Benzodiazepine Use Possibly Increases Cancer Risk:A Population-Based Retrospective Cohort Study in Taiwan
6
0
0
全文
(2) Clinical Points. Cohort Study of Benzodiazepine Use and Cancer Risk. ■■ This population-based study has shed light on a. possible relationship between benzodiazepine use and an increased cancer risk.. ■■ Clinicians should consider the potentially increased. cancer risk of benzodiazepine use in clinical practice.. included gender, birth date, occupation, and residential area. Diagnoses were coded according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Study Subjects Subjects who were prescribed a benzodiazepine for at least 2 months during the study period (mean prescription frequency was 26.7 times [standard deviation (SD) = 34.3 times]) were identified (N = 59,647) and defined as the benzodiazepine cohort (mean age = 47.9 years, SD = 17.3 years). The initial benzodiazepine treatment date was defined as the index date. We excluded patients with a history of malignant cancer (ICD-9-CM codes 140–208) diagnosed before the index date or with missing information about age or sex. A nonbenzodiazepine control cohort (mean age = 46.4 years, SD = 17.8 years) was also established by randomly frequency-matching age, sex, and index year of the benzodiazepine cases to subjects from the insured population without a history of cancer or benzodiazepine treatment. Each study subject was followed until a diagnosis of cancer was made (ICD-9-CM) or until the time the subject was censored for loss to follow-up, death, or termination of insurance—or to the end of 2009. We then subclassified the benzodiazepine cohort into 4 groups as follows for further analysis according to their disease status: (1) those with sleep disorders (ICD-9-CM codes 780.5 and 307.4 [except for sleep apnea syndrome: codes 780.51, 780.53, and 780.57]); (2) those with anxiety (ICD-9-CM codes 300.0, 300.2, 300.3, 308.3, and 309.81); (3) those with both sleep disorders and anxiety; and (4) those with neither. Statistical Analysis First, we compared the distribution of sociodemographic factors between the benzodiazepine cohort and the comparison group not exposed to benzodiazepines using χ2 tests. Then, we calculated the sex-specific and age-specific incidence density rates of cancer with person-years in each cohort. The incidence rate ratio (IRR) of each variable was estimated by Poisson regression. The Cox proportional hazard regression analysis was used to measure the effect of benzodiazepines on the time to cancer diagnosis. The hazard ratios (HRs) are presented with 99.6% or 99.5% confidence intervals, with the model. Table 1. Comparison of Baseline Characteristics Between the Groups With and Without Benzodiazepine Use Group Without Benzodiazepine Use, N = 59,592 n %. Group With Benzodiazepine Use, N = 59,647 n %. P Characteristic Valuea Sex Women 31,286 52.5 31,341 52.5 Men 28,306 47.5 28,306 47.5 Age, y < 20 2,921 4.9 2,920 4.9 20–39 17,237 28.9 17,240 28.9 40–49 13,381 22.5 13,379 22.4 50–59 10,646 17.9 10,646 17.9 60–69 8,248 13.8 8,248 13.8 ≥ 70 7,159 12.0 7,214 12.1 b < .0001 Urbanization level 1 19,075 