Fax +41 61 306 12 34 E-Mail [email protected] www.karger.com
Original Paper
Nephron Clin Pract 2008;109:c109–c118 DOI: 10.1159/000145453
Outcomes of Stage 3–5 Chronic Kidney
Disease before End-Stage Renal Disease
at a Single Center in Taiwan
Yen-Ling Chiu
a
Kuo-Liong Chien
b
Shuei-Liong Lin
b
Yung-Ming Chen
b
Tun-Jun Tsai
b
Kwan-Dun Wu
b
a Department of Internal Medicine, Far-Eastern Memorial Hospital, and b Department of Internal Medicine, National Taiwan University Hospital, College of Medicine, National Taiwan University, Taipei , Taiwan
die. Conclusion: In this CKD cohort, patients were more like-ly to develop ESRD than cardiovascular death. The rate of GFR decline and predictors of ESRD were comparable to those reported in Western countries. Thus, the high inci-dence of ESRD in Taiwan may be attributed, at least in part, to lower cardiovascular mortality.
Copyright © 2008 S. Karger AG, Basel
Introduction
Chronic kidney diseases (CKD) frequently advances to end-stage renal disease (ESRD), and the number of pa-tients affected is steadily increasing worldwide. Taiwan has the highest incidence of treated ESRD in the world [1] , despite stringently regulated initiation of renal re-placement therapy (RRT) according to local practice guidelines. In the past decade, many important studies identified therapeutic strategies to retard the progression and reduce the mortality of CKD patients, including stringent control of blood pressure and hyperglycemia, use of renin-angiotensin system blockers and reduction of proteinuria [2–6] . These treatments could impact the progression and outcomes of CKD patients greatly, but regretfully angiotensin-converting enzyme inhibitors and angiotensin receptor blockers are frequently
Key Words
Cardiovascular disease ⴢ Chronic kidney disease progression ⴢ End-stage renal disease
Abstract
Background: Taiwan has the highest incidence of end-stage renal disease (ESRD) in the world, but little is known about the outcomes of patients with chronic kidney disease (CKD) before ESRD in Taiwan. This study investigated the rate of renal progression and predictors for ESRD and death in a prospective cohort of patients under usual nephrologic care at a single center. Methods: A total of 433 patients at CKD stage 3–5 short of dialysis were recruited from nephrology clinics. Patients were monitored for up to 36 months or until ESRD, death or loss to follow-up. Glomerular filtration rates (GFR) were calculated by the Modification of Diet in Renal Disease abbreviated formula. Results: At baseline, mean age was 65.6 years, 61.7% were male, 33.3% were diabetic and 29.1% had cardiovascular diseases (CVD). At the end of fol-low-up, 123 patients (28.4%) had advanced to ESRD and 41 (9.5%) had died. Mean annual declines in GFR were 2.24, 4.22, and 3.23 ml/min/1.73 m 2 for stages 3, 4, and 5, respectively. By Cox regression model, patients with CVD, lower BMI and higher systolic BP were more likely to develop ESRD. Older patients with CVD and lower systolic BP were more likely to
Received: October 25, 2007 Accepted: April 1, 2008 Published online: July 25, 2008
Yung-Ming Chen, MD
Department of Internal Medicine, National Taiwan University Hospital College of Medicine, National Taiwan University, No. 7 Chung-Shan South Road Taipei 100 (Taiwan)
Tel. +886 2 2312 3456, ext. 5993, Fax +886 2 2322 2955, E-Mail [email protected] © 2008 S. Karger AG, Basel
1660–2110/08/1093–0109$24.50/0 Accessible online at:
utilized [7] and blood pressure is not optimally controlled [8] . On the other hand, while it had also been suggested that renal failure patients should be referred to nephrolo-gists early [9] , no contemporary study has been conduct-ed to study the progression and clinical outcomes of renal failure patients under routine care provided by nephrolo-gists.
Besides, the reasons for Taiwan’s ESRD endemic re-main largely unknown. Recent epidemiological data es-timate the prevalence of stage 3–5 CKD to be around 6.4%, representing 1.5 million individuals [10] . This fig-ure is not so different from that of industrialized coun-tries with a similarly high incidence of ESRD, such as Japan (6.7%) [11] and the United States (4.6%) [12] but is appreciably lower than that of Australia (11.2%) where ESRD incidence and prevalence are one-half that of Tai-wan [13] . Hence, TaiTai-wan’s high incidence of ESRD cannot be explained by the size of the CKD pool. One recent study shows similar CKD prevalence rates in the United States and Norway, but the relative risk for progression from CKD stage 3 or 4 to ESRD in US white patients was 2.5 times that of Norwegian patients [14] . Given similar rates of cardiovascular death in the two countries, it was suggested that a slower rate of CKD progression in Nor-way have contributed to its lower incidence of ESRD. However, the progression rate and mortality of Taiwan-ese pre-ESRD CKD patients have never been reported. This study was thus initiated to investigate the rate and predictors of renal progression and pre-ESRD mortality in a Taiwanese CKD cohort under nephrologists’ care.
Methods
Subjects and CKD Stratification
National Taiwan University Hospital is a major medical center located in northern Taiwan that serves as a referral center for more than 2 million residents of metropolitan Taipei area. From September 2003 to March 2004, we consecutively screened per-sons with stage 3–5 CKD short of ESRD from the nephrologic outpatient clinic. Taiwanese adults 1 20 years old with stable renal function for at least 3 months and not expecting to start dialysis or undergo renal transplantation within 6 months were included. Patients with active infection or decompensated liver cirrhosis at the time of screening were excluded. A total of 433 patients were enrolled and received regular clinic follow-up. GFR was estimated according to the Modification of Diet in Renal Disease (MDRD) abbreviated formula: 186 ! Scr –1.154 ! age –0.203 ! 0.742 (if fe-male) ! 1.212 if African-American. Because no participant was of African descent, the last factor was ignored. CKD stage was determined as described by the National Kidney Foundation of the United States. At the time of entry, GFRs of 30–59, 29–15 and ! 15 ml/min/1.73 m 2 for more than 3 months were classified as
CKD stages 3, 4 and 5, respectively. The study protocol was ap-proved by the Research and Ethics Committee of the Hospital (No. 9461701018).
