©2010 Taiwan Pediatric Association
O R I G I N A L A RT I C L E
*Corresponding author. Department of Pediatrics, Pingtung Christian Hospital, No.60, Da-Lian Road, Pingtung City 90059, Taiwan. E-mail: [email protected]
Background: To study the epidemiology of childhood intussusception and risk fac-tors of recurrence and operation based on a nationwide data.
Methods: Children with hospitalization due to intussusception (ICD9: 560.0) between 1998 and 2007 were identified from a national health insurance database. The inci-dence was calculated by age, sex, calendar year and month of admission. Recurrence and operation rates, duration and costs of hospitalization were analyzed.
Results: A total of 8217 intussusception-related hospitalizations were identified in 7541 children. The incidence of intussusception peaked between 3 and 36 months of age. Male -to-female incidence rate ratio increased from 1.31 in the first year to 2.52 in the ninth year of life. The overall recurrence and operation rates were 7.9% and 24.9%, respectively. In children less than 1 year old, the recurrence rate was 10.1%, which decreased to 5.3% in children over 3 years old. Multiple logistic regression analysis showed that children receiving operation had a significantly lower risk of recurrence with an odds ratio (95% confidence interval) of 0.31 (0.24−0.41) after controlling for age and sex. There are significantly more cases occurring during the warmer months between May and October compared to the cooler months between November and April.
Conclusions: There was a male predominance of intussusception with a dynamic male-to-female incidence rate ratio. Children under 1 year of age have the highest recurrence and operation rates. Seasonal variation of intussusception was sus-pected in Taiwan.
Epidemiology of Childhood Intussusception and
Determinants of Recurrence and Operation:
Analysis of National Health Insurance Data
Between 1998 and 2007 in Taiwan
Solomon Chih-Cheng Chen
1,2, Jung-Der Wang
2,3, Hong-Yuan Hsu
4,
Mee-Mee Leong
1,5, Teck-Siang Tok
1, Yow-Yue Chin
1*
1Department of Pediatrics, Pingtung Christian Hospital, Pingtung, Taiwan
2Institute of Occupational Medicine and Industrial Hygiene, College of Public Health, National Taiwan University, Taipei, Taiwan
3Department of Environmental and Occupational Medicine, National Taiwan University Hospital, Taipei, Taiwan
4Department of Pediatrics, National Taiwan University Hospital, Taipei, Taiwan 5Department of Pediatrics, China Medical University Hospital, Taichung, Taiwan
Received: Dec 17, 2009 Revised: Feb 22, 2010 Accepted: Mar 13, 2010 KEY WORDS: hospitalization; insurance; recurrence; seasonal variation; sex ratio
1.
Introduction
Intussusception is the most common intestinal ob-struction among infants and young children.1
Epi-demiological studies of intussusception have been performed, either for surveillance of adverse effects of rotavirus vaccine or to provide baseline epide-miological data.2−7 Recurrence of intussusception is
possible after successful reduction, with an approx-imate rate of 8−10%.8−11 Failure of nonsurgical
re-duction for intussusception may require surgical intervention.12−14 However, the epidemiological
fea-tures of intussusception recurrence and surgical re-duction are not well understood.
Taiwan, an island country with approximately 23 million people, has a National Health Insurance (NHI) system that covers almost 99% of the popula-tion, and NHI health care databases contain suffi-cient information to provide national epidemiology data on a specific disease. In 2005, Ho et al3 first
described the epidemiology of intussusception in Taiwanese children based on NHI data collected be-tween 1999 and 2001. However, the results and con-clusions of this study were based on only 3 calendar years and may not be long enough for making an inference on the recurrence rate.
The objectives of this study were (1) to explore the epidemiological features of intussusception in Taiwanese children based on a longer period of NHI data (1998−2007), and (2) to determine the rates of surgical intervention and recurrence of intussus-ception and their risk factors.
2.
