Wireless Health Care Service System
for Elderly With Dementia
Chung-Chih Lin, Member, IEEE, Ming-Jang Chiu, Chun-Chieh Hsiao, Ren-Guey Lee, Member, IEEE,
and Yuh-Show Tsai, Member, IEEE
Abstract—The purpose of this paper is to integrate the
technolo-gies of radio frequency identification, global positioning system, global system for mobile communications, and geographic infor-mation system (GIS) to construct a stray prevention system for elderly persons suffering from dementia without interfering with their activities of daily livings. We also aim to improve the pas-sive and manpowered way of searching the missing patient with the help of the information technology. Our system provides four monitoring schemes, including indoor residence monitoring, out-door activity area monitoring, emergency rescue, and remote mon-itoring modes, and we have developed a service platform to imple-ment these monitoring schemes. The platform consists of a web service server, a database server, a message controller server, and a health-GIS (H-GIS) server. Family members or volunteer workers can identify the real-time positions of missing elderly using mobile phone, PDA, Notebook PC, and various mobile devices through the service platform. System performance and reliability is analyzed. Experiments performed on four different time slots, from three lo-cations, through three mobile telecommunication companies show that the overall transaction time is 34 s and the average deviation of the geographical location is about 8 m. A questionnaire surveyed by 11 users show that eight users are satisfied with the system stability and 10 users would like to carry the locating device themselves, or recommend it to their family members.
Index Terms—Dementia, elder, geographic information system
(GIS), global positioning system (GPS), global system for mobile communications (GSM), health care, radio frequency identification (RFID), ubiquitous network.
I. INTRODUCTION
C
HRONIC diseases are the greatest health threat faced by the elderly in an aging society. In general, about 75% of the elderly have one or more chronic disease, of which dementia is one of the most common. Previous studies show that theManuscript received September 2, 2005; revised December 11, 2005. This work was supported in part by the National Science Council, Taiwan, R.O.C., under Grant NSC 94-2614-E-182-003.
C.-C. Lin is with the Department of Computer Science and Information Engineering, Chang Gung University, Tao-Yuan 333, Taiwan, R.O.C. (e-mail: [email protected]).
M.-J. Chiu is with the Department of Neurology and the College of Medicine, National Taiwan University, Taipei 100, Taiwan, R.O.C. (e-mail: [email protected]).
C.-C. Hsiao is with the Department of Computer and Information Network Engineering, Lunghwa University of Science and Technology, Tao-Yuan 333, Taiwan, R.O.C. (e-mail: [email protected]).
R.-G. Lee is with the Department of Electronic Engineering, Na-tional Taipei University of Technology, Taipei 106, Taiwan, R.O.C. (e-mail: [email protected]).
Y.-S. Tsai is with the Department of Biomedical Engineering, Chung Yuan Christian University, Chung Li 32023, Taiwan, R.O.C. (e-mail: [email protected]).
Digital Object Identifier 10.1109/TITB.2006.874196
incidence of dementia in the elderly is about 5%–6% in the developed countries [1]–[4]. This rate rises to as high as 10%– 20% among the elderly aged over 85 years. Research on elderly persons with dementia recently carried out in Taiwan [6]–[8] has found that the incidence of dementia among the elderly is about 4%. Problems specific to dementia include memory impairments, behavioral problems, other mental symptoms, and patients’ inability to take care of themselves. Due to the problem of memory loss, the elderly with dementia are prone to straying when outdoors. The safety of missing elderly persons may be seriously jeopardized if caretakers cannot locate them within the “golden 24 h.”
Many successful health care applications based on ubiqui-tous computing and communication technologies have been pre-sented in the literature [12], [14], [16], [19], [20]. These appli-cations can help physicians obtain patients’ electronic records anywhere and anytime in the hospitals. Locating the current positions of patients outside the hospitals is one important re-quirement in the health care system design. We have integrated global positioning system (GPS), global system for mobile com-munications (GSM), and geographic information system (GIS) to monitor patients with arrhythmia [13], [21], and also to im-plement emergency dispatching of ambulances [22] and conduct disease prevention tasks in public health [23]. An advanced com-prehensive health care employing wearable biosensors allows ongoing in-home health monitoring of individual patients [15]. Various applications have been proposed for the care of the el-derly with dementia. Examples include use of video games and computers to infer the cognitive performance of the elderly [10], and observation of the elderly with dementia via monitoring of daily living facilities [11], [17], or with computer vision tech-niques [18] that do not disturb the patient’s normal life.
