行政院國家科學委員會專題研究計畫 成果報告
鎝-99m MIBI 造影結果與 Pgp/MRP 基因表現於副甲狀腺腺
瘤的相關性
計畫類別: 個別型計畫 計畫編號: NSC91-2314-B-039-031-執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日 執行單位: 中國醫藥大學附設醫院核醫科 計畫主持人: 高嘉鴻 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中
華
民
國 92 年 8 月 20 日
行政院國家科學委員會補助專題研究計畫
■ 成 果 報
告 □期
中進度
報
告
鎝-99m MIBI 造影結果 Pgp/MRP 基因表現於副甲狀
腺腺瘤的相關性
計畫類別:■ 個別型計畫
□ 整合型計畫
計畫編號:NSC 91-2314-B-039-031
執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日
計畫主持人:
高嘉鴻
共同主持人:
計畫參與人員:
成果報告類型(依經費核定清單規定繳交):■精簡報告 □完整
報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究
計畫、列管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公
開查詢
執行單位:中國醫藥大學附設醫院核子醫學科
中 華 民 國
九 十 二
年
八
月 十
九 日
中文摘要
副甲狀腺腺體大小被認為是影響 Tc-99m MIBI 副甲狀腺造影來定位副甲狀腺瘤 的主要因素。此外,由於先前的研究顯示即使是巨大的副甲狀腺瘤也會出現偽陰 性的造影而非常微小的腺瘤亦可能顯示真陽性的結果,副甲狀腺瘤之 P-糖蛋白 的表現被認為是另外可能影響副甲狀腺瘤在副甲狀腺造影之定位的因素。因此, 此項研究的目的在於回溯性地評估副甲狀腺造影的結果及副甲狀腺瘤的 P-糖蛋 白或是多重抗藥性相關蛋白之表現的相互關係。47 位有較大副甲狀腺瘤(大於 1.5 公克)的病人在手術前進行早期(靜脈注射 Tc-99m MIBI 後 10 分鐘)及延遲(靜脈注 射 Tc-99m MIBI 後 2 小時)的副甲狀腺造影。同時利用手術檢體的不連續片段來 進行免疫組織化學分析,以偵測 P-糖蛋白或是多重抗藥性相關蛋白之表現。根 據免疫組織化學分析的結果,34 個副甲狀腺瘤被分別歸類為 4 個組別:(1) P-糖 蛋白和多重抗藥性相關蛋白之表現均為陽性的有 3 個;(2) P-糖蛋白之表現為陽 性而多重抗藥性相關蛋白之表現為陰性的有 1 個;(3) P-糖蛋白之表現為陽性而 多重抗藥性相關蛋白之表現為陽性的有 4 個;(4) P-糖蛋白和多重抗藥性相關蛋 白之表現均為陰性的有 39 個。在第 4 組中所有 39 個副甲狀腺瘤均可被 Tc-99m MIBI 副甲狀腺造影所發現。而第 1 至第 3 組中所有 8 個副甲狀腺瘤均無法被 Tc-99m MIBI 副甲狀腺造影所發現(p < 0.05)。因此,手術前利用 Tc-99m MIBI 副 甲狀腺造影來定位副甲狀腺的敏感性不只是受限於副甲狀腺瘤的大小,更重要的 還有 P-糖蛋白和多重抗藥性相關蛋白之表現。關鍵字
Technetium-99m methoxyisobutylisonitrile (Tc-99m MIBI);副甲狀腺瘤;P-糖蛋 白;多重抗藥性相關蛋白
英文摘要
Gland size was considered to be the major factor to influence localization of parathyroid adenomas by technetium-99m methoxyisobutylisonitrile (99mTc MIBI) parathyroid imaging. In addition, P-glycoprotein (P-gp) expression in parathyroid adenomas has been considered to be an another possible factor to influence localization of parathyroid adenomas because false-negative studies have been reported with large tumors and true-positives reported with very small tumors in previous studies. Therefore, the purpose of this study was to retrospectively to evaluate the relationship between 99mTc MIBI parathyroid imaging results and Pgp or multidrug resistance related protein (MRP) expression in parathyroid adenomas. Before surgery, 47 patients with larger parathyroid adenomas (larger than 1.5 gm) underwent early and delay parathyroid imaging, 10 minutes and 2 hours after intravenous injection of 99mTc MIBI. Immunohistochemical analyses (IHA) were performed, using multiple nonconsecutive sections of the operative specimens, to detect Pgp or MRP expression. According to the results of IHA, the 34 parathyroid adenomas were separated into four groups: (1) 3 adenomas with both positive Pgp and positive MRP expression, (2) 1 adenomas with positive Pgp but negative MRP expression, (3) 4 adenomas with negative Pgp but positive MRP expression, and (4) 39 adenomas with both negative Pgp and negative MRP expression. All of 39 adenomas in the group 4 could be detected by 99mTc MIBI parathyroid imaging. All of 8 adenomas in the groups 1 to 3 could not be detected by 99mTc MIBI parathyroid imaging (p < 0.05). Not only the size of parathyroid adenomas, but also significant Pgp or MRP expression limited the sensitivity of 99mTc MIBI parathyroid imaging to localize parathyroid adenomas before operation.
