ORIGINAL ARTICLE
Certain bio-psychosocial
–spiritual problems associated
with dyspnea among advanced cancer patients in Taiwan
Chih-Te Ho&Hua-Shui Hsu&Chia-Ing Li&
Chiu-Shong Liu&Chin-Yu Lin&Cheng-Chieh Lin&
Wen-Yuan Lin
Received: 28 April 2011 / Accepted: 6 September 2011 # Springer-Verlag 2011
Abstract
Purpose Dyspnea is a multidimensional phenomenon among advanced cancer patients. We aim to explore the association between bio-psychosocial–spiritual prob-lems and dyspnea among advanced cancer patients in Taiwan.
Methods We retrospectively analyzed advanced cancer patients admitted to the hospice palliative ward in a tertiary hospital in Taiwan from 2002 to 2005. A total of 687 consecutive advanced cancer patients were enrolled. Physical, psychosocial, and spiritual problems for each patient were collected. Multiple logistic regression anal-yses were used to evaluate the association between dyspnea and other physical, psychosocial, and spiritual problems.
Results The top four primary sites of cancer among these patients are the liver/biliary tract (19.9%), lung (15.6%), colon/rectum (12.8%), and head/neck (9.9%). During admission period, 260 (37.8%) patients experi-enced dyspnea. For primary cancer types and metastatic locations, subjects with dyspnea tended to have lung cancer, lung metastasis, or brain metastasis. The clinical symptoms/signs related to dyspnea are pain, anorexia, constipation, nausea/vomiting, coughing, pleural effu-sion, edema, anxiety, and propriety preparation problem, that is, arranging one’s will, feelings of isolation, fear of death, and survival. After further adjustments for potential confounders, subjects with problems of propri-ety preparation were found to be strongly associated with dyspnea. The adjusted odds ratio of having
C.-T. Ho
:
H.-S. Hsu:
C.-S. Liu:
C.-C. Lin:
W.-Y. Lin (*) Department of Family Medicine,China Medical University Hospital, 2, Yuh-Der Road,
Taichung, Taiwan 404, Republic of China e-mail: [email protected] C.-T. Ho e-mail: [email protected] H.-S. Hsu e-mail: [email protected] C.-S. Liu e-mail: [email protected] C.-C. Lin e-mail: [email protected] C.-I. Li
Department of Medical Research, China Medical University Hospital, Taichung, Taiwan, Republic of China
e-mail: [email protected]
C.-Y. Lin
Department of Nursing, China Medical University Hospital, Taichung, Taiwan, Republic of China
e-mail: [email protected]
C.-S. Liu
:
C.-C. Lin:
W.-Y. LinSchool of Medicine, China Medical University, Taichung, Taiwan, Republic of China
C.-C. Lin
:
W.-Y. LinGraduate Institute of Clinical Medical Science, China Medical University,
Taichung, Taiwan, Republic of China
C.-C. Lin
Institute of Health Care Administration, College of Health Science, Asia University, Taichung, Taiwan, Republic of China DOI 10.1007/s00520-011-1273-y
dyspnea caused by the problem of propriety preparation was 1.91 (95% confidence interval, 1.15–3.19).
Conclusions Advanced cancer patients with certain psy-chosocial and spiritual problems, such as, the problem of propriety preparation, fear of death, and anxiety, tended to have dyspnea. Among these factors, propriety preparation plays an important role among dyspnea patients. Advanced cancer patients with dyspnea have greater needs for propriety preparation.
Keywords Palliative care . Dyspnea . Propriety . Anxiety . Fear of death . Advanced cancer
Introduction
Dyspnea is a common and distressing symptom in advanced cancer patients. The prevalence of dyspnea increases as death approaches, with 50–70% of ad-vanced cancer patients experiencing dyspnea [3, 5, 11,
12,15,16,18,19,22,26]. The symptoms usually become persistent, uncontrollable, and aggravated as the disease progresses. Previous studies have found that dyspnea troubles 56.6% of advanced cancer patients in Taiwan [4]. Respiratory diseases, cardiovascular diseases, anemia, metabolic abnormalities, and neuropsychiatric factors are the possible causes of dyspnea [1, 2, 9, 26]. In addition, dyspnea is a multidimensional phenomenon; its patho-physiology is not well understood [1,8–10,20,21,23,26,
28,29,31].
