中國醫藥大學機構典藏 China Medical University Repository, Taiwan:Item 310903500/50308
56
0
0
全文
(2) 中文摘要 研究目的 慢性病毒性肝炎在治療結核病病患的過程中是否會影響病人肝 功能異常出現的機會和肝功能異常出現的時間目前仍有爭論。本 研究的目的在探討在治療前肝功能正常的急性結核病病人在接受 抗結核藥物治療時,慢性病毒性肝炎是否會影響肝功能異常的比 率和出現的時間。 研究方法 所有在 2002 到 2009 年間在這個中臺灣三級轉診醫學中心新 診斷的結核病人資料會經由電腦資訊系統收集病人一系列的肝功 能資料,包括轉胺酶和黃膽指數。暫時性肝臟生化指數異常的定 義如以下,需合乎以下兩個條件 (1)假如轉胺酶上昇高於正常 值,但是在持續用抗結核藥物的情况下,肝臟生化指數又回復到 正常的範圍 (2)假如藥物一開始因為肝臓生化指數異常而停用, 但在肝臟生化指數回復到正常後,重新使用抗結核藥物後並未再. i.
(3) 出現肝臟生化指數異常。藥物引起的肝炎定義為服用抗結核藥物 後肝臟生化檢查中的轉胺酶超過 120 IU/L 合併急性肝炎的症 狀,或是轉胺酶超過了 200 IU/L 合併或未合併急性肝炎症狀。當 肝功能回復正常後,在重新使用抗結核藥物後轉胺酶又超過了 120IU/L。肝臟生化檢查異常出現的比率和出現的時間會在有 B 型肝炎、C 型肝炎及無慢性病毒性肝炎(對照組)間比較。 研究結果 共有 533 病人進入此研究。藥物引起的肝炎的比率,在治療前 肝功能正常者,在有慢性病毒性肝炎和無慢性病毒性肝炎的對照 組比較並無顯著差異 [8% (32/392) 比上 7% (11/161), P > 0.05], 暫時肝臟生化檢查異常出現的比率在無慢性病毒性肝炎者的比率 較低且有統計上的明顯差異 [2% (9/392) 比上 12% (20/161), P < 0.001]。平均肝臟生化檢查異常出現的時間,在藥物引起的肝炎 者在對照組是 40 天,在慢性病毒性 B 型肝炎者是 39 天, 在慢 性病毒性 C 型肝炎者是 67 天 (所有 P > 0.05)。 暫時性肝臟生 化檢查異常出現的時間,在對照組是 23 天,在慢性病毒性 B 型 ii.
(4) 肝炎者是 48 天,在慢性病毒性 C 型肝炎者是 68 天( 和對照組 比較,所有 P < 0.05)。在慢性病毒性肝炎的病人,發生暫時性肝 臟生化檢查的比率是藥物引起的肝炎發生的兩倍,不論異常是否 發生在服藥開始的兩個月內。而在無病毒性肝炎的病人,在前兩 個月發生肝功能異常者,有 76%是藥物引起的肝炎,而在兩個月 後發生的肝功能異常者,完全是藥物引起的肝炎。 研究結論 在有慢性病毒性肝炎的病人,肝臟生化功能檢查異常的原因以暫 時性肝臟生化檢查異常的比率較高,暫時性肝臟生化檢查異常發 生的時間也較晚,而藥物引起的肝炎發生的時間則無明顯差異。 醫師需要將肝功能異常發生時間列入考量,以決定是否要停藥。. iii.
(5) 英文摘要 Objective: Whether chronic viral hepatitis affects the incidence and onset time of elevation of liver biochemistry test during anti-tuberculosis (TB) treatment in patients with chronic hepatitis is still controversial. The aim of this retrospective study was to answer whether chronic viral hepatitis would influence the incidence and onset time of liver biochemistry test in patients with normal baseline liver function. Methods: All patients diagnosed with active TB and being treated at a tertiary referral hospital in central Taiwan between 2002 and 2009 were identified from medical records, among which 533 patients enrolled in the study. Serial liver function tests at baseline and during anti-TB treatment were collected including levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin and direct bilirubin. Transient liver function impairment (TLI) was defined under 2 sets of conditions: (1) if AST or ALT levels increased at any level, but resolved spontaneously despite iv.
(6) continued anti-TB medications; (2) if the drug was first discontinued and the patient was successfully re-challenged with the drug after the liver function test results were normal. Drug induced hepatitis (DIH) was confirmed in a patient if the liver transaminase level exceeded 120 IU/L with symptoms of acute hepatitis or exceeded 200 IU/L with or without symptoms while the anti-TB drug treatment was stopped, and the liver transaminase level increased to >120 IU/L when the patient was re-challenged with the culprit drug. The incidence and onset time of DIH and TLI in patients with and without chronic viral hepatitis (controls) were compared. Results: The incidence of DIH was similar in patients with and without chronic hepatitis (8% [32/392] vs. 7% [11/161], P > 0.05). The incidence of transient liver function impairment (TLI) was significantly lower in controls than in chronic hepatitis patients (2% [9/392] vs. 12% [20/161], P < 0.001. The mean onset of DIH in the control, hepatitis B virus (HBV), and hepatitis C virus (HCV) groups were not significantly different (40 days, 39 days, and 67 days, respectively, all P > 0.05). The mean onset times of TLI in the control, v.
(7) HBV, and HCV groups were significantly different (23 days, 48 days, and 68 days, respectively, all P < 0.05). In patients with chronic viral hepatitis, liver function impairment during anti-TB therapy may be caused by TLI or DIH, and the chance of TLI is approximately twice of DIH regardless of whether the onset time is within the first 2 months after initiation of anti-TB therapy. Whereas in patients without chronic hepatitis who experienced liver function impairment within 2 months of treatment, the likelihood of DIH is 76%, TLI is 24% and liver function impairment occurred after 2 months were all caused by DIH. Conclusions: Liver function impairment during anti-TB therapy in patients with chronic viral hepatitis was mostly because of TLI, with TLI occurring later than in controls. Chronic viral hepatitis had no significant effect on the incidence of DIH. Physicians should take the onset time of liver function impairment into consideration to decide whether the potential hepatotoxic drug should be stopped.. vi.
