Betel-Quid Dependence Domains and Syndrome Associated with Betel-Quid Ingredients Among Chewers: An Asian Multi-Country Evidence
Chien-Hung Lee1,2#, Shang-Lun Chiang3#, Albert Min-Shan Ko4, Chun-Hung Hua5, Ming-Hsui Tsai5,Saman Warnakulasuriya6, Salah Osman Ibrahim7, Sunarjo8, Rosnah Binti Zain9,Tian-You Ling10, Chieh-Liang Huang11,Hsien-Yuan Lane12, Cheng-Chieh Lin13, Ying-Chin Ko3,14*
1 Department of Public Health, Kaohsiung Medical University, Kaohsiung, Taiwan 2 Centre of Excellence for Environmental Medicine, Kaohsiung Medical University,
Kaohsiung, Kaohsiung, Taiwan
3 Environment-omics-Disease Research Centre, China Medical University hospital, Taichung, Taiwan
4 Max Planck Institute for Evolutionary Anthropology, Leipzig, Germany
5 Department of Otorhinolaryngology, China Medical University Hospital, Taichung, Taiwan
6 Department of Oral Medicine, King’s College London, and WHO Collaborating Centre for Oral Cancer and Precancer, London, United Kingdom
7 Department of Biomedicine, University of Bergen, Bergen, Norway
8 Department of Public Health & Preventive Medicine, Airlangga University, Surabaya, Indonesia
9 Oral Cancer Research & Coordinating Centre, Faculty of Dentistry, University of Malaya, Kuala Lumpur, Malaysia
10 Department of Stomatology, The Second Xiangya Hospital, Central South University, Hunan, China
11 Department of Addiction Psychiatry, China Medical University Hospital, Taichung, Taiwan
12 Department of Psychiatry, China Medical University and Hospital, Taichung, Taiwan
13 Department of Family Medicine, China Medical University, Taichung, Taiwan 14 Graduate Institute of Clinical Medical Science, College of Medicine, China
Medical University, Taichung, Taiwan
#Drs. Lee and Chiang contributed equally to this work.
*Correspondence: Ying-Chin Ko, MD, PhD, Professor, College of Medicine, China Medical University, 91, Hsueh Shih Rd., Taichung 404, Taiwan. Tel: +886-4-2205-7153; Fax: +886-4-2206-0248; E-mail: [email protected]
Running head: Betel-quid dependence and betel-quid ingredients Word count: 3427 words
Declaration of interest: This study was supported by a grant from the Center of Excellence for Environment Medicine, Kaohsiung Medical University (KMU-EM-99-1-1), and China Medical University Hospital (DMR-103-118), No any connection of any of the researchers with the tobacco, alcohol, pharmaceutical or gaming industries or any body substantially funded by one of these organisations.
ABSTRACT
Background and Aims: Betel-quid (BQ) contains biologically psychoactive ingredients; however, data are limited concerning the symptoms and syndrome of BQ dependence among chewers. The aims of this study were to evaluate the ingredients-associated BQ dependence syndrome and country-specific chewing features and behavior for BQ dependence among chewers of six Asian communities.
Design: An inter-country Asian Betel-quid Consortium study.
Setting: Six Asian general communities in Taiwan, Mainland China, Indonesia,
Malaysia, Sri Lanka and Nepal.
Participants: Six multistage random-samples of BQ chewers in the Asian Betel-quid
Consortium study (n=2078).
Measurements: All chewers were evaluated for BQ dependence using the DSM-IV and
ICD-10 criteria.
Findings: The 12-month BQ dependence rate was 12.5-92.6% and 47.9-99.3% among tobacco-free and tobacco-added BQ chewers, with a higher dependence rate in chewers who used tobacco-free BQ with lime-added than without (23.3-95.6% vs. 4.0%,
P0.001) across the six Asian communities. Taiwanese and Hunanese BQ chewers both notably endorsed the dependency domain of ‘time spent chewing’. ‘Tolerance’ and ‘withdrawal’ were the major dependence domains associated with the Nepalese and Indonesian chewers with high BQ dependence rates. Malaysian and Sri Lankan chewers formed a BQ dependence cluster closely linked to ‘craving’. In Sri Lanka, the quantity consumed explained 90.5% of the excess dependence risk for TA-BQ use, and could be a mediator between tobacco-derived psychoactive effect and BQ dependence development.
