Su-Fei Huang et al. Fall-Related Injuries 163
Journal of Research in Education Sciences 2018, 63(2), 163-186
doi:10.6209/JORIES.201806_63(2).0007
Effects of Fall Prevention Programs for Older
Adults on Fall-Related Injuries: A Systematic
Review and Meta-Analysis
Su-Fei Huang
Ting-Ting Yang
Shueh-Fen Chen
Department of Senior Citizen Service, Mackay Junior College of Medicine,
Nursing, and Management
Wisdom Distribution Service Corporation Department of Senior Citizen Care and Welfare,
Ching Kuo Institute of Management & Health
Li-Ting Lu
Jung-Yu Liao
Department of Health Management for Elderly Society, University of Kang Ning
Department of Tourism and Leisure Management, Vanung University
Abstract
This study aimed to evaluate the effects of fall prevention programs on fall-related injuries, and the characteristics of these programs. The Cochrane Library, Medline, PubMed, PsycARTICLES, PsycINFO, ERIC, AgeLine, CINAHL, Psychology and Behavioral Sciences Collection databases were searched for randomized clinical trials on fall-related injuries among older adults from 1996 to 2016. A meta-analysis was performed to calculate the combined effects of fall prevention programs on fall-related injuries. A total of 33 research papers were included in the meta-analysis (68,736 participants). The meta-analysis found that fall prevention programs had a significant effect in preventing fall-related injuries (OR=0.86, 95% CI: 0.75-0.97), but a borderline-significant effect in preventing fractures (OR=0.80, 95% CI: 0.63-1.03). The fall prevention programs had a significant effect on fall-related injuries when both male and female participants were included in the study sample, interventions involved healthcare professionals, more than 20% of the patient population had a history of falling, interventions occurred in the community setting, and multiple interventions were used. Thus, fall prevention programs had a small but significant effect in preventing fall-related injuries but only a borderline effect in preventing fractures. When planning fall prevention programs,
Corresponding Author: Jung-Yu Liao, E-mail: [email protected]
164 Fall-Related Injuries Su-Fei Huang et al.
future policy makers and clinical workers should consider the different characteristics of older adults to propose appropriate intervention programs.
Su-Fei Huang et al. Fall-Related Injuries 165
Introduction
Every year, approximately 28%-35% of elderly people aged 65 years or older experience falls; for those older than 70 years, the incidence of falls increases to 32%-42% (World Health Organization, 2008). In the United States (U.S.), an estimated 3.2 million elderly individuals aged 65 years and above experienced falls annually, i.e., an incidence of 32.3%. From 2004 to 2013, the number of elderly women increased by 4% each year, with the incidence of falls being the highest in women above 75 years of age (Verma et al., 2016). Approximately 10%-31% of older adults who experience falls suffer from a fall-related injury annually (Alexander, Rivara, & Wolf, 1992; Gill, Murphy, Gahbauer, & Allore, 2013; Stevens, Mack, Paulozzi, & Ballesteros, 2008). It is similar in Taiwan that 21% of older adults experience falls in the past year and one third of them suffer from a fall-related injury (Ministry of Health and Welfare, 2014).
There are numerous factors that increase falls in the elderly, and many researchers have developed preventive strategies against various risk factors. Some studies have concluded that intervention programs are ineffective (Vind, Andersen, Pedersen, Jørgensen, & Schwarz, 2009), but results from meta-analyses have found that intervention programs can effectively reduce the incidence of falls in elderly people. Gillespie et al. (2009) found no significant decrease in the risk of falls and fractures after participants completed a fall prevention program. However, El-Khoury, Cassou, Charles, and Dargent-Molina (2013) found that fall prevention programs successfully reduced fall-related injuries. The findings of previous meta-analyses are inconsistent. In addition, Gillespie et al.s’ study was published eight years ago, in 2009. Hence, there is a need to conduct another meta-analysis to explore the summary effects.
Currently, most meta-analyses have focused on analyzing the effectiveness of fall prevention programs for the elderly on the incidence of falls and recurrent falls. Few studies have analyzed the effects of fall prevention programs on fall-related injuries in the elderly.
In this study, the definition of fall-related injury included bruising, sprains, cuts, abrasions, as well as serious injuries, such as lacerations, skin lacerations requiring suturing, and head injuries (Baranzini et al., 2009; Elley et al., 2008). Fractures are both the most frequent and most expensive type of non-fatal injuries that occur (Stevens, Corso, Finkelstein, & Miller, 2006). This is a critical concern, as fractures not only increase the burden of care, but also incur large medical expenses (Hartholt et al., 2011; Hoffman, Hays, Shapiro, Wallace, & Ettner, 2017). Thus, we analyzed fractures and fall-related injuries separately. Here we conducted a meta-analysis to investigate the effectiveness of fall prevention programs for the older adults in preventing fall-related injuries.
166 Fall-Related Injuries Su-Fei Huang et al.
Fall-related injuries were divided into two categories: overall injury and fractures.
Methods
Literature search
The study collected English language papers on fall prevention programs from 1996 to 2016. Electronic journal databases, including Cochrane Library, Medline, PubMed, PsycARTICLES, PsycINFO, ERIC, AgeLine, CINAHL, Psychology and Behavioral Sciences Collection databases were searched. The following Medical Subject Headings (MeSH) subject terms and keywords were used: “fall,” “elderly,” “injury,” “prevention program,” or “intervention.” Google Scholar was used as a supplement for these databases to search for possible omissions. Additionally, we reviewed the bibliography of collected articles to identify those that were missing from the electronic databases.
Study selection
The study eligibility criteria were as follows: (a) English language papers from 1996 to June, 2016; (b) studies with participants who were older adults aged 65 years and above; (c) studies with statistical data about injury due to falls after intervention; (d) randomized control trials (RCTs) on fall prevention interventions (with single or multiple interventions); and (e) used quantitative and statistical methods to calculate the effect size.
The exclusion criteria included: Lack of fall-related injury data, age <65 years, lack of quantitative data, not an RCT, not enough statistic value to calculate odds ratio (OR), and studies with the same sample. Single-arm studies, systematic reviews, retrospective reviews, meta-analysis, and repeat publications were also not included in the present analysis.