Materials and Methods
2.1. Patients and enrollment criteria
Children with a diagnosis of intussusceptions, and who were hospitalized between January 1998 and December 2007, were identified from the NHI Research Database. From this database, we identi-fied intussusception cases on the basis of the Inter-national Classification of Diseases, 9th Revision,
Clinical Modification (ICD-9-CM) code for intussus-ception (560.0), listed as any one of the first three major diagnoses.
Due to regulations of the Personal Electronic Data Protection Law of Taiwan, the identification (ID) numbers of all persons and hospitals in this database were encrypted to be unrecognizable from the original ID numbers. The new ID numbers permitted us to analyze a patient’s data while remaining blind to the patient’s identity. Date of birth, admission date and sex information were included in the NHI data files. We sorted the new ID numbers and carefully checked patients’ birth dates, admission dates and
discharge dates. If one person was re-admitted to the hospital within 3 days (inclusive) of the previous admission date, the new admission was considered as an early recurrence. Otherwise it was considered as a late recurrence. Length of hospitalization and hospital costs were also compared between the operation and nonoperation cases.
The initial onset of intussusception was identi-fied by the first admission date of intussusception-related hospitalization for each case. The incidence of intussusception was calculated according to age, sex, calendar year and month of hospitalization. The yearly incidences of intussusception were cal-culated as the number of intussusception cases di-vided by the population size of children less than 15 years of age during each calendar year between 1998 and 2007.
2.2. Data of weather statistics
Weather statistics were obtained from the archives of Central Weather Bureau of Taiwan.15 The monthly temperature was averaged across 25 weather sta-tions that continuously collect meteorological data for the entire island of Taiwan to obtain an average monthly temperature. The total number of hospi-talized cases in each month and the mean monthly temperatures were shown together.
2.3. Statistical analyses
The incidence rate was expressed as the number of intussusception cases per 100,000 person-years. Statistical data on the population size for each age group of males and females were obtained from National Statistics, Republic of China (Taiwan).16 In addition to simple tabulation of demographic data, multiple logistic regression model were constructed for risk factors associated with recurrence or op-eration of intussusception, including age, sex, season (warmer or cooler), previous operation and recur-rence. Data were analyzed using Microsoft Excel and SPSS software (version 16.0; SPSS Inc., Chicago, IL, USA).
2.4. Ethical approval
The Ethics Review Board of our institute approved the study protocol. Because this study represents an analysis of secondary data, no informed consent was necessary.
3.
Results
From the Taiwan NHI data collected between 1998 and 2007, a total of 8217 hospitalizations due to
intussusception were identified in 7541 children. Initial onset of intussusception before the first 3 months of life was relatively rare, and case num-bers peaked between 3 and 36 months (Figure 1). The cumulative percentage of intussusception-related hospitalization was 24.8% in children less than 1-year-old, 56.5% in children less than 2 years old and 79.4% in children less than 3 years old (Figure 1).
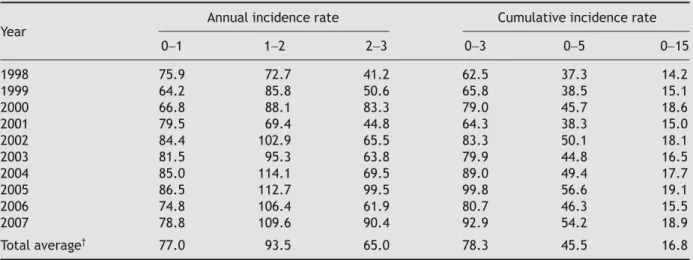
The annual incidence rate of intussusception hospitalization varied slightly among different cal-endar years (Table 1). The incidence rate of intus-susception was higher in the first 3 years of life (Table 1). Male children had a higher incidence
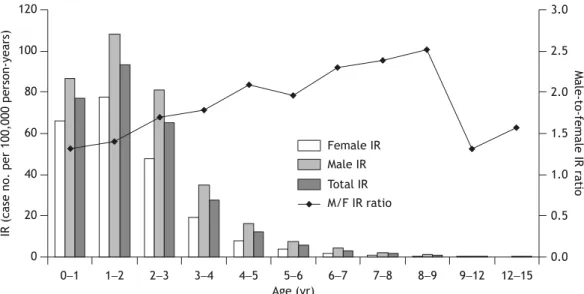
rate than female children (61.3 vs. 38.7 per 100,000 person-years, respectively), and the male-to-female incidence rate ratio showed an increasing trend from 1.31 in the first year of life to 2.52 in the ninth year of life (Figure 2). The mean age of the first episode of intussusception was 27.3 months of life in male children, and 24.9 months in females (p < 0.001).