32.0 18,674 31.3 2 17,359 29.1 17,001 28.5 3 10,774 18.1 10,297 17.3 4 7,167 12.0 7,918 13.3 5 5,215 8.8 5,757 9.7 aχ2 test. No P values are given for sex and age since the selection of subjects with no benzodiazepine exposure was constrained by the distribution of sex and age in the subjects with benzodiazepine use. bUrbanization level: 1 indicates the highest level of urbanization, and 5 indicates the lowest. The townships within which subjects registered for insurance were grouped into 5 levels of urbanization that were based on a score calculated by incorporating variables indicating population density (people/km2), population ratio of different educational levels, population ratio of the elderly, population ratio of agricultural workers, and number of physicians per 100,000 people.16. controlling for sociodemographic factors. The Bonferroni adjustment was used in multiple comparisons. All analyses were performed using SAS statistical software, Version 9.1 (SAS Institute Inc, Cary, North Carolina), and the significance level was set at .05. RESULTS The frequency matching by sex and age worked well, as displayed in Table 1. Only slight differences are observed between the 2 cohorts with respect to urbanization, but the differences are statistically significant due to the large sample size and statistical power. The incidence density and crude rate ratio of cancer by age and sex is shown in Table 2. Overall, compared with the group not exposed to benzodiazepines, subjects with benzodiazepine use were 1.29 times more likely to develop cancer (a rate of 5.08 vs 3.95 per 1,000 person-years), with the highest IRR appearing in the group aged 20–39 years (IRR = 1.95; 95% CI, 1.50–2.54). The sex-specific incidence rate of cancer shows that the benzodiazepine cohort had a higher IRR than the group not exposed to benzodiazepines for both women (IRR = 1.19; 95% CI, 1.07–1.32) and men (IRR = 1.37; 95% CI, 1.25–1.49). The IRR among men aged 20–39 years in the benzodiazepine cohort was 2.81 times higher (95% CI, 1.81–4.35) than among subjects in the same age group without benzodiazepine exposure (Table 2). Figure 1 exhibits the Kaplan-Meier curves of freedom from cancer in the 2 cohorts—patients with versus without benzodiazepine use. There was a statistically significant. © COPYRIGHT 2012 PHYSICIANS POSTGRADUATE PRESS, INC. © COPYRIGHT 2012 PHYSICIANS POSTGRADUATE RESS2012 , INC. J Clin Psychiatry 73:4,PApril e556.
(3) Cohort Study of Benzodiazepine Use and Cancer Risk. Table 2. Comparisons of Incidence Density of Cancer Between the Groups With (N = 59,647) and Without (N = 59,592) Benzodiazepine Use by Age and Sex Group Without Benzodiazepine Use Group With Benzodiazepine Use Variable Cancer Cases, N Person-Years Ratea Cancer Cases, N Person-Years All subjects, age, y < 20 3 19,545 0.15 4 19,683 20–39 82 112,487 0.73 167 117,539 40–49 201 90,663 2.22 301 92,147 50–59 281 69,559 4.04 447 70,073 60–69 409 53,396 7.66 511 55,011 ≥ 70 532 36,336 14.60 582 41,500 Overall 1,508 381,985 3.95 2,012 395,954 Women, age, y < 20 1 11,224 0.09 1 11,294 20–39 55 62,590 0.88 89 66,160 40–49 114 51,799 2.20 