(8) 誌謝辭. 能夠進入臨床醫學研究所就讀,修完必要的學分,並完成碩 士論文,最最感謝是我的兩位指導老師,徐武輝主任和吳禮字老 師。謝謝陳志銘醫師,也是常久以來一直很照顧我的學長,建議 我找這兩位好老師擔任我的指導教授,也在一直關心我的論文進 度。也感激兩位老師能同意指導我這個研究能力薄弱的學生。徐 主任有繁重的行政和醫療工作,但仍花費大量心思和時間指導我 的論文。經過和徐主任反覆的討論和修改後,我慢慢比較能了解 科學論文寫作的方向,能以較簡潔的文字和合邏輯的推論闡述要 點。吳禮字老師對我的實驗購想提供了很寶貴的意見,從老師那 我學習到了解實驗原理的重要性,希望以後還能有再和老師學習 的機會。還有在百忙中抽空任我論文口試委員的盧章智主任,曹 世明主任及賴志和老師,您寶貴的意見和研究方向的建議對我有 很大的幫助。 vii.
(9) 能夠在半工半讀下攻讀碩士,最大的動力是來自彰基感染科 劉尊榮主任的鼓勵。也感謝科內主治醫師對我的論文提供修改的 建議,科內吳彬彬醫師和許瑛敉醫師協助會診和住院病人的照 顧,讓我能無後顧之憂的完成學業。還有兩位個案管理師,淑琪 和佩霖,沒有你們,這個研究絕對無法完成。 感謝我的父母和最親愛的太太琪美,有你們無窮的支持,讓 我能渡過種種的低潮,你們是上天給我最大的禮物!. viii.
(10) 目錄. 中文摘要 --------------------------------------------------------- i 英文摘要 --------------------------------------------------------- iv 誌謝辭 ------------------------------------------------------------ vii 目錄 --------------------------------------------------------------- ix 表目錄 ------------------------------------------------------------ xii. 論文正文. 第一章 前言 1.1 研究背景 ---------------------------------------- 1 1.2 研究目的 ---------------------------------------- 3 第二章 研究方法 ix.
(11) 2.1 研究材料 ---------------------------------------- 4 2.2 研究設計 ---------------------------------------- 5 2.2.1 資料收集 2.2.2 定義 2.2.3 治療和監測 2.3 統計方法 ---------------------------------------- 10 第三章 研究結果 3.1 描述性統計分析 ------------------------------- 11 3.1.1 病人背景資料 3.1.2 排除病人描述 3.2 推論性統計分析 -------------------------------- 13 3.2.1 肝功能異常發生的機率 3.2.2 黃膽發生的機率 3.2.3 藥物引起肝炎的嚴重程度 3.2.4 肝功能異常出現的時間 3.2.5 不同種類的抗結核病藥物引起肝功能異常的出 x.
(12) 現時間 第四章 討論 4.1 結果討論 ---------------------------------------- 19 4.2 其他相關性討論 --------------------------------- 21 4.3 研究限制 ---------------------------------------- 24 第五章 結論與建議 5.1 結論 ---------------------------------------------- 25 5.2 建議 ---------------------------------------------- 26 參考文獻 -------------------------------------------------------- 28 表. ----------------------------------------------------------------- 34. xi.
(13) 表目錄. Table 1. Baseline characteristics of patients with chronic viral hepatitis and control subjects. ------------------------------- 34 Table 2. Incidences of hepatitis during anti-TB treatment in different patient groups. ----------------------------------------------- 36 Table 3. The association between jaundice and the drug induced hepatotoxicity. ----------------------------------------------- 37 Table 4. Incidence of jaundice in different group of patients. -------------------------------------------------------------------- 38 Table 5. The onset of liver function impairment. --------- 39 Table 6. Number of patients developed liver function impairment in different periods. --------------------------------------------. 41. Table 7. Days of onset of DIH in different drugs. --------- 42 Table 8. Significance of the effect of drugs on the onset of DIH. --------------------------------------------------------------------- 43. xii.
(14) 第一章 前言 1.1 研究背景 Tuberculosis (TB) remains a major health concern worldwide [1]. Short-course chemotherapies based on a combination of isoniazid and rifampicin have been shown to be highly effective in treating TB [2]. Addition of pyrazinamide shortens the time course of treatment; however, the effectiveness is offset by the increased incidence of drug-induced hepatotoxicity (DIH), which may limit the use of these drugs [2]. DIH may be fatal if not recognized promptly. Previous studies have discussed the factors that can cause an increased risk of DIH. These factors include advanced age, female gender, alcohol use, and malnutrition [3-5]. Chronic liver disease has also been shown to be a factor for increased risk. It is still controversial whether the incidence of DIH is higher in patients with chronic hepatitis B virus (HBV) infection than in those without infection during anti-TB treatment [6-10]. Lee et al. included 110 inactive HBV carriers in the largest 1.
(15) study population to date. They reported that elevations in liver enzyme levels during anti-TB therapy were more common in HBV carriers than in controls (8% vs. 4%), but the difference was not statistically significant [8]. However, few studies reported about the potential association of chronic liver disease with the onset of DIH. Here, we report our investigation on the association between chronic hepatitis and the onset time of DIH during anti-TB treatment in patients with active TB.. 2.
(16) 1.2 研究目的 Investigate the association between chronic viral hepatitis with the incidence of liver function impairment and the onset time of DIH.. 3.
(17) 第二章 研究方法 2.1 研究材料 We retrospectively enrolled patients diagnosed with TB who were receiving anti-TB agents at the Changhua Christian Hospital, a tertiary referral hospital in central Taiwan, from January 2002 to December 2009.. 4.
(18) 2.2 研究設計 2.2.1 資料收集 Information was collected by a computer-assisted search of medical records of patients diagnosed with TB. The following data were collected: age, sex, underlying diseases, concurrent use of other hepatotoxic agents, dates of prescribing and stopping anti-TB agents, regimens and doses of anti-TB agents, serology testing for hepatitis B virus surface antigen (HBsAg) and hepatitis C virus (HCV) antibodies, serial liver function tests at baseline and during anti-TB treatment (including levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), and total and direct bilirubin), associated symptoms of hepatitis (including poor appetite, nausea, vomiting, fatigue, lower leg edema, abdominal discomfort, and jaundice), and treatment outcomes. Patients with abnormal baseline liver function tests, HIV infection, those who were lost to follow-up, transferred to other institutions, had stopped anti-TB treatment because an alternative diagnosis was made, 5.