Previous studies have found that anxiety is associated with dyspnea among advanced cancer patients [3, 5]. Another study reported that psychological distress, presence of organic causes, cough, and pain are significantly associated with dyspnea in advanced lung cancer patients [21]. Delgado-Guay et al. found that advanced cancer patients with depressive or anxious moods express higher frequency of dyspnea [10].
According to Weisman's description, good death is one in which a patient’s suffering is reduced as much as possible and is accompanied by dignity [27]. Having good death is an important issue in Chinese culture. The problem of dyspnea among advanced cancer patients has strongly influenced the goal of having good death and has deeply bothered the medical staff and families [14]. Many factors, such as organic causes and psychosocial and spiritual factors, may alter dyspnea perception in advanced cancer patients, which have not been well studied in a Chinese population. Therefore, we aim to explore the association between bio-psychosocial–spiritual problems and dyspnea among advanced cancer patients in Taiwan.
Patients and methods
Patients and palliative care setting
In this cross-sectional study, we retrospectively analyzed advanced cancer patients admitted to the Hospice Palliative Care Unit in a tertiary hospital in Taiwan from September 2002 to September 2005. The inclusion criteria include patients aged 20 years and older, patients admitted to the Hospice Palliative Care Unit of the China Medical University Hospital for the first time, and with a level of consciousness clear enough (alert or lethargic conscious-ness) to report symptoms in Mandarin or Taiwanese upon admission. The participants were receiving care provided by a multidisciplinary team consisting of physicians, nurses, psychologists, social workers, clinical Buddhist chaplains, and volunteers. A total of 687 patients were enrolled in this study. Survival was divided into tertiles (I, 1–7 days; II, 8–25 days; III, >25 days). Among 687 individuals, only one patient’s survival could not be confirmed. The study was approved by the ethics committee of the China Medical University Hospital.
Instruments
The assessment tool used was the Symptom Reporting and Clinical Evaluation Forms, which was modified from a previous study and designed by experienced specialists [4,
5, 7, 25]. Upon admission, the measurements of the physical, psychosocial, and spiritual problems of the patients were recorded by the main care-staff members who assessed and recorded the presence or absence of these problems according to patients’ report and clinical evalua-tion. The recorded physical, psychosocial, and spiritual problems of each patient were discussed and confirmed by a multidisciplinary team consisting of physicians, nurses, psychologists, social workers, clinical Buddhist chaplains, and volunteers in a team meeting. Team meetings were held once a week. Data used for this study include routine records, such as demographic data (i.e., age, gender, and primary site of cancer) and the Symptom Reporting and Clinical Evaluation Forms of the patients at the time of admission. Physical problems include pain, fatigue, anorex-ia, dyspnea, cachexanorex-ia, consciousness change, constipation, nausea/vomiting, ascites, cough, pleural effusion, insomnia, jaundice, tumor wound, edema, dysphagia, bleeding, body weight loss, paralysis, lymph edema, incontinence of urine or stool/catheter insertion, pressure ulcers, hallucination, and diarrhea. Psychosocial and spiritual problems include poor awareness of diagnosis; depression; anxiety; emotion-al distress; problem of propriety preparation, that is, arranging one’s will; problems of communication, poor
relationship with families; feelings of isolation; certain family members persisting with their own opinion; unable to make a decision; divarication; problems of bequest management; fear of death; inability to reconcile with the disease; agony; feelings of helplessness, hopelessness, or emptiness; blaming God and man; suicide ideation, guilty conscience; and problems with feelings of gratitude or resentment.
Statistical analysis
Descriptive statistics was summarized as frequencies and percentages for categorical variables; mean and standard deviation (SD) was used for other continuous variables. The Student’s t test and Chi-square test were used as indicated. Multivariate logistic regression analyses were used to estimate the adjusted odds ratios (ORs) and their 95% confidence intervals for the presence of dyspnea in
relation to other factors. All statistical tests were two sided at the 0.05 significance level. These statistical analyses were performed using the PC version of the SPSS statistical software (13th version, SPSS Inc., Chicago, IL, USA).
