung Medical University Hospital.
R
EFERENCES1. Stastney P, Amering M. Integrating consumer perspec-tives on quality of life in research and service planning. In: Katschnig H, Freeman H, Sartorius N, eds. Quality of
Life in Mental Disorders. West Sussex: John Wiley & Sons,
1997:261–9.
2. The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med 1998;28:551–8.
3. Fayers PM, Machin D. Quality of Life: Assessment, Analysis
and Interpretation. West Sussex: John Wiley & Sons,
2000.
4. Albrecht GL, Fitzpatrick R. A sociological perspective on health-related quality of life research. In: Albrecht GL, Fitzpatrick R, eds. Advances in Medical Sociology,
Vol. 5, Quality of Life in Health Care. London: Jai Press,
5. Rasmussen SA, Eisen JL. The epidemiology and differ-ential diagnosis of obsessive-compulsive disorder. J Clin
Psychiatry 1992;53:4–10.
6. World Health Organization. The “Newly Defined” Burden of
Mental Problems. Fact Sheets No. 217. Geneva: WHO, 1999.
7. Hollander E. Obsessive-compulsive disorder: the hid-den epidemic. J Clin Psychiatry 1997;58(Suppl 12):3–6. 8. Koran LM, McElroy SL, Davidson JR, et al. Fluvoxamine
versus clomipramine for obsessive-compulsive disorder: a double-blind comparison. J Clin Psychopharmacol 1996; 16:121–9.
9. Stein DJ, Roberts M, Hollander E, et al. Quality of life and pharmaco-economic aspects of obsessive-compulsive disorder. A South African survey. S Afr Med J 1996; 86(Suppl12):1582–5.
10. Stecketee G. Social support and treatment outcome of obsessive-compulsive disorder at 9-month follow-up.
Behav Psychother 1993;21:81.
11. Leon AC, Portera L, Weissman MM. The social costs of anxiety disorders. Br J Psychiatry 1995;27:19–22. 12. Bobes J, Gonzalez MP, Bascaran MT, et al. Quality of life
and disability in patients with obsessive-compulsive disorder. Eur Psychiatry 2001;16:239–45.
13. Lochner C, Mogotsi M, du Toit PL, et al. Quality of life in anxiety disorders: a comparison of obsessive-compulsive disorder, social anxiety disorder, and panic disorder.
Psychopathology 2003;36:255–62.
14. Tenney NH, Denys DA, van Megen HJ, et al. Effect of a pharmacological intervention on quality of life in patients with obsessive-compulsive disorder. Int Clin
Psychopharmacol 2003;18:29–33.
15. Nesse RM, Zamorski MA. Anxiety disorders in pri-mary care. In Knespar DJ, Riba MB, Schwenk TL, eds.
Primary Care Psychiatry. Philadelphia: Saunders, 1997:
132–62.
16. Yen CF, Kuo CY, Tsai PT, et al. Correlations of quality of life with adverse effects of medication, social support, course of illness, psychopathology, and demographic characteristics in patients with panic disorder. Depress
Anxiety 2007;24:563–70.
17. Yen CF, Chen CC, Lee Y, et al. Association between qual-ity of life and self-stigma, insight, and adverse effects of medication in patients with depressive disorders.
Eur Psychiatry 2010;22(Suppl 1):S24–89.
18. Yen CF, Cheng CP, Huang CF, et al. Quality of life and its association with insight, adverse effects of medication and use of atypical antipsychotics in patients with bipo-lar disorder and schizophrenia in remission. Bipobipo-lar
Disord 2008;10:617–24.
19. Stahl SM. Anxiety disorders and anxiolytics. In: Stahl SM, ed. Neuroscientific Basis and Practical Applications, 3rd edition. New York: Cambridge University Press,
2008:721–72.
20. Doeglas DM, Suurmeijer TP, van den Heuvel WJ, et al. Functional ability, social support, and depression in rheumatoid arthritis. Qual Life Res 2004;13:1053–65.
21. Hansson L, Middelboe T, Merinder L, et al. Predictors of subjective quality of life in schizophrenic patients living in the community. A Nordic multicentre study.
Int J Soc Psychiatry 1999;45:247–58.
22. Koivumaa-Honkanen HT, Viinamaki H, Honkanen R, et al. Correlates of life satisfaction among psychiatric patients. Acta Psychiatr Scand 1996;94:372–8.