Baseline Data
Diabetes was documented by the presence of elevated fasting blood sugar levels or hypoglycemic therapy. Glomerulonephritis, hypertensive nephrosclerosis, or polycystic kidney disease were diagnosed based on clinically relevant medical history or exami-nations. CVD included five categories: (1) sudden death, (2) coro-nary heart disease, (3) congestive heart failure, (4) cerebrovascu-lar infarcts or hemorrhage, and (5) peripheral arterial disease. Coronary heart disease was diagnosed by a cardiologist according to a prior history of myocardial infarction, positive cardiac thal-lium scan or coronary angiography. All laboratory measurements were carried out by the Department of Laboratory Medicine, Na-tional Taiwan University Hospital. The body mass index (BMI) was measured by calculating the individual’s weight divided by the square of the height and expressed as kg/m 2 . Dipstick urinal-ysis was performed with spontaneously voided fresh urine and the result interpreted as (–), (8), (1+), (2+), and (3+). We defined (–) as no proteinuria, (8) to (2+) as mild proteinuria, and (3+) as heavy proteinuria.
Outcome Data
The observation period of each patient was defined to start immediately after the registered measurement of serum creati-nine satisfying the above criteria (designated as the index date) and lasted for 36 months or until ESRD, death or loss to follow-up. ESRD was defined as initiation of RRT, i.e. chronic dialysis or re-nal transplantation. The timing to initiate RRT follows the regu-lations by the Bureau of National Health Insurance, including creatinine clearance ! 15 ml/min or serum Cr 1 6 mg/dl, plus any of the following conditions: (1) blood urea nitrogen 1 100 mg/dl, (2) refractory heart failure, lung edema, metabolic acidosis, or hyperkalemia, (3) pericarditis, (4) bleeding tendency, (5) uremic encephalopathy or neuropathy, and (6) uncontrolled nausea, vomiting, or cachexia. Patients lost to regular clinic follow-up or transferred to other health care facilities were contacted by tele-phone to monitor and record their renal function.
Statistical Analyses
Continuous variables are presented as mean 8 SD. Compari-son of continuous variables between stages of CKD were per-formed using one-way ANOVA. Categorical and nominal data were compared using the 2 test. To calculate the rate of GFR de-cline, the first and latest available serum creatinine data were used. To study CKD stage transition, event rates were calculated using the cumulative rate approach, and the result expressed as the cumulative rates over 36 months. The starting time for sur-vival analysis was the index date of each patient. Differences in baseline demographic data, underlying diseases and laboratory data were calculated by ANOVA for continuous data and by the 2 test for nominal data. The difference in morbidity rate of di-alysis or mortality rate between stages 3, 4 and 5 were tested by the Poisson regression model. The univariate and multivariate association of presumed risk factors with RRT or death was per-formed by Cox proportional hazards model. All analyses were performed with SPSS, version 13.0 (SPSS Inc., Chicago, Ill., USA). p ! 0.05 was considered significant.
Mortality and CKD Progression in Taiwan
Nephron Clin Pract 2008;109:c109–c118 c111
Results
Baseline Demographic Characteristics
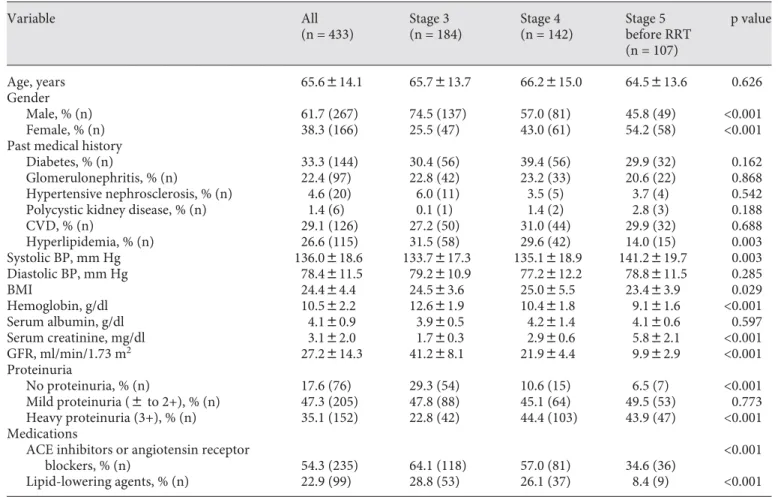
A total of 433 patients with a mean age of 65 years were enrolled. Their baseline demographic characteristics are summarized in table 1 . At the start of the study, 184 (42.5%) patients were at stage 3, 142 (32.8%) at stage 4, and 107 (24.7%) at stage 5 short of RRT. Most were male (267, or 61.7%) and 144 (33.3%) were diabetic. More male pa-tients were at stage 3 CKD, but percentages became more balanced at later stages. The most common primary etiol-ogy of CKD at all stages was likely related to diabetes, followed by glomerulonephritis, hypertensive nephro-sclerosis, and polycystic kidney disease. In 3.9% of pa-tients, the primary etiology of CKD was not clear, but
presumably could be ascribed to chronic tubulointersti-tial disease. The prevalence of CVD was similar across all three CKD stages. Patients with stage 3 CKD had signif-icantly lower systolic blood pressure (BP), higher hemo-globin, less severe proteinuria, higher BMI, and more fre-quently used angiotensconverting enzyme (ACE) in-hibitors, angiotensin receptor blockers and lipid-lowering drugs, when compared to patients at stage 4 or 5. As CKD progressed, BMI gradually decreased but serum albumin levels remained the same.