Results
Characteristics of the study population
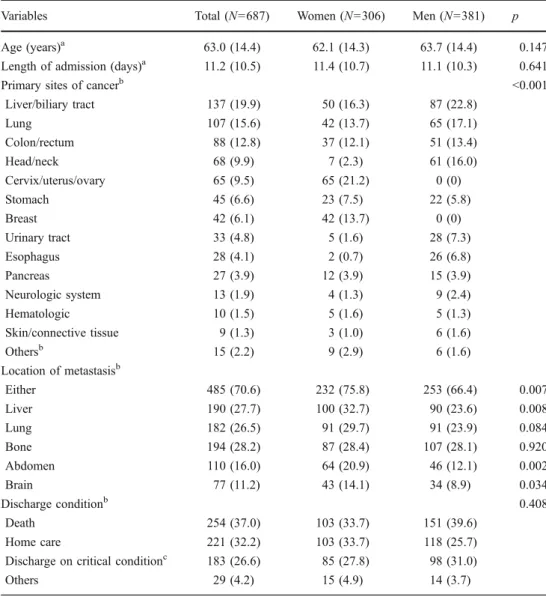
The demographic characteristics of 687 consecutive patients between genders are summarized in Table 1. Among them, 381(55.5%) were men. The mean (SD) age and length of stay were 63.0 (14.4) years and 11.2 (10.5) days, respectively. The top three primary sites of cancer were the liver/biliary tract (19.9%), lung (15.6%), and colon/rectum (12.8%) (Table1).
Table 1 Baseline characteristics of advanced cancer patients by gender
Present with mean (SD) or N (%) as indicated
a
Continuous variables test using Student’s t test between men and women
b
Categorical variables test using chi-square test between men and women
c
Discharge on critical condition: dying at home, wishes of patients or their families
Variables Total (N=687) Women (N=306) Men (N=381) p
Age (years)a 63.0 (14.4) 62.1 (14.3) 63.7 (14.4) 0.147
Length of admission (days)a 11.2 (10.5) 11.4 (10.7) 11.1 (10.3) 0.641
Primary sites of cancerb <0.001
Liver/biliary tract 137 (19.9) 50 (16.3) 87 (22.8) Lung 107 (15.6) 42 (13.7) 65 (17.1) Colon/rectum 88 (12.8) 37 (12.1) 51 (13.4) Head/neck 68 (9.9) 7 (2.3) 61 (16.0) Cervix/uterus/ovary 65 (9.5) 65 (21.2) 0 (0) Stomach 45 (6.6) 23 (7.5) 22 (5.8) Breast 42 (6.1) 42 (13.7) 0 (0) Urinary tract 33 (4.8) 5 (1.6) 28 (7.3) Esophagus 28 (4.1) 2 (0.7) 26 (6.8) Pancreas 27 (3.9) 12 (3.9) 15 (3.9) Neurologic system 13 (1.9) 4 (1.3) 9 (2.4) Hematologic 10 (1.5) 5 (1.6) 5 (1.3) Skin/connective tissue 9 (1.3) 3 (1.0) 6 (1.6) Othersb 15 (2.2) 9 (2.9) 6 (1.6) Location of metastasisb Either 485 (70.6) 232 (75.8) 253 (66.4) 0.007 Liver 190 (27.7) 100 (32.7) 90 (23.6) 0.008 Lung 182 (26.5) 91 (29.7) 91 (23.9) 0.084 Bone 194 (28.2) 87 (28.4) 107 (28.1) 0.920 Abdomen 110 (16.0) 64 (20.9) 46 (12.1) 0.002 Brain 77 (11.2) 43 (14.1) 34 (8.9) 0.034 Discharge conditionb 0.408 Death 254 (37.0) 103 (33.7) 151 (39.6) Home care 221 (32.2) 103 (33.7) 118 (25.7)
Discharge on critical conditionc 183 (26.6) 85 (27.8) 98 (31.0)
Comparison of related factors in patients with and without dyspnea by univariate analysis
At the time of the study, 260 (37.8%) patients suffered from dyspnea. Using the Chi-square test, the factors significantly associated with dyspnea were determined as survival, lung cancer, lung metastasis, brain metastasis, pain, anorexia, constipation, nausea/vomiting, coughing, pleural effusion, edema, anxiety, and problem of propriety preparation, that is, arranging one’s will, feelings of isolation, and fear of death (Tables 2 and 3). The prevalence of dyspnea was signifi-cantly higher in subjects with short survival, lung cancer, lung metastasis, brain metastasis, cough, pleural effusion, edema, anxiety, propriety preparation, and fear of death than in those without. There was no statistically significant difference in the prevalence of dyspnea between genders.