(19) and whose death was not attributable to drug induced hepatitis were excluded. We excluded patients with abnormal baseline liver function tests or human immunodeficiency virus (HIV) infection from the present study. These patients were excluded because: (1) it is difficult to define patients with an abnormal baseline liver function test who develop liver function impairment after therapy; (2) patients with HIV infection may experience abnormal liver function secondary to antiretroviral agents or opportunistic infection; (3) if patients with HIV infection developed liver function impairment during anti-TB treatment, it would be difficult to determine its cause.. 6.
(20) 2.2.2 定義 The criteria used to define transient liver function impairment (TLI) and DIH were based on previous study recommendations [2, 8, 11, 12]. TLI was defined under 2 sets of conditions: (1) if aspartate aminotransferase (AST)/alanine aminotransferase (ALT) levels increased at any level, but resolved spontaneously despite continued anti-TB medications; (2) if the drug was first discontinued and the patient was successfully re-challenged with the drug after the liver function test results were normal. For example, if the liver enzyme level was elevated to 150 IU/L, and this abnormality resolved spontaneously during continuation of anti-TB treatment, we defined this condition as TLI. DIH was confirmed in a patient if the liver transaminase level exceeded 120 IU/L with symptoms of acute hepatitis or exceeded 200 IU/L with or without symptoms while the anti-TB drug treatment was stopped, and the liver transaminase level increased to >120 IU/L when the patient was re-challenged with the drug. Resolution of liver toxicity manifestations after drug withdrawal is evidence of DIH [13]. Mild DIH was defined as 120 7.
(21) IU/L< AST/ALT levels <= 200 IU/L, moderate DIH as 200 IU/L < AST/ALT levels <= 500 IU/L, and severe DIH as AST/ALT levels >500 IU/L.. 8.
(22) 2.2.3 治療和監測 Most patients initially received daily isoniazid, rifampicin, ethambutol, and pyrazinamide in the first 2 months followed by isoniazid, rifampicin, and ethambutol in the subsequent 4 months. Liver function tests were performed once per 2 weeks in the first month after the initiation of treatment and on a monthly basis thereafter. If any liver chemistry abnormalities were detected, monitoring was performed more frequently. Patients developing increased liver transaminase levels but without clinical symptoms were carefully observed without discontinuation of any anti-TB agents. If the patient had symptoms of hepatitis, all drugs that could possibly be hepatotoxic were stopped. After liver transaminase normalization, hepatotoxic drugs were serially restarted. If liver transaminase levels increased during a rechallenge of the therapy, the specific drug was discontinued. A drug was considered responsible for adverse effects if symptoms appeared with the start of the drug, resolved with withdrawal, and reappeared with a challenge of the same drug. 9.
(23) 2.3 統計方法 Values are expressed as mean ± standard deviation or as number (percentage) in the text and tables. Differences with regard to numerical values between different groups were analyzed using the Student t test or the Mann–Whitney U test depending on the distribution of the data. Nominal variables were assessed using the chi-square test or the Fisher exact test. Baseline characteristics among the HBV, HCV, and control groups were analyzed by 1-way ANOVA and post hoc analysis. A P value of <0.05 was considered statistically significant.. 10.
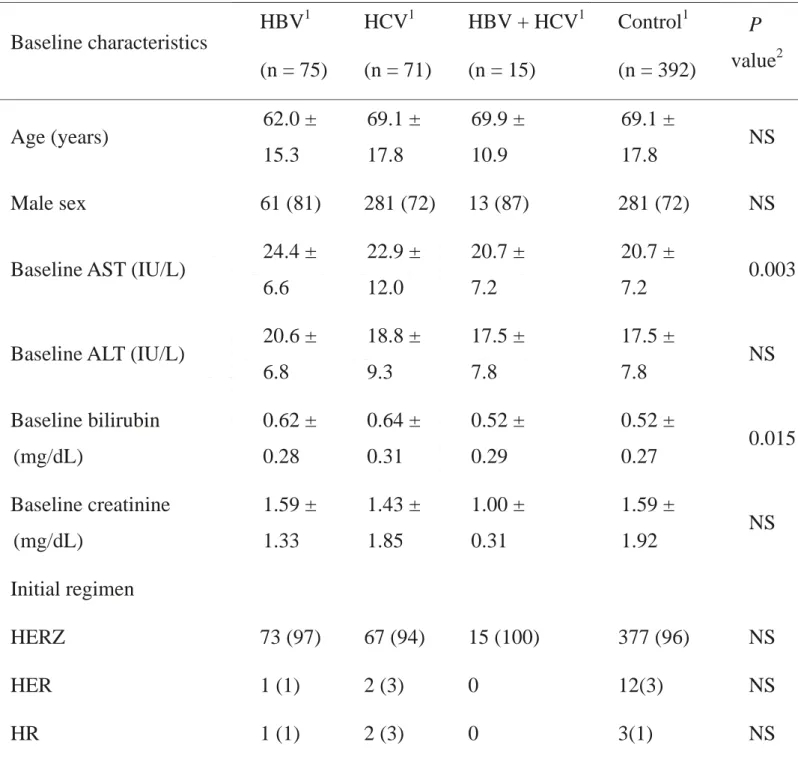
(24) 第三章 研究結果 3.1 描述性統計分析 3.1.1 病人背景資料 A total of 553 patients were enrolled. All patients were screened for HBV and HCV before anti-TB treatment. Of these, 392 were negative for HBsAg and HCV antibody (control group), 75 were positive for HBsAg and negative for HCV antibody (HBV group), and 71 were positive for HCV antibody and negative for HBsAg (HCV group). Fifteen patients were positive for both HBsAg and HCV antibody (HBV + HCV group). Baseline characteristics of the HBV, HCV, HBV + HCV, and control group patients are shown in Table 1. Age, sex, baseline renal function test results, and the initial treatment regimen were almost identical in the 3 groups; most patients (> 90%) started their anti-TB regimen with a standard 4-drug combination, including isoniazid, rifampicin, ethambutol, and pyrazinamide.. 11.