Conclusions: Tobacco additive increases the addictive potential. Tobacco-free BQ
INTRODUCTION
Betel-quid (BQ) chewing has been a part of daily life in numerous Asian cultures. Although BQ preparation methods vary among cultural groups and individual use, it is typically constituted by the raw or processed areca nut (AN; Areca catechu) flavored with local condiments or sweetening agents, and wrapped in a betel leaf (Piper betle) combined with slaked lime (calcium hydroxide). In many parts of Asia, the final product is chewed with the addition of tobacco . After caffeine, alcohol and nicotine, BQ is ranked the fourth most consumed psychoactive drug worldwide . Approximately 600 million people worldwide regularly chew BQ . Research findings by the International Agency for Research on Cancer have indicated that both added BQ (TA-BQ) and tobacco-free BQ (TF-BQ) are carcinogenic to humans . Carcinomas of the upper aerodigestive tract are the primary neoplasms associated with their consumption . Large-scale epidemiological studies have reported that prolonged TF-BQ use is related to obesity, metabolic syndrome and adverse pregnancy outcomes . In Cambodia, a nationwide investigation has shown an association between the intensity of TA-BQ use and HIV/AIDS, dengue fever and typhoid .
Arecoline, a stimulant with a chemical structure comparable to nicotine, is the principal alkaloid in the AN (containing up to 0.2%) . This active ingredient produces a high level of acetylcholine and monoamines (such as adrenaline and noradrenaline), and acts as an agonist at muscarinic acetylcholine receptors . Arecaidine is another active alkaloid in the AN, and acts by inhibiting the reuptake of gamma-amino butyric acid (GABA) to induce anxiolytic effects . Although these psychoactive alkaloids and nicotine (if tobacco-added) likely lead chewers to dependent BQ use, documentation regarding the symptoms and syndrome of BQ dependence (BQ-D) among tobacco-added,
tobacco-free and ingredient-specific BQ users is scant. One Indian study conducted among patients with psychiatric disorders and their relatives showed that 79.5% of TA-BQ chewers and 38.8% to 40.8% of TF-TA-BQ chewers have TA-BQ-D, and both groups of chewers exhibit withdrawal syndrome and endorsed attributes of desirable BQ use . Although the level of BQ-D was low among TF-BQ chewers in one Indian group, approximately 44% of the chewers endorsed at least one dependence-related symptom . Because BQ chewing has been associated with multidimensional health consequences, its dependent use conceivably creates a gateway toward various adverse outcomes. Investigating how the syndrome and the symptoms of BQ-D are associated with different BQ types and their added ingredients can facilitate an understanding of the factors affecting BQ addition and enable formulating intervention strategies for addiction cessation.
To investigate the BQ usage pattern and its associated health effects in Asian communities, and to assemble outreach activities for disease prevention, the Center of Excellence for Environmental Medicine at Taiwan Kaohsiung Medical University (KMU) and the WHO Collaborating Centre for Oral Cancer and Precancer in the United Kingdom launched the Asian Betel-Quid Consortium study in 2008. This research series has awakened the problems and challenges posed by BQ use . For this study, we focused on the issues of (1) evaluating the symptoms and syndrome of BQ-D among chewers who consumed various types of BQ products in six Asian populations using DSM-IV and ICD-10 criteria for substance use disorder , and (2) investigating chewer-related factors accounting for country-specific BQ-D.
Study sample
Six East, Southeast, and Southern Asian study groups, respectively, from KMU (Taiwan), Central South University (Mainland China), the University of Malaya (Malaysia), Airlangga University (Indonesia), the University of Peradeniya (Sri Lanka) and Kathmandu University (Nepal) participated in this joint cross-sectional investigation. The Ethical Review Committee at each study affiliation reviewed and approved the identical research proposal, which was applied in all study populations with the aim of a comparative framework.
The study method details are as follows . Using demographic data from census records and the household registry of individual participating countries, a multistage random-sampling approach was applied to select representative samples from the civilian, non-institutionalized population (aged 15 years) in each investigated community. Participant recruitment began in January 2009 and ended in February 2010. Prior to data collection, study purposes were explained well, and a written informed consent was obtained from each participant. This consortium recruited 1548, 2356, 1003, 1941, 1072 and 1002 participants, respectively, from Southern Taiwan, the Hunan Province of Mainland China, the Selangor, Sabah, and Sarawak States of Malaysia, North Sumatra, East Java, Bali, West Nusa Tenggara, South Sulawesi and the Papua provinces of Indonesia, the central province of Sri Lanka, and the middle of Nepal, with a high participant rate (68-100%). To focus on our research objectives, the study samples were confined to current BQ users (ranged from 74 to 839 participants, Table 1). BQ chewers were the subjects who had consumed at least one quid of any type of betel or areca nut product per day for a minimum of 6 months in the lifetime, and current BQ chewers were defined as participants who had chewed these products within the year prior to the interview.