Methodological quality assessment
Followed the recommendations of the Cochrane Collaboration (Higgins et al., 2011) and the prior study (El-Khoury et al., 2013), we assessed risk of bias in domains that were most important in the study: random sequence generation (selection bias), allocation concealment (selection bias), blinding of the assessment of fall-related injury and fracture (detection bias), incomplete outcome data (attrition bias), and recall bias (over three month). We then judged each trial as a whole to ascertain whether there was low, unclear, or high risk of bias, based on whether the level of bias in each of the defined domains could have led to material biases in the risk estimates. Two authors (SFH, TTY) independently assessed the risks of bias and extracted data. Disagreements were
Su-Fei Huang et al. Fall-Related Injuries 167
resolved by a third party (SFC).
Data extraction
To ensure the quality of the studies and conformance to the study topic, studies selected from the first screening step were read by two experienced authors, who then carried out a second step for selection and analysis based on the data extraction format. Minor discrepancies were resolved by group discussion until all members of research team agreed on the coding of characteristics.
The data extracted in the study included: study quality, sample characteristics (gender, age, history of falls), intervention characteristics (site of intervention, method, whether interveners were healthcare professionals), and types of fall-related injuries (related injury, fracture) (Table 1).
Data synthesis and analysis
We used comprehensive meta-analysis (version 3, Biostat, Englewood, NJ, USA) software to calculate the OR and associated 95% confidence interval (CI) for fall-related injury after fall prevention interventions. The formula for calculating effect sizes was:
OR = Exp (LogOR) (LogOR = Log (A × D) (B × C))
For experimental group data across studies, the number of injuries was designated as A and the number of non-injuries, as B. For control group data across studies, the number of fall-related injuries/fractures was designated as C and the number of non-injuries/non-fractures, as D.
Borenstein, Hedges, Higgins, and Rothstein (2009) indicated that the random-effects model could allow the true effect to vary among studies. Because of the diverse interventions across reviewed studies, we selected the random effects model to determine the OR and associated 95% CI of the combined effect size for fall-related injuries after fall interventions; a p-value < .05 was determined as the cutoff for statistical significance. Q values and I2 were used for heterogeneity testing.
We also did subgroup analyses to assess the influence of fall prevention programs on effect estimates: (a) participant characteristic: gender (both, female), fall history (< 20% vs. ≥ 20%); (b) intervention characteristic: site (community, facility, both), intervention (single, multiple), health professional involved (yes, no/undefined). We also did subgroup analyses to assess the influence of fall prevention programs on effect estimates and used Cochran’s Q statistic to test for subgroup interactions. Due to the heterogeneity of the data acquired, the DerSimonian and Laird (1986) random effects model was utilized. In order to measure heterogeneity, the I2 statistic was used and scores of 25%, 50%, and 75% were considered low, moderate, and high heterogeneity, respectively
170 Fall-Related Injuries Su-Fei Huang et al.
(Higgins, Thompson, Deeks, & Altman, 2003).
Results
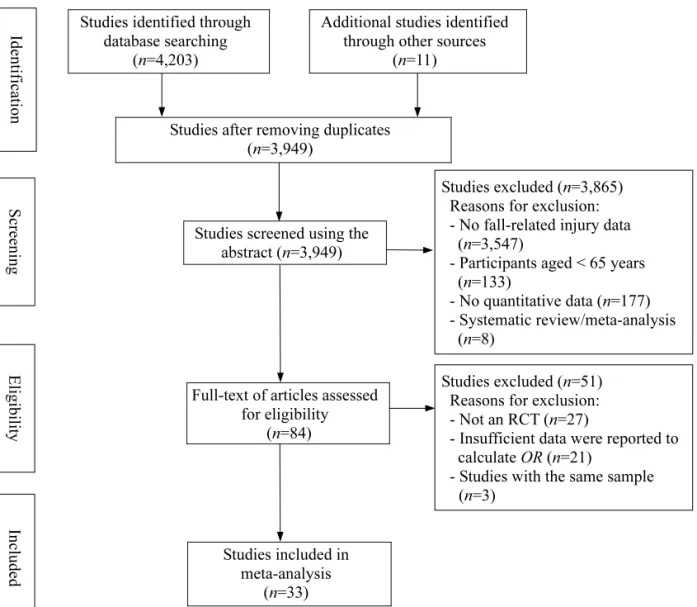
Database searches identified 4,203 studies, and after reading the title and abstract, 3,934 studies were excluded for repeated publication, lack of statistical data on injury, and participants below 65 years. In total, 269 studies met the eligibility criteria. Further exclusion was carried out to exclude papers with no quantitative data (n=177), systematic reviews or meta-analysis (n=8), lack of control group or non-comparative study (n=27), insufficient data were reported to calculate OR (n=21), and studies with the same author and samples (n=3). A total of 33 papers were included in the meta-analysis (Figure 1).
Figure 1. Flow Diagram of the Study Selection Process Studies screened using the
abstract (n=3,949) Studies included in meta-analysis (n=33) Identification Screening Eligibility Included Studies excluded (n=3,865) Reasons for exclusion: - No fall-related injury data
(n=3,547)
- Participants aged < 65 years (n=133)
- No quantitative data (n=177) - Systematic review/meta-analysis
(n=8)
Studies excluded (n=51) Reasons for exclusion: - Not an RCT (n=27)
- Insufficient data were reported to calculate OR (n=21)
- Studies with the same sample (n=3)
Studies identified through database searching
(n=4,203)
Additional studies identified through other sources
(n=11)
Full-text of articles assessed for eligibility
(n=84)
Studies after removing duplicates (n=3,949)
Su-Fei Huang et al. Fall-Related Injuries 171
Characteristics of included studies and injurious falls
Thirty-three studies were included in the effect size analysis, with 68,736 participants from 11 countries. Sample sizes in individual studies ranged from 50 to 46,245 participants. Characteristics of the included studies are presented in Table 1.
In addition, the types of fall-related injuries were diverse. In reviewed studies, 14 (42.42%) reported fall-related injuries and fractures caused by falls, while 19 studies (57.58%) only described the patients who experienced fall-related injuries.