141 52,881 50–59 135 37,989 3.55 194 38,601 60–69 161 27,409 5.87 184 28,208 ≥ 70 177 16,418 10.80 186 19,088 Overall 643 207,429 3.10 795 216,234 Men, age, y < 20 2 8,321 0.24 3 8,388 20–39 27 49,897 0.54 78 51,379 40–49 87 38,863 2.24 160 39,265 50–59 146 31,570 4.62 253 31,472 60–69 248 25,987 9.54 327 26,803 ≥ 70 355 19,918 17.80 396 22,412 Overall 865 174,556 4.96 1,217 179,720 aPer 1,000 person-years. bCompared to group without benzodiazepine use. *P < .05, ***P < .0001. Abbreviation: IRR = incidence rate ratio.. DISCUSSION The results of the adjusted analysis from this population-based cohort study indicated that benzodiazepine use significantly increased the risk of cancer overall and, specifically, of brain cancer in men, liver cancer, bladder/kidney. IRRb. 95% CI. 0.20 1.42 3.27 6.38 9.29 14.00 5.08. 1.32 1.95 1.47 1.58 1.21 0.96 1.29. 0.30–5.92 1.50–2.54*** 1.23–1.76*** 1.36–1.83*** 1.06–1.38* 0.85–1.08 1.20–1.38***. 0.09 1.35 2.67 5.03 6.52 9.74 3.68. 0.99 1.53 1.21 1.41 1.11 0.90 1.19. 0.06–15.9 1.09–2.14* 0.95–1.55 1.14–1.76* 0.90–1.37 0.74–1.11 1.07–1.32*. 0.36 1.52 4.07 8.04 12.20 17.70 6.77. 1.49 2.81 1.82 1.74 1.28 0.99 1.37. 0.25–8.90 1.81–4.35*** 1.40–2.36*** 1.42–2.13*** 1.08–1.51* 0.86–1.14 1.25–1.49***. Figure 1. Kaplan-Meier Curves of Freedom From Cancer in the Groups With (N = 59,647) and Without (N = 59,592) Benzodiazepine Usea 1.00. 0.98 Probability. difference in cancer occurrence between the patients with benzodiazepine use and those without benzodiazepine use (log-rank test, P < .0001). The further analyses on specific cancer types are presented in Table 3. We observed that subjects with benzodiazepine use showed an increased risk of bladder and kidney cancer (HR = 1.76; 99.6% CI, 1.16–2.67), prostate cancer (HR = 1.72; 99.6% CI, 1.10–2.70), and liver cancer (HR = 1.45; 99.6% CI, 1.10–1.90). In addition, men with benzodiazepine use showed an increased risk of brain cancer (HR = 4.90; 99.5% CI, 1.05–22.8). Furthermore, the subclassification analysis separated the benzodiazepine cohort on the basis of whether or not the patients were being treated for sleep disorders, anxiety, both, or neither. The results show that the benzodiazepine cohort without sleep disorders or anxiety had a 1.35-times greater risk (95% CI, 1.24–1.46) of cancer than the group with no benzodiazepine exposure. Additionally, those in the benzodiazepine cohort with sleep disorders alone had a 1.21times greater risk (95% CI, 1.10–1.34) of cancer (Table 4). In contrast, the female subjects in the benzodiazepine cohort with both sleep disorders and anxiety had a decreased risk of cancer (HR = 0.80; 95% CI, 0.66–0.97).. Ratea. 0.96. 0.94. No benzodiazepine use Benzodiazepine use. 0.92 0. 2. 4. 6. 8. 10. Time, y a. Log-rank P < .0001.. cancer, and prostate cancer. In contrast, women with benzodiazepine use had a significantly lower risk of developing cervical cancer. The findings are surprising because they contradict previously held ideas. It is important to share these findings as they may have significant impact. Since 1982, cancer has been the leading cause of death among the general population in Taiwan. The age-adjusted incidence rate has increased steadily and reached 270 new cases per 100,000 people in 2007.17 This trend is different from the Surveillance, Epidemiology, and End Results (SEER) data, which show that overall cancer incidence rates. © JCClin OPYRIGHT 2012 HYSICIANS . Psychiatry 73:4,PApril 2012 POSTGRADUATE PRESS, INC. © COPYRIGHT 2012 PHYSICIANS POSTGRADUATE PRESS, INC e557.