Patient Outcomes
Nearly all, or 411 (94.9%) patients completed the 3-year follow-up or were followed until they reached ESRD or death. Only 22 (5.1%) patients were lost to follow-up.
Table 1. Baseline characteristics of patients by CKD staging
Variable All (n = 433) Stage 3 (n = 184) Stage 4 (n = 142) Stage 5 before RRT (n = 107) p value Age, years 65.6814.1 65.7813.7 66.2815.0 64.5813.6 0.626 Gender Male, % (n) 61.7 (267) 74.5 (137) 57.0 (81) 45.8 (49) <0.001 Female, % (n) 38.3 (166) 25.5 (47) 43.0 (61) 54.2 (58) <0.001
Past medical history
Diabetes, % (n) 33.3 (144) 30.4 (56) 39.4 (56) 29.9 (32) 0.162
Glomerulonephritis, % (n) 22.4 (97) 22.8 (42) 23.2 (33) 20.6 (22) 0.868
Hypertensive nephrosclerosis, % (n) 4.6 (20) 6.0 (11) 3.5 (5) 3.7 (4) 0.542
Polycystic kidney disease, % (n) 1.4 (6) 0.1 (1) 1.4 (2) 2.8 (3) 0.188
CVD, % (n) 29.1 (126) 27.2 (50) 31.0 (44) 29.9 (32) 0.688 Hyperlipidemia, % (n) 26.6 (115) 31.5 (58) 29.6 (42) 14.0 (15) 0.003 Systolic BP, mm Hg 136.0818.6 133.7817.3 135.1818.9 141.2819.7 0.003 Diastolic BP, mm Hg 78.4811.5 79.2810.9 77.2812.2 78.8811.5 0.285 BMI 24.484.4 24.583.6 25.085.5 23.483.9 0.029 Hemoglobin, g/dl 10.582.2 12.681.9 10.481.8 9.181.6 <0.001 Serum albumin, g/dl 4.180.9 3.980.5 4.281.4 4.180.6 0.597 Serum creatinine, mg/dl 3.182.0 1.780.3 2.980.6 5.882.1 <0.001 GFR, ml/min/1.73 m2 27.2814.3 41.288.1 21.984.4 9.982.9 <0.001 Proteinuria No proteinuria, % (n) 17.6 (76) 29.3 (54) 10.6 (15) 6.5 (7) <0.001 Mild proteinuria (8 to 2+), % (n) 47.3 (205) 47.8 (88) 45.1 (64) 49.5 (53) 0.773 Heavy proteinuria (3+), % (n) 35.1 (152) 22.8 (42) 44.4 (103) 43.9 (47) <0.001 Medications
ACE inhibitors or angiotensin receptor
blockers, % (n) 54.3 (235) 64.1 (118) 57.0 (81) 34.6 (36)
<0.001
Lipid-lowering agents, % (n) 22.9 (99) 28.8 (53) 26.1 (37) 8.4 (9) <0.001
Values shown as mean 8 SD. For comparison between 3 patient groups, p values were calculated by ANOVA for continuous data and by Pearson 2 test for nominal data.
CVD = Presence of cardiovascular disease at baseline, including coronary artery disease, peripheral artery disease, cerebrovascu-lar disease and congestive heart failure; BP = blood pressure; GFR = glomerucerebrovascu-lar filtration rate; ACE = angiotensin-converting en-zyme.
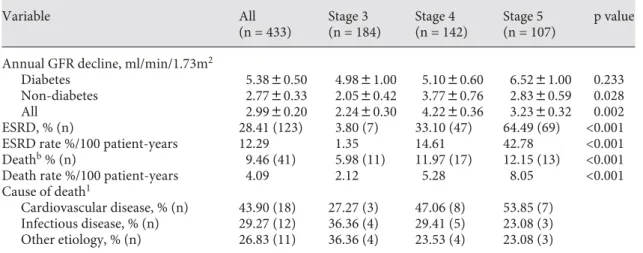
The median period of observation was 27.8 months. Ta-ble 2 summarizes the progression rates and clinical out-comes for patients by CKD stage. The mean annual de-clines in glomerular filtration rates (GFR) were 2.24, 4.22, and 3.23 ml/min/1.73 m 2 for stages 3, 4 and 5, respective-ly. By ANOVA analyses, the annual decline in GFR was significantly greater for patients in stage 4 or 5 compared to those in stage 3 (p = 0.002). This trend was statistically significant in non-diabetic but not in diabetic patients. At the end of the study, 123 patients (28.4%) had started RRT (102, hemodialysis; 19, peritoneal dialysis; 2, renal trans-plantation), and 41 patients had died (9.5%). Compared to patients in stage 3 CKD, patients in stage 4 or 5 were more susceptible to death from any cause, although the differ-ence did not reach statistical significance. The major cause of death was CVD (n = 18), which included sudden death (n = 4), acute coronary syndromes (n = 9), heart failure (n = 4), and cerebrovascular events (n = 1).
Three-year cumulative outcomes grouped by baseline stages of CKD are depicted in figure 1 . The risk for CKD stages 3, 4 and 5 to reach ESRD was 3.8, 33.1 and 64.5%, and to die from any cause, 6.0, 12.0 and 12.1%, respec-tively. Patients with stage 3 CKD had a slightly higher risk of dying than of developing ESRD. Conversely, patients with stage 4 or 5 CKD were appreciably more likely to develop ESRD than to die. A significant portion of pa-tients remained alive and dialysis free (90.2%, stage 3;
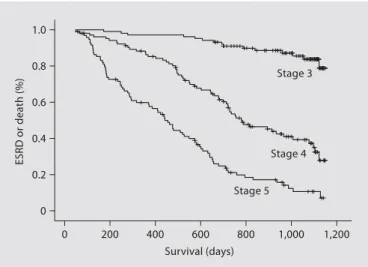
54.9%, stage 4; 22.8%, stage 5). The Kaplan-Meier curves for the combined end point of ESRD and death in patients with different stages of CKD are depicted in figure 2 .