The purpose of this paper is to integrate the technologies of radio frequency identification (RFID), GPS, GSM, and GIS to construct a stray prevention system for the elderly that does not interfere with the elders’ daily lives, and employ informa-tion network technology to improve on past-passive and manual search assistance schemes. Our system provides four monitor-ing schemes, includmonitor-ing indoor residence monitormonitor-ing, outdoor activity area monitoring, emergency rescue, and remote mon-itoring modes. The user interface design allows family mem-bers or other caretakers to identify the real-time positions of the missing elderly persons using mobile phones, PDAs, Note-book PCs, and various mobile devices through a health care platform consisting of a web service server, database server, message controller server, and health-GIS (H-GIS) server. This paper is organized as follows: Section II describes the service
LIN et al.: WIRELESS HEALTH CARE SERVICE SYSTEM FOR ELDERLY WITH DEMENTIA 697
model, database framework, and system design methodology. Section III presents application implementation and assessment. Section IV provides some concluding remarks and areas where further work is needed.
II. SERVICEANALYSIS ANDSYSTEMDESIGN
A. Service Modes
The system’s four monitoring modes include indoor residence monitoring, outdoor activity area monitoring, emergency rescue, and remote monitoring. The services provided in each mode are described as follows.
1) Indoor residence monitoring mode: This system can au-tomatically detect if an elderly person with dementia en-ters or leaves certain specific areas such as a kitchen or bathroom, or leaves home alone without notice. When an elderly person leaves home alone, the system sends a warning message to the call center through a wireless net-work. The neighborhood, care provider, or family member will receive the message immediately, allowing sufficient time to prevent the elderly person from encountering any danger.
2) Outdoor activity area monitoring mode: When family members accompany an elderly person to a hospital or for some outdoor activities, a pushing on the button of the locator can set the patients’ activity area. Once the patient leaves the preset area, an alarm signal will be sent to family members via a GSM network.
3) Emergency rescue mode: When an elderly finds himself or herself in an emergency situation, he or she can press the emergency rescue button to send an emergency message to the call center. After the call center receives this mes-sage, it will examine the transmitted data to identify the patient, record the emergency situation, and transmit the geographical data, including patient profile and location information, to relevant caretakers, search volunteers, and family members.
4) Remote monitoring mode: Family members can connect to the call center through the network when they want to know the current location of an elderly member with dementia. After ID authentication, the system will auto-matically report the current location via a single location report mode or periodic location report mode.
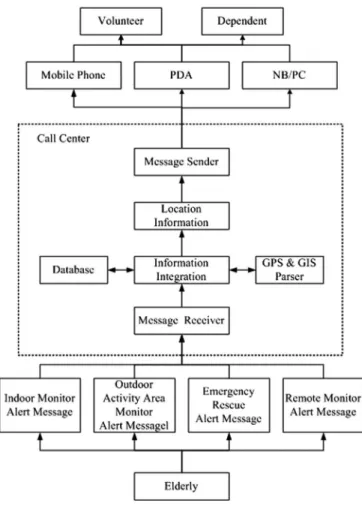
Whenever one of the aforementioned abnormal situations happens to a patient (Fig. 1), the location-monitoring device will immediately send out a message containing the patient’s status and GPS information to the call center. After the call center receives this data packet, it will convert the longitude and latitude coordinates into a street map location using a GPS and GIS parser, and combine this location with other basic in-formation such as personal characteristics, height, weight, and photograph to generate the complete information needed for search and assistance tasks. To facilitate search work, different operating interfaces are provided so that search volunteers or family members can obtain relevant information concerning the missing person via mobile phone, PDA, or notebook PC, etc.
Fig. 1. Flowchart of the search assistance for stray dementia elderly.
B. Conceptual Database Model
When a patient is missing, the system will produce multiple tracing information packages (TIPs) recording the whole search process. A TIP is defined as TIP(TIPID, EventID, EdlerID,
State, DateTime) where TIPID is the increasing serial number
of each TIP, EventID is the unique event ID, and ElderID is the elder’s social ID number referred to as ELDER entity. To trace event status, the TIP also includes State and DateTime proper-ties. The State property is used to describe the tracing mode, and includes the five states of leaving home (H state), leaving activity area (A state), emergency rescue situation (E state), re-mote single location report (S state), periodic location report (P state), and event close (C state). The DateTime property records the time of each TIP. The State and DateTime properties enable users to reconstruct the tracing procedures of each event. When an event occurs (could be active rescue signal from the elderly or remote monitoring), an EventID will be issued. Throughout the rescue searching session, every reply record by the locating de-vice will be marked with the same EventID . For example, when an elderly leaves home alone, the system will receive an alert in-formation and generate the first TIP record (1, 1, G123456789, 2005/12/01 8:00 A.M., H) for this event. If the family mem-bers of the elderly start the mechanism of continuous location report, the system will continuously record consecutive TIPs such as (2, 1, G123456789, 2005/12/01 8:10 A.M., P), (3, 1,
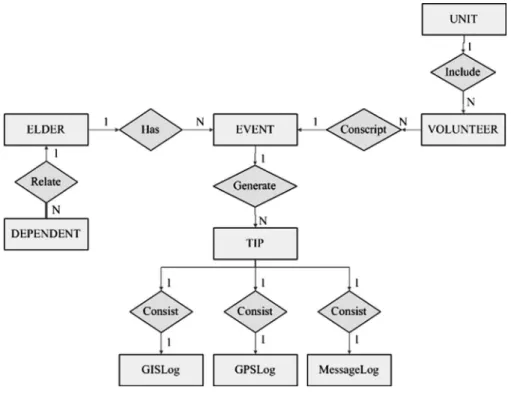
Fig. 2. ER diagram of wireless health care service system for elderly with dementia.