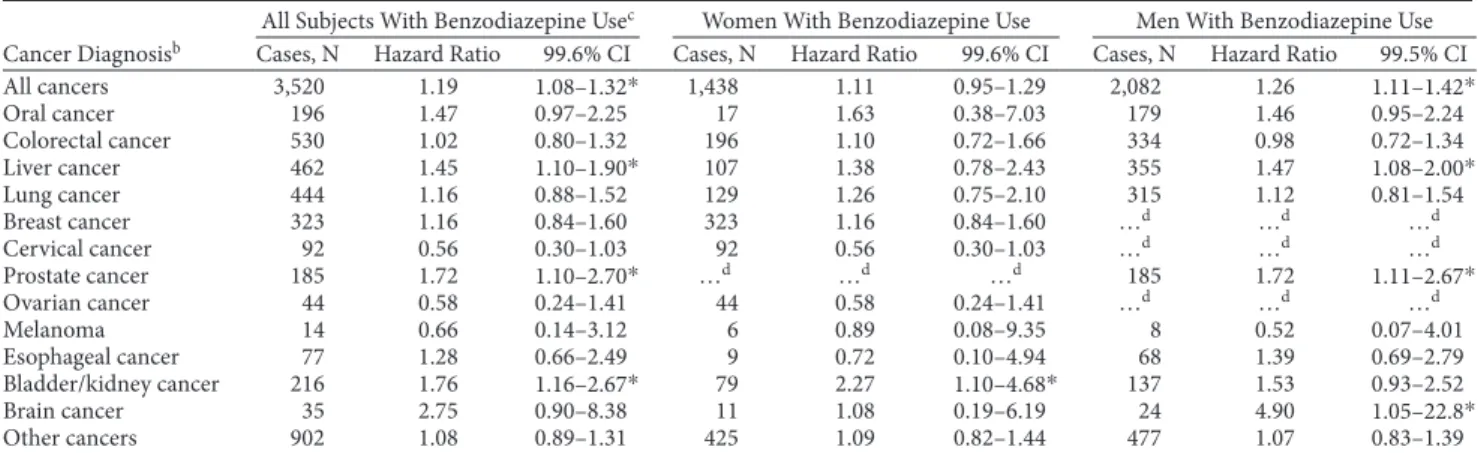
(4) Cohort Study of Benzodiazepine Use and Cancer Risk. Table 3. Hazard Ratios and Confidence Intervals of Cancer Associated With Benzodiazepine Use in Cox Regression Analysis in Different Cancersa All Subjects With Benzodiazepine Usec Women With Benzodiazepine Use Men With Benzodiazepine Use Cancer Diagnosisb Cases, N Hazard Ratio 99.6% CI Cases, N Hazard Ratio 99.6% CI Cases, N Hazard Ratio 99.5% CI All cancers 3,520 1.19 1,438 1.11 0.95–1.29 2,082 1.26 1.08–1.32* 1.11–1.42* Oral cancer 196 1.47 0.97–2.25 17 1.63 0.38–7.03 179 1.46 0.95–2.24 Colorectal cancer 530 1.02 0.80–1.32 196 1.10 0.72–1.66 334 0.98 0.72–1.34 Liver cancer 462 1.45 107 1.38 0.78–2.43 355 1.47 1.10–1.90* 1.08–2.00* Lung cancer 444 1.16 0.88–1.52 129 1.26 0.75–2.10 315 1.12 0.81–1.54 …d …d Breast cancer 323 1.16 0.84–1.60 323 1.16 0.84–1.60 …d Cervical cancer 92 0.56 0.30–1.03 92 0.56 0.30–1.03 …d …d …d Prostate cancer 185 1.72 …d …d …d 185 1.72 1.10–2.70* 1.11–2.67* Ovarian cancer 44 0.58 0.24–1.41 44 0.58 0.24–1.41 …d …d …d Melanoma 14 0.66 0.14–3.12 6 0.89 0.08–9.35 8 0.52 0.07–4.01 Esophageal cancer 77 1.28 0.66–2.49 9 0.72 0.10–4.94 68 1.39 0.69–2.79 Bladder/kidney cancer 216 1.76 79 2.27 137 1.53 0.93–2.52 1.16–2.67* 1.10–4.68* Brain cancer 35 2.75 0.90–8.38 11 1.08 0.19–6.19 24 4.90 1.05–22.8* Other cancers 902 1.08 0.89–1.31 425 1.09 0.82–1.44 477 1.07 0.83–1.39 aAdjusted for age and urbanization level. bICD-9-CM diagnosis codes: oral cancer, 140.xx, 141.xx, 143.xx–146.xx, and 148.xx–149.xx; esophageal cancer, 150.xx; colorectal cancer, 153.xx and 154.xx; liver cancer, 155.xx; lung cancer, 162.xx; breast cancer, 174.xx; melanoma, 172.xx; cervical cancer, 180.xx; ovarian cancer, 183.xx; prostate cancer, 185.xx; bladder and kidney cancer, 188.xx and 189.xx; brain cancer, 191.xx. cAdjusted for sex, age, and urbanization level. dNot applicable. *Significant under Bonferroni correction: all P < .005.. Table 4. Cox Proportional Hazard Regression Analysis for the Risk of Benzodiazepine-Associated Cancer With Interaction of Comorbiditya Cancer Cases, Hazard n Ratio. Group N 95% CI All subjectsb No benzodiazepine use 59,592 1,508 1.00 Reference Benzodiazepine use 59,647 Sleep disorder 15,444 577 1.21 1.10–1.34*** Anxiety 8,898 231 1.04 0.91–1.20 Sleep disorder and anxiety 11,552 272 0.91 0.80–1.04 Neither 23,753 932 1.35 1.24–1.46*** Women No benzodiazepine use 31,286 643 1.00 Reference Benzodiazepine use 31,341 Sleep disorder 8,309 231 1.14 0.98–1.32) Anxiety 4,797 108 1.05 0.86–1.29 Sleep disorder and anxiety 6,975 120 0.80 0.66–0.97** Neither 11,260 336 1.29 1.13–1.48*** Men No benzodiazepine use 28,306 865 1.00 Reference Benzodiazepine use 28,306 Sleep disorder 