Predictors for RRT
Univariate logistic regression shows that diabetes (OR, 1.92; 95% CI, 1.35–2.74), higher systolic BP (per 5 mm Hg; OR, 1.12; 95% CI, 1.07–1.16), mild proteinuria (OR, 4.03; 95% CI, 1.44–11.28), and heavy proteinuria (OR, 14.25; 95% CI, 5.22–38.92) were associated with a higher risk of ESRD ( table 3 ). Higher baseline GFR (OR, 0.88; 95% CI, 0.86–0.90), higher hemoglobin level (OR, 0.753; 95% CI, 0.67–0.85) and use of angiotensin II blockers (OR, 0.50; 95% CI, 0.35–0.71) were associated with a lower risk for ESRD. Compared to those with BMI less than 20, higher BMI levels were associated with lower risk of ESRD (BMI 20.01–24.99, OR, 0.56; 95% CI, 0.34–0.94; BMI 25.00– 29.99, OR, 0.53; 95% CI, 0.30–0.91; BMI 30, OR, 0.41; 95% CI, 0.17–0.96).
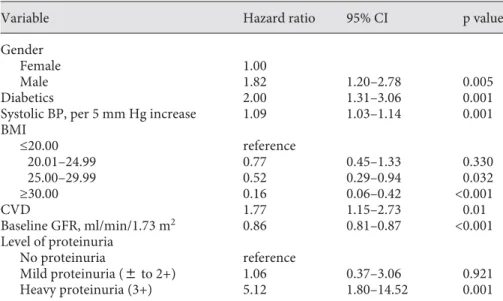
By age-adjusted multivariate Cox survival analysis, being male (OR, 1.82; 95% CI, 1.20–2.78), having diabetes (OR, 2.00; 95% CI, 1.31–3.06), presence of CVD at base-line (OR, 1.77; 95% CI, 1.15–2.73), higher systolic BP (per 5 mmHg; OR, 1.09; 95% CI, 1.03–1.14), lower baseline GFR (OR, 0.86; 95% CI, 0.81–0.87), and heavy proteinuria (OR, 5.12; 95% CI, 1.80–14.52) were independent predic-tors for ESRD ( table 4 ). Compared to BMI ! 20, BMI
Table 2. Clinical outcomes of patients by baseline CKD stages
Variable All (n = 433) Stage 3 (n = 184) Stage 4 (n = 142) Stage 5 (n = 107) p value
Annual GFR decline, ml/min/1.73m2
Diabetes 5.3880.50 4.9881.00 5.1080.60 6.5281.00 0.233
Non-diabetes 2.7780.33 2.0580.42 3.7780.76 2.8380.59 0.028
All 2.9980.20 2.2480.30 4.2280.36 3.2380.32 0.002
ESRD, % (n) 28.41 (123) 3.80 (7) 33.10 (47) 64.49 (69) <0.001
ESRD rate %/100 patient-years 12.29 1.35 14.61 42.78 <0.001
Deathb % (n) 9.46 (41) 5.98 (11) 11.97 (17) 12.15 (13) <0.001
Death rate %/100 patient-years 4.09 2.12 5.28 8.05 <0.001
Cause of death1
Cardiovascular disease, % (n) 43.90 (18) 27.27 (3) 47.06 (8) 53.85 (7)
Infectious disease, % (n) 29.27 (12) 36.36 (4) 29.41 (5) 23.08 (3)
Other etiology, % (n) 26.83 (11) 36.36 (4) 23.53 (4) 23.08 (3)
GFR = Glomerular filtration rate. Values shown as mean 8 SE. For comparison between three patient groups, p values were calculated by ANOVA for continuous data and by Pearson 2 test for nominal data.
ESRD = End-stage renal disease: including outcomes of patients transferred to other hospital facilities. 1 Data expressed as percent of cases of death within each group.
Mortality and CKD Progression in Taiwan
Nephron Clin Pract 2008;109:c109–c118 c113
25.00–29.99 (OR, 0.52; 95% CI, 0.29–0.94) and BMI 1 30 (OR, 0.16; 95% CI, 0.06–0.42) were independent protec-tors from ESRD.
Predictors for Mortality
Being older (OR, 1.10; 95% CI, 1.06–1.13), presence of CVD at baseline (OR, 3.44; 95% CI, 1.86–6.38), lower sys-tolic BP (OR, 0.92; 95% CI, 0.85–0.92), lower diassys-tolic BP (OR, 0.77; 95% CI, 0.67–0.90), lower serum hemoglobin level (OR, 0.81; 95% CI, 0.68–0.96), lower serum albumin level (OR, 0.42; 95% CI, 0.20–0.87) and lower baseline GFR level (OR, 0.96; 95% CI, 0.93–0.98) were associated with all-cause mortality. Compared with BMI less than 20, BMI 20.01–24.99 (OR, 0.31; 95% CI, 0.13–0.73) and BMI 25.00–29.99 (OR, 0.39; 95% CI, 0.16–0.95) were as-sociated with less mortality risk ( table 5 ).
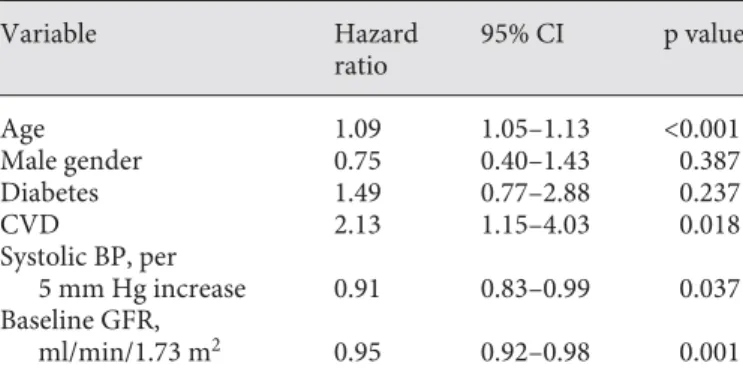
In multivariate Cox survival analysis, being older (OR, 1.09; 95% CI, 1.05–1.13), baseline presence of CVD (OR, 2.13; 95% CI, 1.15–4.03), lower baseline GFR (OR, 0.95; 95% CI, 0.83–0.99), and lower systolic BP (per 5 mm Hg; OR, 0.91; 95% CI, 0.83–0.99) remained independent pre-dictors of mortality before the development of ESRD ( ta-ble 6 ).