(25) 3.1.2 排除病人描述 One hundred and thirty-seven patients were excluded because of the following reasons: 37 had abnormal baseline liver function tests, 3 were alcohol-dependent, 7 had HIV infection, 8 were lost to follow-up, 25 were transferred to other institutions, 43 stopped anti-TB treatment because an alternative diagnosis was made, and 22 died during anti-TB treatment but their death was not attributable to DIH.. 12.
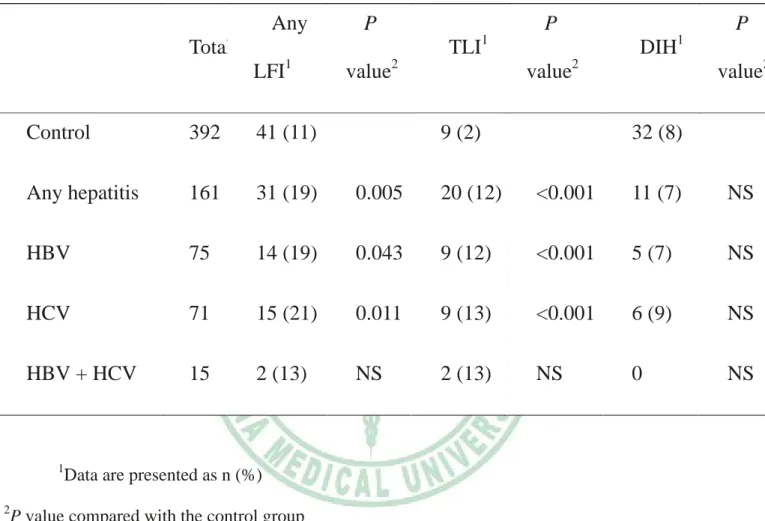
(26) 3.2 推論性統計分析 3.2.1 肝功能異常發生的機率 Seventy-two (13%) patients developed liver function impairment during anti-TB therapy. The incidence of any liver function impairment was higher in patients with HBV or HBV than in those without; incidences of elevated liver function enzyme levels during anti-TB therapy in HBV, HCV, and control groups were 19% (14/75), 21% (15/71), and 11% (41/392), respectively (Table 2). Patients in the HCV or HBV groups had a significantly higher incidence of TLI during treatment than controls (all P < 0.001). However, the incidence of DIH showed no significant differences among the 3 groups (7% [5/75], 9% [6/71], and 8% [32/392], all P > 0.05). The major contribution to the differences in liver function impairment during anti-TB treatment between the HBV, HCV, and control groups was only because of TLI. These results are shown in detail in Table 2.. 13.
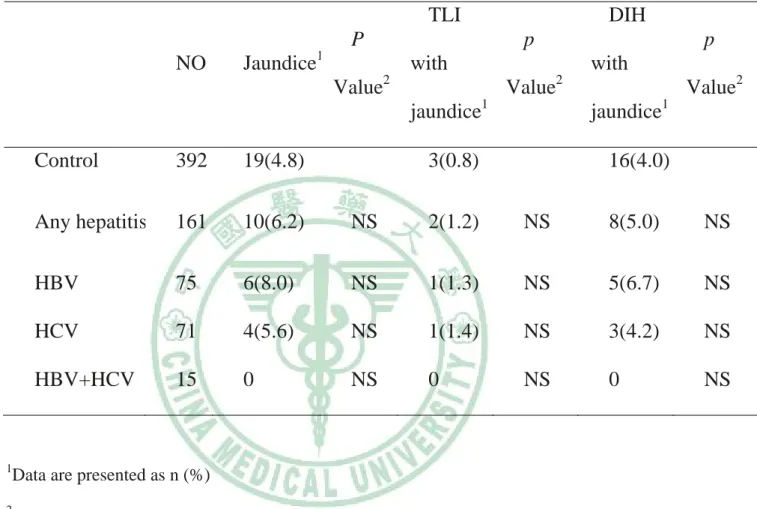
(27) 3.2.2 黃膽發生的機率 The incidence of jaundice was higher in patients with DIH than in those with TLI (Table 3). Jaundice developed in 25 patients with DIH, but only in 5 patients with TLI (odds ratio [OR] 5.2, 95% confidence interval [CI] 2.0–13.7; P < 0.001). In the control group, 3 patients with TLI and 16 patients with DIH developed jaundice (OR 5.5, 95% CI 1.6–19.1; P = 0.004). Among the patients in the HBV and HCV groups, those with DIH had higher incidences of jaundice than those with in TLI, although the differences were not statistically significant. In patients with chronic viral hepatitis, 8 patients with DIH and 2 patients with TLI developed jaundice (OR 4.7, 95% CI 1.0–22.1; P = 0.061). The incidence of jaundice was similar in HBV, HCV and control group at the range from 5 to 8 percent (Table 4).. 14.
(28) 3.2.3 藥物引起肝炎的嚴重程度 There were no significant differences in the severity of liver function impairment in patients in the HBV, HCV, and control groups. Among the patients without chronic hepatitis B or C, mild hepatotoxicity. developed. in. 10. patients. (2.6%),. moderate. hepatotoxicity in 10 (2.6%), and severe toxicity in 11 (2.8%). Among the 5 HBV patients with drug-induced hepatotoxicity, 2 (2.7%) had mild hepatotoxicity, no patient had moderate hepatotoxicity, and 3 (4%) had severe hepatotoxicity. Among the 6 HCV patients with DIH, 2 (2.8%) had mild hepatotoxicity, 2 (2.8%) had moderate hepatotoxicity, and 2 (2.8%) had severe hepatotoxicity.. 15.
(29) 3.2.4 肝功能異常出現的時間 The mean onset times of liver function impairment in patients with TLI and those with DIH were 46 ± 33 days and 47 ± 29 days, respectively (P > 0.05). The mean onset times of TLI in controls, HBV, and HCV were significantly different (23 days, 48 days, and 68 days, respectively, all P < 0.05; Table 5). We did not find any significant effect of the type of anti-TB medication on the time of DIH onset. In the control group, TLI developed within 1 month in 6 patients (6/9 [67%]). In contrast, less than half of the patients developed TLI during the first month of treatment in the HCV and HBV groups. The onset times of DIH are also shown in detail in Table 4. The mean onset times of DIH in controls, HBV, and HCV groups were not significantly different (40 days, 39 days, and 67 days, respectively, all P > 0.05). Eighty percent of HBV patients and 90% of controls developed DIH within 2 months. Nevertheless, 50% of the HCV patients developed DIH after 2 months (P < 0.05). In patients with chronic viral hepatitis who developed liver function 16.
