行政院國家科學委員會專題研究計畫 成果報告
胰島素抵抗性併代謝性不良症候群在社區心血管疾病之流
行病學及遺傳角色研究
計畫類別: 個別型計畫 計畫編號: NSC93-2314-B-002-218- 執行期間: 93 年 08 月 01 日至 94 年 07 月 31 日 執行單位: 國立臺灣大學公共衛生學院預防醫學研究所 計畫主持人: 簡國龍 共同主持人: 許秀卿,李源德 計畫參與人員: 李惠真 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 94 年 10 月 28 日
行政院國家科學委員會補助專題研究計畫
■ 成 果 報 告
□期中進度報告
胰島素抵抗性併代謝不良症候群在社區心血管疾病之流行病學及
遺傳角色研究
計畫類別:■ 個別型計畫 □ 整合型計畫
計畫編號:NSC 93-2314-B-002-218
執行期間:93 年 08 月 01 日至 94 年 07 月 31 日
計畫主持人:簡國龍
共同主持人:李源德 許秀卿
計畫參與人員: 李惠真
成果報告類型(依經費核定清單規定繳交):■精簡報告 □完整報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
執行單位:台灣大學公衛學院預防醫學研究所
中 華 民 國 94 年 10 月 27 日
中文摘要 目的:代謝不良症候群在亞太地區的盛行率並不清楚。本研究是要了解在台灣地區代謝症候群的 演變情形以及對冠狀動脈心臟病及腦中風發生事件的危險。 方法及結果:在1990-1991 年建立的共 3602 位年齡超過 35 歲居民為一世代研究,共追蹤中位數 9 年的時間。 女性有較高的代謝症候群盛行率,而盛行率在最近的一次追蹤時間達到高峰。隨著 代謝症候群數目的逐漸增加,發生冠狀動脈心臟病的危險比有增加的情形,在數目超過3 個以上 的危險比為5.4 (95%信賴區間為 2.2~13.6),而腦中風的危險比為 3.5 (95%信賴區間 1.9~6.6)。在 代謝不良症候群,低的HDL-膽固醇及高的體質比對冠狀動脈心臟病為最高(危險比為 2.3),其次 為代謝症候群(危險比為 1.9) ,對腦中風發作而言,高血壓的危險比最高(3.0),其次為代謝症候 群(2.0)。在族群歸因性危險率(PAR)最高值是在冠狀動脈心臟病為低 HDL 值,在腦中風事件為高 血壓。而對代謝症候群的數目來預測冠心病及腦中風的ROC 曲線面積是相似的。 結論:在社區族群中女性有比男性較高的代謝症候群盛行率,且較高的冠心病及腦中風發病的危 險。 英文摘要
Objective--- Patterns of metabolic syndrome among populations in the Asian-Pacific areas remain
unknown. This study sought to determine the health transition of metabolic syndrome patterns and risks of coronary heart disease (CHD) and stroke.
Methods and Results--- A cohort of 3,602 individuals aged 35 years and above enrolled from one
Taiwan community in 1990-1991 was followed up for a median of 9.0 years. Women had higher
age-standardized metabolic syndrome prevalence rates than men, and the rates increased progressively to a peak in the 5th follow-up. As numbers of metabolic syndrome increased, the hazard risk (HR)
increased significantly, up to 5.4 (95% confidence interval [CI], 2.2-13.6) for coronary heart disease and 3.5 (95% CI, 1.9-6.6) for stroke events. Among the components of metabolic syndrome, low HDL cholesterol and high BMI had the highest risk for coronary heart disease (HR 2.3), and followed by metabolic syndrome (HR, 1.9). For stroke events, hypertension had the highest risk for stroke events (HR, 3.0), followed by metabolic syndrome (HR, 2.0). Highest population attributable risk values in low HDL cholesterol for coronary heart disease event and hypertension for stroke. The areas under ROC curves of the numbers of metabolic syndrome for coronary heart disease and stroke prediction were similar.
Conclusions--- Women had higher prevalence rates of metabolic syndrome than men in the community,
and increased risks of coronary heart disease and stroke events were significant for metabolic syndrome and its components.