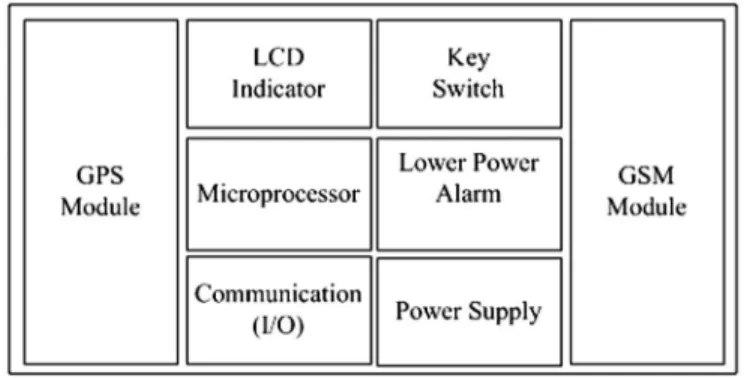
Fig. 3. Block diagram of residence motion sensor.
G123456789, 2005/12/01 8:15 A.M., P), . . ., etc. After the el-derly has been found, a record (N, 1, G123456789, 2005/12/01 9:15 A.M., C) will be generated to finish the whole event.
As shown in Fig. 2, an entity-relationship (ER) diagram can be used to model wireless health care service system scenarios for patients with dementia [24]–[26]. ELDER entity, DEPEN-DENT entity, and VOLUNTEER entity, respectively, contain the attributes of patients with dementia, elders’ family members, and volunteer workers providing searching service. Because an elderly may have more than one stray event, the EVENT en-tity may have a one-to-many relationship. EVENT attributes include event ID (primary key), event start time, and event end time and final result. The tracing of a stray event may consist of several TIPs. The relationship between EVENT and TIP is, thus, a one-to-many relationship. Besides the basic informa-tion (serial number, state, datetime, etc.), the TIP entity also consists of GPSLog, GISLog, and MessageLog. These three entities record location information when the elder is moving. The GPSLog entity records the longitude, latitude, speed, di-rection, and GPS sampling time. The GISLog entity contains the attributes of the intersections, streets, landmarks, and
elec-tronic maps. The MessageLog entity consists of message type (SMS or MMS), ReceiveTime (the time when the message is re-ceived), SendTime (the time when the message is transmitted), ReceiveMessage (the content of the received rescue message), SendMessageText (the content of transmitted text message), and SendMessageImage (GIS image and elder’s photograph).
C. Indoor Residence Motion Sensor
The indoor residence motion sensor utilizes the techniques [26], [27] to place different types of tags in the objects that the elders frequently use (e.g., shoes, key chains, glasses frames, and belts) to install sensors without disturbing the elderly persons’ daily lives. The sensing tags contain various data such as the elders’ identification codes.
The residence sensor mainly consists of a passive RFID reader, a microprocessor, and a GSM module as shown in Fig. 3. The RFID reader is used to sense the tag attached on the patient so as to determine the patient’s identity and current location. The microprocessor processes the data. The GSM module is used to transmit emergency messages. Activity alert area such as the
LIN et al.: WIRELESS HEALTH CARE SERVICE SYSTEM FOR ELDERLY WITH DEMENTIA 699
Fig. 4. Block diagram of body-attached locator.
doorway is controlled via the collocation of adjustment of the antenna and the passive RFID tag. When the embedded micro-processor sensed that the patient left home alone, it will trans-mit a short message via SMS to notify the service management platform. This would initiate necessary measures to prevent the patient from getting lost, or suffering any misfortune.
D. Body-Attached Rescue Locator
The hardware design of the body-attached rescue locator is as shown in Fig. 4 and consists of the following parts.
1) GPS satellite location module: This is used to provide satellite location information needed to trace the patient, such as longitude/latitude coordinates, time, speed, and direction.
2) GSM communication module: This provides a commu-nication channel to transmit emergency rescue messages concerning the senior and receive commands from the remote server.