Keywor ds
Technetium-99m methoxyisobutylisonitrile; Parathyroid adenoma; P-glycoprotein; Multidrug resistance related protein
Intr oduction
The accurate preoperative localization of parathyroid adenomas is important prior to surgery. Techniques used include high-resolution ultrasound, computerized tomography (CT), magnetic resonance imaging (MRI); however, all methods have some limitations [1-3]. A major advance occurred when the nuclear medicine technique with technetium-99m methoxyisobutylisonitrile (99mTc MIBI) parathyroid scan for parathyroid localization [4]. 99mTc MIBI parathyroid imaging has been suggested that routine preoperative localization before operation for hyperparathyroidism may improve long-term cure rate, decrease morbidity, and reduce the cost and the duration of the operation [5].
99m
Tc MIBI is a lipophilic cationic complex and which was originally introduced for myocardial perfusion imaging [6]. 99mTc MIBI nonspecifically localizes in mitochondria and the cytoplasm. It is retained by membrane potentials across the membrane of the cell and mitochondria [7]. 99mTc MIBI localizes in thyroid and parathyroid glands, but it washes out of the thyroid faster than the parathyroid, thus providing a greater parathyroid-to-thyroid uptake ratio with time and thus 99mTc MIBI appears useful for localization of abnormal and hyperfunctioning parathyroid with either subtraction procedure or indeed as a sole agent [8,9]. Malloul et al. found tracer accumulation in oxyphil cells might partially explain the preferential 99mTc MIBI retention in parathyroid lesions [10]. However, the exact mechanisms of visualization of abnormal and hyperfunctioning parathyroid tissue is not yet clear.
Previous studies [11,12] have reported a correlation between tumor size and detectability of parathyroid adenomas by 99mTc MIBI parathyroid imaging. However, false-negative results have been reported in large tumors and some very small tumors have been detected. From a review of the literature regarding Pgp or MRP expression in cancer cell lines and animal models, Pgp or MRP expression prevent accumulation of some lipophilic cationic radiopharmaceuticals such as 99mTc MIBI [13-15]. Thus, a possible factor to influence detection of parathyroid adenomas by 99mTc MIBI parathyroid imaging is not only the size of parathyroid adenomas but also significant Pgp expression in adenomas [16]. Therefore, the aim of this study was to compare 99mTc MIBI parathyroid imaging results and immunohistochemical analyses of Pgp and MRP expressions in larger parathyroid adenoma.
Methods and mater ials
Patients. Forty-seven patients (31 females, 16 males, ages: 32 - 67 years) with parathyroid adenoma (larger than 1.5 gm) received operations were enrolled in this
retrospective study. Before operations, early and delay (10min and 2hr) 99mTc MIBI parathyroid imaging including neck and chest images, was performed for all of the 47 patients. All of the 47 parathyroid adenomas were obtained for immunohistochemical analysis (IHA) within 2 weeks of the 99mTc MIBI parathyroid imaging.
Technetium-99m Methoxyisobutylisonitrile Parathyroid Imaging. There was a delay of 30 minutes from the time of oral intake of 500mg perchlorate to the start of imaging procedure to prevent abnormal uptake of free 99mTc pertechnetate. A commercial MIBI preparation (max. 5.56 Gb (150mCi) in approximately 1 to 3ml) was obtained from Dupont Company (Cardiolite). The labeling and quality control procedures were carried out according to the manufacturer’s instructions. Labeling efficiencies were consistently higher than 95 percent. In order to detect possible ectopic parathyroid adenoma in the chest, we used a large-field-of-view gamma camera with a low-energy, high-resolution collimator instead of a pinhole device routinely. Early and delay parathyroid imaging was performed 10 minutes and 2 hours after intravenous injection of 740 MBq (20 mCi) 99mTc MIBI on a gamma camera using a 140-keV photo-peak with a 20% window; counts of 500k per view were acquired. The field of the view included the entire neck and chest with the supine position and the neck extended. All of the 99mTc MIBI parathyroid images were retrospectively and visually interpreted agreement by at least two of three nuclear medicine physicians without knowledge of the results of surgery and histopathological diagnosis in each patient. Both early and delay analog 99mTc MIBI parathyroid images of a given patient were placed side by side for comparison. A positive 99mTc MIBI parathyroid imaging finding with the presence of a parathyroid adenoma was defined as a focal area of increased uptake of 99mTc MIBI in the thyroid bed or mediastinum which either progressively increased over time or showed fixed uptake [9].