7,135 346 1.27 1.12–1.44** Anxiety 4,101 123 1.04 0.86–1.26 Sleep disorder and anxiety 4,577 152 1.02 0.85–1.21 Neither 12,493 596 1.39 1.25–1.54*** a Adjusted for age and urbanization level. bAdjusted for sex, age, and urbanization level. **P < .001, ***P < .0001.. in the United States for all racial/ethnic groups combined decreased by 0.7% per year between 1999 and 2006.18 As this issue continues to be a challenge for public health in Taiwan, it has come to the attention of the government, thus resulting in population-based investigations regarding cancer-preventive epidemiology. As the Taiwanese National Health Insurance program provides comprehensive coverage, the National Health Insurance Research Database contains ambulatory service records, hospital service records, and prescription claim data. The database allows us to appropriately select matched subjects representative of. the underlying population. We recently used this database to evaluate the risk of malignancy for patients with end-stage renal disease and published the article indicating some positive findings.19 This present study used a similar design to determine the effect of benzodiazepine use on the risk of cancer development. To our knowledge, this current study is the first populationbased investigation of these 59,647 Taiwanese persons with benzodiazepine use. In order to create a comparison group, we used age, sex, and index calendar year to randomly frequency-match each individual with benzodiazepine use to a person from the cohort that had no benzodiazepine use. With regard to the cancer risk analysis, Horrobin and Trosko20 discussed the possible effect of diazepam on cancer development and growth in 1982 and suggested that epidemiologic studies in humans were urgently required. Rosenberg et al12 conducted a large case-control surveillance study in 1995 and investigated the relationship between benzodiazepine use and the risk of selected cancers. These authors suggested that benzodiazepines do not influence the risk of cancer as a whole, but they mentioned that the possibility of selection bias could not be excluded definitively. We were surprised to find in our results that individuals with benzodiazepine use had a significantly higher overall risk of cancer. However, this finding is consistent with a previous report,21 which showed that the adjusted hazard of sleeping-pill usage was a statistically significantly elevated risk of cancer. In regard to risks for individual cancers, our data showed that the risks for developing liver, prostate, and bladder/ kidney cancers among patients with benzodiazepine use were significantly higher. During the literature review, we found scarce data discussing the relationship between these cancers and benzodiazepine use. For liver cancer, data from earlier animal studies6,7 showed an interaction between benzodiazepines and hepatocarcinogenesis, although no human data are available to support the interaction. We also found that. © COPYRIGHT 2012 PHYSICIANS POSTGRADUATE PRESS, INC. © COPYRIGHT 2012 PHYSICIANS POSTGRADUATE RESS2012 , INC. J Clin Psychiatry 73:4,PApril e558.
