A Population-Based Nested Case-Control Study: The Use of 5-Alpha-Reductase Inhibitors and the Increased Risk of Osteoporosis Diagnosis in Patients With Benign Prostate Hyperplasia
Running title: 5-Alpha-Reductase Inhibitors and Osteoporosis Diagnosis
Wen-Ling Lin1, 2, Yow-Wen Hsieh1,2, Cheng-Li Lin3, Fung-Chang Sung3,4, Chieh-Hsi Wu2, Chia-Hung Kao4,5
1Department of Pharmacy, China Medical University Hospital, Taichung, Taiwan
2Institute of Pharmacy, China Medical University, Taichung, Taiwan
3Management Office for Health Data, China Medical University Hospital, Taichung,
Taiwan
4Graduate Institute of Clinical Medical Science and School of Medicine, College of
Medicine, China Medical University, Taichung, Taiwan
5Department of Nuclear Medicine and PET Center, China Medical University
Hospital, Taichung, Taiwan
Wen-Ling Lin and Yow-Wen Hsieh contributed equally to this study.
University, No. 2, Yuh-Der Road, Taichung 40447, Taiwan. Tel.: +886-4-22052121 ext.7412, Fax: +886-4-22336174, E-mail: [email protected]
These authors’ individual contributions were as follows. Conception and design: Wen-Ling Lin, Yow-Wen Hsieh, Chieh-Hsi Wu, Chia-Hung Kao. Administrative support: Cheng-Li Lin, Fung-Chang Sung. Collection and assembly of data: Wen-Ling Lin, Yow-Wen Hsieh, Chieh-Hsi Wu, Chia-Hung Kao. Data analysis and interpretation: Cheng-Li Lin, Chia-Hung Kao. Manuscript writing: All authors. Final approval of manuscript: All authors
Funding
The study was supported by grants from the China Medical University Hospital (DMR-102-014 and DMR-102-023); Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW103-TDU-B-212-113002); Health and welfare surcharge of tobacco products, China Medical University Hospital Cancer Research Center of Excellence (MOHW103-TD-B-111-03, Taiwan); and International Research-Intensive Centers of Excellence in Taiwan (I-RiCE) (NSC101-2911-I-002-303).
ABSTRACT
Background: 5-alpha-reductase inhibitors (5ARIs) are the potent androgen
responsible for the development and enlargement of the prostate gland by decreasing dihydrotestosterone (DHT). This results in inhibition of the conversion of testosterone to dihydrotestosterone and markedly suppresses serum dihydrotestosterone levels [1]. Testosterone replacement therapy improves bone density in men with hypogonadal osteoporosis. This study explores the possible association between the use of 2 typical 5ARIs (finasteride and dutasteride) and the subsequent risk of osteoporosis diagnosis.
Methods: We identified 1352 osteoporosis diagnosis cases and 5387 control cases
without osteoporosis diagnosis from the claims data for patients with benign prostate hyperplasia (BPH), which are collected in the Taiwanese National Health Insurance Research Database (NHIRD). Four controls were frequency matched to each case according to age (every 5 years) and diagnosis date. We measured the effect of 5ARIs and determined the adjusted odds ratios (ORs) with 95% confidence intervals (CIs).
Results: We observed a 1.54-fold increase in osteoporosis diagnosis among patients
with BPH using finasteride (95% CI, 1.02-2.32). Furthermore, a dosage analysis showed that higher doses of finasteride were associated with higher osteoporosis diagnosis risk (OR = 1.68; 95% CI, 1.01-2.81), relative to the patients not using 5ARIs.
Conclusion: This population-based nested case-control study suggests that the use of
finasteride can increase the risk of osteoporosis diagnosis among patients with BPH. The effects were more prominent in patients using higher doses of finasteride.