報告內容
Coronary heart disease (CHD) and stroke events constitute a global public health burden, and prevention strategy should be implemented during the early atherosclerosis phase. Insulin resistance has an
Components of metabolic syndrome, including high glucose and blood pressure, dyslipidemia, and obesity are clustering together and with strong enhancement in diabetes risk.3,4 Incidences of diabetes increased progressively globally, especially among Asian-Pacific countries. 5 The Third Report of the National Cholesterol Education Program’s Adult Treatment Panel has proposed a general working criterion for the metabolic syndrome, eliciting important risk factors for monitoring community-based intervention programs.6
The incidences of CHD were lower and those of stroke were higher in the Asian-Pacific countries than in western countries. This might be associated with different patterns of contributory risk factors among ethnical groups. For example, Asian countries use lower body mass indexes than Caucasian people as obesity index.7 In general, the concentration of high density lipoprotein (HDL) cholesterol is lower for Asian populations than for Caucasian population, especially for men. Furthermore, by the process of urbanization and globalization, unhealthy lifestyle such as obesity, sedentary and smoking have become prevalent among Asian populations in recent years.8 No prospective cohort study has investigated the trends of metabolic syndrome patterns associating with CHD and stroke for Chinese population, especially in the community-based population. In this study, we investigated the prevalence rates of metabolic syndrome in a community cohort, examined the atherosclerotic risk factors serially during the follow-up periods, and compared the patterns as time progressed. Also, hazard risks on CHD and stroke events were assessed.
Materials and Methods Study design and population
The Chin-Shan Community Cardiovascular Cohort study has begun in 1990, following 1703 men and 1899 women aged 35 years old and above, homogenous in Chinese ethnicity, in Northern Taiwan for the study of cardiovascular diseases.9,10 Participants received baseline health examination at the
enrollment at a clinic set up at the community health center.10 Participants have undergone biannual repeated check-ups until the fifth follow-up in 2000.
In the survey, all study participants were individually interviewed from a structured questionnaire, for the information on socio-demographic characteristics, lifestyle, dietary characteristics, personal and family histories of diseases and hospitalizations. With the consent of participants, physicians and medical students medical conducted physical examinations and laboratory tests. Blood pressure was measured by trained medical assistants in the rest position. Body mass index (BMI) was calculated as weight (in kilograms)/height (in meters)2. Waist circumstance was measured by a trained examiner and determined using a measuring tape positioned at the midway between the lowest rib and the iliac crest. The measurement was made at minimal respiration status, with the tape snug but not compressing the skin. Electrocardiogram and echocardiography were also measured to evaluate cardiac structure and functions.
Blood sampling and analytic methods
The procedures of blood sampling and analytic methods have been described previously.10 In brief, serum samples were stored at -70℃ prior to the batch assay using standard enzymatic tests for
cholesterol and triglyceride (Merck 14354 and 14366, Germany) and precipitation methods for HDL and LDL cholesterol (Merck 14993 and Merck 14992). Glucose levels were measured by enzymatic assay (Merck 3389) using an Eppendorf 5060 autoanalyzer.
Definition of metabolic syndrome
We determined the metabolic syndrome status using criteria defined by the Third Adult Treatment Pane,6 modification by using the baseline BMI data instead of waist circumference for Asian
population.11 Therefore, a participant with three of following five criteria was defined as having the metabolic syndrome: 1) blood pressure of at least 130/85 mmHg or treated hypertension; 2) serum triglyceride of at least 150 mg/dL; 3) HDL cholesterol of <40 mg/dL in men and <50 mg/dL in women; 4) fasting glucose of 110 mg/dL or more; 5). BMI of 27 kg/m2 or greater,7 or waist circumference greater than 90 cm in men and 80 cm in women.12
Endpoint Verification
CHD events in this study included those with CHD events, such as myocardial infarction, and hospitalization due to procedures of coronary artery bypass graft and percutaneous coronary intervention. Death due to coronary heart disease was verified by medical records, office death certificates, or
household visit. Silent myocardial ischemia, defined by electrocardiographic deep Q wave pattern, was excluded. The stroke event was defined as death from stroke or hospitalization due to sudden
neurological deficit of vascular origin. Neuro-imaging studies for stroke cases were available for 20% in this rural area. To ensure the quality of the diagnosis of stroke morbidity and mortality, a committee was setup to review and confirm the death events and hospitalization history. Interview with family members were conducted in each death cases to verify unclear issues. All preliminary diagnoses and death
certificates were presented to this committee. The consistency of diagnostic meeting was maintained by regular discussion among the same committee members.