3) Microprocessor: The microprocessor performs signal analysis, command execution, and logical judgment. One of the most important logical judgments is determination of the activity area. When the locator sets the activity area, the microprocessor first records the original GPS coordinates (E1, N1) and then generates a new pair of GPS coordinates (Et, Nt) for every fixed time interval t.
If the distance between the original GPS coordinates and the new GPS coordinates exceeds some threshold value
D, the system will initiate reporting that the patient has
departed the activity area.
4) Low-power alarm: When 10% of the power is left, this function sends a message to the patient’s caregiver to re-place the battery so as to ensure the normal operation of the system.
5) Human–machine interface: This interface consists of an LED display indicating the current operating status of the device and providing two function keys, respectively, allowing the user to perform emergency rescue and activity area settings.
The body-attached rescue locator and the backend manage-ment platform communicate with each other via GSM short messages. The command format is (#ID, PW, CommandID, [Message*]#). All the instructions are enclosed within two “#” signs. The ID and PW stand for user ID and password,
respec-tively. When the user ID and password are authenticated, the in-struction issued by CommandID and Message will be executed. There are two types of instructions. Type I instructions are trans-mitted from the server to the locator. This type of instructions mostly concerns system settings, such as set time intervals for periodic reporting, request to send current location immediately, etc. Upon receiving the instruction, the locator will perform the instruction and send an acknowledgement code to the server. Type II instructions are used by the locator to report current lo-cation information to server. The reporting modes can be the sin-gle location-reporting mode for an emergent call, or the periodic location-reporting mode. The fourth parameter is an optional [Message] parameter. The “∗” sign signifies that the message may have zero, one, or multiple values depending on the function of the instructions. The parameters are separated by commas.
E. Service Management Health Care Platform
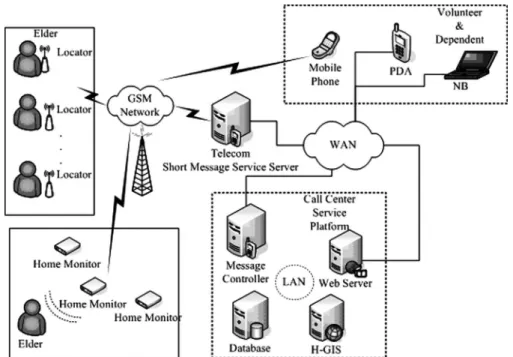
This platform consists of four servers as shown in Fig. 5. The first one is a database server responsible for data storage and management. The second one is a web service server, which provides portal service for external users. This server is also responsible for data integrating and GUI format converting for different resolutions and aspect ratio of display devices. The third one is a message controller connected to the telecom’s short message server through a network. This server imple-mented the acceptation and transmission of a large volume of short messages via network packets to enhance the efficiency of message processing. The last one is a HGIS. GISs are widely used in transportation and emergency rescue work. In this study, the concept of graphic overlays is used to represent different information concerning place of residence, community medical resources, and location of the elderly person with dementia. The geographic information interface allows searchers to efficiently acquire geographical spatial information concerning the miss-ing patient and dispatch personnel more effectively. The other function of the H-GIS is to convert the GPS longitude/latitude coordinates to location information in terms of street address and important landmarks, allowing the history of the patient’s movements to be recorded. If both the search assistants and pa-tient have a GPS locator with them, the server will track the movements of both parties, while also will inform members of the search team of the shortest path to the elderly patient.
III. SYSTEMIMPLEMENTATION ANDASSESSMENT The indoor residence motion sensor is installed beside the main entrance of the elder’s home to detect whether the elder’s tag has appeared within a range of 2 m. When the sensor detected the RFID tag while the elder is either entering or closing to the hot area, a timer is started as depicted in Fig. 6. If a family member’s tag is detected within a preset time T (T is 3 min in this study), indicating that the elder is accompanied by a family member, then the timer is stopped. If, on the contrary, a family member’s tag is not detected within a preset time T , indicating that the elder is leaving home alone, then our system will transmit an alarm short message via GSM to relevant
Fig. 5. System architecture of service platform in call center.
Fig. 6. Flowchart for indoor residence monitoring.
Fig. 7. Top layer (left) and bottom layer (right) of locator’s PCS.
personnel, who can initiate various necessary measures to prevent the elder from getting lost.