Related factors of dyspnea by multivariate logistic regression
Using multivariate logistic regression analyses with adjust-ment for potential confounders, the adjusted OR of having dyspnea among subjects with lung cancer and/or lung metastasis was 3.06 (95% CI, 1.80–5.19) and 2.71 (1.81– 4.07), respectively (Table 4). Among the physical factors, subjects with cough, pleural effusion, and edema were more likely to have dyspnea (OR, 3.04 (95% CI, 1.83–5.05); OR, 4.77 (95% CI, 2.68–8.50); and OR, 2.09 (95% CI, 1.13– 3.89), respectively). Among psychosocial–spiritual factors, subjects with propriety preparation problem, anxiety, and fear of death were more likely to have dyspnea (OR, 1.91 (95% CI, 1.15–3.19); OR, 1.45 (95% CI, 0.96–2.20); and OR, 1.58 (95% CI, 0.99–2.53), respectively). However,
Table 2 Demographic charac-teristics according to dyspnea status among advanced cancer patients
Present with mean (SD) or N (%) as indicated
aContinuous variables test using
Student’s t test between subjects with and without dyspnea
bCategorical variables test using
chi-square test between subjects with and without dyspnea
c
Survival was divided by ter-tiles. Among 687 individuals, only one patient’s survival was not confirmed
d
Discharge on critical condition: dying at home and wishes of patients or their families
Variables Dyspnea (N=260) No dyspnea(N=427) p
Age (years)a 63.1 (15.1) 62.8 (14.0) 0.188
Genderb
Women 114 (43.8) 192 (45) 0.775
Men 146 (56.2) 235 (55)
Length of admission (days)b
1 to 7 133 (51.2) 193 (45.2) 0.271 8 to 14 59 (22.7) 116 (27.2) >14 68 (26.1) 118 (27.6) Education (years)b <7 142 (54.6) 232 (54.3) 0.822 7 to 12 92 (35.4) 146 (34.2) >12 26 (10) 49 (11.5) Discharge conditionb Death 107 (41.2) 147 (34.4) 0.245
Discharge on critical conditiond 68 (26.2) 115 (26.9)
Home care 77 (29.6) 144 (33.7)
Others 8 (3.1) 21 (4.9)
Survival (days (mean (SD), median)) 26.2 (49.7, 11) 38.0 (89.8, 16)
Survival I (n=234c; 1 to 7 days) 108 (41.7) 126 (29.5) <0.001
Survival II (n=226c; 8 to 25 days) 84 (32.4) 142 (33.3)
Survival III (n=226c; >25 days) 67 (25.9) 159 (37.2)
Primary cancer sitesb
Lung 71 (27.3) 36 (8.4) <0.001 Other cancers 189 (72.7) 391 (91.6) Location of metastasisb Either 195 (75.0) 290 (67.9) 0.048 Liver 67 (25.8) 123 (28.8) 0.388 Lung 99 (38.1) 83 (19.4) <0.001 Bone 83 (31.9) 111 (26) 0.094 Abdomen 35 (13.5) 75 (17.6) 0.155 Brain 38 (14.6) 39 (9.1) 0.027
subjects with anorexia were less likely to have dyspnea (OR, 0.64; 95% CI, 0.42–0.96) (Table4)
Discussion
We demonstrated that dyspnea was significantly correlated with lung cancer, lung metastasis, cough, pleural effusion, edema, propriety preparation, and anorexia among ad-vanced cancer patients. Adad-vanced cancer patients with certain psychosocial and spiritual problems, such as, propriety preparation problem, fear of death, and anxiety,
tended to have dyspnea. Among these factors, propriety preparation plays an important role among dyspnea patients.