Statistical Analysis
We described the prevalence rates of metabolic syndrome status and components by gender and age, and plotted patterns of metabolic syndrome status by follow-up periods. The direct age-standardized prevalence rates of the metabolic syndrome were also calculated, using the world population as references.13
The effects of individual and multiple metabolic syndrome components on cardiovascular events were determined by Cox proportional hazards model, adjusting for age and smoking variables. We excluded participants who were cases of CHD or stroke in baseline, defined by history and
electrocardiographically abnormal Q wave. The proportionality assumption and the fit of the proportional hazards model were verified graphically and tested by the Grambsch and Therneau statistics.14
We specified the analyses by sex, and compared the importance of various metabolic syndrome components for predicting CHD and stroke events by 3 tests. The first was to test the magnitude of regression coefficients (hazard risk comparison) for each binary risk factors, which were compared by a test statistics z, where z=(b[MS]-b[C])/SE. b[MS] and b[C] were the regression coefficients of metabolic
syndrome components respectively, while SE was the standard error of the difference in the coefficients, computed as the square root of the sum of the squares of the standard error for the 2 coefficients. The z statistics tested the equality of hazard risks between metabolic syndrome and its specific components.15 The population attributable risk (PAR) fraction was used to estimate the effects attributed to the change in the risk proportion of the population. The formula was as follows: PAR=[(Prevalence x (Relative Risk-1)]/[Prevalence x (Relative Risk-1)+1]
Second, we used prediction model to estimate the ability to separate those who suffered CHD or stroke events from those who did not, for the discrimination between outcomes. We quantified the discrimination by calculating the quantity of c statistic, analogous to the area under a receiver operating characteristic (ROC) curve.16 The area-under-curve statistics showed the probability in the model and assigned a high risk to those who developed events than to those who did not. We also compared the areas under two receiver operating curves graphically by sex.
Third, we used the Hosmer-Lemeshow Chi-square statistic to test the agreement between predicted and observed outcomes based on calibration ability, dividing the cohort population risk for CHD or stroke events in the whole study period.17 The small Chi-square statistics indicated good calibration, and values exceeding 20 indicated significant lack of calibration. All statistical analyses were performed using SAS version 8.2 (SAS Institute, Inc., Cary, NC) and STATA version 7 (Stata Corp., College Station, Texas).
Results
Among 3,602 subjects in the cohort, age-standardized prevalence rates of metabolic syndrome were higher in women than in men (26.4% vs. 20.2% by world population, 28.2% vs. 19.7% by European population). Figure 1 shows that prevalence rates for women increased as age increased until 65-74 years old, and increased as the follow-up progressed, to a peak of 39.8% in the 5th follow-up. On the other hand, the rates for men were stable as age increased except for those aged 75 and above in the 2nd follow-up period. The age-specific changes among follow-up were somewhat moderate for men. The gender difference was much greater when the prevalence was estimated by the waist circumstance for central obesity than by BMI (Figure 2).
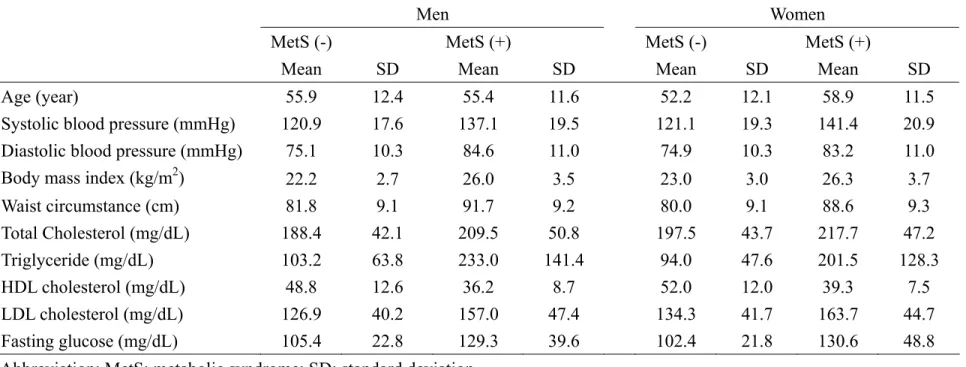
Table 1 shows the average baseline age and atherosclerotic risk measured by sex and metabolic syndrome status. Women with metabolic syndrome had the highest average values in age, systolic blood pressure, body mass index, total and LDL cholesterol and fasting glucose levels, and men with
metabolic syndrome had highest triglyceride and lowest HDL cholesterol. These atherosclerotic risk prevalence rates among persons with metabolic syndrome were also higher for women than men, particularly in hypertension (82% vs. 76 %) and low HDL (95% vs. 76 %). Men had much higher smoking rates than women. There was no significant association between smoking and metabolic syndrome.