Immunohistochemical Analyses. All IHC analyses were done at the same time. In this study, 3 to 5 sections of various parts of the tumors were cut by pathologic specialists. Formalin-fixed paraffin sections (5-µm) of surgical specimens of the
parathyroid adenoma were deparaffinized in an oven at 50 for 40 minutes, then hydrated with varying concentrations of ethanol-water dilutions. For MRP
immunohistochemical staining, antigen retrieval was performed by treatment in citrate buffer in a 700 W microwave oven for 5 minutes. Endogenous peroxidase was blocked by 3% hydrogen peroxide for 15 minutes, followed by 5 minutes in phosphate buffer saline (PBS) buffer. The sections were incubated overnight in
moist chamber at 4 with primary antibody MRP QCRL-1 (10ìg/ml, Signet Laboratories, Inc., Dedham, MA, USA) at 1:100 concentration. For Pgp immunohistochemical staining, endogenous peroxidase was blocked by 3% hydrogen peroxide for 15 minutes. Antigen retrieval was performed by treatment with enzyme digestion in 0.1% trypsin in PBS for 5 minutes at room temperature and inhibited with 10% skim milk in PBS for 5 minutes. The sections were incubated for 2 hours in a
moist chamber at 37 -1 (50ìg/ml, Boehringer Mannheim with primary antibody JSB
Biochemica, Germany) at 1:50 concentration. After three 5 minites washes in PBS buffer, detection of the primary antibody was performed with a link antibody according to the manufacturer’s instructions (DAKO LSAB® 2 System, Peroxidase, Dako Corporation, Carpinteria, CA, USA) [17-19]. All specimen evaluations were performed on a Nikon microscope (AFX-DX) using an ocular magnification of ×20 with an eyepiece grid. Positive cells were quantified by evaluating four randomly selected high-power fields (minimum 800 tumor cells). The normal kidney was used as a general positive control [20]. Pgp or MRP expressions was interpreted by an experienced pathologist blinded to clinical outcome as follows: negative = less than 10%, and positive = equal to or more than 10% stained tumor cells.
Statistical Analyses. The incidence differences of positive Pgp or MRP expression between positive and negative 99mTc MIBI parathyroid imaging findings among the 4 groups were assessed by Fisher’ exact or Chi-Square tests. If the p value was < 0.05, the difference was considered significant.
Results
The correlation of parathyroid imaging findings and IHC results are shown in Table 1. The gland size of the parathyroid adenomas relates to Tc-99m MIBI parathyroid imaging findings and immunohistochemical analysis results are shown in Table 2.
99m
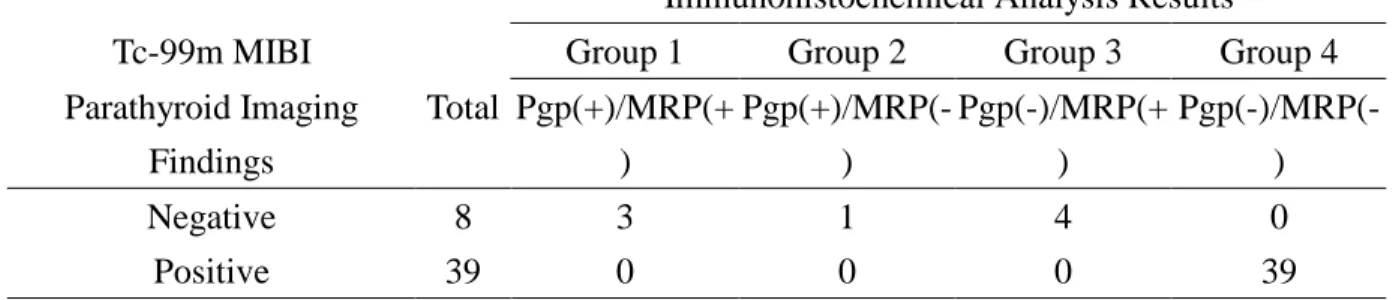
Tc MIBI parathyroid imaging could not detect all of the 3 parathyroid adenomas in the group 1 (3 adenomas with both positive Pgp and positive MRP), group 2 (1 adenoma with positive Pgp but negative MRP expression), and group 3 (4 adenomas with negative Pgp but positive MRP expression). However, 99mTc MIBI parathyroid imaging could detect all of the 39 parathyroid adenomas in the group 4 with both negative Pgp and negative MRP expression. The difference was significant (p value < 0.05).