Keywords: 5-alpha-reductase inhibitors (5ARIs); osteoporosis diagnosis; benign prostate hyperplasia
INTRODUCTION
Osteoporosis is a disease of the bones that leads to an increased risk of fractures [2]. In the treatment of benign prostatic hyperplasia, finasteride decreases
dihydrotestosterone (DHT), which is the potent androgen responsible for the
development and enlargement of the prostate gland. Serum concentrations of DHT are reduced by 70% with daily dosing of finasteride 5 mg [3]. A 70-year-old man taking finasteride (5 mg/day) for several years developed progressive weakness of the arms and legs, combined with respiratory distress. Drug cessation resulted in a gradual increase of muscle strength, and dyspneic symptoms improved over a 1-month period [4]. Many of the physical and behavioral changes that occur in men as they age are similar to those that occur in younger men with hypogonadism. These changes include decreased muscle mass, strength, bone mass, and sexual function, and increased body fat, fatigue, and depression. It is therefore reasonable to consider whether testosterone deficiency contributes to the adverse physical and behavioral changes of aging and whether these could be ameliorated by the administration of testosterone [5].
Benign prostate hyperplasia (BPH) is the most common prostate disease in men 60 years and older, and patients may require medication to relieve urinary symptoms. Androgens play a critical role in prostatic growth and contribute to the pathogenesis
of prostate disease [6-7].The 5-alpha-reductase inhibitors (5ARIs) convert
testosterone into the more potent dihydrotestosterone (DHT), and enhance androgenic signals in tissue [8]. Finasteride and dutasteride are 2 well-known 5ARIs that are used to treat BPH. Both agents result in similar volume reductions in prostate glands and the relief of urinary symptoms. In addition, both agents achieve long-term results [9]. Currently, no related research exists on the use of 5ARIs and the increased risk of osteoporosis in patients with BPH. One of the major secondary causes of osteoporosis in men is hypogonadism, which is observed in nearly 20% of men with symptomatic vertebral fractures and 50% of elderly men with hip fractures [10].Although the pathogenesis of osteoporosis in men is multi-factorial, testosterone is known to play a critical role in the maintenance of the male skeleton. Testosterone replacement
therapy improves bone density in men with hypogonadal osteoporosis, particularly if the epiphyses remain open [11].
Thus, it is reasonable to evaluate the association between the use of 5ARIs and osteoporosis diagnosis because the literature comprises only 4 comprehensive studies. We conducted this study by using data from the National Health Insurance (NHI) system in Taiwan and analyzed the risk for osteoporosis diagnosis and the use of 5ARIs.
MATERIALS
Data source
The National Health Insurance (NHI) program, a universal health program established in 1995, covers approximately 99% of the population (23.74 million people) and is contracted with 97% of the hospitals and clinics in Taiwan [12].In this study we used reimbursement claims data of the Longitudinal Health Insurance Database (LHID) established by the National Health Research Institute (NHRI) of the Department of Health. The database includes claims data for one million people covered by the NHI from 1996-2010. No significant difference exists in the distribution of gender and age between LHID and all beneficiaries. We used the scrambled identification numbers to link data sets and safeguard the confidentiality of the insured population, avoiding ethical violations. In addition, this study was
approved by the Institutional Review Board of China Medical University in Central Taiwan (CMU-REC-101-012).
Study sample
This study was conducted as a nested case-control study. First, we used the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) to identify newly diagnosed BPH patients (ICD-9-CM codes 600.xx; n = 46,997)
as the exposure cohort (Figure 1). We excluded patients with a history of osteoporosis diagnosis before January 1, 2005. Each patient was followed from 2005-2010.
Patients with a diagnosis of osteoporosis (ICD-9-CM codes 733.0) became part of the case group and patients without an osteoporosis diagnosis became part of the non-osteoporosis diagnosis group. As a comparison group, we randomly selected 4 people from the non-osteoporosis diagnosis group and frequency matched them to each patient of the case group based on age, BPH year, osteoporosis diagnosis index year, and osteoporosis diagnosis index month. In total, we included 1352 patients in the osteoporosis diagnosis case group and 5387 in the non-osteoporosis diagnosis control group.