Figure 3 shows the prevalence of metabolic syndrome components and incidence rates for CHD and stroke events by metabolic syndrome numbers in each sex. Both CHD and stroke rates increased when the numbers of metabolic syndrome component increased, reaching to the peak among individuals
with 4 or 5 components. Also, the stroke incidence rates were higher than CHD rates, and men were at higher risk than women in all category groups.
The 11-year survival rates of CHD were 94.2% among those with metabolic syndrome and 96.9% among those with no metabolic syndrome (data not shown). As components of metabolic syndrome increased, the 11-year survival rates of CHD events decreased progressively, from 99.3% for individuals with none of these components to 92.7% for those with 4-5 components. A similar pattern of metabolic syndrome risk was also observed on stroke events with the corresponding survival rates of 96.2% and 91.7%, respectively. Both survival relationships appeared the dose-response trend significantly (P<0.001).
Hazard risks for CHD and stroke events with the metabolic syndrome and its components, adjusted for age, genders and smoking status, were significant in both genders (Table 2). As numbers of
metabolic syndrome increased, the hazard risks (HR) increased in significant dose-response trends to 5.4 (95% confidence interval [CI]=2.2 to13.6) for CHD and 3.5 (95% CI=1.9 to 6.6) for stroke events with 4-5 components. Low HDL cholesterol and high BMI were the components of metabolic syndrome associated with the highest risk of CHD (HR 2.3), followed by metabolic syndrome (HR, 1.9), while hypertension was the factor associated with the highest risk of stroke events (HR, 3.0; 95% CI=2.0 to 4.4) also followed by metabolic syndrome (HR, 2.0; 95% CI=1.4 to 2.9).
The population attributable risk (PAR) fraction varied among those components. The low HDL cholesterol had the greatest PAR (39%) to CHD events but the least PAR (10%) to stroke. Instead, hypertension has the greatest impact (PAR, 45%) on stroke.
To estimate the discrimination ability of components and numbers of metabolic syndrome in the prediction of CHD and stroke events, we calculated the area under ROC curve. The areas under ROC curves using the numbers of metabolic syndrome as a single factor for both CHD and stroke prediction were similar (0.6603 for CHD and 0.6604 for stroke). The measures of discrimination ability showed that metabolic syndrome alone had the highest c statistics among all components of metabolic syndrome (0.774 in CHD and 0.787 in stroke, Figure 4). The discrimination ability of hypertension was similar to that of metabolic syndrome in stroke event prediction. The calibrations of metabolic syndrome and components for predicting CHD and stroke events, partitioned by the Hosmer and Lemeshow test, were well-fitted with the P values of the chi-square test, 0.265 for CHD and 0.159 for stroke.
計畫成果自評
Metabolic syndrome components and status played important roles for CHD and stroke events for Taiwanese population. We clearly demonstrated that prevalence rates of metabolic syndrome increased progressively, especially among older women. Also, the metabolic syndrome as an entity had the highest discrimination ability to specify cardiovascular events. It can serve as a prominent modifiable risk aimed at preventing stroke through hypertension control and preventing CHD through both lipid lowering and hypertension control.
Urbanization and globalization in developing countries have contributed a great impact on
an indicator among public health burdens. Increasing rates of metabolic syndrome among community should be taken into serious consideration, even in areas with a low incidence of CHD. Our study showed the age-standardized prevalence rates of metabolic syndrome in Taiwan were higher than that in the US and European countries.18,19 Also, the rates in this study cohort increased significantly, reached to a peak in the most recent follow-up periods. It implied that metabolic syndrome had cumulative impacts on general population, especially for women. Racial difference between metabolic syndrome prevalence was found: American Africans and American Indians had higher prevalence but their myocardial
infarction risk was not proportionally increased.20 The emerging issue of high metabolic syndrome rates in Taiwan should be taken into consideration for planning further prevention program including health promotion and lifestyle intervention.