The mean number of monthly cases was signif-icantly higher during the warmer months of May through October (mean ± SD, 728 ± 51) compared with that of the cooler months of November through April (mean ± SD, 641 ± 27) with a p value of 0.004 (Figure 3).
Table 1 Incidence rate of intussusception by age groups in Taiwanese children less than 15 years of age from 1998 to 2007*
Annual incidence rate Cumulative incidence rate Year 0−1 1−2 2−3 0−3 0−5 0−15 1998 75.9 72.7 41.2 62.5 37.3 14.2 1999 64.2 85.8 50.6 65.8 38.5 15.1 2000 66.8 88.1 83.3 79.0 45.7 18.6 2001 79.5 69.4 44.8 64.3 38.3 15.0 2002 84.4 102.9 65.5 83.3 50.1 18.1 2003 81.5 95.3 63.8 79.9 44.8 16.5 2004 85.0 114.1 69.5 89.0 49.4 17.7 2005 86.5 112.7 99.5 99.8 56.6 19.1 2006 74.8 106.4 61.9 80.7 46.3 15.5 2007 78.8 109.6 90.4 92.9 54.2 18.9 Total average† 77.0 93.5 65.0 78.3 45.5 16.8
*Incidence rate was defined as the number of cases per 100,000 person-years in the same age group; †mean of all children in the specified age category.
0 0 − 3− 6− 9− 12 − 15 − 18 − 21 − 24 − 27 − 30 − 33 − 36 − 39 − 42 − 45 − 48 − 51 − 54 − 57 − 60 − 72 − 84 − 96 − 108 − 120 − 132 − 144 − 156 − 168 − 180 200 400 600 800 Age (mo) Cases ( n ) 0 10 20 30 40 50 60 70 80 90 100 Cumulative percentage (%) Cases (n) Cumulative %
Figure 1 Case numbers and cumulative percentage of intussusception in Taiwanese children less than 15 years of age between 1998 and 2007.
Among the 7541 children, 597 children (7.9%) were hospitalized more than once. In total, there were 676 episodes of recurrent hospitalization with 295 episodes (43.6%) recurring within 3 days of pre-vious admission date and the remaining 381 epi-sodes (56.4%) recurring later. However, the recurrence rate decreased as the age of initial onset increased (Table 2), and the recurrence rates were similar between male and female children (8.0% vs. 7.8%, respectively, p = 0.826 by Pearson χ2 test). A total
of 1878 children (24.9%) underwent surgical interven-tion. The rate of operation was significantly higher (34.3%) in cases with initial onset age of less than 1 year; the rates remained between 21% and 23% after the first year (Table 2). The 1878 cases receiv-ing surgical intervention incurred a higher mean med-ical cost [New Taiwan (NT) $51,411 or US$1606] and a longer mean hospital stay (6.4 days) than those who did not require surgery (NT$8716 or US$272 US with a mean hospitalization of 2.6 days). The oper-ation rate among cases with recurrence was signifi-cantly less than those without recurrence (Table 2). The mean age and sex ratio were not different be-tween the operation and nonoperation groups.
4.