Weisman’s definition of good death, which was modified in accordance with Chinese and Taiwanese culture, consists of five factors, namely, (1) awareness, awareness of one’s dying; (2) acceptance, accepting death peacefully; (3) propriety, arranging one’s will; (4) timeliness, death timing, and (5) comfort, degree of physical comfort 3 days before death [24,27,30]. Propriety, that is, arranging one’s will is
an important factor of good death. We found that dyspnea among advanced cancer patients was significantly
correlat-Table 3 Prevalence of physical, psychosocial, and spiritual factors according to dyspnea status among advanced cancer patients
Present with N (%) and test using Chi-square test
aThe assessment tool used was
the Symptom Reporting and Clinical Evaluation Forms. Upon admission, the measure-ments of patients’ physical, psy-chosocial, and spiritual problems were recorded by the main care-staff members who assessed and recorded the presence or absence of these problems according to patients’ reports and clinical eval-uation. The recorded physical, psychosocial, and spiritual prob-lems of each patient were dis-cussed and confirmed by a multidisciplinary team consisting of physicians, nurses, psycholo-gists, social workers, clinical Buddhist chaplains, and volun-teers in a team meeting. Team meetings were held once a week
Variables Dyspnea (N=260) No dyspnea (N=427) p
Physical factorsa Pain 199 (76.5) 363 (85) 0.005 Fatigue 171 (65.8) 288 (67.4) 0.651 Anorexia 142 (54.6) 288 (67.4) 0.001 Cachexia 90 (34.6) 162 (37.9) 0.381 Conciousness change 80 (30.8) 120 (28.1) 0.456 Constipation 62 (23.8) 135 (31.6) 0.029 Nausea/vomiting 52 (20) 141 (33) <0.001 Ascites 44 (16.9) 73 (17.1) 0.953 Cough 69 (26.5) 36 (8.4) <0.001 Pleural effusion 71 (27.3) 21 (4.9) <0.001 Insomnia 28 (10.8) 56 (13.1) 0.363 Jaundice 25 (9.6) 58 (13.6) 0.122 Tumor wound 23 (8.8) 46 (10.8) 0.415 Edema 40 (15.4) 25 (5.9) <0.001 Dysphagia 30 (11.5) 33 (7.7) 0.093 Bleeding 20 (7.7) 42 (9.8) 0.342
Body weight loss 16 (6.2) 41 (9.6) 0.112
Psychosocial and spiritual factorsa
Poor awareness of diagnosis 120 (46.2) 179 (41.9) 0.278
Depression 111 (42.7) 176 (41.2) 0.704
Anxiety 95 (36.5) 105 (24.6) 0.001
Other emotional distress 74 (28.5) 103 (24.1) 0.207
Others psychosocial problems 51 (19.6) 84 (19.7) 0.986
Propriety preparation 52 (20) 45 (10.5) 0.001
Problems of communication 41 (15.8) 49 (11.5) 0.106
Poor relationship with families 23 (8.8) 55 (12.9) 0.106
Feeling of isolation 12 (4.6) 39 (9.1) 0.028
Unable to make a decision 17 (6.5) 15 (3.5) 0.068
Divarication 3 (1.2) 14 (3.3) 0.082
Problems of bequest management 3 (1.2) 7 (1.6) 0.606
Fear of death 59 (22.7) 71 (16.6) 0.049
Inability to reconcile with the disease 47 (18.1) 69 (16.2) 0.515
Agony 29 (11.2) 52 (12.2) 0.686
Helplessness/hopelessness 31 (11.9) 48 (11.2) 0.786
ed with the propriety preparation problem. To our knowl-edge, this is the first study comparing the propriety preparation problem with dyspnea among advanced cancer patients. The possible problems of propriety preparation were “no reference to the patient’s will” and “conflict between the patient’s will and that of the family.” The Buddhist funeral ceremony adjusted for Confucian culture, Taoism, and Taiwanese folk religion is one of the most common funeral ceremonies in Taiwan. Funeral ceremonies and the place of death are very important for most people in Taiwan. The Chinese saying,“Luo Yeh Guei Gen,” reflects the traditional beliefs in having a good death, stating that dying at home is as natural as the leaves falling down to the roots of a tree [30]. One possible conflict between the will of the patient and that of the family is that some patients wish to die at home, but their families want them to remain in the hospital until their death [30]. The reasons may be related to“the patient’s families worrying that they cannot handle the patient suffering at home” and “no caregivers are