(5) Cohort Study of Benzodiazepine Use and Cancer Risk. patients with benzodiazepine use had a marginally significantly higher risk for oral cancer. Both oral and liver cancers are related to viral infections, and patients with immunocompromised status are more vulnerable to viral infections. Normally, individuals with benzodiazepine use have more psychological problems. Psychological parameters may alter immune function, and it has long been hypothesized that, through this pathway, psychosocial factors may affect the incidence of cancer.22 The growing evidence implicates a role for the immune system as a link between the central nervous system and disease processes.23 Various studies in this field have proven that external factors such as stress, depression, or lack of social support have significant influence on components of the immune system that, in turn, influence the onset as well as the course of cancer.24 Regarding bladder/kidney cancer, Kripke11 also pointed out that bladder cancer is associated with an increased mortality caused by hypnotic drug use. The mechanism is still being studied, but the pharmacologic action and excretion of benzodiazepines may play a role. We analyzed earlier the relationship between anxiety and cancer and found that patients with anxiety disorders had a higher risk of prostate cancer— but a lower risk of cervical cancer (J.A.L., L.M.S., K.P.S., et al; unpublished data, 2011). One possible explanation is that the intrinsic personality of patients with anxiety disorders causes them to have more frequent cancer screening tests, and, therefore, more diagnoses of prostate cancer and carcinoma in situ cervical cancer can be expected. The current study also reflects similar findings, showing a significantly higher risk for prostate cancer in men with benzodiazepine use—but a marginally significantly lower risk for cervical cancer in women with benzodiazepine use. These findings imply a possible pathway: anxiety→benzodiazepine use→cancer. We are concerned about whether the increased cancer risk is actually from the underlying psychological problems instead of the benzodiazepine; however, Table 4 indicates that, among individuals with benzodiazepine use, those without anxiety or sleep disorders still had a higher risk of developing cancer. One of the strengths of this study is the population-based design with its inherent representativeness. However, the study has some limitations. First, detailed information such as smoking habits, alcohol consumption, body mass index, socioeconomic status, and family history of cancer were not available from the National Health Insurance Research Database; all of these variables are major risk factors for multiple cancers and could plausibly be associated with benzodiazepines. However, since the National Health Insurance Research Database covers almost the whole population of Taiwan and the reimbursement policy is universally the same, it is unlikely that these factors would affect the prescription of benzodiazepines. Second, the organ-specific pattern of cancer occurrence does not appear to correspond to any biological hypothesis of benzodiazepine action. We think it most likely that our findings in part reflect a “healthy non-user effect” (ie, those with healthier lifestyles and behaviors may be less likely to have indications for benzodiazepines or may. be more likely to address such problems with nonpharmacologic approaches). Third, the evidence derived from a cohort study is generally of lower quality than that derived from randomized control trials because a cohort study design is subject to many biases related to confounding adjustment. Despite our meticulous study design with adequate control of confounding factors, a key limitation is that bias could still remain if there are unmeasured or unknown confounders. Fourth, the diagnoses in the National Health Insurance claims primarily serve the purpose of administrative billing and do not undergo verification for scientific purposes. We were not able to contact the patients directly about their use of benzodiazepines because of the anonymity provided by their identification numbers. Prescriptions for these drugs before 1996 would not have been captured in our analysis. This time point cutoff could have caused underestimation of the cumulative