Instrument and data collection
Survey items of sociodemographic profiles and other substance usages were developed using appropriate materials from WHO surveys and other national prevalence studies. BQ-D syndromes were measured by questions modified from the Structured Clinical Interview for DSM-IV-TR Axis I Disorders for Substance Use Disorders and Schedules for Clinical Assessment in Neuropsychiatry (SCAN) . We constructed a structured questionnaire to collect the needed information. The survey items were first written in English and then translated into the appropriate language for each study community. All items were back-translated into English to confirm content and semantic equivalence by bilingual specialists. The final interview was conducted in the local language.
After the study samples were drawn, the research teams conducted door-to-door visits to the participants’ homes to conduct the interviews. Before this work, interviewers were required to finish a training course for this project under the direction of principal investigators. Survey data were collected on demographics, anthropometric features and usage patterns for BQ, alcohol and tobacco consumption, including the starting age of use, quantities of daily consumption, years used, and the type and frequency of substance consumed. In the study areas, each type of BQ product contains fixed ingredients. To identify BQ type-specific ingredients, we created numerous pictograms to elicit the ingredients used in the BQ of each study area from the participants. We printed a pictogram of each type of BQ on the questionnaire to enable the interviewers to obtain data on BQ consumption. The final versions of the BQ pictograms were confirmed based on consensus obtained from each study center. Further, additional information was gathered on substance cessations, abuse conditions and current health.
and ICD-10 BQ-D. These include [1] Tolerance; [2] Withdrawal; [3] Larger intake: BQ is chewed in larger amounts or over a longer period than intended; [4] Unsuccessful cut-down: unsuccessful efforts to cut-down or control BQ use; [5] Time spent chewing: spending large amounts of time obtaining BQ or chewing BQ; [6] Giving up activities: reduction in important social, occupational or recreational activities because of BQ use; [7] Continued use despite problems: continued BQ chewing, despite the awareness of physical or psychological problems caused by chewing; and [8] Craving: a strong desire or sense of compulsion to take BQ.
A diagnosis of DSM-IV BQ-D required at least 3 of the domains [1]-[7] presented in the past 12 months, and a diagnosis of ICD-10 BQ-D required 3 or more of the domains [1]-[3], [5] and [7]-[8] presented in the 12-month period before the interview. BQ chewers who met either DSM-IV or ICD-10 diagnostic criteria were defined as those experiencing any BQ-D (aBQ-D). The 12-month BQ-D rate indicated the proportion of current chewers who were determined to have BQ-D according to the DSM-IV or ICD-10 criteria.
Statistical analysis
The study data was analyzed using Stata survey-data modules . All analyses, including means, percentages, standard errors, and regression modeling were conducted on weighted data that took multi-stage sampling design into account. Data analyses were focused on the difference of BQ-D domains and syndromes between chewers who consumed tobacco-added, tobacco-free and other specific types of BQ products within the same country. The discrepancy between TF-BQ chewers in Taiwan and Mainland China was also evaluated. For continuous and binary outcomes, we applied multiple linear and logistic regression models to assess covariate-adjusted mean