available to care for the dying patient all day.” In addition, with the earlier involvement of hospice care in the cancer treatment, a continuous relationship among the hospice staff, cancer patients, and their families will grow, contrib-uting to better discharge planning, propriety preparation, and death preparation for palliative home care [30]. A possible explanation for the association between propriety preparation and dyspnea is that the problem of propriety preparation may lead to psychological distress, which may cause dyspnea, according to previous studies on lung cancer patients [21]. Chochinov et al. reported that as death draws near, psychological variables are replaced by physical mediators of variation in the will to live and that the four main predictor variables of the will to live are depression, anxiety, shortness of breath, and sense of well-being [6]. These findings also suggest another explanation for the relationship among dyspnea, low will to live, and propriety preparation. Our results suggest that the appro-priate management of the propriety preparation problem by
Table 4 Unadjusted and adjusted ORs (95% confidence interval) of having dyspnea among advanced cancer patients using logistic regression analysis in different models, adjusted for potential confounders
Variables Model 1a Model 2b Model 3c
Primary cancer sites and location of metastasis
Lung cancer 4.08 (2.64–6.32)* 3.17 (1.88–5.32)* 3.06 (1.80–5.19)*
Lung metastasis 2.55 (1.80–3.60)* 2.65 (1.79–3.94)* 2.71 (1.81–4.07)*
Brain metastasis 1.70 (1.06–2.74)** 0.97 (0.54–1.73) 1.21 (0.66–2.20)
Survival
Survival I (n=234)d 1.00 (reference) 1.00 (reference) 1.00 (reference)
Survival II (n=226)d 0.69 (0.48–1.00) 0.58 (0.37–0.90)** 0.57 (0.36–0.89)** Survival III (n=226)d 0.49 (0.34–0.72)* 0.47 (0.30–0.74)*** 0.46 (0.29–0.73)*** Physical factors Pain 0.58 (0.39–0.85)** 0.69 (0.44–1.09) 0.65 (0.40–1.04) Anorexia 0.58 (0.42–0.80)*** 0.67 (0.45–0.99)** 0.64 (0.42–0.96)** Constipation 0.68 (0.48–0.96)** 0.69 (0.46–1.05) 0.76 (0.50–1.17) Nausea/vomiting 0.51 (0.35–0.73)* 0.73 (0.47–1.14) 0.77 (0.49–1.23) Cough 3.92 (2.53–6.08)* 2.90 (1.77–4.74)* 3.04 (1.83–5.05)* Pleural effusion 7.26 (4.33–12.17)* 5.34 (3.05–9.37)* 4.77 (2.68–8.50)* Edema 2.92 (1.73–4.95)* 2.51 (1.38–4.56)*** 2.09 (1.13–3.89)**
Psychosocial and spiritual factors
Anxiety 1.77 (1.26–2.47)*** 1.40 (0.94–2.07) 1.45 (0.96–2.20) Propriety preparation 2.12 (1.38–3.27)*** 2.09 (1.27–3.44)*** 1.91 (1.15–3.19)** Feeling of isolation 0.48 (0.25–0.94)** 0.73 (0.35–1.51) 0.72 (0.34–1.52) Fear of death 1.47 (1.00–2.17)** 1.67 (1.06–2.61)** 1.58 (0.99–2.53) *p<0.001; **p<0.05; ***p<0.01 a Unadjusted
bAdjusted for lung cancer, lung metastasis, brain metastasis, pain, anorexia, constipation, nausea/vomiting, cough, pleural effusion, and edema c
Adjusted for lung cancer, location of metastasis, pain, anorexia, constipation, nausea/vomiting, cough, pleural effusion, edema, anxiety, propriety preparation, feeling of isolation, fear of death, and survival (survival I as reference)
d
a multidisciplinary hospice care team and hospice home care may be beneficial for good death and improving dyspnea among advanced cancer patients. Therefore, patients with dyspnea have greater needs for propriety preparation.