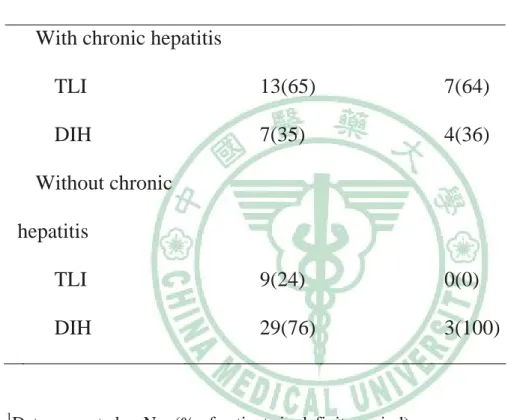
(30) impairment, approximately 40% developed DIH either <2 months or >2 months after initiation of anti-TB therapy. Conversely, among patients without chronic viral hepatitis, 76% developed liver dysfunction within 2 months due to DIH, and no patient developed TLI after 2 months.. 17.
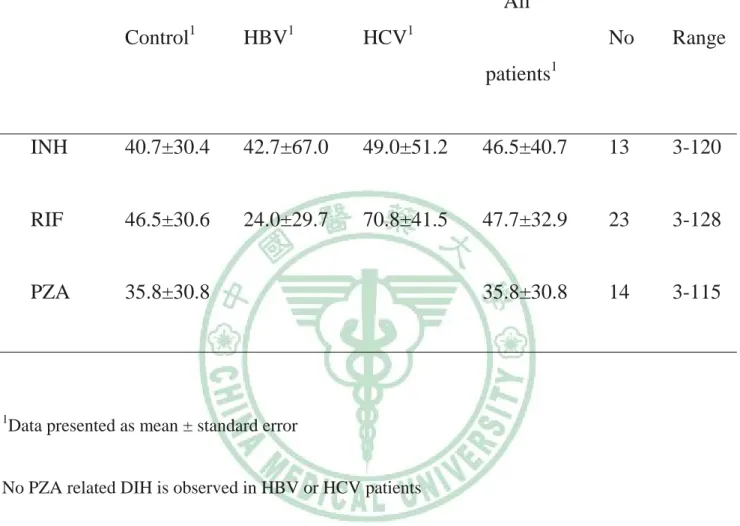
(31) 3.2.5 不同種類的抗結核病藥物引起肝功能異常的出現 時間 The. onset. time. of. DIH. in. isoniazid-,. rifampicin-,. and. pyrazinamide-related hepatotoxicity were 47 ± 41 days (range, 3–120 days), 48 ± 33 days (range, 3–128 days), and 36 ± 31 days (range, 3–115 days), respectively (Table 7). We did not find any significant effect of different types of anti-TB medication on the onset of DIH with all P value larger than 0.05 (Table 8).. 18.
(32) 第四章 討論 4.1 結果討論 In clinical practice it is difficult to decide whether anti-TB treatment should be continued because TLI is relatively common in patients with anti-TB treatment. A newly acquired viral hepatitis or acute exacerbation of chronic hepatitis is of particular concern in areas where the disease is endemic [2, 14, 15]. Inability to recognize other causes of hepatotoxicity and unnecessary discontinuation of anti-TB medication may prolong the course of treatment, increase the possibility of treatment failure, and increase the rate of drug resistance. On the other hand, failure to find true DIH and discontinuation of medication promptly may be fatal [16, 17]. Recent reports on large series of patients with anti-TB DIH demonstrate that fatality is not uncommon occurring in over 20% of patients with anti-TB DIH particularly in those who exhibit jaundice. In fact the mortality with the occurrence of acute liver failure is still higher over 67% [18 - 20]. 19.
(33) In our study, we found that TLI had a significantly higher incidence in the HBsAg- or HCV antibody-positive patients (14.3%) than in controls (2.3%). Moreover, TLI was observed more often (14.3%) than DIH (7.1%) in patients with chronic viral hepatitis. Conversely, the incidences of DIH and TLI were 8.7% and 2.3%, respectively, in patients without chronic viral hepatitis. The incidence of DIH was about the same in patients with or without chronic hepatitis (7.1% vs. 8.7%). These results are valuable and are worthy of further consideration in anti-TB treatment.. 20.
(34) 4.2 其他相關性討論 The severity of DIH in HBV carriers and control groups has been discussed by Lee et al [8]. They found that HBsAg-positive carriers had a higher proportion of moderate-to-severe DIH compared with HBsAg-negative subjects. However, our results found that the severity of DIH was not significantly different between the HBV, HCV, and control groups. The findings may be different because we included 30 DIH patients in our control group whereas Lee et al. included only 4 in their study. The effect of chronic hepatitis on the onset of liver function impairment during anti-TB chemotherapy has been mentioned in a few studies. Previous studies have reported that DIH usually occurred within the initial 2 months of therapy [21, 22]. We found that TLI occurred later in patients with chronic hepatitis. One possible explanation is a flare-up of the chronic hepatitis virus. A future study with detailed follow-up of hepatitis viral load in patients with viral hepatitis taking anti-TB medication would help to find out if this 21.
(35) assumption is valid. We observed that the HCV group had a tendency towards a later onset of DIH than the HBV and control groups, although the difference was not statically significant. However, we still found that DIH developed more frequently in the HCV group than in the control group, more than 2 months after initiating anti-TB therapy. Therefore, we suggest that patients with HCV should have liver function tests routinely during the later period of anti-TB treatment even when DIH does not occur within first 2 months. Chien et al. also studied the onset of DIH [23]. They found that the onset of DIH in patients without chronic hepatitis was approximately 40 days, and our study had a similar finding. One anomaly in their study was that co-infection with HBV was associated with a later onset at a mean of 102 days in 3 patients. Wang et al. investigated the impact of baseline HBV and HCV viral load on hepatitis during anti-TB treatment [24]. They found a high baseline hepatitis viral load is associated with higher odds of getting DIH and flare up of viral hepatitis whereas in chronic viral hepatitis patients carrying low or undetectable baseline viral loads the odds is not different from 22.