Discussion
The analysis of the national data of the last 10 years (1998−2007) showed that the incidence rate of intus-susception was low for infants younger than 3 months old, then increased rapidly and peaked between 3 and 36 months of age (Figure 1). This finding is consist-ent with another nationwide epidemiological study in Switzerland.6 The average yearly incidence rate
of intussusception in Taiwanese children was 77.0
per 100,000 person-years in infants less than 1 year old (Table 1), very similar to other areas, such as Singapore with 60 per 100,000, Hong Kong with 78−100 per 100,000, the United States with 62 per 100,000 and Europe with 66−75 per 100,000.4−6,17,18
Some previous studies cited a peak incidence of intussusception during the first year of life,4,6,7,19 but
a previous Taiwanese study favored the second year.3
In Table 1, we found that both the first year and sec-ond year possibly have the highest incidence. Since the peak incidence of intussusception resembles a continuous plateau during months 3−36, as shown in Figure 1, therefore, it may not be easy to tell the exact age of peak incidence being in the first year or the second year of life. Table 1 also demonstrated a stable, although with some fluctuation, incidence of intussusception among different calendar years.
A predominance of intussusception among males has been noted in previous studies, with male-to-female ratios ranging from 1.3 to 2.0.2,4,18,20 An
in-teresting finding in this study was that the incidence rate ratio between two sexes was dynamic, increas-ing from 1.31 in children less than 1 year old to 2.52 in children 9 years old. The gradual increase of male-to-female incidence rate ratio by age may be related to the differential onset time between the two sexes, as the mean age of the initial onset of intussusception was significantly older in males than in females (27.3 months vs. 24.9 months, re-spectively, p < 0.001). The male-to-female inci-dence rate ratio decreased after 9 years of age, but the limited number of cases does not permit us to make any strong inference among older children or adolescents.
In this study, we found a total recurrence rate of 7.9%, which is consistent with the previously
0 20 40 60 80 100 120 0−1 1−2 2−3 3−4 4−5 5−6 6−7 7−8 8−9 9−12 12−15 Age (yr)
IR (case no. per 100,000 person-years)
0.0 0.5 1.0 1.5 2.0 2.5 3.0 Male-to-female IR ratio Female IR Male IR Total IR M/F IR ratio
Figure 2 Incidence rates (case number per 100,000 person-years) of intussusception of the two sexes and the male-to-female incidence rate (IR) ratio in Taiwanese children less than 15 years of age between 1998 and 2007.
published recurrence rates of 8−10%.5,8−11 No sex
difference in recurrence rate was noted; the inci-dence among males was 8.0% and among females was 7.8% (p = 0.826). In assessing the age of the recur-rence, this study found that the percentage of re-currence decreased with increasing age of initial onset. In children less than 1 year old, the recurrence rate was 10.1%, which decreased to 5.3% in children over 3 years old (Table 2). Children receiving oper-ation had a significantly lower risk of recurrence with an odds ratio (95% confidence interval) of 0.31 (0.24−0.41). This was reasonable because the leading
point may be removed and the intestines may be adhesive to surrounding tissues, and both factors reduced the recurrence of intussusception.
The operation rate was higher among cases with only one hospitalization (no recurrence) and re-mained constant regardless of the times of hospitali-zation among those cases with recurrences (Table 2). In this study, only 10 out of the 48 cases with more than three episodes of recurrences received an op-eration. This finding supports the opinion that each recurrence should be managed as though it were the first episode, and surgical reduction should be
Table 2 Odds ratio (OR) and 95% confidence interval (CI) of multiple logistic regression model for risk factors associated with recurrence or operation of intussusception
Recurrence Operation
Cases (n)
Cases n (%) OR (95% CI) Cases n (%) OR (95% CI) Age (yr) 0−1 1869 200 (10.7) 1 641 (34.3) 1 1−2 2382 192 (8.1) 0.65 (0.53−0.80) 518 (21.7) 0.51 (0.45−0.59) 2−3 1736 122 (7.0) 0.55 (0.44−0.70) 363 (20.9) 0.48 (0.41−0.56) ≥ 3 1554 83 (5.3) 0.42 (0.32−0.55) 356 (22.9) 0.53 (0.46−0.62) Sex Female 2823 221 (7.8) 1 675 (23.9) 1 Male 4718 376 (8.0) 1.08 (0.90−1.28) 1203 (25.5) 1.12 (1.01−1.26) Season Cooler 3525 278 (7.9) 1 897 (25.4) 1 Warmer 4016 319 (7.9) 1.00 (0.84−1.18) 981 (24.4) 0.94 (0.85−1.05) Operation No 5663 533 (9.4) 1 Yes 1878 64 (3.4) 0.31 (0.24−0.41) Recurrence No 6944 1814 (26.1) 1 Yes 597 64 (10.7) 0.31 (0.24−0.41) Total 597 (7.9) 1878 (24.9) 0 300 600 900
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
C a ses ( n ) 0 5 10 15 20 25 30 M ean tem p e ratu re ( ° C) Admissions Temperature (°C)
Figure 3 Monthly mean temperature and case numbers of intussusception hospitalizations in Taiwanese children less than 15 years of age between 1998 and 2007 were shown together.