23. Yanos PT, Rosenfield S, Horwitz AV. Negative and sup-portive social interactions and quality of life among per-sons diagnosed with severe mental illness. Community
Ment Health J 2001;37:405–19.
24. Jaracz K, Kozubski W. Quality of life in stroke patients.
Acta Neurol Scand 2003;107:324–9.
25. Yen CF, Tsai JJ, Lu PL, et al. Quality of life and its corre-lates in HIV/AIDS male outpatients receiving highly active antiretroviral therapy in Taiwan. Psychiatry Clin
Neurosci 2004;58:501–6.
26. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (MINI): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin
Psychiatry 1998;59(Suppl 20):34–57.
27. American Psychiatric Association. Diagnostic and
Statis-tical Manual of Mental Disorders, 4thedition. Washington
DC: American Psychiatric Association, 1994.
28. Yao G, Chung CW, Yu CF, et al. Development and veri-fication of validity and reliability of the WHOQOL-BREF Taiwan version. J Formos Med Assoc 2002;101: 342–51.
29. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Arch Gen Psychiatry 1989;46:1006–11. 30. Beck AT, Steer RA, Brown GK. Manual for the Beck
Depres-sion Inventory-II. San Antonio: Psychological Corporation,
1996.
31. Lu ML, Che HH, Chang SW, et al. Reliability and validity of the Chinese version of the Beck Depression Inventory-II. Taiwanese J Psychiatry 2002;16:301–10. 32. Wang YH. Study on life quality and its associated
fac-tors of rheumatoid arthritis patients. J Chang Gung Inst
Technol 1999;2:108–20.
33. Barrera M, Sandler I. Preliminary development of a scale of social support: studies on college students.
Am J Community Psychol 1981;9:435–47.
34. Gorman J, Shear K, Cowley D, et al. Treatment of patients with panic disorder. In: McIntyre JS, Charles SC, eds. Practice Guidelines for the Treatment of
Psychi-atric Disorders. Washington DC: American PsychiPsychi-atric
Association, 2002:635–96.
35. Rin H, Schooler C, Caudill WA. Symptomatology and hospitalization. Culture, social structure and psycho-pathology in Taiwan and Japan. J Nerv Ment Dis 1973; 157:296–312.
36. Fineberg NA, Craig KJ. Pharmacotherapy for obsessive-compulsive disorder. In: Stein DJ, Hollander E, Rothbaum BO, eds. Textbook of Anxiety Disorders, 2nd edition.
Washington DC: American Psychiatric Publishing, Inc, 2010: 311–37.
37. Tsai HC, Yeh TL, Hsieh MH, et al. Association between serotonin transporter availability and overall rating scores of quality of life in healthy volunteers.
Prog Neuropsychopharmacol Biol Psychiatry 2009;33:
711–4.
38. Taylor D, Paton C, Kerwin R. The South London and
Maudsley NHS Trust & Oxleas NHS Trust: 2005–2006 Prescribing Guidelines. London: Taylor & Francis,
2005:135–204.
39. Bystritsky A, Saxena S, Maidment K, et al. Quality-of-life changes among patients with obsessive-compulsive disorder in a partial hospitalization program. Psychiatr
Serv 1999;50:412–4.
40. Shumaker SA, Ellis S, Naughton M. Assessing health-related quality of life in HIV disease: key measurement issues. Qual Life Res 1997;6:475–80.
41. Berlim MT, Pavanello DP, Caldieraro MAK, et al. Reli-ability and validity of the WHOQOL BREF in a sample of Brazilian outpatients with major depression. Qual
Life Res 2005;14:561–4.
42. Atkinson M, Zibin S, Chuang H. Characterizing quality of life among patients with chronic mental illness: a critical examination of the self-report methodology.
Am J Psychiatry 1997;154:99–105.
43. Katschnig H. How useful is the concept of quality of life in psychiatry? In: Katschnig H, Freeman H, Sartorius N, eds. Quality of Life in Mental Disorders. West Sussex: John Wiley & Sons, 1997:3–16.
收文日期: 98 年 6 月 1 日 接受刊載: 99 年 3 月 2 日 通訊作者:葉怡君醫師 高雄醫學大學附設醫院精神科 高雄市三民區自由一路 100 號