(36) patients without chronic hepatitis. In our study, the incidence of DIH is not increased in patients with chronic HBV or HCV may be contributed to our strict inclusion criteria. We excluded patients with abnormal baseline liver function. Based on the results of our study and Wang’s study, we infer that the chances of DIH will not increase in chronic viral hepatitis with baseline normal liver biochemistry test. Another interesting finding is with regard to jaundice. We did not find that chronic hepatitis had a significant effect on the incidence and onset of jaundice. Patients with DIH had a higher incidence of jaundice than those with TLI. This reflects true organ toxicity in patients with DIH. If jaundice develops during anti-TB treatment, DIH should be considered first regardless of previous hepatitis status. Discontinuation of the hepatotoxic drug and close observation are necessary even in patients with chronic hepatitis. On the contrary, TLI reflects flare up of chronic viral hepatitis or hepatic adaption to anti-tuberculosis chemotherapy [25]. Patients may develop some sort of tolerance to the drug in question and therefore may never develop hepatitis the second time the drug is administered. 23.
(37) 4.3 研究限制 Because this was a retrospective study, it has some limitations. First, precise information on concurrent use of other herbal medicines or so-called health foods that are commonly consumed by Taiwanese patients was not available from medical chart review. Second, the measurement of liver function in most patients was performed on a regular biweekly or monthly basis. Therefore, the exact day of the onset of liver function impairment may be earlier than the day recorded in this study. Third, most patients who developed liver function impairment were not routinely checked for HBV and HCV viral load, hepatitis A virus IgM, and hepatitis E virus IgM, which are endemic in Taiwan [26]. Occasionally, definite causes of hepatitis were not determined.. 24.
(38) 第五章 結論與建議 5.1 結論 In conclusion, we found that liver function impairment during anti-TB therapy was mostly because of TLI in patients with chronic viral hepatitis, and because of DIH in patients without chronic viral hepatitis. Chronic hepatitis had no significant effect on the onset of DIH, but TLI occurred later in patients with chronic hepatitis. Our study can help clinicians to proper management of liver function impairment in patients receiving anti-TB treatment.. 25.
(39) 5.2 建議 We emphasize that the present study found some important clinical effects. First, physicians shall not worry about a higher likelihood of DIH in their chronic viral hepatitis patients during anti-TB therapy whose baseline liver biochemistry tests are normal. Second, physicians should take the onset of liver function impairment and whether the patient had chronic hepatitis into consideration to decide whether the potential hepatotoxic drug should be stopped. In patients with chronic viral hepatitis developing abnormal liver function test during anti-TB therapy, continue anti-tuberculosis medication is a rational approach unless hepatitis symptoms occur. Because the chance of TLI is approximately twice of DIH regardless of the onset time of abnormal liver function test according to our observation. In patients without chronic hepatitis who experienced liver function, the onset time is an important factor for clinical decision. If liver function impairment occurred after 2 months, we suggested hepatotoxic agents shall be stopped instantly and rechallenge the drug separately to 26.
(40) determine the culprit medication. Third, in patients with chronic hepatitis, we suggested follow up liver biochemistry test intensely even after 2 months of initializing anti-TB therapy owing to half of HCV patients developed DIH during this period.. 27.
(41) 參考文獻 1.Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC: Consensus statement. Global burden of tuberculosis: Estimated incidence, prevalence, and mortality by country. Who global surveillance and monitoring project. JAMA : the journal of the American Medical Association 1999;282:677-686. 2.Blumberg HM, Burman WJ, Chaisson RE, Daley CL, Etkind SC, Friedman LN, Fujiwara P, Grzemska M, Hopewell PC, Iseman MD, Jasmer RM, Koppaka V, Menzies RI, O'Brien RJ, Reves RR, Reichman LB, Simone PM, Starke JR, Vernon AA: American thoracic society/centers for disease control and prevention/infectious diseases society of America: Treatment of tuberculosis. American journal of respiratory and critical care medicine 2003;167:603-662. 3.Dossing M, Wilcke JT, Askgaard DS, Nybo B: Liver injury during antituberculosis treatment: An 11-year study. Tubercle and lung disease : the official journal of the International Union against Tuberculosis and Lung Disease 1996;77:335-340. 28.
(42) 4.Pande JN, Singh SP, Khilnani GC, Khilnani S, Tandon RK: Risk factors for hepatotoxicity from antituberculosis drugs: A case-control study. Thorax 1996;51:132-136. 5.Schaberg T, Rebhan K, Lode H: Risk factors for side-effects of isoniazid, rifampin and pyrazinamide in patients hospitalized for pulmonary tuberculosis. The European respiratory journal : official journal of the European Society for Clinical Respiratory Physiology 1996;9:2026-2030. 6.Amarapurkar DN, Prabhudesai PP, Kalro RH, Desai HG: Antituberculosis drug-induced hepatitis and HBsAg carriers. Tubercle and lung disease : the official journal of the International Union against Tuberculosis and Lung Disease 1993;74:215-216. 7.Hwang SJ, Wu JC, Lee CN, Yen FS, Lu CL, Lin TP, Lee SD: A prospective clinical study of isoniazid-rifampicin-pyrazinamide-induced liver injury in an area endemic for hepatitis B. Journal of gastroenterology and hepatology 1997;12:87-91. 8.Lee BH, Koh WJ, Choi MS, Suh GY, Chung MP, Kim H, Kwon 29.
(43) OJ: Inactive hepatitis B surface antigen carrier state and hepatotoxicity during antituberculosis chemotherapy. Chest 2005;127:1304-1311. 9.Wong WM, Wu PC, Yuen MF, Cheng CC, Yew WW, Wong PC, Tam CM, Leung CC, Lai CL: Antituberculosis drug-related liver dysfunction in chronic hepatitis B infection. Hepatology 2000;31:201-206. 10.Wu JC, Lee SD, Yeh PF, Chan CY, Wang YJ, Huang YS, Tsai YT, Lee PY, Ting LP, Lo KJ: Isoniazid-rifampin-induced hepatitis in hepatitis B carriers. Gastroenterology 1990;98:502-504. 11.Ungo JR, Jones D, Ashkin D, Hollender ES, Bernstein D, Albanese AP, Pitchenik AE: Antituberculosis drug-induced hepatotoxicity. The role of hepatitis C virus and the human immunodeficiency virus. American journal of respiratory and critical care medicine 1998;157:1871-1876. 12.Yee D, Valiquette C, Pelletier M, Parisien I, Rocher I, Menzies D: Incidence of serious side effects from first-line antituberculosis drugs among patients treated for active tuberculosis. 30.