The body-attached rescue locator device (Fig. 7) consists of a low-power microcontroller, a GSM module, a GPS module, power management, and other I/O circuit. The Texas Instrument MSP430F149 is chosen as the core control unit due to its ul-tra low-power consumption. The GSM and GPS functions of the locator are performed by a Wavecom Q2403 GSM mod-ule and a U-Blox TIM-LP GPS modmod-ule. The power consump-tion of the GSM module is 260-mA average current in voice
LIN et al.: WIRELESS HEALTH CARE SERVICE SYSTEM FOR ELDERLY WITH DEMENTIA 701
Fig. 8. Workflow of tracking service.
communication (GSM 9000, Pmax) and less than 16 mA in idle mode. Whereas the GPS module consumes an average of 56 mA, the rest of the locator circuit power consumption is es-timated less than 5 mA at 3-V supply. The overall current is 321 mA (peak) and 77 mA (standby). By using an 800-mAH lithium rechargeable battery, the locator offers 623-min (∼10 h) standby time. For the continuous tracking mode, the locator reports GPS information every 3 min via GSM/SMS, if it takes 15 s to send a short message, the locator can last for 495 min (∼8.25 h), theoretically. An experiment has been conducted to test the actual power consumption in the 3-min continuous tracking mode. The results showed that a locator, with a fully charged 800-mA·H battery, could last for 422 min. The locator reports the geographical position via the GSM network under different operating modes. Even when the patient has entered a building where GPS signal is invalid, the system can report the location and time of the last available GPS information that can be used as the clue for searching patients.
The database server, H-GIS, short message controller, and web service Server are implemented on four independent server systems. Only the web service server has an external IP address; the other servers are all located within a firewall to enhance the system security. As shown in Fig. 8, to overcome the problem
Fig. 9. User interfaces for (a) SMS mobile phone, (b) PDA + GPRS, (c) MMS mobile phone, and (d) notebook PC + wireless network.
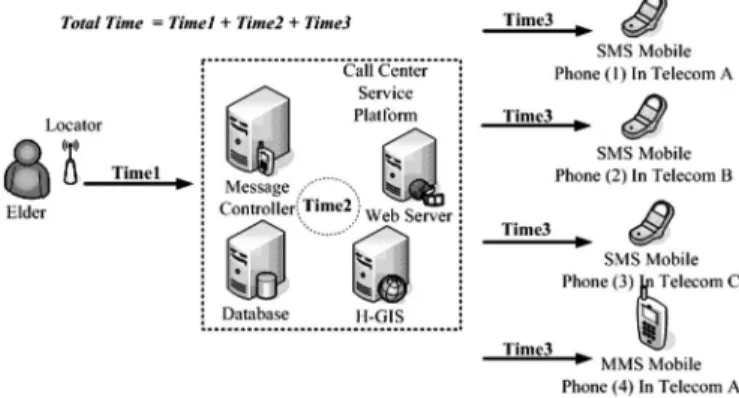
Fig. 10. Diagram to depict the experiment design of performance evaluation.
that GPS are usually limited by bad weather, landscapes, and buildings (e.g., indoor), our system will not only record the last valid GPS coordinates but also utilize GSM location to trace the location of the elder. When the GPS signal is invalid, the patient’s location information can be attained via the GSM-locating ser-vice provided by a local GSM network company. Though the precision is not as good as GPS, it can resolve the problem of not being able to locate the elder in bad weather conditions.
For the data display, our system provides a PC-based user interface (UI), PDA-based UI, MMS mode, and SMS mode to display data. When short message controller receives the latest GPS data from the elderly, H-GIS will immediately pro-duce two GIS images with different resolutions (480× 480 and 240× 240) used to display appropriate GIS on different devices. This also help lessen the loading of backend servers when mul-tiple users try to browse the data of a similar case at around the same time, the server does not need to produce GIS images re-peatedly since the images are produced once in advance. When users are connected to the system via PC or PDA, the system can determine the monitor resolution of the device by version of the browser and can provide appropriate image format to let the user get adaptive messages in different devices (Fig. 9).
As far as performance evaluation experiments were con-cerned, the system response time including the time needed for the location signal to be processed and transmitted from the patient to the servers (Time1), the data processing time of the servers (Time2), and the transmission time from the servers to the GSM users (Time3) were measured for users with mobile
TABLE I
RESULTS OFEXPERIMENTSFORPERFORMANCEANALYSIS
phones from three different service providers (top three in mar-ket share and with a total marmar-ket share above 75%) at the same time. As can be observed from Fig. 10, Time1 is mainly com-posed of locator processing time (GPS fetching, data encoding) and GSM short message transmission time, Time2 mainly con-sists of the time needed for server data inquiry and GIS image file production, and Time3 mainly consists of transmission time for the messages transmitted from servers to the users’ mobile phones. Four different models of the mobile phone were used in the experiment. Three of them were SMS mobile phones that could only receive text messages, and the other was an MMS mobile phone that could receive 15 kB of data including text messages and two image files (the elder’s photograph and an electronic map).