The diseases considered as comorbidities included hypertension (ICD-9- CM codes 401 to 405), diabetes (ICD-9-CM code 250), hyperlipidemia (ICD-9-CM code 272), chronic obstructive pulmonary disease (COPD)(ICD-9-CM codes 490-496), obesity ((ICD-9-CM code 278), lower urinary tract strictures (ICD-9-CM codes596.0, 598, 599.6), ureteral catheterization(ICD-9-CM procedural codes 59.8) and
testosterone treatment. The average daily dose of finasteride and dutasteride, which were counted when patient finasteride or dutasteride prescriptions prior to within 2 years of and at index, and calculated the average exposure as total finasteride or dutasteride exposure (mg) divided by the period between within 2 years of and at
index (per day). Finasteride or dutasteride average exposure is partitioned in to 2 segments by median. Medications were classified into 3 groups: none (control), dutasteride, and finasteride.
Statistical analysis
We compared the distributions of demographic characteristics, medication use, and comorbidity between the osteoporosis diagnosis and the non-osteoporosis diagnosis groups, using the Chi-square test. We then calculated the odds ratio (OR; the ratio of osteoporosis diagnosis risk for medication user to that for non-user) and a 95% confidence interval (95% CI), using the multivariable logistic regression model. The multivariable models were simultaneously adjusted for demographic
characteristics, comorbidities of hypertension, diabetes, hyperlipidemia, COPD, obesity, lower urinary tract strictures, and treatment of testosterone, and ureteral catheterization. Models were also used for estimating the risk between the dosages of dutasteride and finasteride for osteoporosis diagnosis.
RESULTS
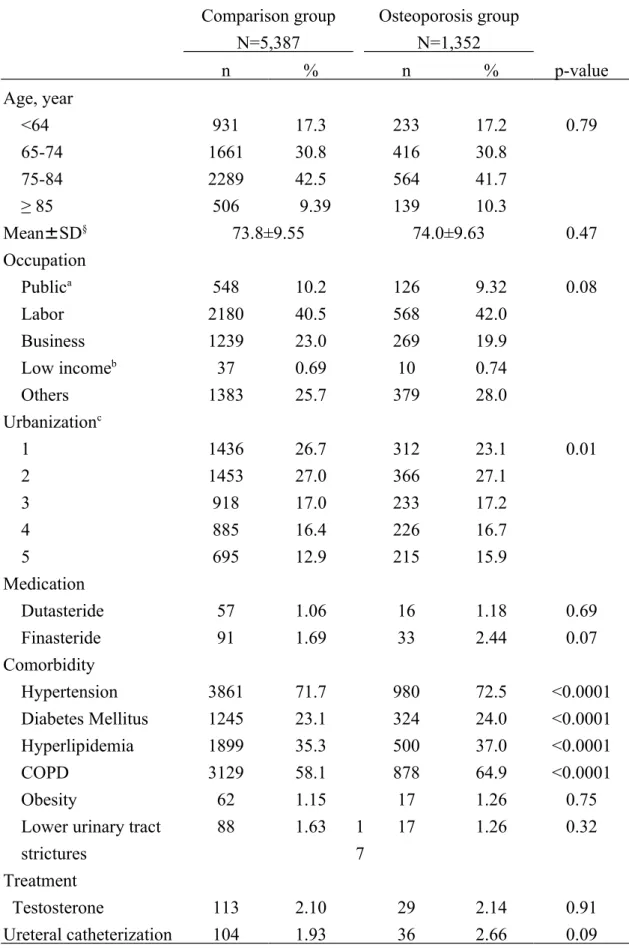
Table 1 shows a comparison of distributions of demographic characteristics, medication, and baseline comorbidity between the osteoporosis diagnosis and the
non-osteoporosis diagnosis groups. Among the 1352 patients with osteoporosis diagnosis, most were between 65 and 84 years of age (72.5%). The mean age was 74.0 ± 9.63 years for the osteoporosis diagnosis group and 73.8 ± 9.55 years for the non-osteoporosis diagnosis comparison group. The distributions of medication use between patients with osteoporosis diagnosis (1.18% for dutasteride, 2.44% for finasteride) and patients with non-osteoporosis diagnosis (1.06% for dutasteride, 1.69% for finasteride) did not differ substantially between the 2 groups. The
osteoporosis diagnosis group was more likely to have hypertension, diabetes mellitus, hyperlipidemia, and COPD compared with the non-osteoporosis diagnosis group (all p-value <0.0001). The results of the multivariate logistic regression model of
medication use associated with osteoporosis diagnosis risk in patients with BPH are shown in Table 2. Overall, compared with patients not using 5ARIs, we observed a 1.54-fold significant increase of osteoporosis diagnosis in patients with BPH using finasteride (95% CI, 1.02-2.33). The results of the medication dosage analysis are shown in Table 3. We observed that higher doses of finasteride are associated with a higher osteoporosis diagnosis risk (OR = 1.70; 95% CI, 1.01-2.84), relative to the patients not using 5ARIs.