Discussion
This study is the first to demonstrate renal progression and stage transition in a prospective cohort of moderate-to-severe CKD patients over a period of 3 years in Taiwan where ESRD is endemic. The annual GFR decline of 2.99 ml/min in this cohort was no faster than that reported in
major renal clinical trials (2–6 ml/min per year), which were conducted mostly in patients with milder CKD, i.e. stage 2–3 [3, 15–17] . A recent report by Hou et al. [18] shows an annual GFR decline of 3.2–5 ml/min in Chinese non-diabetic patients with stage 4 CKD, which is compa-rable to similar patients in our study (3.77 ml/min/year) ( table 2 ). At the end of study, a significant portion of pa-tients remained alive and dialysis free ( fig. 1 ).
Patients with CKD in Western countries frequently die of CVD before developing ESRD [19–21] . By contrast, this study shows that Taiwanese patients are more likely
0 10 20 30 40 50 60 70 80 90 100
Stage 3 Stage 4 Stage 5 RRT Death Stage 4 Stage 5 RRT Death Stage 5 RRT Death 12.2 65.0 22.8 12.0 33.1 16.9 38.0 6.0 3.8 3.8 23.9 62.5 % Baseline stage 3 (n = 184) Baseline stage 4 (n = 142) Baseline stage 5 (n = 107) Patients’ outcomes
Fig. 1. Three-year cumulative outcomes
grouped by baseline stages of CKD. Col-lectively, more patients develop ESRD than death from any cause, and the prob-ability of stage progression or death is higher in patients with more severe CKD.
1,200 1,000 800 600 400 200 0 1.0 0.8 0.6 0.4 0.2 0 ESRD or death (%) Stage 3 Stage 4 Stage 5 Survival (days)
Fig. 2. Kaplan-Meier curves showing the combined end point of
ESRD and death in patients with different stages of CKD (log-rank tests indicate p ! 0.001 between any 2 of the 3 groups).
Variable Hazard ratio 95% CI p value Gender
Female 1.00
Male 1.82 1.20–2.78 0.005
Diabetics 2.00 1.31–3.06 0.001
Systolic BP, per 5 mm Hg increase 1.09 1.03–1.14 0.001
BMI ≤20.00 reference 20.01–24.99 0.77 0.45–1.33 0.330 25.00–29.99 0.52 0.29–0.94 0.032 ≥30.00 0.16 0.06–0.42 <0.001 CVD 1.77 1.15–2.73 0.01 Baseline GFR, ml/min/1.73 m2 0.86 0.81–0.87 <0.001 Level of proteinuria No proteinuria reference Mild proteinuria (8 to 2+) 1.06 0.37–3.06 0.921 Heavy proteinuria (3+) 5.12 1.80–14.52 0.001
CVD = Presence of cardiovascular disease at baseline, including coronary artery dis-ease, peripheral artery disdis-ease, cerebrovascular disease and congestive heart failure; BP = blood pressure; GFR = glomerular filtration rate.
Table 4. Age-adjusted multivariate
Cox proportional model for the effect of baseline variables on risk of ESRD
Variable Hazard ratio 95% CI p value Age 0.99 0.98–1.00 0.169 Male gender 0.86 0.98–1.24 0.423 Diabetics 1.92 1.35–2.74 <0.001 Glomerulonephritis 0.87 0.56–1.33 0.511 CVD 1.25 0.86–1.83 0.247 Hyperlipidemia 0.61 0.39–0.95 0.027
Systolic BP, per 5 mm Hg increase 1.12 1.07–1.16 <0.001
Diastolic BP, per 5 mm Hg increase 1.06 0.97–1.16 0.255
BMI ≤20.00 reference 20.01–24.99 0.56 0.34–0.94 0.028 25.00–29.99 0.53 0.30–0.91 0.023 ≥30.00 0.41 0.17–0.96 0.04 Hemoglobin, g/dl 0.75 0.67–0.83 <0.001 Serum albumin, g/dl 0.78 0.49–1.23 0.292 Baseline GFR, ml/min/1.73 m2 0.88 0.86–0.90 <0.001 Level of proteinuria No proteinuria reference Mild proteinuria (8 to 2+) 4.03 1.44–11.28 0.008 Heavy proteinuria (3+) 14.25 5.22–38.92 <0.001
ACE inhibitors or angiotensin receptor
blockers 0.45 0.35–0.71 <0.001
Lipid-lowering agents 0.59 0.37–0.95 0.028
CVD = Presence of cardiovascular disease at baseline, including coronary artery dis-ease, peripheral artery disdis-ease, cerebrovascular disease and congestive heart failure; BP = blood pressure; GFR = glomerular filtration rate; ACE = angiotensin-converting enzyme.
Table 3. Univariate analyses of baseline
Mortality and CKD Progression in Taiwan
Nephron Clin Pract 2008;109:c109–c118 c115
to develop ESRD than to die. Death rates from any cause were appreciably lower in this cohort than in those in in-dustrialized countries [20, 22] . Reasons for this differen-tial mortality are not clear but may be related to racial disparities. Indeed, the prevalence of coronary heart dis-ease or heart failure in association with CKD varies sub-stantially between racial populations [23] . Wong et al. [24] have reported a survival advantage of Asian can dialysis patients compared with Caucasian Ameri-cans. Further, based on United State Renal Data System (USRDS) data for 1995–2000, Young et al. [25] have shown that Asian and Hispanic American ESRD patients exhibit lower rates of myocardial infarction compared with Caucasians. Since progression of CKD toward ESRD is a continuous process, a cardiovascular survival advan-tage could explain the high incidence of ESRD in Taiwan. It is important to note that CVD remained the most com-mon cause of death in this cohort. Hence, strategies to prevent or reduce CV risk factors should be implemented in all patients with CKD irrespective of stage.