Based on the suggestion of Coe (2002), the normal distribution of effect sizes for meta-analysis was an issue that needed to be addressed. We found that the value of kurtosis of 33 effect sizes was 3.724. A value of kurtosis within the range -2 to +2 is considered acceptable for normal univariate distribution (George & Malley, 2010). After deleting the effect size of two studies (No. 9 and No. 27), which were the outliers on the both sides of the scattered plot, the value of kurtosis of 31 effect sizes decreased to 0.464 that indicated that the normal distribution was acceptable. Based on this rationale, we would like to present the meta-analyses consisting of 33 and 31 studies, respectively.
Methodological quality
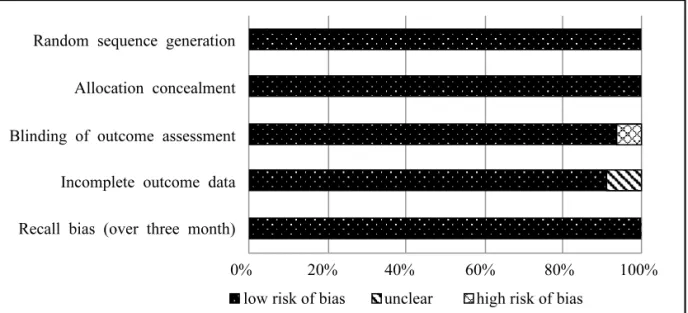
The assessments of risk of bias yielded of the reviewed studies indicated excellent quality. As shown in Figure 2, all trials of reviewed studies (33/33) were at low risk of bias for sequence generation, 100% (33/33) at low allocation concealment, 93.94% (31/33) at low detection bias, 90.91% (30/33) at low attrition bias, and 96.97% (32/33) at low recall bias, respectively.
Figure 2. Methodological Quality Graph: Review of Authors’ Judgments About Each Methodological Quality Item Presented as Percentages Across All Included Studies
Random sequence generation
Recall bias (over three month) Incomplete outcome data Blinding of outcome assessment Allocation concealment
0% 20% 40% 60% 80% 100%
172 Fall-Related Injuries Su-Fei Huang et al.
Effect of fall prevention programs on fall-related injury
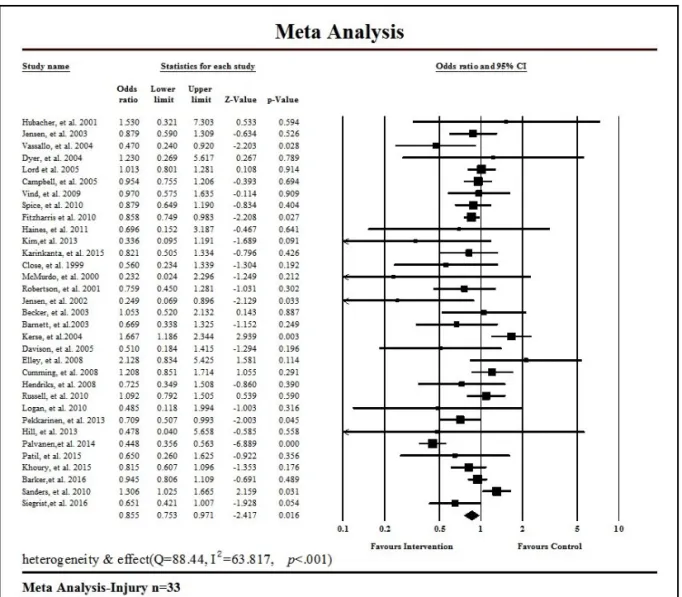
Regarding fall-related injuries, 33 effect sizes were included in the analysis, with a combined effect size of OR=0.86 (95% CI: 0.75-0.97, Z=-2.42, p= .016) (Figure 3), indicating that fall prevention programs had a significant effect in decreasing fall-related injuries. Heterogeneity testing found a Q value of 88.44 (p < .001), indicating that diversity in these 33 effect sizes were greater than that attributable to sampling error and were not homogeneous, with medium to large heterogeneity (I2 = 63.817).
Figure 3. Pooled OR, 95% CI, Z-values, and p-values of Each Study Presented by Forest Plot from the Meta-Analysis of Interventions on a Number of Fall-Related Injuries
After the exclusion of outliers, 31 effect sizes were included for sensitivity analysis, with an overall effect size of OR=0.90 (95% CI: 0.82-0.98, Z=-2.41, p= .016), indicating that fall prevention programs had a significant effect in preventing fall-related injuries. Heterogeneity testing found a Q
Su-Fei Huang et al. Fall-Related Injuries 173
value of 40.39 (p= .098), indicating that these 31 effect sizes were not heterogeneous and were of low heterogeneity (I2=25.72).
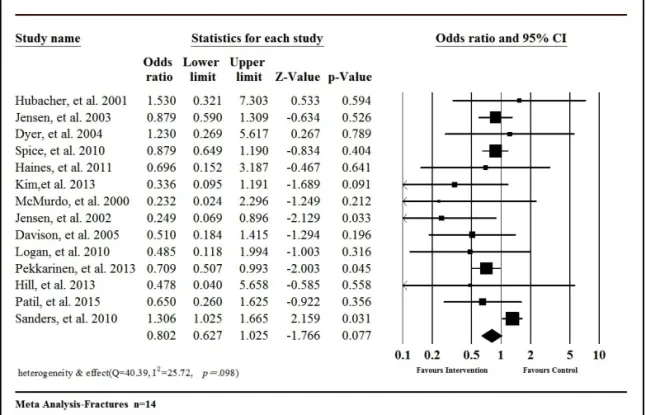
In the analysis of effect size of fall prevention programs on preventing fractures, 14 studies were included in the analysis, with a combined effect size of OR=0.92 (95% CI: 0.80-1.06, Z=-1.14, p= .254) (Figure 4), showing that fall prevention programs had no significant effect in preventing fractures. The heterogeneity testing indicates these 14 effect sizes were homogenous.