Discussion
function as an ATP-dependent efflux pump [14,15]. Previous studies [21-23] demonstrated the relationship between 99mTc MIBI tumor uptake with Pgp or MRP expression, and implied a potential for 99mTc MIBI scintigraphy to be used as a non-invasive imaging tool for Pgp or MRP expression assessment. Therefore, in our study, we compared 99mTc MIBI parathyroid imaging results with Pgp or MRP expression by IHA in larger parathyroid adenoma.
99m
Tc MIBI parathyroid imaging also noted that false-negative results have been reported in large adenomas [11,12]. In our study, all of 47 parathyroid adenomas were larger than 1.5gm. In addition, precedent literature [16] supported our findings that Pgp expression correlated with 99m
Tc MIBI parathyroid imaging results. 99m
Tc MIBI parathyroid imaging could not detect all of the 8 parathyroid adenomas with either po sitive Pgp or positive MRP (groups 1 to 3), but it could detect all of the 39 parathyroid adenomas in the group 4 with both negative Pgp and negative MRP expression. Therefore, Pgp or MRP expression in parathyroid adenomas has been postulated to be the other important factor to influence the results of 99m
Tc MIBI parathyroid imaging.
Our study found that there is significant reverse relationship between the results of
99m
Tc MIBI parathyroid imaging and Pgp or MRP expression. We concluded that Pgp or MRP expression play a important role in the false-negative results of 99mTc MIBI parathyroid imaging to localize parathyroid adenoma in addition to tumor size. However, further studies are indicated to confirm the possible methods of decreased false-negative 99mTc MIBI parathyroid imaging results through the use of competitions of inhibitors of the Pgp or MRP pump.
Refer ences
1. Coakley AJ. Parathyroid imaging. Nucl Med Commun 1995; 16: 522-533. 2. Goris ML, Basso LV, Keeling C. Parathyroid imaging. J Nucl Med 1991; 32:
887-889.
3. Miller DL, Doppman JL, Shawker TH, Krudy AG, Norton JA, Vucich JJ, Morrish KA, Marx SJ, Spiegel AM, Aurbach GD. Localization of parathyroid adenomas in patients who have undergone surgery. Part I. Noninvasive imaging methods. Radiology 1987; 62: 133-137.
4. Greenspan BS, Brown ML, Dillehay GL, McBiles M, Sandler MP, Seabold JE, Sisson JC. Procedure guideline for parathyroid scintigraphy. Society of Nuclear Medicine. J Nucl Med 1998; 39: 1111-1114.
5. Casas AT, Burke GJ, Mansberger AR Jr, Wei JP. Impact of technetium-99m-sestamibi localization on operative time and success of operations for primary hyperparathyroidism. Am Surg 1994;60:12-17.
6. Baillet GY, Mena IG, Kuperus JH, Robertson JM, French WJ. Simultaneous technetium-99m MIBI angiography and myocardial perfusion imaging. J Nucl Med 1989; 30: 38-44.
7. Chiu ML, Kronauge JF, Piwnica Worms D. Effect of mitochondrial and plasma membrane potentials on accumulation of hexakis (2-methoxyisobutylisonitrile) technetium(I) in cultured mouse fibroblasts. J Nucl Med 1990; 31: 1646-1653.
8. O'Doherty MJ, Kettle AG, Wells P, Collins RE, Coakley AJ. Parathyroid imaging with technetium-99m-sestamibi: preoperative localization and tissue uptake studies. J Nucl Med 1992; 33: 313-318.
9. Taillefer R, Boucher Y, Potvin C, Lambert R. Detection and localization of parathyroid adenomas in patients with hyperparathyroidism using a single radionuclide imaging procedure with technetium-99m-sestamibi (double-phase study). J Nucl Med 1992; 33: 1801-1807.
10. Melloul M, Paz A, Koren R, Cytron S, Feinmesser R, Gal R. 99mTc-MIBI scintigraphy of parathyroid adenomas and its relation to tumour size and oxyphil cell abundance. Eur J Nucl Med 2001;28:209-213.
11. Leslie WD, Riese KT, Dupont JO, Peterdy AE. Parathyroid adenomas without sestamibi retention. Clin Nucl Med 1995; 20: 699-702.