The estimated hazard risks of cardiovascular disease events associated with metabolic syndrome components were compatible with other community-based studies for the elderly population,21 Indian American20 and European.22,23 But elaborative observations revealed specific patterns for the population in ethnic Chinese. The prevalence rates of metabolic syndrome appeared to be higher in women than in men by either age or follow-up chronicle period, with obesity playing limited role among Taiwanese. Obesity index was also found not to be an independent risk for CHD in some study,24 and the possible explanation was that obesity was rather important risk for younger age. When study population was older, obesity did not emerge as an independent predictor, especially when other components of
metabolic syndrome were included. Moreover, an accurate measurement of increased visceral adiposity might be used a surrogate marker.
Low HDL cholesterol and hypertension were the most prevalent and important components of metabolic syndrome in Taiwan. In contrast, central obesity is the highest risk attribute among general American, and the rates of metabolic syndrome were higher for men than women.18 It has been noted that cholesterol levels were lower in the Asian-Pacific populations,25 compared with that in Caucasians, implicating the low HDL cholesterol as an important role in CHD events among Asian-Pacific
populations.
In addition to having the strongest effect on the risk of stroke, hypertension appeared an important risk factor for CHD as well in this study, having a significant PAR fraction. In conjunction with BMI and triglyceride, measurements of HDL cholesterol and blood pressure are useful for the awareness of CHD risk and crucial for reducing atherosclerotic risk burdens among population.
Other than individual disease prediction, metabolic syndrome as multiple risk clusters is a useful tool for identifying the magnitude of cardiovascular diseases in a community, and measuring the abilities of discrimination and calibration. We found that subjects with metabolic syndrome had an elevated likelihood of developing cardiovascular diseases. For population in Taiwan, high comorbidities such as hypertension, hyperglycemia and hyperlipidemia are also demonstrated in other screening programs.26 It is important to provide counseling on lifestyle modification to persons with metabolic syndrome.
even after a decade follow-up and it might have less power to validate model fitting. Second, we did not stratify stroke events into subtypes. Although different pathogenesis is implied between ischemic and hemorrhagic strokes, it is practical to consider stroke as one entity for the purpose of disease control. We integrated all types of stroke into one endpoint due to a large portion of unclassified stroke (around one third), and we focused on the risk profiles on one stroke endpoint.9 Finally, we used BMI instead of waist circumstance as the indicator of central obesity in the baseline. The national survey data in Taiwan has demonstrated a significant relationship between BMI and waist circumstance.27 Even waist
circumstance was not an universal risk for CHD in various population. 24
Summary
Our study suggests that metabolic syndrome is prevalent in the study community, especially among older women. The components of metabolic syndrome had differential effects on CHD and stroke events, and had capability to discriminate these events. Of the risk factors identified, interventions for stroke prevention through hypertension control and for CHD prevention through lipid and hypertension control would have a great impact on the health of the study population.
參考文獻
1. Reaven GM. Role of insulin resistance in human disease: Banting lecture 1988. Diabetes 1988;37:1595-1607.
2. DeFronzo RA, Ferrannini E. Insulin resistance. A multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovasular disease. Diabetes Care 1991;14:173-194.
3. Boyko EJ, MD MPH, de Courten MM, Zimmet PZ, MD, Chitson PM, Tuomilehto JP, Alberti K, George MM, DPHIL. Features of the Metabolic Syndrome Predict Higher Risk of Diabetes and Impaired Glucose Tolerance: A prospective study in Mauritius. Diabetes Care 2000;23:1242-1248.
4. Hanson RL, Imperatore G, Bennett PH, Knowler WC. Components of the "Metabolic Syndrome" and Incidence of Type 2 Diabetes. Diabetes 2002;51:3120-3127.
5. Zimmet P, Alberti KG, Shaw J. Global and societal implications of the diabetes epidemic. Nature 2001;414:782-787.
6. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult treatment panel III). J A M A 2001;285:2486-2497.
7. WHO expert consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004;363:157-63.
8. Reddy KS. Cardiovascular disease in non-Western countries. N Engl J Med 2004;350:2438-2440.
9. Chien KL, Sung FC, Hsu HC, Su TC, Lin RS, Lee YT. Apolipoprotein A1 & B, and stroke events in a community-based cohort in Taiwan: Report of Chin-Shan Community Cardiovascular Study. Stroke 2002;33 :39-44.
Chin-Shan Community Cardiovascular Cohort in Taiwan: baseline data and five-year follow-up morbidity and mortality. J Clin Epidemiol 2000;53:836-846.