After excluding the two outliers, 12 studies were included in the analysis, with an effect size of OR=0.80 (95% CI: 0.63-1.03, Z=-1.77, p= .077), showing that fall prevention programs had a borderline-significant effects on preventing fractures. Heterogeneity testing found a Q value of 21.86, (p= .058), with low to medium heterogeneity (I2=40.54).
In the analysis of the results of various characteristics and fall-related injuries, 31 studies were included. The differences in effect sizes of the moderators in fall-related injuries were: sample including both male and female participants (OR=0.90, 95% CI: 0.84-0.97, p= .006), participants’ falling history ≥20% (OR=0.88, 95% CI: 0.79-0.97, p= .008), intervention site was in the community (OR=0.90, 95% CI: 0.84-1.00, p= .010), multiple interventions (OR=0.90, 95% CI: 0.83-0.96, p= .003), and interventions involved healthcare professionals (OR=0.91, 95% CI: 0.84-0.99, p= .022) (Table 2).
Figure 4. Pooled OR, 95% CI, Z-values, and p-values of Each Study Presented by Forest Plot from the Meta-Analysis of Interventions on Number of Fractures
Su-Fei Huang et al. Fall-Related Injuries 175
Discussion
In the present review, we pooled the effects of 33 RCTs to examine the overall effect of fall prevention interventions on fall-related injuries. The quality of reviewed studies was at low risk in several types of bias based on the recommendations of the Cochrane Collaboration. We found that a fall prevention intervention had a positive effect on fall-related injuries, but its effect on fracture injuries was borderline-significant. In addition, subgroup analyses indicate that the moderators include gender, participants’ falling history, intervention site, multiple interventions, and interventions involving healthcare professionals.
Here we presented a meta-analysis that showed that fall prevention programs for older participants had a significant positive effect in preventing fall-related injuries, although the effect size was small. Gates, Fisher, Cooke, Carter, and Lamb (2008) carried out a meta-analysis on the effects of multiple evaluations and interventions on older adults from the community and emergency care in preventing fall-related injuries; the results showed that fall prevention interventions had no significant effects in preventing related injuries, in contrast to the results of the study. It could be due to the limited number of studies included in the Gate’s meta-analysis (Gates et al., 2008) (n=8). The meta-analysis of El-Khoury et al. (2013) found that exercise interventions could reduce all types of fall-related injuries in community-dwelling older adults, which is similar to that of ours. There are multiple predisposing factors for fractures resulting from falls. El-Khoury et al. (2013) who also found that exercise interventions could significantly decrease the rate of fractures in community-dwelling older adults (pooled effect of 0.39, 95% CI: 0.23-0.66, I2=0, six studies). Oliver et al. (2007) found that multiple interventions in hospitals and care homes did not show any significant preventive effects on falls resulting in fractures (RR=0.59, 95% CI: 0.22-1.58, 13 studies, and RR=0.91, 95% CI: 0.54-1.53, 8 studies). The combined effect size was also small, which could be due to the small number of studies. Our findings were similar to that of the study conducted by Oliver et al. (2007), even if we included the 14 studies to be reviewed.
Stevens and Sogolow (2005) found that elderly patients who had non-fatal fall-related injuries and who were sent for medical treatment consisted mostly of women. Fractures were the most commonly observed injuries. Women had a higher incidence of two or more prior fractures or limb injuries as compared to men. Therefore, they recommended that fall intervention programs should consider gender differences. Heesch, Byles, and Brown (2008) investigated the association between falls and physical activity in 8,188 community-dwelling elderly women. Their results showed that
176 Fall-Related Injuries Su-Fei Huang et al.
people with higher physical activity had a lower possibility of incurring a fracture within 6 years (OR=0.53, 95% CI: 0.34-0.83, p= .01). Clemson et al. (2004) carried out a fall prevention program applying multiple interventions on community-dwelling elderly who had experienced a fall in the past year. Results showed that both genders had a 31% reduction in falls (RR=0.69, 95% CI: 0.50-0.96, p= .025), with a 68% reduction in falls in men only (RR=0.32, 95% CI: 0.17-0.59, p= .003). In addition, the meta-analysis (n=4) performed by Robertson, Campbell, Gardner, and Devlin (2002) found that exercise interventions could reduce 35% of falls and fall-related injuries, with similar effects between both genders. The gender effects in the reduction of fall-related injuries of fall prevention programs still were not consistent across previous studies. Findings from our meta-analysis indicate that the subgroup with both genders presented a significant effect on fall-related injuries, but this was not the case with the subgroup of only female participants, and this revealed the differences on reduction effects on fall-related injuries between both genders. The inconsistency in the findings of studies suggests that the protective effects of intervention of fall prevention on injury will be different depending on the gender and the type of intervention program.
Chang et al. (2004) pointed out that implementing a multiple fall prevention program would be most feasible by targeting selected participants, such as those with a history of falls. The meta-analysis found study participants with a history of falls ≥ 20% who had undergone fall prevention programs showed an improvement in fall-related injuries. Hence, older participants who have experienced falls should be encouraged to participate in fall prevention programs.
The intervention sites were classified into community and institution. Fall preventive interventions conducted in the community showed a significant effect in reducing related injuries, as compared to those conducted in institutions. However, the comparison of fall incidence in the community versus institutions for older adults may be biased because of different health status, age, and physical functions. Further studies are needed to more deeply assess the effectiveness of preventive effects on fall-related injuries among institutionalized older adults.
Goodwin et al. (2014) conducted a meta-analysis (n=17), showing that multiple interventions could help reduce the number of individuals who fell (RR=0.85, 95% CI: 0.80-0.91) and the incidence of falls (RR=0.80, 95% CI: 0.72-0.89). Campbell and Robertson (2007) also pointed out that multiple interventions were effective in reducing falls, regardless of whether the intervention was targeted at individuals or communities. Our findings also suggest that multiple interventions had a significant effect in reducing fall-related injuries and may result from the reduced risk of falling.