The experiments were performed on three different locations (a tableland, a train station, and a community with four 17-floor buildings with 300 households) and four different time slots (5:00–6:00A.M., 8:00–9:00A.M., 5:00–6:00 P.M., and 11:00– 12:00P.M.) to measure the transmission efficiency and location accuracy. Time1, Time2, and Time3 were each measured for twenty times to obtain the mean and standard deviation for each experiment. The results of the measurements in this experiment are shown in Table I. The average of Time1 is 22± 6.9 s (the rightmost column in Table I). Time1 is mainly affected by two factors. First, the terrain will affect the time the locator needs to fetch the effective GPS data. Second, the different traffic load of a telecom during different periods of time can also cause message transmission delay. The average of time around the train station is, thus, slightly higher than the other two loca-tions. Time2 mainly consists of the time the system needs to receive and process the message and the time taken to transmit the data to telecom short message dispatch server via network.
The overall average of Time2 is 5.4± 2 s. Time3 is the time needed for the mobile phone of family members to receive the geographical information of the elderly. Time3 depends on the telecom systems. The average values for three different tele-coms are 8.5± 3.9, 5.8 ± 1.3, and 6.5 ± 1.3, respectively. In the total of 320 instances of our experiment, the average of total time starting from the transmission of locator signal up to the reception of short message to family members is 34.3± 7.7 s. If the system transmits information to family members via MMS (phone4 in Fig. 10), the average transmission time of the MMS is 33.3± 3 s and the total time is about 26 s longer than the one transmitting SMS. As for the experiments for GIS accuracy, the average error of three different locations is about 8 m (11 m at the tableland, 7 m for the train station, and 7 m for the community). User questionnaires were taken after 11 healthy volunteers used our system. As for the size and weight of the locator, 81.9% (n = 9) of the users feel satisfied (n = 8) or very satisfied (n = 1). 72.7% of the users feel very satisfied (n = 1) or satisfied (n = 7) with the system stability. The dissatisfaction is mainly due to that the terrain and weather can easily affect the use of GPS. 72.7% of the users are satisfied (n = 6) or very satisfied (n = 2) with the system operation interface and the reason of not being satisfied is owing to the too short standby time of the locator. 63.6% of the users (n = 7) suggest that the standby time and size of the locator should be improved. The standby time should be prolonged to at least 48 h and the size of locator should be shrunk to a hand ring or integrated with a walking stick to be convenient for the wearing of the elderly. All of the users believe that the provision of location information would be very helpful for the search assistance of the elderly with dementia. 88.8% of the users are willing to use our system or recommend it to the others.
LIN et al.: WIRELESS HEALTH CARE SERVICE SYSTEM FOR ELDERLY WITH DEMENTIA 703
IV. CONCLUSION
The aging of the population and the consequent problems are major issues in the developed countries. The problem of dementia among the elderly will become even more serious as the average age of the population increases. In this paper, satellite positioning, wireless communication, and information processing are integrated to develop a wireless emergency health care system for the elderly persons with dementia in a real health care environment. Thanks to the development of a residence motion sensor and a body-attached rescue locator; our system can prevent patients from getting lost by providing four monitoring schemes consisting of indoor residence monitoring, outdoor activity area monitoring, emergency rescue scheme, and remote monitoring mode. For the data management, a TIP format is defined to clearly describe the detailed tracing condition of a stray event, and a service management platform consisting of web service server, database server, message controller, and H-GIS server is constructed to let family members and volunteer workers acquire the real-time location of the missing patient via different mobile devices. Analysis of system performance and reliability using different telecoms and different models of mobile phones reveals that the system can provide family members with the patient’s latest location information within 34 seconds. All short messages were received and processed by our system correctly.
Our future efforts will primarily focus on two aspects. One is the monitoring and analysis of elders’ indoor behavior, which will either help patients avoid danger or provide information to specialists who would evaluate the patients’ health conditions. The other is integration with a wireless network to enhance the coverage area and precision of positioning and reduce commu-nication costs via double networks. We believe that this research will result in better health care for elderly persons with dementia and reduce the burden of the caregivers at the same time.
REFERENCES
[1] A. Hofman, W. A. Rocca, C. Brayne, M. M. B. Breteler, M. Clarke, B. Cooper, J. R. M. Copeland, J. F. Dartigues, A. D. S. Droux, O. Hagnell, T. J. Herren, K. Engedal, C. Joker, J. Lindesay, A. Lobo, A. H. Mann, P. K. Molsa, K. Morgan, D. W. O’Connor, R. Sulkava, D. W. K. Kay, and L. Amaducci, “The prevalence of dementia in Europe: A collaborative study of 1980–1990 findings,” Int. J. Epidemiol., vol. 20, pp. 736–748, 1991.
[2] E. Kokmen, C. M. Beard, and K. P. Offord, “Prevalence of medically diagnosed dementia in a defined United States population: Rochester, Minnesota, January 1, 1975,” Neurology, vol. 39, pp. 773–776, 1989. [3] C. Brayne, C. Gill, and F. A. Huppert, “Incidence of clinically diagnosed
subtypes dementia in an elderly population: Cambridge project for later,”
Br. J. Psychiatry, vol. 167, pp. 255–262, 1995.