11. Wong ND, Sciammarella MG, Polk D, Gallagher A, Miranda-Peats L, Whitcomb B, Hachamovitch R, Friedman JD, Hayes S, Berman DS. The metabolic syndrome, diabetes, and subclinical atherosclerosis assessed by coronary calcium. J Am Coll Cardiol 2003;41:1547-1553.
12. Inoue S, Zimmet P. The Asia-Pacific Perspective: redefining obesity and its treatment. Sidney: Health Communications Asutralia Pty Limited; 2000.
13. Breslow NE, Day NE. Statistical methods in cancer research. Volume II. The design and analysis of cohort studies. Lyon: IARC; 1987.
14. Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika 1994;81:515-526.
15. D'Agostino RB, Sr., Grundy S, Sullivan LM, Wilson P. Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation. J A M A 2001;286:180-187.
16. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982;143:29-36.
17. Hosmer DWJr, Lemeshow S. Applied logistic regression. New York: John Wiley & Sons; 1989.
18. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA 2002;287:356-359.
19. Hu G, Qiao Q, Tuomilehto J, Balkau B, Borch-Johnsen K, Pyorala K. Prevalence of the metabolic syndrome and its relation to all-cause and cardiovascular mortality in nondiabetic European men and women. Arch Intern Med 2004;164:1066-1076.
20. Resnick HE, PhD, On behalf of the Strong Heart Study Investigators. Metabolic Syndrome in American Indians. Diabetes Care 2002;25:1246-1247.
21. Lindblad U, Langer RD, 2, Wingard DL, 2, Thomas RG, 2, Barrett-Connor EL, 2. Metabolic Syndrome and Ischemic Heart Disease in Elderly Men and Women. American Journal of Epidemiology 2001;153:481-489.
22. Isomaa BM, Almgren PM, Tuomi TM, Forsen BM, Lahti KM, Nissen MM, Taskinen MRM, Groop LM. Cardiovascular Morbidity and Mortality Associated With the Metabolic Syndrome. Diabetes Care 2001;24:683-689.
23. Lakka HMM, Laaksonen DE, MD MPH, Lakka TA, MD P, Niskanen LK, MD P, Kumpusalo EM, Tuomilehto JM, Salonen JT, MD P. The Metabolic Syndrome and Total and Cardiovascular Disease Mortality in Middle-aged Men. JAMA 2002;288:2709-2716.
24. Ninomiya JK, L'Italien G, Criqui MH, Whyte JL, Gamst A, Chen RS. Association of the metabolic syndrome with history of myocardial infarction and stroke in the third national health and nutrition examination survey. Circulation 2004; 109:42-46.
Classification Involves the Metabolic Syndrome in Japanese. Diabetes Care 2002;25:1252-1253. 26. Chen TH, Chiu YH, Luh DL, Yen MF, Wu HM, Chen LS, Tung TH, Huang CC, Chan CC, Shiu MN, Yeh YP, Liou HH, Liao CS, Lai HC, Chiang CP, Peng HL, Tseng CD, Yen MS, Hsu WC, Chen CH. Community-based multiple screening model: design, implementation, and analysis of 42,387 participants. Cancer 2004;100:1734-1743.
27. Pan WH, Flegal KM, Chang HY, Yeh WT, Yeh CJ, Lee WC. Body mass index and
obesity-related metabolic disorders in Taiwanese and US whites and blacks: implications for definitions of overweight and obesity for Asians. Am J Clin Nutr 2004;79:31-39.
附錄
Figure legends:
Figure 1. Prevalence rates of the metabolic syndrome among study population by sex and age during follow-up periods.
Figure 2. Comparisons in prevalence rates of the metabolic syndrome between men and women in the Chin-Shan Community for baseline and follow-up periods by body mass index (BMI) ≥ 27 kg/m2 and waist circumstance (WC) (men ≥90 cm, women ≥80cm).
Figure 3. Prevalence of metabolic syndrome components (bar) and incidence of CHD and stroke by metabolic syndrome components (line) among the study population, stratified by genders
Figure 4. Discrimination ability, presented by c statistics, of metabolic syndrome and components for CHD and stroke events among study population
11
Table 1. Basic demographic and atherosclerotic risk factors of metabolic syndrome among the study population.