Although multifactorial fall risk assessment and intervention seems a plausible and attractive strategy for preventing falls and fall related injuries in older people it is not supported by strong
Su-Fei Huang et al. Fall-Related Injuries 177
evidence. Current evidence suggests that it may reduce the number of fallers by only a modest amount. Evidence of its effects on other outcomes such as the rate of falls and injuries is insufficient. Higher intensity interventions that provide treatments to address risk factors rather than information and referral may be more effective (Gates et al., 2008). In addition, the prior studies revealed that length of exercise intervention is associated with fall prevention (El-Khoury et al., 2013; Sherrington, Tiedemann, Fairhall, Close, & Lord, 2011; Sherrington et al., 2008). It may be the truth that the effective strategies and higher intensity interventions are necessary to be include in the fall prevention. However, in 22 analyzed studies with multifactorial interventions, duration time of each intervention in each study is not described clearly, such as referral, health assessment, fall risk assessment, hazard environmental modification. Therefore, analysis related to duration time of each intervention in each study can be discussed in the future research. Tinetti (2003) suggested that provision of effective interventions on fall prevention programs needed to consider the involvement of experienced healthcare professionals. A meta-analysis by Gillespie et al. (2012) found that when occupational therapists participated in the community fall prevention and home improvement programs for high-risk elderly, and when family physicians participated in medication adjustment intervention programs, there is a significant decrease in falls in the elderly. In the present meta-analysis, the presence of healthcare professionals as program implementers also contributed to the reduction on fall-related injuries. The results support that healthcare professionals play roles of guards in fall prevention works. Through referral, health assessment, fall risk assessment, hazard environmental modification, they can protect older adults from fallings and injuries. Further studies may explore the role of the healthcare professionals on the preventive effects of fall-related injuries.
Strengths and limitations
This meta-analysis has several limitations. First, because the power of our meta-analysis was large enough to make the findings robust, we did not include articles published before 1996. Second, if a trial did not report the desired statistic values for calculating OR and 95% CI, it was not included in the meta-analyses.
The strengths of our meta-analysis are that it included a high number of studies in the analyses, and that it found significant moderators on the preventive effect in fall-related injuries. Fall prevention programs are a promising intervention to reduce the incidence of falling and accompanying fall-related injuries. Given the paucity of RCT on fall-related fractures, we suggest that further studies should report the outcome of fractures after participants’ falls to examine possible protective effects of fall prevention interventions. Therefore, we suggest that future fall
178 Fall-Related Injuries Su-Fei Huang et al.
prevention trials should regularly report the outcomes of fall-related injuries and fractures separately. Because fractures, especially hip fractures, can incapacitate older adults, they can lead to disability and death (Marks, 2011). The potential effects of fall prevention programs on injurious fractures need to be emphasized. If the researchers and practitioners regularly deliver the fall prevention programs to older adults, caregiver’s burden and medical care expenses caused by falls will be promising to decrease.
Conclusions
The study conducted a meta-analysis to analyze the effect sizes of fall prevention programs in preventing fall-related injuries. Results showed that fall prevention programs had a significant effect in preventing fall-related injuries with a small effect size, but a borderline statistically significant effect in preventing fractures. Subgroup analyses found subgroups with both genders combined, participants’ history of falls ≥ 20%, community as intervention site, multiple interventions, and studies involved healthcare professionals as interveners showed significant effect sizes.
The present study included more studies to show that fall prevention programs for the older adults had a significant effect in preventing fall-related injuries, providing a reference for policy makers and practitioners regarding fall prevention programs for the older adults.
Acknowledgements
We would like to thank authors of some reviewed articles who provided data required for meta-analysis.
Su-Fei Huang et al. Fall-Related Injuries 179
References
Alexander, B. H., Rivara, F. P., & Wolf, M. E. (1992). The cost and frequency of hospitalization for fall-related injuries in older adults. American Journal of Public Health, 82(7), 1020-1023. doi: 10.2105/AJPH.82.7.1020
Baranzini, F., Diurni, M., Ceccon, F., Poloni, N., Cazzamalli, S., Costantini, C., …Callegari, C. (2009). Fall-related injuries in a nursing home setting: Is polypharmacy a risk factor? BMC Health Services Research, 9(1), 228. doi:10.1186/1472-6963-9-228
Barker, A. L., Morello, R. T., Wolfe, R., Brand, C. A., Haines, T. P., Hill, K. D., ...Kamar, J. (2016). 6-PACK programme to decrease fall injuries in acute hospitals: Cluster randomised controlled trial. BMJ, 352. doi:10.1136/bmj.h6781
Barnett, A., Smith, B., Lord, S. R., Williams, M., & Baumand, A. (2003). Community‐based group exercise improves balance and reduces falls in at‐risk older people: A randomised controlled trial. Age and Ageing, 32(4), 407-414. doi:10.1093/ageing/32.4.407
Becker, C., Kron, M., Lindemann, U., Sturm, E., Eichner, B., Walter‐Jung, B., & Nikolaus, T. (2003). Effectiveness of a multifaceted intervention on falls in nursing home residents. Journal of the American Geriatrics Society, 51(3), 306-313. doi:10.1046/j.1532-5415.2003.51103.x
Borenstein, M., Hedges, L. V., Higgins, J. P. T., & Rothstein, H. R. (2009). Introduction to Meta-analysis. Chichester, UK: John Wiley & Sons. doi:10.1002/9780470743386
Campbell, A. J., & Robertson, M. C. (2007). Rethinking individual and community fall prevention strategies: A meta-regression comparing single and multifactorial interventions. Age and Ageing, 36(6), 656-662. doi:10.1093/ageing/afm122
Campbell, A. J., Robertson, M. C., La Grow, S. J., Kerse, N. M., Sanderson, G. F., Jacobs, R. J., ... Hale, L. A. (2005). Randomised controlled trial of prevention of falls in people aged ≥75 with severe visual impairment: The VIP trial. BMJ, 331(7520), 817. doi:10.1136/bmj.38601. 447731.55
Chang, J. T., Morton, S. C., Rubenstein, L. Z., Mojica, W. A., Maglione, M., Suttorp, M. J., ... Shekelle, P. G. (2004). Interventions for the prevention of falls in older adults: Systematic review and meta-analysis of randomised clinical trials. BMJ, 328(7441), 680. doi:10.1136/ bmj.328.7441.680
Clemson, L., Cumming, R. G., Kendig, H., Swann, M., Heard, R., & Taylor, K. (2004). The effectiveness of a community‐based program for reducing the incidence of falls in the elderly:
180 Fall-Related Injuries Su-Fei Huang et al.
A randomized trial. Journal of the American Geriatrics Society, 52(9), 1487-1494. doi:10.1111/j. 1532-5415.2004.52411.x
Close, J., Ellis, M., Hooper, R., Glucksman, E., Jackson, S., & Swift, C. (1999). Prevention of falls in the elderly trial (PROFET): A randomised controlled trial. The Lancet, 353(9147), 93-97. doi:10.1016/S0140-6736(98)06119-4
Coe, R. (2002, September). It’s the effect size, stupid: What effect size is and why it is important. Paper presented at the 2002 Annual Conference of the British Educational Research Association, University of Exeter, Exeter, Devon, England.
Cumming, R. G., Sherrington, C., Lord, S. R., Simpson, J. M., Vogler, C., Cameron, I. D., & Naganathan, V. (2008). Cluster randomised trial of a targeted multifactorial intervention to prevent falls among older people in hospital. BMJ, 336(7647), 758-760. doi:10.1136/bmj.39499. 546030.BE
Davison, J., Bond, J., Dawson, P., Steen, I. N., & Kenny, R. A. (2005). Patients with recurrent falls attending accident & emergency benefit from multifactorial intervention – A randomised controlled trial. Age and Ageing, 34(2), 162-168. doi:10.1093/ageing/afi053
DerSimonian, R., & Laird, N. (1986). Meta-analysis in clinical trials. Controlled Clinical Trials, 7(3), 177-188. doi:10.1016/0197-2456(86)90046-2
Dyer, C. A. E., Taylor, G. J., Reed, M., Dyer, C. A., Robertson, D. R., & Harrington, R. (2004). Falls prevention in residential care homes: A randomised controlled trial. Age and Ageing, 33(6), 596-602. doi:10.1093/ageing/afh204
El-Khoury, F., Cassou, B., Charles, M.-A., & Dargent-Molina, P. (2013). The effect of fall prevention exercise programmes on fall induced injuries in community dwelling older adults: Systematic review and meta-analysis of randomised controlled trials. BMJ, 347. doi:10.1136/ bmj.f6234
El-Khoury, F., Cassou, B., Latouche, A., Aegerter, P., Charles, M.-A., & Dargent-Molina, P. (2015). Effectiveness of two year balance training programme on prevention of fall induced injuries in at risk women aged 75-85 living in community: Ossébo randomised controlled trial. BMJ, 351. doi:10.1136/bmj.h3830
Elley, C. R., Robertson, M. C., Garrett, S., Kerse, N. M., McKinlay, E., Lawton, B., ...Campbell, A. J. (2008). Effectiveness of a falls‐and‐fracture nurse coordinator to reduce falls: A randomized, controlled trial of at‐risk older adults. Journal of the American Geriatrics Society, 56(8), 1383-1389. doi:10.1111/j.1532-5415.2008.01802.x
Su-Fei Huang et al. Fall-Related Injuries 181
Effects on fall rates and injurious fall rates. Age and Ageing, 39(6), 728-733. doi:10.1093/ ageing/afq109
Gates, S., Fisher, J. D., Cooke, M. W., Carter, Y. H., & Lamb, S. E. (2008). Multifactorial assessment and targeted intervention for preventing falls and injuries among older people in community and emergency care settings: Systematic review and meta-analysis. BMJ, 336(7636), 130-133. doi:10.1136/bmj.39412.525243.BE
George, D., & Malley, P. (2010). SPSS for windows step by step: A simple study guide and reference, 17.0 update (10th ed.). Boston, MA: Pearson.
Gill, T. M., Murphy, T. E., Gahbauer, E. A., & Allore, H. G. (2013). Association of injurious falls with disability outcomes and nursing home admissions in community-living older persons. American Journal of Epidemiology, 178(3), 418-425. doi:10.1093/aje/kws554
Gillespie, L. D., Robertson, M. C., Gillespie, W. J., Lamb, S. E., Gates, S., Cumming, R. G., & Rowe, B. H. (2009). Interventions for preventing falls in older people living in the community. Cochrane Database Systematic Reviews, 2. doi:10.1002/14651858.CD007146.pub2
Gillespie, L. D., Robertson, M. C., Gillespie, W. J., Sherrington, C., Gates, S., Clemson, L. M., & Lamb, S. E. (2012). Interventions for preventing falls in older people living in the community. Cochrane Database Systematic Reviews, 9. doi:10.1002/14651858.CD007146.pub3
Goodwin, V. A., Abbott, R. A., Whear, R., Bethel, A., Ukoumunne, O. C., Thompson-Coon, J., & Stein, K. (2014). Multiple component interventions for preventing falls and fall-related injuries among older people: Systematic review and meta-analysis. BMC Geriatrics, 14(1), 15. doi:10.1186/1471-2318-14-15
Haines, T. P., Hill, A.-M., Hill, K. D., McPhail, S., Oliver, D., Brauer, S., ...Beer, C. (2011). Patient education to prevent falls among older hospital inpatients: A randomized controlled trial. Archives of Internal Medicine, 171(6), 516-524. doi:10.1001/archinternmed.2010.444
Hartholt, K. A., van Beeck, E. F., Polinder, S., van der Velde, N., van Lieshout, E. M. M., Panneman, M. J. M., ...Patka, P. (2011). Societal consequences of falls in the older population: Injuries, healthcare costs, and long-term reduced quality of life. The Journal of Trauma: Injury Infection, and Critical Care, 71(3), 748-753. doi:10.1097/ TA.0b013e3181f6f5e5
Heesch, K. C., Byles, J. E., & Brown, W. J. (2008). Prospective association between physical activity and falls in community-dwelling older women. Journal of Epidemiology and Community Health, 62(5), 421-426. doi:10.1136/jech.2007.064147
Hendriks, M. R. C., Bleijlevens, M. H. C., van Haastregt, J. C. M., Crebolder, H. F. J. M., Diederiks, J. P. M., Evers, S. M. A. A., ...van Eijk, J. T. M. (2008). Lack of effectiveness of a