Gysels et al. reported that chronic obstructive pulmonary disease patients with breathlessness are usually isolated and become invisible, and a palliative care approach is promoted and essential priorities are identified to reduce barriers to access [13]. However, our results suggest that feelings of isolation are not associated with dyspnea after adjusting for related factors (Table4, model 3; OR, 0.72; 95% CI, 0.34–1.52). The possible explanation is that hospice admission cancer patients receive initial hospice palliative care consultations or hospice outpatient-clinic visits. Therefore, early hospice palliative care may improve the feelings of isolation among advanced cancer patients.
Although fear of death and anxiety were not significant-ly associated with increased risks of dyspnea after adjust-ment for other confounders among advanced cancer patients, the positive association was similar to other studies [3,5,10, 17]. For example, Bruera et al. reported that anxiety is associated with dyspnea [3]. Delgado-Guay et al. also found that patients with anxiety are more likely to have dyspnea [10]. The possible reason for this result may be due to the small sample size in our study.
Our results suggest that patients with anorexia are less likely to have dyspnea (Table4, model 3) and that cachexia is not significantly related to dyspnea. However, Dudgeon et al. reported that cachexia is one of the causes of dyspnea indirectly caused by cancer [12]. To our knowledge, no similar study has investigated the relationship between cachexia and dyspnea after adjusting for primary cancer, metastasis, and other psychosocial–spiritual problems. Further research is required to clarify the mechanism linking anorexia, cachexia, and dyspnea.
Some limitations of this study should be noted. First, the study is cross-sectional, and causality remains to be determined. Further longitudinal studies can provide better evidence. Second, the participants were inpatients in a hospice palliative care unit in Taiwan; therefore, the results of this study may not apply to other races or cultures.
Conclusions
Advanced cancer patients with certain psychosocial and spiritual problems, such as, the propriety preparation problem, fear of death, and anxiety are more likely to suffer from dyspnea. After adjusting for lung cancer, location of metastasis, and physical–psychosocial–spiritual factors, advanced cancer patients with dyspnea were found to have greater needs for propriety preparation.
Financial disclosure None reported.
Funding/support This study was financially supported by grants from the National Science Council of Taiwan (NSC94-2314-B-039-025, NSC95-2314-B-039-008, and NSC96-2314-B-039-015) and China Medical University Hospital (DMR-96-118, DMR-97-067, DMR-98-090, and DMR-99-110).
Reference
1. Ben-Aharon I, Gafter-Gvili A, Paul M, Leibovici L, Stemmer SM (2008) Interventions for alleviating cancer-related dyspnea: a systematic review. J Clin Oncol 26:2396–2404
2. Booth S, Moosavi SH, Higginson IJ (2008) The etiology and management of intractable breathlessness in patients with ad-vanced cancer: a systematic review of pharmacological therapy. Nat Clin Pract Oncol 5:90–100
3. Bruera E, Schmitz B, Pither J, Neumann CM, Hanson J (2000) The frequency and correlates of dyspnea in patients with advanced cancer. J Pain Symptom Manage 19:357–362
4. Chiu TY, Hu W, Chen C (2000) Prevalence and severity of symptoms in terminal cancer patients: a study in Taiwan. Support Care Cancer 8:311–313
5. Chiu TY, Hu WY, Lue BH, Yao CA, Chen CY, Wakai S (2004) Dyspnea and its correlates in Taiwanese patients with terminal cancer. J Pain Symptom Manage 28:123–132
6. Chochinov HM, Tataryn D, Clinch JJ, Dudgeon D (1999) Will to live in the terminally ill. Lancet 354:816–819