reserved for cases with failure of hydrostatic re-duction, positive peritoneal sign or suspected exis-tence of pathological leading points.10,12 As cases
that received operations usually had longer hospital stays and incurred higher costs,3,21 the risk and
ben-efit of operation for recurrent intussusception should be fully explained to patients’ families. The opera-tion rate was also significantly higher in children less than 1 year old than those in the older ages (Table 2). However, the age and sex distribution did not differ between operation and nonoperation cases.
The seasonality of the occurrence of intussus-ception was controversial before; some studies re-ported no seasonal variations3,4,6,7,19,22 while other
studies favored seasonality.6,23 In this study, we found
the mean number of monthly cases being significantly higher during the warmer months than that in the cooler months (728 ± 51 vs. 641 ± 27, respectively,
p = 0.004 as shown in Figure 3). We thought young
children may have more outdoor activities in warmer seasons that possibly results in a higher chance to get viral infection and an increased tendency for intussusception.24 How ever, the reasons of seasonal
variation need further studies to clarify.
This study, using the NHI database, has several limitations. First, the data came from hospitalization records, so the intussusception cases that only pre-sented to an emergency department or an outpa-tient clinic would not be included. This limitation may underestimate the occurrences of intussuscep-tion. However, as the yearly incidence rate of in-tussusception reported in current paper is similar to other countries, we think such estimation is ac-ceptable. Second, the NHI reimbursement database is not originally collected for academic research, so we did not have all the clinical information, such as types of enema reduction, data of viral isolation or the pathology report for the surgical cases. Third, mortality due to intussusception could not be iden-tified because case ID numbers were encrypted, preventing us from linking the mortality file to the national statistics. However, mortality from intus-susception is generally rare and may be ignored. In spite of the limitations of the data used in this study, the NHI database still provides useful information for studying disease incidence on a national scale.
5.
Conclusions
This nationwide epidemiological study documented the peak incidence rate of intussusception between 3 and 36 months of age and showed a dynamic change of male-to-female incidence rate ratio from 1.31 in the first year to 2.52 in the ninth year of life. The overall recurrence and operation rates were 7.9% and 24.9%, respectively, and both of them were
higher in those aged less than 1 year old. Finally, there were a greater number of cases occurring dur-ing the warmer months between May and October in Taiwan and the seasonal variation of intussus-ception was suspected.
Acknowledgments
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health, and managed by National Health Research Institutes. The interpretation and conclusions con-tained herein do not represent those of the Bureau of National Health Insurance, Department of Health or National Health Research Institutes of Taiwan. The authors sincerely thank Ms Yu-Yin Chang for her great assistance on data management.
References
1. Wyllie R. Ileus, adhesions, intussusception and closed-loop obstruction. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson Textbook of Pediatrics, 18th ed. Philadelphia, PA: Saunders, 2007:1568−71.
2. Archibong AE, Usoro IN, Ikpi E, Inyang A. Paediatric intus-susception in Calabar, Nigeria. East Afr Med J 2001;78:19−21. 3. Ho WL, Yang TW, Chi WC, Chang HJ, Huang LM, Chang MH.
Intussusception in Taiwanese children: analysis of incidence, length of hospitalization and hospital costs in different age groups. J Formos Med Assoc 2005;104:398−401.