(44) American journal of respiratory and critical care medicine 2003;167:1472-1477. 13.Yew WW, Leung CC: Antituberculosis drugs and hepatotoxicity. Respirology 2006;11:699-707. 14.Chemotherapy and management of tuberculosis in the United Kingdom: Recommendations 1998. Joint Tuberculosis Committee of the British Thoracic Society. Thorax 1998;53:536-548. 15.Turktas H, Unsal M, Tulek N, Oruc O: Hepatotoxicity of antituberculosis therapy (rifampicin, isoniazid and pyrazinamide) or viral hepatitis. Tubercle and lung disease : the official journal of the International Union against Tuberculosis and Lung Disease 1994;75:58-60. 16.Tost JR, Vidal R, Cayla J, Diaz-Cabanela D, Jimenez A, Broquetas JM: Severe hepatotoxicity due to anti-tuberculosis drugs in spain. The international journal of tuberculosis and lung disease : the official journal of the International Union against Tuberculosis and Lung Disease 2005;9:534-540. 17.Whittington RM: Fatal hepatotoxicity of anti-tubercular 31.
(45) chemotherapy. Lancet 1991;338:1083-1084. 18.Kumar R, Shalimar, Bhatia V, Khanal S, Sreenivas V, Gupta SD, Panda SK, Acharya SK. Antituberculosis therapy-induced acute liver failure: magnitude, profile, prognosis, and predictors of outcome. Hepatology 2010;51:1665-1674. 19.Devarbhavi H, Dierkhising R, Kremers WK. Antituberculosis therapy drug-induced liver injury and acute liver failure. Hepatology 2010;52:798-799. 20.Devarbhavi H, Singh R, Patil M, Sheth K, Adarsh CK, Balarajuet G. Outcome and determinants of mortality in 269 patients with combination anti-tuberculosis drug-induced liver injury. Journal of Gastroenterol Hepatol 2013;28 (1):161-7 21.Girling DJ: Adverse effects of antituberculosis drugs. Drugs 1982;23:56-74. 22.Sun HY, Chen YJ, Gau CS, Chang SC, Luh KT: A prospective study of hepatitis during antituberculous treatment in Taiwanese patients and a review of the literature. Journal of the Formosan Medical Association 2009;108:102-111. 32.
(46) 23.Chien JY, Huang RM, Wang JY, Ruan SY, Chien YJ, Yu CJ, Yang PC: Hepatitis C virus infection increases hepatitis risk during anti-tuberculosis treatment. The international journal of tuberculosis and lung disease : the official journal of the International Union against Tuberculosis and Lung Disease 2010;14:616-621. 24.Wang JW, Liu CH, Hu FC, Chang HC, Liu JL, Chen JM, Yu CJ, Lee LN, Kao JH, Yang PC. Risk factors for hepatitis during antituberculous treatment and implications of hepatitis viral load. J infection 2011;62:448-55 25.Senior JR. Monitoring for hepatotoxicity: what is the predictive value of liver "function" tests? Clin Pharmacol Therapeu 2009;85:331-334 26.Lee SD, Wang YJ, Lu RH, Chan CY, Lo KJ, Moeckli R: Seroprevalence of antibody to hepatitis E virus among Chinese subjects in Taiwan. Hepatology 1994;19:866-870.. 33.
(47) Table 1. Baseline characteristics of patients with chronic viral hepatitis and cont subjects. HBV1. HCV1. HBV + HCV1. Control1. P. (n = 75). (n = 71). (n = 15). (n = 392). value2. 62.0 ±. 69.1 ±. 69.9 ±. 69.1 ±. 15.3. 17.8. 10.9. 17.8. 61 (81). 281 (72). 13 (87). 281 (72). 24.4 ±. 22.9 ±. 20.7 ±. 20.7 ±. 6.6. 12.0. 7.2. 7.2. 20.6 ±. 18.8 ±. 17.5 ±. 17.5 ±. 6.8. 9.3. 7.8. 7.8. Baseline bilirubin. 0.62 ±. 0.64 ±. 0.52 ±. 0.52 ±. (mg/dL). 0.28. 0.31. 0.29. 0.27. Baseline creatinine. 1.59 ±. 1.43 ±. 1.00 ±. 1.59 ±. (mg/dL). 1.33. 1.85. 0.31. 1.92. HERZ. 73 (97). 67 (94). 15 (100). 377 (96). NS. HER. 1 (1). 2 (3). 0. 12(3). NS. HR. 1 (1). 2 (3). 0. 3(1). NS. Baseline characteristics. Age (years) Male sex Baseline AST (IU/L). Baseline ALT (IU/L). NS NS 0.003. NS. 0.015. NS. Initial regimen. 34.
(48) 1. Data are presented as mean ± standard error or n (%). 2. P value: 1-way ANOVA.. ALT = alanine aminotransferase; AST = aspartate aminotransferase; HBV, HBV = surface antigen positive and anti-HCV antibody negative; HCV = HBV surface antigen negative and HCV antibody positive; HBV + HCV = both HBV surface antigen positive and anti-HCV antibody positive; HER = isoniazid, ethambutol, and rifampicin; HERZ = isoniazid, ethambutol, rifampicin, and pyrazinamide; HR, isoniazid and rifampicin; IU = International Unit; NS = not significant.. 35.