dosage and may have weakened the observed association. However, the data for the prescription of benzodiazepines and for cancer diagnoses were very reliable. In conclusion, this population-based retrospective cohort study unexpectedly found a significant increase in overall cancer risk as well as the risk of some individual cancers in individuals with benzodiazepine use. These findings contradict our previous thinking, and the reasons for these results are still unclear. Further large, unbiased population-based studies and randomized control trials to investigate the relative cancer risk between different benzodiazepines and specific types of cancer are needed to support our findings before any confirmatory conclusions can be made. Drug names: diazepam (Diastat, Valium, and others). Author affiliations: Department of Nuclear Medicine and PET Center (Dr Kao), Department of General Psychiatry and Mind-Body Interface Laboratory (Dr Su), Management Office for Health Data (Mss Chang and Muo and Dr Sung), and Department of Radiation Oncology (Dr Liang), China Medical University Hospital, Taichung, Taiwan; Institute of Clinical Medicine Science and School of Medicine, College of Medicine (Drs Kao, Su, and Liang), Institute of Environmental Health, College of Public Health (Mss Chang and Muo and Dr Sung), and the PhD Program for Cancer Biology and Drug Discovery (Ms Chang), China Medical University, Taichung, Taiwan; Department of Radiation Oncology, Zuoying Armed Forces General Hospital, Kaohsiung, Taiwan (Dr Sun); and Institute of Biomedical Sciences, Academia Sinica, Taipei, Taiwan (Ms Chang). Author contributions: Drs Kao and Sun contributed equally to this work. Potential conflicts of interest: Drs Kao, Sun, Su, Sung, and Liang and Mss Chang and Muo declare that there were no actual or potential conflicts of interest relative to the subject of this study. Funding/support: Supported by study projects (DMR-100-076 and DMR-100-077) at China Medical University Hospital, Taichung, Taiwan, and by the Taiwan Department of Health Clinical Trial and Research Center of Excellence (DOH101-TD-B-111-004) and the Taiwan Department of Health Cancer Research Center of Excellence (DOH101-TD-C-111-005).. REFERENCES 1. Madhusoodanan S, Bogunovic OJ. Safety of benzodiazepines in the geriatric population. Expert Opin Drug Saf. 2004;3(5):485–493. doi:10.57/438 PubMed 2. Hogan DB, Maxwell CJ, Fung TS, et al; Canadian Study of Health and Aging. Prevalence and potential consequences of benzodiazepine use in senior citizens: results from the Canadian Study of Health and Aging. Can J Clin Pharmacol. 2003;10(2):72–77.PubMed 3. Zandstra SM, Furer JW, van de Lisdonk EH, et al. Different study criteria affect the prevalence of benzodiazepine use. Soc Psychiatry Psychiatr Epidemiol. 2002;37(3):139–144. doi:10.7/s2 6PubMed. © JCClin OPYRIGHT 2012 HYSICIANS . Psychiatry 73:4,PApril 2012 POSTGRADUATE PRESS, INC. © COPYRIGHT 2012 PHYSICIANS POSTGRADUATE PRESS, INC e559.
(6) Cohort Study of Benzodiazepine Use and Cancer Risk 4. Alvarenga JM, Loyola Filho AI, Firmo JO, et al. Prevalence and sociodemographic characteristics associated with benzodiazepines use among community dwelling older adults: the Bambuí Health and Aging Study (BHAS). Rev Bras Psiquiatr. 2008;30(1):7–11. doi:10.59/S6-420 PubMed 5. Cheng JS, Huang WF, Lin KM, et al. Characteristics associated with benzodiazepine usage in elderly outpatients in Taiwan. Int J Geriatr Psychiatry. 2008;23(6):618–624. doi:10.2/gps95PubMed 6. Diwan BA, Rice JM, Ward JM. Tumor-promoting activity of benzodiazepine tranquilizers, diazepam and oxazepam, in mouse liver. Carcinogenesis. 1986;7(5):789–794. doi:10.93/carn758PubMed 7. Préat V, de Gerlache J, Lans M, et al. Promoting effect of oxazepam in rat hepatocarcinogenesis. Carcinogenesis. 1987;8(1):97–100. doi:10.93/carn87PubMed 8. Karmali RA, Volkman A, Muse P, et al. The influence of diazepam administration in rats bearing the R3230AC mammary carcinoma. Prostaglandins Med. 1979;3(3):193–198. doi:10.6/-43(79)10PubMed 9. World Health Organization/International Agency for Research on Cancer (IARC) Working Group on the Evaluation of Carcinogenic Risks to Humans. Diazepam. IARC Monogr Eval Carcinog Risks Hum. 1996;66: 37–96.PubMed 10. Kripke DF. Risks of chronic hypnotic use. National Library of Medicine Bookshelf ID: NBK6630. http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi? book=eurekah&part=A28844. Verified on January 11, 2012. 