Variable Hazard ratio 95% CI p value Age 1.10 1.06–1.13 <0.001 Male gender 0.70 0.38–1.30 0.260 Diabetics 1.42 0.76–2.66 0.277 Glomerulonephritis 0.45 0.18–1.15 0.094 CVD 3.44 1.86–6.38 <0.001 Hyperlipidemia 0.68 0.33–1.43 0.314
Systolic BP, per 5 mm Hg increase 0.92 0.85–0.98 0.047
Diastolic BP, per 5 mm Hg increase 0.77 0.67–0.90 0.001
BMI ≤20.00 reference 20.01–24.99 0.31 0.13–0.73 0.007 25.00–29.99 0.39 0.16–0.95 0.038 ≥30.00 0.32 0.02–1.09 0.060 Hemoglobin, g/dl 0.81 0.68–0.96 0.016 Serum albumin, g/dl 0.42 0.20–0.87 0.02 Baseline GFR, ml/min/1.73 m2 0.96 0.93–0.98 0.001 Level of proteinuria No proteinuria reference Mild proteinuria (8 to 2+) 2.07 0.79–5.40 0.138 Heavy proteinuria (3+) 1.49 0.52–4.30 0.460
ACE inhibitors or angiotensin receptor blockers
0.49 0.26–0.92 0.491
Lipid-lowering agents 0.60 0.27–1.36 0.220
CVD = Presence of cardiovascular disease at baseline, including coronary artery dis-ease, peripheral artery disdis-ease, cerebrovascular disease and congestive heart failure; BP = blood pressure; GFR = glomerular filtration rate; ACE = angiotensin-converting enzyme.
Table 5. Univariate analyses of
baseline variables in association with risk of death
Table 6. Multivariate Cox proportional model for the effect of
baseline variables on risk of death
Variable Hazard ratio 95% CI p value Age 1.09 1.05–1.13 <0.001 Male gender 0.75 0.40–1.43 0.387 Diabetes 1.49 0.77–2.88 0.237 CVD 2.13 1.15–4.03 0.018 Systolic BP, per 5 mm Hg increase 0.91 0.83–0.99 0.037 Baseline GFR, ml/min/1.73 m2 0.95 0.92–0.98 0.001
CVD = Presence of cardiovascular disease at baseline, includ-ing coronary artery disease, peripheral artery disease, cerebro-vascular disease and congestive heart failure; BP = blood pres-sure; GFR = glomerular filtration rate.
Very few studies had investigated the role of CVD as an independent risk factor for CKD progression and ESRD development. In this cohort, presence of CVD at baseline is a strong predictor for ESRD, even after multi-variable adjustment for other established risk factors. This finding is reminiscent of that reported by Levin et al. [26] , which showed that presence of CVD at baseline increased the probability of progression to ESRD by 50% in a Canadian cohort of patients with stage 2–5 CKD short of dialysis. Interestingly, CVD has also been associ-ated with decline of renal function and development of kidney disease in a large community-based population with normal baseline renal function [27] .
Accumulating evidence indicates that higher BMI is a risk factor for CKD in apparently healthy persons [28, 29] , and graft loss in kidney transplantation recipients [30] . The result of a recent study from Taiwan [31] also supports this notion. By contrast, our study identifies lower BMI as an independent predictor for ESRD in pa-tients with stage 3–5 CKD. This seemingly paradoxical finding could be reminiscent of the ‘reverse epidemiolo-gy’ seen in the dialysis population where low BMI and the associated malnutrition were liable for an augmented hazard of death worse than for those with high BMI [32– 34] .
Our observation that systolic BP was a stronger pre-dictor for progression than diastolic BP is consistent with that reported in the AIPRD (ACE inhibition in Progres-sive Renal Disease) [15] and RENAAL (Reduction of End Points in NIDDM with the Angiotensin II Receptor An-tagonist Losartan) studies [5] . In addition, we found that lower systolic BP was closely associated with higher all-cause mortality, and similar observation had been re-ported by Kovesdy et al. [35] . It is assumed that lower systolic BP may reflect worsening cardiovascular func-tion or a consequence of increasing uremic burden dur-ing progression, such as autonomic neuropathy and dif-fuse calcification.
There are several limitations in this study. First, poten-tial selection bias exists since patients prone to the devel-opment of ESRD might be preferentially recruited given the high prevalence of proteinuria. However, proteinuria is also a risk factor for CVD [36] ; yet most patients in this cohort, unlike Western counterparts, develop ESRD rather than cardiovascular death. This suggests that oth-er factors such as racial disparities may play a more im-portant role in the differential evolution of ESRD and CVD. Secondly, there is a controversy about adjustment for racial coefficient while using the modified MDRD formula in Asian people. Ma et al. [37] have constructed
a modified MDRD formula for the Chinese. However, the formula was derived mainly from non-diabetic patients with very mild CKD, and its applicability to diabetic, ad-vanced CKD persons still awaits verification. Neverthe-less, when our data were calculated by using Ma’s formu-la, the trend of GFR decline among different stages of CKD remain the same (data not shown). Finally, since this was an observational study, the presence of con-founding factors such as nonrandomized use of erythro-poietin, ACE inhibitors, angiotensin receptor blockers or statins cannot be excluded. In spite of that, this study was designed to follow individual patient’s renal function un-der routine nephrologists’ care; thus, many of our find-ings could be valuable for physicians and health person-nel while taking care of CKD patients. Further multi-center prospective studies are needed to confirm the external validity of the findings accrued from this study.