[4] D. L. Bachman, P. A. Wolf, and R. T. Lin, “Incidence of dementia and probable Alzheimer’s disease in a general population: The Framingham study,” Neurology, vol. 43, pp. 515–519, 1993.
[5] C. H. Kawas and R. Katzman, “Epidemiology of dementia and Alzheimer’s disease,” in Alzheimer’s Disease, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 1999, pp. 95–116.
[6] C. K. Liu, R. T. Lin, Y. F. Chen, C. T. Tai, Y. Y. Yen, and S. L. Howng, “Prevalence of dementia in an urban area in Taiwan,” J. Formosan Med.
Assoc., vol. 95, pp. 762–768, 1996.
[7] H. C. Liu, J. L. Fuh, and S. J. Wang, “Prevalence and subtypes of dementia in a rural Chinese population,” Alzheimer Dis. Assoc. Disord., vol. 12, pp. 127–134, 1998.
[8] P. K. Yip, Y. I. Shyu, S. I. Liu, J. Y. Lee, C. F. Chou, and R. C. Chen, “An epidemiological survey of dementia among elderly in an urban district of Taipei,” Acta Neurologyica Sinica, vol. 1, pp. 347–354, 1992.
[9] H. Jimison, M. Pavel, J. McKanna, and J. Pavel, “Unobtrusive monitoring of computer interactions to detect cognitive status in elders,” IEEE Trans.
Inf. Technol. Biomed., vol. 8, no. 3, pp. 248–252, Sep. 2004.
[10] T. Adlam, R. Faulkner, R. Orpwood, K. Jones, J. Macijauskiene, and A. Budraitiene, “The installation and support of internationally distributed equipment for people with dementia,” IEEE Trans. Inf. Technol. Biomed., vol. 8, no. 3, pp. 253–257, Sep. 2004.
[11] K. Lorincz, D. J. Malan, T. R. F. Fulford-Jones, A. Nawoj, A. Clavel, V. Shnayder, G. Mainland, and M. Welsh, “Sensor networks for emergency response: Challenges and opportunities,” Pervasive Comput., vol. 3, no. 4, pp. 16–23, Oct.–Dec. 2004.
[12] K. J. Liszka, M. A. Mackin, M. J. Lichter, and D. W. York, “Keeping a Beat on then Heart,” Pervasive Comput., vol. 3, no. 4, pp. 42–49, Oct.–Dec. 2004.
[13] E. Dishman, “Inventing wellness system for aging in place,” Computer, vol. 37, no. 5, pp. 34–41, May 2004.
[14] S. Fischer, T. E. Stewart, S. Mehta, R. Wax, and S. E. Lapinsky, “Handheld computing in medicine,” J. Amer. Med. Inf. Assoc., vol. 10, no. 2, pp. 139– 149, Mar.–Apr. 2003.
[15] H. H. Asada, P. Shaltis, A. Reisner, S. Rhee, and R. C. Hutchinson, “Mobile monitoring with wearable photoplethysmographic biosensors,”
IEEE Eng. Med. Biol. Mag., vol. 22, no. 3, pp. 28–40, May–Jun. 2003.
[16] M. D. Rodriguez, J. Favela, E. A. Martinez, and M. A. Munoz, “Location-aware access to hospital information and services,” IEEE Trans. Inf.
Technol. Biomed., vol. 8, no. 4, pp. 448–455, Dec. 2004.
[17] M. Perry, A. Dowdall, L. Lines, and K. Hone, “Multimodal and ubiquitous computing systems: Supporting independent-living older users,” IEEE
Trans. Inf. Technol. Biomed., vol. 8, no. 3, pp. 258–270, Sep. 2004.
[18] A. Mihailidis, B. Carmichael, and J. Boger, “The use of computer vision in an intelligent environment to support aging in place, safety, and inde-pendence in the home,” IEEE Trans. Inf. Technol. Biomed., vol. 8, no. 3, pp. 238–247, Sep. 2004.
[19] J. Favela, M. Rodriguez, A. Preciado, and V. M. Gonzalez, “Integrating context-aware public displays into a mobile hospital information system,”
IEEE Trans. Inf. Technol. Biomed., vol. 8, no. 3, pp. 279–286, Sep. 2004.
[20] Y.-H. Lin, I.-C. Jan, P. C.-I. Ko, Y.-Y. Chen, J.-M. Wong, and G.-J. Jan, “A wireless PDA-based physiological monitoring system for patient trans-port,” IEEE Trans. Inf. Technol. Biomed., vol. 8, no. 4, pp. 439–447, Dec. 2004.