DISCUSSION
Approximately 5% of the serum testosterone produced in men undergoes 5 alpha-reduction to form the more potent androgen DHT [13].During embryogenesis, DHT affects the development of the male external genitalia. In adults, DHT affects the prostate and hair follicles [14].Two 5ARI isoenzymes have been observed in humans [15].Type 2 5ARI is observed primarily in the prostate and is inhibited by finasteride, which reduces the serum level of DHT by approximately 70% [16]. Previous studies have shown that the long-term administration of finasteride is not associated with bone mineral density, lipoprotein concentrations, or overall health [17-18]. Finasteride has been used successfully in many men for the treatment of BPH [19] and male pattern baldness [20].Dutasteride inhibits Type 1 5 alpha-reductase (located in the skin, gut, liver, and other tissues) and Type 2 5 alpha-reductase, causing a 95% decrease in serum DHT levels [21].Dutasteride is an inhibitor of both 5-alpha reductase enzymes and may be more potent than finasteride [22]. It is less clear whether the greater DHT suppression resulting from inhibition of both isozymes of 5-alpha-reductase by dutasteride has important effects on other androgen
responsive tissues such as bone. Because low serum concentrations of androgens are associated with an increased risk of osteoporosis and fracture, therapy that decreases DHT has the potential to decrease BMD and increase fracture risk [23]. In men with
BPH, finasteride or dutasteride administration causes a marked decrease in DHT production, which leads to a 25% reduction in prostate volume, an improvement of the symptoms associated with BPH, and a significant reduction in the risk of acute urinary retention and the need for surgical intervention [24-26].It is unclear whether the greater DHT suppression resulting from the inhibition of both 5 alpha-reductase isozymes with dutasteride affects additional androgen responsive tissues, such as bones, lipoprotein metabolism, hemoglobin, prostate specific antigen (PSA), and sexual functions. Therapies that reduce DHT have the potential to reduce bone mineral density and increase fracture risk because low serum concentrations of androgens are associated with an increased risk of osteoporosis and fractures [27]. Amory et al indicated that the profound suppression of circulating serum DHT induced with finasteride and dutasteride in 1 year does not adversely affect bones, serum lipoproteins, or hemoglobin [28].Circulating DHT does not appear to play a clinically significant role in modulating bone mass, hematopoiesis, or lipid
metabolism in healthy men. A case-control study found no positive association between use of finasteride and hip fracture, and actually found some evidence of lower risk of fracture with finasteride use [29].
However, we demonstrated a 1.54-fold significant increase of osteoporosis diagnosis in patients with BPH using finasteride (95% CI, 1.02-2.32). Furthermore,
the results of the medication dosage analysis are shown in Table 3. We observed that higher doses of finasteride are associated with an increased risk of osteoporosis diagnosis (OR = 1.68; 95% CI, 1.01-2.81) relative to the patients not using 5ARIs. The combined use of alpha blockers and 5ARI is more effective in treating BPH [30].