7. Chuang RB, Hu WY, Chiu TY, Chen CY (2004) Prediction of survival in terminal cancer patients in Taiwan: constructing a prognostic scale. J Pain Symptom Manage 28:115–122
8. Corner J, Plant H, A'Hern R, Bailey C (1996) Non-pharmacological intervention for breathlessness in lung cancer. Palliat Med 10:299– 305
9. Cuervo Pinna MA, Mota Vargas R, Redondo Moralo MJ, Correas MA (2008) Pharmacologic intervention for cancer-related dys-pnea. J Clin Oncol 26:4225 (author reply 4226)
10. Delgado-Guay M, Parsons HA, Li Z, Palmer JL, Bruera E (2009) Symptom distress in advanced cancer patients with anxiety and depression in the palliative care setting. Support Care Cancer 17:573–579
11. Drings P (1999) Dyspnea in cancer patients. Support Care Cancer 7:215–216
12. Dudgeon DJ, Kristjanson L, Sloan JA, Lertzman M, Clement K (2001) Dyspnea in cancer patients: prevalence and associated factors. J Pain Symptom Manage 21:95–102
13. Gysels M, Higginson IJ (2008) Access to services for patients with chronic obstructive pulmonary disease: the invisibility of breathlessness. J Pain Symptom Manage 36:451–460
14. Hu WY, Chiu TY, Cheng SY, Chen CY (2004) Morphine for dyspnea control in terminal cancer patients: is it appropriate in Taiwan? J Pain Symptom Manage 28:356–363
15. Mancini I, Body JJ (1999) Assessment of dyspnea in advanced cancer patients. Support Care Cancer 7:229–232
16. Potter J, Hami F, Bryan T, Quigley C (2003) Symptoms in 400 patients referred to palliative care services: prevalence and patterns. Palliat Med 17:310–314
17. Reddy SK, Parsons HA, Elsayem A, Palmer JL, Bruera E (2009) Characteristics and correlates of dyspnea in patients with advanced cancer. J Palliat Med 12:29–36
18. Ripamonti C (1999) Management of dyspnea in advanced cancer patients. Support Care Cancer 7:233–243
19. Ripamonti C, Fusco F (2002) Respiratory problems in advanced cancer. Support Care Cancer 10:204–216
20. Smith EL, Hann DM, Ahles TA, Furstenberg CT, Mitchell TA, Meyer L, Maurer LH, Rigas J, Hammond S (2001) Dyspnea, anxiety, body consciousness, and quality of life in patients with lung cancer. J Pain Symptom Manage 21:323–329
21. Tanaka K, Akechi T, Okuyama T, Nishiwaki Y, Uchitomi Y (2002) Factors correlated with dyspnea in advanced lung cancer patients: organic causes and what else? J Pain Symptom Manage 23:490–500
22. Tanaka K, Akechi T, Okuyama T, Nishiwaki Y, Uchitomi Y (2002) Prevalence and screening of dyspnea interfering with daily life activities in ambulatory patients with advanced lung cancer. J Pain Symptom Manage 23:484–489
23. Thomas JR, von Gunten CF (2002) Clinical management of dyspnoea. Lancet Oncol 3:223–228
24. Tsai JS, Wu CH, Chiu TY, Hu WY, Chen CY (2005) Fear of death and good death among the young and elderly with terminal cancers in Taiwan. J Pain Symptom Manage 29:344–351
25. Tsai JS, Wu CH, Chiu TY, Hu WY, Chen CY (2006) Symptom patterns of advanced cancer patients in a palliative care unit. Palliat Med 20:617
26. Viola R, Kiteley C, Lloyd NS, Mackay JA, Wilson J, Wong RK (2008) The management of dyspnea in cancer patients: a systematic review. Support Care Cancer 16:329–337
27. Weisman AD (1988) Appropriate death and the hospice program. Hosp J 4:65
28. Wilcock A, Crosby V, Hughes A, Fielding K, Corcoran R, Tattersfield AE (2002) Descriptors of breathlessness in patients with cancer and other cardiorespiratory diseases. J Pain Symptom Manage 23:182–189
29. Williams CM (2006) Dyspnea. Cancer J 12:365–373
30. Yao CA, Hu WY, Lai YF, Cheng SY, Chen CY, Chiu TY (2007) Does dying at home influence the good death of terminal cancer patients? J Pain Symptom Manage 34:497–504
31. Zhao I, Yates P (2008) Non-pharmacological interventions for breathlessness management in patients with lung cancer: a systematic review. Palliat Med 22:693–701