[21] U. Anliker, J. A. Ward, P. Lukowicz, G. Troster, F. Dolveck, M. Baer, F. Keita, E. B. Schenker, F. Catarsi, L. Coluccini, A. Belardinelli, D. Shklarski, M. Alon, E. Hirt, R. Schmid, and M. Vuskovic, “AMON: A wearable multiparameter medical monitoring and alert system,” IEEE
Trans. Inf. Technol. Biomed., vol. 8, no. 4, pp. 415–427, Dec. 2004.
[22] G. Derekenaris, J. Garofalakis, C. Makris, J. Prentzas, S. Sioutas, and A. Tsakalidis, “Integrating GIS, GPS and GSM technologies for the effec-tive management of ambulances,” Comput., Environ. Urban Syst., vol. 25, pp. 267–278, 2001.
[23] M. N. K. Boulos, A. V. Roudsari, and E. R. Carson, “Health geomatics: An enabling suite of technologies in health and healthcare,” J. Biomed.
Inf., vol. 34, pp. 195–219, 2001.
[24] R. Elmasri and S. B. Navathe, Fundamentals of Database Systems, 4th ed. Reading, MA: Addison-Wesley, 2003, ch. 3, ch. 4.
[25] A. Silberschatz, H. F. Korth, and S. Sudarshan, Database System Concepts, 4th ed. New York: McGraw-Hill, 2002, ch. 2–3.
[26] R. Want, “Enabling ubiquitous sensing with RFID,” Computer, vol. 7, no. 4, pp. 84–86, Apr. 2004.
[27] L. M. Ni, Y. Liu, Y. C. Lau, and A. P. Patil, “LANDMARC: Indoor location sensing using active RFID,” in Proc. IEEE PerCom’03, Mar. 23–26, 2003, pp. 407–415.
Chung-Chih Lin (S’95–M’00) received the Ph.D.
degree in electrical engineering from National Taiwan University, Taipei, Taiwan, R.O.C., in 1999.
Since 2003, he has been an Assistant Professor in the Department of Computer Science and In-formation Engineering, Chang Gung University, Tao-Yuan, Taiwan, R.O.C. His research interests in-clude medical informatics, data mining, and man– machine interface for the elderly.
Ming-Jang Chiu received the B.Med. degree in
medicine and the Ph.D. degree in electrical engineer-ing from National Taiwan University, Taipei, Taiwan, R.O.C., in 1984 and 2000, respectively.
In 1989, he became a board certified Neurologist in Taiwan, R.O.C. He is currently an Attending Neu-rologist with National Taiwan University Hospital, Taipei, specializing in the diagnosis and treatment of patients with dementia. His research interests include cognitive neuroscience, sleep medicine, and clinical neurophysiology.
Dr. Chiu has been the Standing Board Member of the Taiwan Alzheimer’s Disease Association and the Secretary General of the Taiwan Society of Clinical Neurophysiology, both since 2004.
Chun-Chieh Hsiao was born in 1962. He received
the M.S. degree in electrical and computer engineer-ing from the State University of New York, Buffalo, in 1990.
During 1991–1993, he was with the Computer and Communication Laboratory, Industrial Technology Research Institute, to focus on the research and de-velopment of advanced computer graphics systems. From 1993 to 2003, he was with the Department of Electrical Engineering, Lunghwa University of Science and Technology (LHU), Tao-Yuan, Taiwan, R.O.C. Since 2003, he has been with the Department of Computer Information and Network Engineering, LHU. His research interests include telecare and mobile-care systems, wireless sensor networks for biomedical applications, and advanced computer systems.
Ren-Guey Lee (M’06) was born in 1965. He
re-ceived the M.S. degree from the Department of Elec-trical Engineering, National Chen Kung University, Tainan, Taiwan, R.O.C., in 1989, and the Ph.D. de-gree from the Department of Electrical Engineering, National Taiwan University, Taipei, Taiwan, R.O.C., in 2000.
Since 2002, he has been with the Department of Electronic Engineering, National Taipei University of Science and Technology, Taipei, where he is cur-rently an Associate Professor. His research interests include medical informatics, telecare and mobile-care systems, and wireless sensor networks for biomedical applications.
Yuh-Show Tsai (S’82–M’85) received the B.S. and
M.S. degrees from Chung Yuan Christian Univer-sity, Chung Li, Taiwan, R.O.C., in 1983 and 1985, respectively, and the Ph.D. degree from Vanderbilt University, Nashville, TN, in 1998, all in biomedical engineering.
Since 1989, he has been a faculty member at Chung Yuan Christian University, where he is cur-rently an Associate Professor in the Department of Biomedical Engineering and the Department of Bio-science Technology. His research interests include medical informatics, bioinformatics, and Bio-SOC design and applications.
Dr. Tsai is a member of the Biomedical Engineering Society, Taiwan, R.O.C., and the IEEE Engineering in Medicine and Biology Society. He is the Secretary of the Medical Image Standard Association, Taiwan, R.O.C.