The strengths of this study include its use of population-based data and the use of records from the NHIRD, rather than from self-reported drug use. In addition, Taiwan launched a national health insurance (NHI) in 1995, operated by a single-buyer, the government. All insurance claims should be scrutinized by medical reimbursement specialists and peer review. The diagnoses of osteoporosis and BPH were based on the ICD-9 code determined by qualified clinical physicians under strict audit in the reimbursement process. Therefore the diagnoses and codes for osteoporosis and BPH should be accurate and reliable. However, certain limitations should be mentioned. First, critical data are not included in the NHIRD, such as detailed demographic information, including dietary factors, smoking habits, alcohol consumption, body mass index, socioeconomic status, and family history of systemic diseases. These are major risk factors for osteoporosis diagnosis and may be indirectly associated with 5ARI use. However, because the NHIRD covers a highly representative sample of the general population in Taiwan and the reimbursement policy is universal, it is unlikely that these factors affected the prescription of 5ARIs. Second, the evidence derived
from a nested case-control study typically has a lower quality than that from
randomized trials because a nested case-control study design is subject to numerous biases related to the adjustments for confounding variables. Despite our meticulous study design, which featured adequate control of confounding factors, a critical limitation is that bias can remain if unmeasured or unknown confounders are present. Third, the diagnoses recorded in NHI claims primarily serve the purpose of
administrative billing and do not undergo verification for scientific purposes. We were unable to contact patients directly to inquire as to their use of 5ARIs because the anonymity of all beneficiaries listed in the NHIRD is assured. Furthermore, our analysis was unable to consider prescriptions for 5ARIs issued before 1996. This omission could have caused an underestimation of the cumulative dosage and may have weakened the observed association. However, the data for the prescription of the 5ARIs and the BPH diagnoses were reliable.
CONCLUSION
This population-based nested case-control study suggests that the use of finasteride can increase osteoporosis diagnosis risk among patients with BPH. The effects were more prominent in patients using higher doses of finasteride.
References
1. http://www.uptodate.com/contents/finasteride-drug-information? topicKey=DRUG_GEN
%2F8672&elapsedTimeMs=0&source=search_result&searchTerm=5-al %E2%80%A6.
2. Brian K Alldredge; Koda-Kimble, Mary Anne; Young, Lloyd Y.; Wayne A Kradjan; B. Joseph Guglielmo (2009). Applied therapeutics: the clinical use of drugs. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. pp.101–3.
3. Product Information: PROSCAR(R) oral tablets, finasteride oral tablets. Merck Sharp & Dohme Corp, Whitehouse Station, NJ, 2010.
4. Haan J, Hollander JM, van Duinen SG, Saxena PR, Wintzen AR (1997) Reversible severe myopathy during treatment with finasteride. Muscle Nerve. 20:502-4.
5. Basaria S, Coviello AD, Travison TG, Storer TW, Farwell WR, Jette AM, Eder R, Tennstedt S, Ulloor J, Zhang A, Choong K, Lakshman KM, Mazer NA, Miciek R, Krasnoff J, Elmi A, Knapp PE, Brooks B, Appleman E, Aggarwal S, Bhasin G, Hede-Brierley L, Bhatia A, Collins L, LeBrasseur N, Fiore LD, Bhasin S (2010) Adverse events associated with testosterone administration. N Engl J Med.
6. Pritchard CC, Nelson PS (2008) Gene expression profiling in the developing prostate. Differentiation 76: 624-40.
7. Nelson PS, Clegg N, Arnold H, Ferguson C, Bonham M, White J, Hood L, Lin B (2002) The program of androgen-responsive genes in neoplastic prostate
epithelium. Proc Natl Acad Sci U S A 99:11890-5.
8. Meikle AW, Stringham JD, Wilson DE, Dolman LI (1979) Plasma 5-reduced androgens in men and hirsute women: role of adrenals and gonads. J Clin Endocrinol Metab 48:969-75.
9. Nickel JC (2004) Comparison of clinical trials with finasteride and dutasteride. Rev Urol 6:S31-S39.
10. Tuck SP, Francis RM (2009) Testosterone, bone and osteoporosis. Front Horm Res. 37:123-32.
11. Francis RM (1999) The effects of testosterone on osteoporosis in men. Clin Endocrinol (Oxf). 50(4):411-4.
12. Cheng TM (2009) Taiwan’s National Health Insurance system: high value for the dollar. In Okma, K.G.H. and Crivelli, L. ed. Six Countries, Six Reform Models: The Health Reform Experience of Israel, the Netherlands, New Zealand, Singapore, Switzerland and Taiwan. New Jersey: World Scientific, pp.71-204. 13. Ito T, Horton R (1971) The source of plasma dihydrotestosterone in man. J Clin
14. Russell DW, Wilson JD (1994) Steroid 5 alpha-reductase: two genes/two enzymes. Annu Rev Biochem 63:25-61.
15. Thigpen AE, Silver RI, Guileyardo JM, Casey ML, McConnell JD, Russell DW (1993) Tissue distribution and ontogeny of steroid 5-alpha reductase isozymes expression. J Clin Invest 92:903-10.