In conclusion, this study shows the current status of CKD progression and stage transition in a single-center cohort under daily nephrologic care over a period of 3 years. It is not clear to what extent our cohort represents the general CKD population in Taiwan. The nationwide CKD education program endorsed by the Bureau of Health Promotion in Taiwan was launched in 2005, but longitudinal CKD registry data are not likely available for analysis before 2010. For now, suffice it to say that CKD patients in this cohort were more likely to develop ESRD than cardiovascular death. Because the rate of GFR decline and predictors of ESRD were comparable to those reported in Western countries, it is surmised that the high incidence of ESRD in Taiwan may be at-tributed, at least in part, to lower cardiovascular mortal-ity.
Acknowledgements
This work was supported by grants from the Ta-Tung Kidney Foundation, and the Mrs. Hsiu-Chin Lee Kidney Research Fund, Taipei, Taiwan.
Mortality and CKD Progression in Taiwan
Nephron Clin Pract 2008;109:c109–c118 c117
9 Martinez-Ramirez HR, Jalomo-Martinez B, Cortes-Sanabria L, Rojas-Campos E, Barra-gan G, Alfaro G, Cueto-Manzano AM: Renal function preservation in type 2 diabetes mel-litus patients with early nephropathy: a com-parative prospective cohort study between primary health care doctors and a nephrolo-gist. Am J Kidney Dis 2006; 47: 78–87. 10 Hsu CC, Hwang SJ, Wen CP, Chang HY,
Chen T, Shiu RS, Horng SS, Chang YK, Yang WC: High prevalence and low awareness of CKD in Taiwan: a study on the relationship between serum creatinine and awareness from a nationally representative survey. Am J Kidney Dis 2006; 48: 727–738.
11 Nakamura K, Okamura T, Hayakawa T, Kadowaki T, Kita Y, Ohnishi H, Saitoh S, Sakata K, Okayama A, Ueshima H: Chronic kidney disease is a risk factor for cardio-vascular death in a community-based popu-lation in Japan: Nippon data 90. Circ J 2006; 70: 954–959.
12 Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS: Prevalence of chronic kidney dis-ease and decrdis-eased kidney function in the adult us population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis 2003; 41: 1–12.
13 Chadban SJ, Briganti EM, Kerr PG, Dunstan DW, Welborn TA, Zimmet PZ, Atkins RC: Prevalence of kidney damage in Australian adults: The AUSDIAB kidney study. J Am Soc Nephrol 2003; 14:S131–S138.
14 Hallan SI, Coresh J, Astor BC, Asberg A, Powe NR, Romundstad S, Hallan HA, Lyder-sen S, Holmen J: International comparison of the relationship of chronic kidney disease prevalence and ESRD risk. J Am Soc Nephrol 2006; 17: 2275–2284.
15 Jafar TH, Stark PC, Schmid CH, Landa M, Maschio G, de Jong PE, de Zeeuw D, Sha-hinfar S, Toto R, Levey AS: Progression of chronic kidney disease: the role of blood pressure control, proteinuria, and angioten-sin-converting enzyme inhibition: a patient-level meta-analysis. Ann Intern Med 2003; 139: 244–252.
16 Agodoa LY, Appel L, Bakris GL, Beck G, Bourgoignie J, Briggs JP, Charleston J, Cheek D, Cleveland W, Douglas JG, Douglas M, Dowie D, Faulkner M, Gabriel A, Gassman J, Greene T, Hall Y, Hebert L, Hiremath L, Ja-merson K, Johnson CJ, Kopple J, Kusek J, Lash J, Lea J, Lewis JB, Lipkowitz M, Massry S, Middleton J, Miller ER, 3rd, Norris K, O’Connor D, Ojo A, Phillips RA, Pogue V, Rahman M, Randall OS, Rostand S, Schul-man G, Smith W, Thornley-Brown D, Tisher CC, Toto RD, Wright JT Jr, Xu S: Effect of ramipril vs. amlodipine on renal outcomes in hypertensive nephrosclerosis: a random-ized controlled trial. JAMA 2001; 285: 2719– 2728.
17 Chan JC, Ko GT, Leung DH, Cheung RC, Cheung MY, So WY, Swaminathan R, Nich-olls MG, Critchley JA, Cockram CS: Long-term effects of angiotensin-converting en-zyme inhibition and metabolic control in hypertensive type 2 diabetic patients. Kid-ney Int 2000; 57: 590–600.
18 Hou FF, Zhang X, Zhang GH, Xie D, Chen PY, Zhang WR, Jiang JP, Liang M, Wang GB, Liu ZR, Geng RW: Efficacy and safety of benazepril for advanced chronic renal insuf-ficiency. N Engl J Med 2006; 354: 131–140. 19 Adler AI, Stevens RJ, Manley SE, Bilous RW,
Cull CA, Holman RR: Development and progression of nephropathy in type 2 diabe-tes: the United Kingdom Prospective Diabe-tes Study (UKPDS 64). Kidney Int 2003; 63: 225–232.
20 Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 2004; 351: 1296–1305.
21 Kovesdy CP, Trivedi BK, Anderson JE: As-sociation of kidney function with mortality in patients with chronic kidney disease not yet on dialysis: a historical prospective co-hort study. Adv Chron Kidney Dis 2006; 13: 183–188.
22 Keith DS, Nichols GA, Gullion CM, Brown JB, Smith DH: Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care orga-nization. Arch Intern Med 2004; 164: 659– 663.
23 Nguyen HT, Stack AG: Ethnic disparities in cardiovascular risk factors and coronary dis-ease prevalence among individuals with chronic kidney disease: Findings from the Third National Health and Nutrition Exam-ination Survey. J Am Soc Nephrol 2006; 17: 1716–1723.
24 Wong JS, Port FK, Hulbert-Shearon TE, Car-roll CE, Wolfe RA, Agodoa LY, Daugirdas JT: Survival advantage in Asian-American end-stage renal disease patients. Kidney Int 1999; 55: 2515–2523.