182 Fall-Related Injuries Su-Fei Huang et al.
multidisciplinary fall‐prevention program in elderly people at risk: A randomized, controlled trial. Journal of the American Geriatrics Society, 56(8), 1390-1397. doi:10.1111/j.1532-5415. 2008.01803.x
Higgins, J. P. T., Thompson, S. G., Deeks, J. J., & Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ, 327(7414), 557-560. doi:10.1136/bmj.327.7414.557
Higgins, J. P. T., Altman, D. G., Gotzsche, P. C., Juni, P., Moher, D., Oxman, A. D., ...Sterne, J. A. C. (2011). The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ, 343. doi:10.1136/bmj.d5928
Hill, A.-M., Etherton-Beer, C., & Haines, T. P. (2013). Tailored education for older patients to facilitate engagement in falls prevention strategies after hospital discharge – A pilot randomized controlled trial. PLoS One, 8(5). doi:10.1371/journal.pone.0063450
Hoffman, G. J., Hays, R. D., Shapiro, M. F., Wallace, S. P., & Ettner, S. L. (2017). The costs of fall‐ related injuries among older adults: Annual per‐faller, service component, and patient out‐of‐ pocket costs. Health Services Research, 52(5), 1794-1816. doi:10.1111/1475-6773.12554 Hubacher, M., & Wettstein, A. (2001). Acceptance of hip protectors for hip fracture prevention in
nursing homes. Osteoporosis International, 12(9), 794-799. doi:10.1007/s001980170057 Jensen, J., Lundin-Olsson, L., Nyberg, L., & Gustafson, Y. (2002). Fall and injury prevention in
older people living in residential care facilities: A cluster randomized trial. Annals of Internal Medicine, 136(10), 733-741. doi:10.7326/0003-4819-136-10-200205210-00008
Jensen, J., Nyberg, L., Gustafson, Y., & Lundin‐Olsson, L. (2003). Fall and injury prevention in residential care – Effects in residents with higher and lower levels of cognition. Journal of the American Geriatrics Society, 51(5), 627-635. doi:10.1034/j.1600-0579.2003.00206.x
Karinkanta, S., Kannus, P., Uusi-Rasi, K., Heinonen, A., & Sievänen, H. (2015). Combined resistance and balance-jumping exercise reduces older women’s injurious falls and fractures: 5-year follow-up study. Age and Ageing, 44(5), 784-789. doi:10.1093/ageing/afv064
Kerse, N., Butler, M., Robinson, E., & Todd, M. (2004). Fall prevention in residential care: A cluster, randomized, controlled trial. Journal of the American Geriatrics Society, 52(4), 524-531. doi:10.1111/j.1532-5415.2004.52157.x
Kim, H., Yoshida, H., & Suzuki, T. (2014). Falls and fractures in participants and excluded non‐ participants of a fall prevention exercise program for elderly women with a history of falls: 1‐ year follow‐up study. Geriatrics & Gerontology International, 14(2), 285-292. doi:10.1111/ggi. 12095
Su-Fei Huang et al. Fall-Related Injuries 183
Avery, A. J. (2010). Community falls prevention for people who call an emergency ambulance after a fall: Randomised controlled trial. BMJ, 340. doi:10.1136/bmj.c2102
Lord, S. R., Tiedemann, A., Chapman, K., Munro, B., Murray, S. M., Gerontology, M., …Sherrington, C. (2005). The effect of an individualized fall prevention program on fall risk and falls in older people: A randomized, controlled trial. Journal of the American Geriatrics Society, 53(8), 1296-1304. doi:10.1111/j.1532-5415.2005.53425.x
Marks, R. (2011). Physical activity and hip fracture disability: A review. Journal of Aging Research, 2011, 1-18. doi:10.4061/2011/741918
McMurdo, M. E. T., Millar, A. M., & Daly, F. (2000). A randomized controlled trial of fall prevention strategies in old peoples’ homes. Gerontology, 46(2), 83-87. doi:10.1159/000022139 Ministry of Health and Welfare. (2014). Fall prevention for elderly. Retrieved from https://www.hpa.
gov.tw/Pages/EBook.aspx?nodeid=1193
Oliver, D., Connelly, J. B., Victor, C. R., Shaw, F. E., Whitehead, A., Genc, Y., ...Gosney, M. A. (2007). Strategies to prevent falls and fractures in hospitals and care homes and effect of cognitive impairment: Systematic review and meta-analyses. BMJ, 334(7584), 82. doi:10.1136/ bmj.39049.706493.55
Palvanen, M., Kannus, P., Piirtola, M., Niemi, S., Parkkari, J., & Järvinen, M. (2014). Effectiveness of the Chaos Falls Clinic in preventing falls and injuries of home-dwelling older adults: A randomised controlled trial. Injury, 45(1), 265-271. doi:10.1016/j.injury.2013.03.010
Patil, R., Uusi‐Rasi, K., Tokola, K., Karinkanta, S., Kannus, P., & Sievänen, H. (2015). Effects of a multimodal exercise program on physical function, falls, and injuries in older women: A 2‐year community‐based, randomized controlled trial. Journal of the American Geriatrics Society, 63(7), 1306-1313. doi:10.1111/jgs.13489
Pekkarinen, T., Löyttyniemi, E., & Välimäki, M. (2013). Hip fracture prevention with a multifactorial educational program in elderly community-dwelling Finnish women. Osteoporosis International, 24(12), 2983-2992. doi:10.1007/s00198-013-2381-y
Robertson, M. C., Campbell, A. J., Gardner, M. M., & Devlin, N. (2002). Preventing injuries in older people by preventing falls: A meta‐analysis of individual‐level data. Journal of the American Geriatrics Society, 50(5), 905-911. doi:10.1046/j.1532-5415.2002.50218.x
Robertson, M. C., Devlin, N., Gardner, M. M., & Campbell, A. J. (2001). Effectiveness and economic evaluation of a nurse delivered home exercise programme to prevent falls. 1: Randomised controlled trial. BMJ, 322(7288), 697. doi:10.1136/bmj.322.7288.697