Men Women
MetS (-) MetS (+) MetS (-) MetS (+)
Mean SD Mean SD Mean SD Mean SD
Age (year) 55.9 12.4 55.4 11.6 52.2 12.1 58.9 11.5
Systolic blood pressure (mmHg) 120.9 17.6 137.1 19.5 121.1 19.3 141.4 20.9
Diastolic blood pressure (mmHg) 75.1 10.3 84.6 11.0 74.9 10.3 83.2 11.0
Body mass index (kg/m2) 22.2 2.7 26.0 3.5 23.0 3.0 26.3 3.7
Waist circumstance (cm) 81.8 9.1 91.7 9.2 80.0 9.1 88.6 9.3 Total Cholesterol (mg/dL) 188.4 42.1 209.5 50.8 197.5 43.7 217.7 47.2 Triglyceride (mg/dL) 103.2 63.8 233.0 141.4 94.0 47.6 201.5 128.3 HDL cholesterol (mg/dL) 48.8 12.6 36.2 8.7 52.0 12.0 39.3 7.5 LDL cholesterol (mg/dL) 126.9 40.2 157.0 47.4 134.3 41.7 163.7 44.7 Fasting glucose (mg/dL) 105.4 22.8 129.3 39.6 102.4 21.8 130.6 48.8
Abbreviation: MetS: metabolic syndrome; SD: standard deviation,
Table 2. Hazard risk (HR), 95% confidence interval (CI) and estimated population attributable risk (PAR) by numbers of metabolic syndrome and component , controlling for sex, age and smoking status.
CHD Stroke
Numbers HR 95% CI P value PAR HR 95% CI P value PAR
0: Reference 1.0 1.0
1 1.9 0.8 4.6 0.139 0.22 1.0 0.5 1.8 0.883 0.02
2 4.0 1.7 9.1 0.001 0.40 2.3 1.3 4.0 0.004 0.22
12
4-5 5.4 2.2 13.6 <0.0001 0.29 3.5 1.9 6.6 <.0001 0.19
P for trend <0.0001 <0.0001
Metabolic syndrome 1.9 1.2 3.0 0.007 0.17 2.0 1.4 2.9 <.0001 0.20
Hypertension 1.8 1.1 2.8 0.011 0.25 3.0 2.0 4.4 <.0001 0.45
High body mass index 2.3 1.4 3.9 0.002 0.16 1.7 1.1 2.6 0.020 0.09
High triglycerides 1.9 1.2 2.9 0.007 0.17 1.6 1.2 2.3 0.006 0.14
Low HDL cholesterol 2.3 1.5 3.7 <0.0001 0.39 1.2 0.9 1.7 0.233 0.10
Hyperglycemia 1.2 0.8 1.8 0.476 0.05 1.7 1.2 2.4 0.002 0.18
Abbreviation: CHD: coronary heart disease, HR: hazard risk, CI: confidence interval, PAR: population attributable risk, Figure 1.
20
30
40
50
60
70
Women: 5th F/U
Women: 2nd F/U
Women: 1st F/U
Women: baseline
Men: 5th F/U
Men: 2nd F/U
Men: 1st F/U
Men: baseline
13 Figure 2.
Women, WC
Women, BMI
Men, BMI
Men, WC
10
15
20
25
30
35
40
45
50
55
Baseline
1st 2nd
5th
Follow-up
P
rev
al
enc
e r
ate (
%
)
14 Figure 3.
0
10
20
30
40
0 1 2 3 4, 5
Prev
alenc
e
rat
es
(%)
0
2
4
6
8
10
12
CHD i
nci
de
nce
ra
te
s(
/1
00
0)
0
10
20
30
40
0
1
2
3 4,5
P
rev
alenc
e
ra
te
s
0
2
4
6
8
10
12
S
tro
ke
inc
idenc
e
ra
te
s
(/1000)
0
10
20
30
40
0
1
2
3 4, 5
P
rev
alenc
e
ra
te
s(%
)
0
2
4
6
8
10
12
S
tro
ke
inc
idenc
e
ra
te
s(
/1
000)
0
10
20
30
40
0 1 2 3 4,5
Prev
alenc
e
ra
te
s
0
2
4
6
8
10
12
CHD i
nci
de
nce
rat
es
(/
1000)
Men
Women
15 Figure 4. 0.72 0.73 0.74 0.75 0.76 0.77 0.78 0.79 0.80
Coronary heart disease Stroke
c statisti
cs
Metabolic syndrome numbers High blood pressure
High body mass index Hypertriglyceridemia Low HDL-C