25 Young BA, Rudser K, Kestenbaum B, Seliger SL, Andress D, Boyko EJ: Racial and ethnic differences in incident myocardial infarc-tion in end-stage renal disease patients: the USRDS. Kidney Int 2006; 69: 1691–1698. 26 Levin A, Djurdjev O, Barrett B, Burgess E,
Carlisle E, Ethier J, Jindal K, Mendelssohn D, Tobe S, Singer J, Thompson C: Cardiovascu-lar disease in patients with chronic kidney disease: getting to the heart of the matter. Am J Kidney Dis 2001; 38: 1398–1407. 1 Collins AJ, Kasiske B, Herzog C, Chavers B,
Foley R, Gilbertson D, Grimm R, Liu J, Lou-is T, Manning W, Matas A, McBean M, Mur-ray A, St Peter W, Xue J, Fan Q, Guo H, Li S, Roberts T, Snyder J, Solid C, Wang C, Wein-handl E, Arko C, Chen SC, Dalleska F, Daniels F, Dunning S, Ebben J, Frazier E, Johnson R, Sheets D, Forrest B, Berrini D, Constantini E, Everson S, Frederick P, Eg-gers P, Agodoa L: Excerpts from the United States Renal Data System 2004 Annual Data Report: atlas of end-stage renal disease in the united states. Am J Kidney Dis 2005; 45:A5– A7.
2 Klahr S, Levey AS, Beck GJ, Caggiula AW, Hunsicker L, Kusek JW, Striker G: The ef-fects of dietary protein restriction and blood-pressure control on the progression of chron-ic renal disease: modifchron-ication of diet in renal disease study group. N Engl J Med 1994; 330: 877–884.
3 The GISEN Group (Gruppo Italiano di Studi Epidemiologici in Nefrologia): Randomised placebo-controlled trial of effect of ramipril on decline in glomerular filtration rate and risk of terminal renal failure in proteinuric, non-diabetic nephropathy. Lancet 1997; 349: 1857–1863.
4 Diabetes Control and Complications (DCCT) Research Group: Effect of intensive therapy on the development and progression of diabetic nephropathy in the diabetes con-trol and complications trial. Kidney Int 1995; 47: 1703–1720.
5 Bakris GL, Weir MR, Shanifar S, Zhang Z, Douglas J, van Dijk DJ, Brenner BM: Effects of blood pressure level on progression of dia-betic nephropathy: results from the renal study. Arch Intern Med 2003; 163: 1555– 1565.
6 Barnett AH, Bain SC, Bouter P, Karlberg B, Madsbad S, Jervell J, Mustonen J: Angioten-sin-receptor blockade versus enzyme inhibition in type 2 diabetes and nephropathy. N Engl J Med 2004; 351: 1952– 1961.
7 Winkelmayer WC, Fischer MA, Schneeweiss S, Wang PS, Levin R, Avorn J: Underuse of ACE inhibitors and angiotensin II receptor blockers in elderly patients with diabetes. Am J Kidney Dis 2005; 46: 1080–1087. 8 Ostchega Y, Dillon CF, Hughes JP, Carroll M,
Yoon S: Trends in hypertension prevalence, awareness, treatment, and control in older US adults: data from the national health and nutrition examination survey 1988 to 2004. J Am Geriatr Soc 2007; 55: 1056–1065.
27 Elsayed EF, Tighiouart H, Griffith J, Kurth T, Levey AS, Salem D, Sarnak MJ, Weiner DE: Cardiovascular disease and subsequent kidney disease. Arch Intern Med 2007; 167: 1130–1136.
28 Gelber RP, Kurth T, Kausz AT, Manson JE, Buring JE, Levey AS, Gaziano JM: Associa-tion between body mass index and CKD in apparently healthy men. Am J Kidney Dis 2005; 46: 871–880.
29 Hsu CY, McCulloch CE, Iribarren C, Dar-binian J, Go AS: Body mass index and risk for end-stage renal disease. Ann Intern Med 2006; 144: 21–28.
30 Ducloux D, Kazory A, Simula-Faivre D, Chalopin JM: One-year post-transplant weight gain is a risk factor for graft loss. Am J Transplant 2005; 5: 2922–2928.
31 Kuo HW, Tsai SS, Tiao MM, Yang CY: Epi-demiological features of CKD in Taiwan. Am J Kidney Dis 2007; 49: 46–55.
32 Kalantar-Zadeh K, Block G, Humphreys MH, Kopple JD: Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Kidney Int 2003; 63: 793– 808.
33 Beddhu S: The body mass index paradox and an obesity, inflammation, and atherosclero-sis syndrome in chronic kidney disease. Semin Dialysis 2004; 17: 229–232.
34 Pliakogiannis T, Trpeski L, Taskapan H, Shah H, Ahmad M, Fenton S, Bargman J, Oreopoulos D: Reverse epidemiology in peritoneal dialysis patients: the Canadian experience and review of the literature. Int Urol Nephrol 2007; 39: 281–288.
35 Kovesdy CP, Trivedi BK, Kalantar-Zadeh K, Anderson JE: Association of low blood pres-sure with increased mortality in patients with moderate to severe chronic kidney dis-ease. Nephrol Dial Transplant 2006; 21: 1257– 1262.
36 Gerstein HC, Mann JF, Yi Q, Zinman B, Din-neen SF, Hoogwerf B, Halle JP, Young J, Rashkow A, Joyce C, Nawaz S, Yusuf S: Albu-minuria and risk of cardiovascular events, death, and heart failure in diabetic and non-diabetic individuals. JAMA 2001; 286: 421– 426.
37 Ma YC, Zuo L, Chen JH, Luo Q, Yu XQ, Li Y, Xu JS, Huang SM, Wang LN, Huang W, Wang M, Xu GB, Wang HY: Modified glo-merular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol 2006; 17: 2937– 2944.