11. Kripke DF. Evidence that new hypnotics cause cancer (draft 2). eScholarship, Department of Psychiatry, University of California San Diego. Updated March 17, 2008. http://escholarship.org/uc/ item/12r2f32g. Verified on January 11, 2012. 12. Rosenberg L, Palmer JR, Zauber AG, et al. Relation of benzodiazepine use to the risk of selected cancers: breast, large bowel, malignant melanoma, lung, endometrium, ovary, non-Hodgkin’s lymphoma, testis, Hodgkin’s disease, thyroid, and liver. Am J Epidemiol. 1995;141(12): 1153–1160.PubMed 13. Halapy E, Kreiger N, Cotterchio M, et al. Benzodiazepines and risk for. breast cancer. Ann Epidemiol. 2006;16(8):632–636. doi:10.6/janepm251.04PubMed 14. Harlow BL, Cramer DW. Self-reported use of antidepressants or benzodiazepine tranquilizers and risk of epithelial ovarian cancer: evidence from two combined case-control studies (Massachusetts, United States). Cancer Causes Control. 1995;6(2):130–134. doi:10.7/BF523PubMed 15. Lu JF, Hsiao WC. Does universal health insurance make health care unaffordable? Lessons from Taiwan. Health Aff (Millwood). 2003;22(3):77–88. doi:10.37/hltaf2PubMed 16. Liu CY, Hung YT, Chuang YL, et al. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Manag. 2006;14:1–22. 17. Taiwan Department of Health/National Public Health Association. Taiwan Cancer Registry: Cancer Statistics. http://tcr.cph.ntu.edu.tw/ main.php?Page=N2. Verified on January 11, 2012. 18. Edwards BK, Ward E, Kohler BA, et al. Annual report to the nation on the status of cancer, 1975–2006, featuring colorectal cancer trends and impact of interventions (risk factors, screening, and treatment) to reduce future rates. Cancer. 2010;116(3):544–573. doi:10.2/cnr476PubMed 19. Liang JA, Sun LM, Yeh JJ, et al. The association between malignancy and end-stage renal disease in Taiwan. Jpn J Clin Oncol. 2011;41(6):752–757. doi:10.93/jchyr5PubMed 20. Horrobin DF, Trosko JE. The possible effect of diazepam on cancer development and growth. Med Hypotheses. 1981;7(1):115–125. doi:10.6/3-987()2XPubMed 21. Kripke DF, Marler MR. Specific causes of mortality associated with prescription sleeping pill usage [abstract]. Sleep Res Online. 1999;2:144. 22. Schwarz S, Messerschmidt H, Dören M. [Psychosocial risk factors for cancer development] [article in German]. Med Klin (Munich). 2007; 102(12):967–979.PubMed doi:10.7/s63-28y 23. Cox T, Mackay C. Psychosocial factors and psychophysiological mechanisms in the aetiology and development of cancers. Soc Sci Med. 1982;16(4):381–396. doi:10.6/27-953(8)4XPubMed 24. Reynaert C, Libert Y, Janne P. [“Psychogenesis” of cancer: between myths, misuses and reality] [article in French]. Bull Cancer. 2000;87(9):655–664.PubMed. © COPYRIGHT 2012 PHYSICIANS POSTGRADUATE PRESS, INC. © COPYRIGHT 2012 PHYSICIANS POSTGRADUATE RESS2012 , INC. J Clin Psychiatry 73:4,PApril e560.
(7)
數據


相關文件
– The The readLine readLine method is the same method used to read method is the same method used to read from the keyboard, but in this case it would read from a
The underlying idea was to use the power of sampling, in a fashion similar to the way it is used in empirical samples from large universes of data, in order to approximate the
8.2.1 In the 2012 Study, only the enrolment ratio method was used in projecting demand from local students. In the present study, both the enrolment ratio and the grade transition
• we used population genomic and transcriptom ic data from Drosophila melanogaster and its clos e relatives to investigate the origin and spread of de novo genes within
• In the present work, we confine our discussions to mass spectro metry-based proteomics, and to study design and data resources, tools and analysis in a research
The objective of this study is to analyze the population and employment of Taichung metropolitan area by economic-based analysis to provide for government
In this study the GPS and WiFi are used to construct Space Guidance System for visitors to easily navigate to target.. This study will use 3D technology to
Therefore, a new method, which is based on data mining technique, is proposed to classify driving behavior in multiclass user traffic flow.. In this study, driving behaviors