184 Fall-Related Injuries Su-Fei Huang et al.
S. C. (2010). A randomized controlled trial of a multifactorial falls prevention intervention for older fallers presenting to emergency departments. Journal of the American Geriatrics Society, 58(12), 2265-2274. doi:10.1111/j.1532-5415.2010.03191.x
Sanders, K. M., Stuart, A. L., Williamson, E. J., Simpson, J. A., Kotowicz, M. A., Young, D., & Nicholson, G. C. (2010). Annual high-dose oral vitamin D and falls and fractures in older women: A randomized controlled trial. JAMA, 303(18), 1815-1822. doi:10.1001/jama.2010.594 Sherrington, C., Tiedemann, A., Fairhall, N., Close, J. C. T., & Lord, S. R. (2011). Exercise to
prevent falls in older adults: An updated meta-analysis and best practice recommendations. New South Wales Public Health Bulletin, 22(3-4), 78-83. doi:10.1071/NB10056
Sherrington, C., Whitney, J. C., Lord, S. R., Herbert, R. D., Cumming, R. G., & Close, J. C. (2008). Effective exercise for the prevention of falls: A systematic review and meta‐analysis. Journal of the American Geriatrics Society, 56(12), 2234-2243. doi:10.1111/j.1532-5415.2008.02014.x Siegrist, M., Freiberger, E., Geilhof, B., Salb, J., Hentschke, C., Landendoerfer, P., ...Blank, W. A.
(2016). Fall prevention in a primary care setting: The effects of a targeted complex exercise intervention in a cluster randomized trial. Deutsches Ärzteblatt International, 113(21), 365-372. doi:10.3238/arztebl.2016.0365
Spice, C. L., Morotti, W., George, S., Dent, T. H. S., Rose, J., Harris, S., & Gordon, C. J. (2009). The Winchester falls project: A randomised controlled trial of secondary prevention of falls in older people. Age and Ageing, 38(1), 33-40. doi:10.1093/ageing/afn192
Stevens, J. A., Corso, P. S., Finkelstein, E. A., & Miller, T. R. (2006). The costs of fatal and non-fatal falls among older adults. Injury Prevention, 12(5), 290-295. doi:10.1136/ip.2005.011015 Stevens, J. A., Mack, K. A., Paulozzi, L. J., & Ballesteros, M. F. (2008). Self-reported falls and
fall-related injuries among persons aged ≥65 years? – United States, 2006. Journal of Safety Research, 39(3), 345-349. doi:10.1016/j.jsr.2008.05.002
Stevens, J. A., & Sogolow, E. D. (2005). Gender differences for non-fatal unintentional fall related injuries among older adults. Injury Prevention, 11(2), 115-119. doi:10.1136/ip.2004.005835 Tinetti, M. E. (2003). Preventing falls in elderly persons. New England Journal of Medicine, 348(1),
42-49. doi:10.1056/NEJMcp020719
Vassallo, M., Vignaraja, R., Sharma, J. C., Hallam, H., Binns, K., Briggs, R., ...Allen, S. (2004). The effect of changing practice on fall prevention in a rehabilitative hospital: The hospital injury prevention study. Journal of the American Geriatrics Society, 52(3), 335-339. doi:10.1111/j. 1532-5415.2004.52102.x
Su-Fei Huang et al. Fall-Related Injuries 185
K. (2016). Falls and fall-related injuries among community-dwelling adults in the United States. PLoS One, 11(3). doi:10.1371/journal.pone.0150939
Vind, A. B., Andersen, H. E., Pedersen, K. D., Jørgensen, T., & Schwarz, P. (2009). An outpatient multifactorial falls prevention intervention does not reduce falls in high‐risk elderly danes. Journal of the American Geriatrics Society, 57(6), 971-977. doi:10.1111/j.1532-5415.2009. 02270.x
World Health Organization. (2008). WHO global report on falls prevention in older age 2007. Retrieved from http://www.who.int/ageing/publications/Falls_prevention7March.pdf?ua=1
186 Fall-Related Injuries Su-Fei Huang et al. 教育科學研究期刊 第六十三卷第二期 2018年,63(2),163-186 doi:10.6209/JORIES.201806_63(2).0007
預防計畫對於老人跌倒相關傷害之成效:
統合分析
黃素妃
*楊婷婷
陳雪芬
馬偕學校財團法人馬偕醫護管理專科學校 高齡服務事業科 大智通文化行銷股份有限公司 經國管理暨健康學院 高齡照顧福祉系呂莉婷
廖容瑜
康寧大學 高齡社會健康管理科 觀光與休閒事業管理系 萬能科技大學摘要
本研究目的為評估預防計畫對老人跌倒相關傷害之成效,從 Cochrane Library、Medline、 PubMed、PsycARTICLES、PsycINFO、ERIC、AgeLine、CINAHL、Psychology、BehavioralSciences Collection databases等,蒐集所有相關的臨床隨機試驗研究,文獻年代範圍從 1996 年
至 2016 年間,並應用探索性統合分析,計算老人跌倒預防計畫之效果量。共計 33 篇期刊論 文納入分析(68,736 人),探索性統合分析結果顯示,跌倒預防計畫對因跌倒所造成的傷害 具顯著效果(OR=0.86, 95% CI:0.75-0.97),但是對於骨折的預防效果則介於邊緣性顯著差 異(OR=0.80, 95% CI:0.63-1.03)。此外,跌倒預防計畫若是不分男女、介入內容包含健康 照護專家、當參與者超過 20%具跌倒經驗、社區為介入場域、包含多元介入等,本研究發現 預防計畫對於預防跌倒相關傷害具有小卻顯著的效果,因此,未來規劃跌倒預防計畫時,政 策制定者及臨床工作者應考量不同特性的老人,並提出合適的介入計畫。 關鍵詞: 老人、統合分析、跌倒預防、意外跌倒、傷害 通訊作者:廖容瑜,E-mail: [email protected] 收稿日期:2017/09/25;修正日期:2018/01/08、2018/01/30;接受日期:2018/03/01。