16. Rittmaster RS, Lemay A, Zwicker H, Capizzi TP, Winch S, Moore E, Gormley GJ (1992) Effect of finasteride, a 5 alpha-reductase inhibitor, on serum
gonadotropins in normal men. J Clin Endocrinol Metab 75:484-8.
17. Gormley GJ, Stoner E, Bruskewitz RC, Imperato-McGinley J, Walsh PC, McConnell JD, Andriole GL, Geller J, Bracken BR, Tenover JS, E. Darracott Vaughan, Frances Pappas, Alice Taylor, Bruce Binkowitz, Jennifer Ng and the Finasteride Study Group (1992) The effect of finasteride in men with benign prostatic hyperplasia. The Finasteride Study Group. N Engl J Med 327:1185-91. 18. Matsumoto AM, Tenover L, McClung M, Mobley D, Geller J, Sullivan M,
Grayhack J, Wessells H, Kadmon D, Flanagan M, Zhang GK, Schmidt J, Taylor AM, Lee M, Waldstreicher J; Pless Study Group (2002) The long-term effect of specific type II 5alpha-reductase inhibition with finasteride on bone mineral density in men: results of a 4-year placebo controlled trial. J Urol 167:2105-8. 19. Wilton L, Pearce G, Edet E, Freemantle S, Stephens MD, Mann RD (1996) The
interventionalobservational cohort study in 14,772 patients. Br J Urol 78:379-84. 20. Price VH, Menefee E, Sanchez M, Kaufman KD (2006) Changes in hair weight
in men with androgenetic alopecia after treatment with finasteride (1 mg daily): threeand 4-year results. J Am Acad Dermatol 55:71-4.
21. Clark RV, Hermann DJ, Cunningham GR, Wilson TH, Morrill BB, Hobbs S (2004) Marked suppression of dihydrotestosterone in men with benign prostatic hyperplasia by dutasteride, a dual 5alpha-reductase inhibitor. J Clin Endocrinol Metab 89:2179-84.
22. Wu XJ, Zhi Y, Zheng J, et al. (2014) Dutasteride on benign prostatic hyperplasia: a meta-analysis on randomized clinical trials in 6460 patients. Urology 83:539.
23. Jackson JA, Riggs MW, Spiekerman AM (1992) Testosterone deficiency as a risk factor for hip fractures in men: a case-control study. Am J Med Sci 304:4. 24. McConnell JD, Bruskewitz R, Walsh P, Andriole G, Lieber M, Holtgrewe HL,
Albertsen P, Roehrborn CG, Nickel JC, Wang DZ, Taylor AM, Waldstreicher J (1998) The effect of finasteride on the risk of acute urinary retention and the need for surgical treatment among men with benign prostatic hyperplasia. Finasteride Long-Term Efficacy and Safety Study Group. N Engl J Med 338:557-63.
MC, Malek GH, Gottesman JE, Suryawanshi S, Drisko J, Meehan A,
Waldstreicher J; Proscar Long-Term Efficacy and Safety Study Group (2004) Sustained decrease in incidence of acute urinary retention and surgery with finasteride for 6 years in men with benign prostatic hyperplasia. J Urol 171:1194-8.