12. Rauth JD, Sessions RB, Shupe SC, Ziessman HA. Comparison of Tc-99m MIBI and TI-201/Tc-99m pertechnetate for diagnosis of primary hyperparathyroidism. Clin Nucl Med 1996; 21: 602-608.
13. Vergote J, Moretti JL, de Vries EG, Garnier-Suillerot A. Comparison of the kinetics of active efflux of 99mTc-MIBI in cells with P-glycoprotein-mediated
and multidrug-resistance protein-associated multidrug-resistance phenotypes. Eur J Biochem 1998; 252: 140-146.
14. Hendrikse NH, Franssen EJ, van der Graaf WT, Meijer C, Piers DA, Vaalburg W, de Vries EG. 99mTc-sestamibi is a substrate for P-glycoprotein and the multidrug resistance-associated protein. Br J Cancer 1998; 77: 353-358.
15. Takami H, Oshima M, Sugawara I, Satake S, Ikeda Y, Nakamura K, Kubo A. Pre-operative localization and tissue uptake study in parathyroid imaging with technetium-99msestamibi. Aust N Z J Surg 1999; 69: 629-631.
16. Sun SS, Shiau YC, Lin CC, Kao A, Lee CC. Correlation between P-glycoprotein (P-gp) expression in parathyroid and Tc-99m MIBI parathyroid image findings. Nucl Med Biol 2001;28:929-933.
17. Kreisholt J, Sorensen M, Jensen PB, Nielsen BS, Andersen CB, Sehested M. Immunohistochemical detection of DNA topoisomerases IIá, p-glycoprotein and multidrug resistance protein (MRP) in small-cell and non-small-cell lung cancer. Br J Cancer 1998; 77: 1469-1473.
18. Chuman Y, Sumizawa T, Takebayashi Y, Niwa K, Yamada K, Haraguchi M, Furukawa T, Akiyama S, Aikou T. Expression of the multidrug-resistance-associated protein (MRP) gene in human colorectal, gastric and non-small-cell lung carcinomas. Int J Cancer1996; 66: 274-279. 19. Mitchell BK, Cornelius EA, Zoghbi S, Murren JR, Ghoussoub R, Flynn SD,
Kinder BK. Mechanism of technetium 99m sestamibi parathyroid imaging and the possible role of p-glycoprotein. Surgery 1996; 120: 1039-1045.
20. Kao CH, Tsai SC, Wang JJ, Ho YJ, Ho ST, Changlai SP. Technetium-99m-sestamethoxyisobutylisonitrile scan as a predictor of chemotherapy in malignant lymphomas compared with P-glycoprotein expression, multidrug resistance-related protein expression and other prognosis factors. Br J Haematol 2001; 113: 369-374.
21. Kao CH, Tsai SC, Liu TJ, Ho YJ, Wang JJ, Ho ST, ChangLai SP. P-glycoprotein and multidrug resistance-related protein expression in relation to technetium-99m methoxybutylisonitrile scintimammography findings. Cancer Res 2001; 61: 1412-1414.
22. Kao A, Shiau SC, Hsu NY, Sun SS, Lee CC, Lin CC. Technetium-99m methoxybutylisonitrile chest imaging for small-cell lung cancer: relationship to chemotherapy response (six courses of combination of cisplatin and etoposide) and p-glycoprotein or multidrug resistance related protein expression. Ann Oncol 2001;12:1561-1566.
23. Moretti JL, Duran Cordobes M, Starzec A, de Beco V, Vergote J, Benazzouz F, Boissier B, Cohen H, Safi N, Pierno-Neumann S, Kouyoumdjian JC. J Nucl
Table 1. Correlation of Tc-99m MIBI parathyroid imaging findings and immunohistochemical analysis results in parathyroid adenomas
Immunohistochemical Analysis Results
Tc-99m MIBI Group 1 Group 2 Group 3 Group 4
Parathyroid Imaging Findings Total Pgp(+)/MRP(+ ) Pgp(+)/MRP(-) Pgp(-)/MRP(+ ) Pgp(-)/MRP(-) Negative 8 3 1 4 0 Positive 39 0 0 0 39
Table 2. The gland size of the parathyroid adenomas relates to Tc-99m MIBI parathyroid imaging findings and immunohistochemical analysis results
Gland Size of Parathyroid Adenoams (gm)
Tc-99m MIBI Group 1 Group 2 Group 3 Group 4
Parathyroid Imaging Findings Total Pgp(+)/MRP(+) Pgp(+)/MRP(-) Pgp(-)/MRP(+) Pgp(-)/MRP(-) Negative 3.15±1.30 1.50, 2.80, 5.30 2.50 1.80, 3.20, 3.60, 4.50 No Case