4. Boudville IC, Phua KB, Quak SH, et al. The epidemiology of paediatric intussusception in Singapore: 1997 to 2004. Ann Acad Med Singapore 2006;35:674−9.
5. Huppertz HI, Soriano-Gabarro M, Grimprel E, et al. Intus-susception among young children in Europe. Pediatr Infect Dis J 2006;25:S22−9.
6. Buettcher M, Baer G, Bonhoeffer J, Schaad UB, Heininger U. Three-year surveillance of intussusception in children in Switzerland. Pediatrics 2007;120:473−80.
7. Awasthi S, Agarwal GG, Mishra V, et al. Four-country sur-veillance of intestinal intussusception and diarrhoea in chil-dren. J Paediatr Child Health 2009;45:82−6.
8. Daneman A, Alton DJ, Lobo E, Gravett J, Kim P, Ein SH. Patterns of recurrence of intussusception in children: a 17-year review. Pediatr Radiol 1998;28:913−9.
9. Gonzalez-Spinola J, Del Pozo G, Tejedor D, Blanco A. Intussusception: the accuracy of ultrasound-guided saline enema and the usefulness of a delayed attempt at reduction. J Pediatr Surg 1999;34:1016−20.
10. Yang CM, Hsu HY, Tsao PN, Chang MH, Lin FY. Recurrence of intussusception in childhood. Acta Paediatr Taiwan 2001;42: 158−61.
11. Ramachandran P, Gupta A, Vincent P, Sridharan S. Air enema for intussusception: is predicting the outcome important? Pediatr Surg Int 2008;24:311−3.
12. Pierro A, Donnell SC, Paraskevopoulou C, Carty H, Lloyd DA. Indications for laparotomy after hydrostatic reduction for intussusception. J Pediatr Surg 1993;28:1154−7.
13. Daneman A, Navarro O. Intussusception. Part 2: an update on the evolution of management. Pediatr Radiol 2004;34: 97−108; quiz 87.
14. Chang YT, Lee JY, Wang JY, Chiou CS, Lin JY. Early laparoscopy for ileocolic intussusception with multiple recurrences in children. Surg Endosc 2009;23:2001−4.
15. Climate statistics: Monthly mean temperature. Central Weather Bureau, Taiwan. Available at: http://www.cwb.gov.tw/ [Date accessed: November 1, 2009]
16. National Statistics, R.O.C.(Taiwan). Vital statistics: live births, birth rate, deaths and mortality. Available at: http://www.stat.gov.tw/ [Date accessed: November 1, 2009] 17. Nelson EA, Tam JS, Glass RI, Parashar UD, Fok TF. Incidence
of rotavirus diarrhea and intussusception in Hong Kong using standardized hospital discharge data. Pediatr Infect Dis J 2002;21:701−3.
18. Tate JE, Simonsen L, Viboud C, et al. Trends in intussuscep-tion hospitalizaintussuscep-tions among US infants, 1993−2004: impli-cations for monitoring the safety of the new rotavirus vaccination program. Pediatrics 2008;121:e1125−32.
19. Chen YE, Beasley S, Grimwood K. Intussusception and rota-virus associated hospitalisation in New Zealand. Arch Dis Child 2005;90:1077−81.
20. Blanch AJ, Perel SB, Acworth JP. Paediatric intussusception: epi-demiology and outcome. Emerg Med Australas 2007;19:45−50. 21. Dawod ST, Osundwa VM. Intussusception in children under
2 years of age in the State of Qatar: analysis of 67 cases. Ann Trop Paediatr 1992;12:121−6.
22. Parashar UD, Holman RC, Cummings KC, et al. Trends in intussusception-associated hospitalizations and deaths among US infants. Pediatrics 2000;106:1413−21.
23. Carneiro PM, Kisusi DM. Intussusception in children seen at Muhimbili National Hospital, Dar es Salaam. East Afr Med J 2004;81:439−42.
24. Hsu HY, Kao CL, Huang LM, et al. Viral etiology of intussuscep-tion in Taiwanese childhood. Pediatr Infect Dis J 1998;17: 893−8.