26. Debruyne F, Barkin J, van Erps P, Reis M, Tammela TL, Roehrborn C;
ARIA3001, ARIA3002 and ARIB3003 Study Investigators (2004) Efficacy and safety of longterm treatment with the dual 5 alpha-reductase inhibitor dutasteride in men with symptomatic benign prostatic hyperplasia. Eur Urol 46:488-94. 27. Jackson JA, Riggs MW, Spiekerman AM (1992) Testosterone deficiency as a
risk factor for hip fractures in men: a case-control study. Am J Med Sci 304:4-8. 28. Amory JK, Anawalt BD, Matsumoto AM, Page ST, Bremner WJ, Wang C,
Swerdloff RS, Clark RV (2008) The effect of 5alpha-reductase inhibition with dutasteride and finasteride on bone mineral density, serum lipoproteins,
hemoglobin, prostate specific antigen and sexual function in healthy young men. J Urol. 179:2333-8.
29. Jacobsen SJ, Cheetham TC, Haque R, et al. (2008) Association between 5-alpha reductase inhibition and risk of hip fracture. JAMA 300:1660.
Foley JP, Foster HE, Jacobs SC, Kaplan SA, Kreder KJ, Lieber MM, Lucia MS, Miller GJ, Menon M, Milam DF, Ramsdell JW, Schenkman NS, Slawin KM, Smith JA; Medical Therapy of Prostatic Symptoms (MTOPS) Research Group. For the MTOPS Research Group (2003) The long term effect of doxazosin, finasteride and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 349:2385-239.
Figure Legend:
Table 1. Distribution of demographics and medication between comparison group and osteoporosis group
Comparison group N=5,387 Osteoporosis group N=1,352 n % n % p-value Age, year <64 931 17.3 233 17.2 0.79 65-74 1661 30.8 416 30.8 75-84 2289 42.5 564 41.7 ≥ 85 506 9.39 139 10.3 Mean±SD§ 73.8±9.55 74.0±9.63 0.47 Occupation Publica 548 10.2 126 9.32 0.08 Labor 2180 40.5 568 42.0 Business 1239 23.0 269 19.9 Low incomeb 37 0.69 10 0.74 Others 1383 25.7 379 28.0 Urbanizationc 1 1436 26.7 312 23.1 0.01 2 1453 27.0 366 27.1 3 918 17.0 233 17.2 4 885 16.4 226 16.7 5 695 12.9 215 15.9 Medication Dutasteride 57 1.06 16 1.18 0.69 Finasteride 91 1.69 33 2.44 0.07 Comorbidity Hypertension 3861 71.7 980 72.5 <0.0001 Diabetes Mellitus 1245 23.1 324 24.0 <0.0001 Hyperlipidemia 1899 35.3 500 37.0 <0.0001 COPD 3129 58.1 878 64.9 <0.0001 Obesity 62 1.15 17 1.26 0.75
Lower urinary tract strictures 88 1.63 1 7 17 1.26 0.32 Treatment Testosterone 113 2.10 29 2.14 0.91 Ureteral catheterization 104 1.93 36 2.66 0.09
Chi-square test; §t- test
a Government, education, and military.
b Insured income is lower than the level required for charging premium.
Table 2. Adjusted odds and 95% confidence interval of osteoporosis among medication
Osteoporosis group
Medication N event OR& (95% CI)
None 6,558 1,305 1 (reference)
Dutasteride 65 15 1.21 (0.68-2.17)
Finasteride 116 32 1.54 (1.02-2.33)*
&Adjusted for age, occupation, urbanization, hypertension, diabetes, hyperlipidemia, COPD, obesity, lower urinary tract strictures, testosterone, and ureteral catheterization
Table 3. Adjusted odds and 95% confidence interval of osteoporosis in BPH patients among medication dosage
Osteoporosis
Dosage† N Case OR& (95% CI)
Dutasteride None 6666 1336 1.00 (reference) Low 37 10 1.49 (0.71-3.09) High 28 5 0.89 (0.34-2.35) Finasteride None 6615 1319 1.00 (reference) Low 45 11 1.32 (0.66-2.61) High 71 21 1.70 (1.01-2.84)*
†Average dosage (mg/per day) median: Avodart: low: < 0.02 mg; high: ≥ 0.02 mg; Finasteride: low: < 0.1 mg; high: ≥ 0.1 mg
& Adjusted for age, occupation, urbanization, hypertension, diabetes, hyperlipidemia, COPD, obesity, lower urinary tract strictures, testosterone, and ureteral catheterization