(49) Table 2. Incidences of hepatitis during anti-TB treatment in different patien groups. Any. P. P. Total. TLI LFI. 2. 1. DIH 2. value. value2. value. Control. 392. 41 (11). Any hepatitis. 161. 31 (19). 0.005. 20 (12). <0.001. 11 (7). NS. HBV. 75. 14 (19). 0.043. 9 (12). <0.001. 5 (7). NS. HCV. 71. 15 (21). 0.011. 9 (13). <0.001. 6 (9). NS. HBV + HCV. 15. 2 (13). NS. 2 (13). NS. 0. NS. 1. 2. 1. P. 1. 9 (2). 32 (8). Data are presented as n (%). P value compared with the control group. DIH = drug-induced hepatotoxicity; HBV = HBV surface antigen positive and anti-HCV antibody negative; HBV + HCV = HBV surface antigen positive and anti-HCV antibody positive; HCV = HBV surface antigen negative and HCV antibody positive; LFI = liver function impairment; NS = not significant; TLI = transient liver function impairment.. 36.
(50) Table 3. The association between jaundice and the drug induced hepatotoxicity. TLI and. DIH and. jaundice/ jaundice/ Total All TLI. All DIH. patients. patients. OR. 95% CI. P value. Control. 392. 3/9. 16/32. 5.5. 1.6–19.1. 0.004. Any hepat. 161. 2/20. 8/11. 4.7. 1.0–22.1. 0.061. All. 553. 5/29. 25/43. 5.2. 2.0–13.7. <0.001. CI = confidence interval; DIH = drug-induced hepatitis; OR = odds ratio; TLI = transient liver function impairment.. 37.
(51) Table 4. Incidence of jaundice in different group of patients. TLI P NO. Jaundice. DIH p. 1. p. with 2. with 2. Value. Value2. Value jaundice1. jaundice1. Control. 392. 19(4.8). Any hepatitis. 161. 10(6.2). NS. 2(1.2). NS. 8(5.0). NS. HBV. 75. 6(8.0). NS. 1(1.3). NS. 5(6.7). NS. HCV. 71. 4(5.6). NS. 1(1.4). NS. 3(4.2). NS. HBV+HCV. 15. 0. NS. 0. NS. 0. NS. 1. Data are presented as n (%). 2. P value compared with the control group. 3(0.8). 16(4.0). DIH = drug-induced hepatotoxicity; HBV = HBV surface antigen positive and anti-HCV antibody negative; HBV + HCV = HBV surface antigen positive and anti-HCV antibody positive; HCV = HBV surface antigen negative and HCV antibody positive; NS = not significant; TLI = transient liver function impairment.. 38.
(52) Table 5. The onset of liver function impairment. Control. HBV. HCV. ~21–97. ~17–120. P. P. value1. value2. TLI Range (days) Mean ± SD. ~5–60. 0.043. 0.004. 22.6 ± 22.3. 47.7 ± 30.8. 67.8 ± 32.8. <2 weeks. 5 (56). 0. 0. 0.029. 0.029. <1 months. 6 (67). 4 (44). 1 (11). NS. 0.05. <2 months. 9 (100). 7 (78). 4 (44). NS. 0.029. <3 months. 9 (100). 8 (89). 7 (78). NS. NS. <4 months. 9 (100). 9 (100). 9 (100). NS. NS. 3–115. 3–120. 10–128 NS. NS. Onset time. DIH Range (days) Mean ± SD. 39.5 ± 26.6. 39.4 ± 48.2. 66.7 ± 44.9. <2 weeks. 6 (19). 3 (60). 1 (17). NS. NS. <1 months. 14 (44). 3 (60). 2 (33). NS. NS. <2 months. 29 (91). 4 (80). 3 (50). NS. 0.039. <3 months. 31 (97). 4 (80). 4 (67). NS. NS. Onset time. 39.
(53) <4 months. 32 (100). 5 (100). 1. 5 (83). NS. 2. NS. P value: HBV group compared with the control group; HCV group compared with the control group. DIH = drug-induced hepatitis; NS = not significant; TLI = transient liver function impairment. 40.
(54) Table 6. Number of patients developed liver func impairment in different periods. <=2 month1. >2 month1. With chronic hepatitis TLI. 13(65). 7(64). DIH. 7(35). 4(36). TLI. 9(24). 0(0). DIH. 29(76). 3(100). Without chronic hepatitis. 1. Data presented as No. (% of patients in definite period). TLI = Transient liver function impairment; DIH = Drug induced hepatitis. 41.
(55) Table 7. Days of onset of DIH in different drugs. All Control1. HBV1. HCV1. No. Range. patients1. 1. INH. 40.7±30.4. 42.7±67.0. 49.0±51.2. 46.5±40.7. 13. 3-120. RIF. 46.5±30.6. 24.0±29.7. 70.8±41.5. 47.7±32.9. 23. 3-128. PZA. 35.8±30.8. 35.8±30.8. 14. 3-115. Data presented as mean ± standard error. No PZA related DIH is observed in HBV or HCV patients. INH = isoniazid; PZA = pyrazinamide; RIF = rifampicin. 42.
(56) Table 8. Significance of the effect of drugs on the onset of DIH. All patients. Control. HBV. HCV. INH vs. RIF. 0.925. 0.961. 0.745. 0.56. INH vs. PZA. 0.897. 0.998. RIF vs. PZA. 0.968. 0.949. No PZA related DIH is observed in HBV or HCV patients. INH = isoniazid; PZA = pyrazinamide; RIF = rifampicin. 43.
(57)
數據

+6


相關文件
After RT alone or combined with chemotherapy, the patients were evaluated at 1-month intervals for the first year, at 2-month intervals during the second year, every 3
Of the 19 patients with clinical stage 2, one (5.3%) patient had a normal epithelium, 16 (84.2%) patients had only epithelial changes (EE + HE), and two (10.5%) patients had
Methods: In two neighboring German cities, prevalence and additional factors of the development of BP-ONJ in multiple myeloma patients with bisphosphonates therapy were recorded
The clinical and radiological features of 6 cases of NBCCS were characterized into major and minor criteria and compared with features reported in Indian patients and in patients
In view of both spread of the HIV epidemic in Africa and poor access to highly active antiretroviral therapy (HAART), infected patients often develop rapidly progressive KS with
Aim: This study examined and classified patients who were treated at the Faculty of Dentistry at Ankara University Dentistry to determine the incidence of different types of
Material and Methods: The databases Scopus, embase, ebsco and PubMed were reviewed from January/2003 to October/2010 with the following keywords: laser therapy, low-level
Aim: The aim of this study is to investigate the prevalence of medical con- ditions and medications used by patients accessing emergency dental care at Manchester Dental