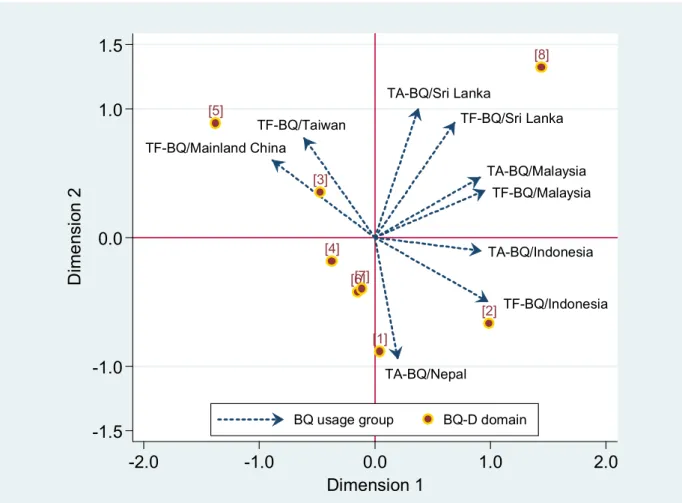
and proportional differences. Because the correlation structure between 8 BQ-D domains and 9 BQ usage groups investigated revealed a two-dimensional pattern, a two-dimensional biplot that concomitantly shows the relative positions of the variables was used to illustrate the relationship between BQ-D domains and BQ usage groups. The adjusted odds ratio (aOR) obtained from multivariate logistic regression models was used to measure the effect of demographic factors, chewing features and substance use on aBQ-D. To summarize these findings, meta-analytic methods were applied to calculate the pooled effect sizes and statistically analyze the collective data. We assessed inter-study heterogeneity using the Q statistic. Random-effect models were applied to the meta-analytic procedures to allow for all levels of heterogeneity, whether detectable in significance tests or not. Because a higher aBQ-D rate was detected in chewers who used TA-BQ than those who used TF-BQ in the Sri Lankan community (47.9% vs. 12.5%, P=0.001), the degree to which chewing characteristics explain the excess risk of aBQ-D in TA-BQ users as compared to TF-BQ users was appraised by computing the formula, (aOR1-aOR2)/(aOR1-1), where aOR1 is the aBQ-D risk for
TA-BQ chewers obtained from the gender, age, education, drinking and smoking-adjusted base model; aOR2 is the risk after additionally adjusting for chewing features; and
aOR1-1 is the excess risk of aBQ-D in TA-BQ users vs. TF-BQ users .
RESULTS
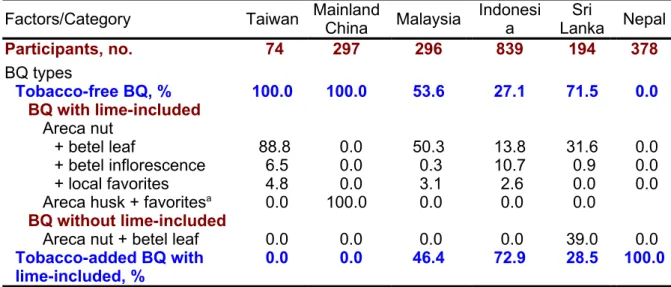
The type and ingredients of BQ chewed by the six study populations are shown in Table 1. All Chinese chewers consumed TF-BQ, with most Taiwanese users (88.8%) chewing a whole unripe AN wrapped with a piece of betel leaf of Piper betle pasted with slaked lime, whereas 100% of Mainland Chinese users chewed a halved dried husk of the areca fruit (not the solid AN) marinated with bittern (containing lime) and diverse flavored
additives, such as mint, cinnamon and orange flavors (supplementary Fig. 1). A higher percentage of chewers consumed TF-BQ (53.6-71.5%) more than TA-BQ (28.5-46.4%) in Malaysian and Sri Lankan communities. Conversely, a large proportion of chewers used TA-BQ (72.9%) compared to TF-BQ (27.1%) in Indonesian community. Sri Lankan chewers typically consume a ripe and dried AN (named Karunka), or an unripe AN soaked in a ditch or under water (named Madapuwak). Among the Sri Lankan TF-BQ users, more than half of the chewers used AN wrapped with a betel leaf, without lime. All Nepalese users chewed TA-BQ. Supplementary Table 1 shows the sociodemographic profiles and user features according to the major BQ type consumed for each chewer sample. Dissimilarities exist in the distribution of gender, age and educational level between BQ user groups, but these differences were considered during group comparisons.
The 12-month BQ-D rate defined by either DSM-IV or ICD-10 criteria among chewers was higher in Nepal and Indonesia (86.4-99.3%) than in Malaysia, Taiwan, Mainland China and Sri Lanka (12.5-51.3%, P<0.001, Table 2). On average, these chewer groups had 3.9-5.4 and 1.4-3.3 dependence domains, respectively. In Sri Lanka, the aBQ-D rate was appreciably greater in TA-BQ users than in TF-BQ users (47.9% vs. 12.5%, P=0.001). A higher percentage of Taiwanese TF-BQ chewers endorsed ‘tolerance’ and ‘craving’ than that declared by Mainland Chinese TF-BQ chewers. Among the Indonesian chewers, more TA-BQ users had dependence domains of ‘withdraw’ and ‘unsuccessful cut-down’, compared to TF-BQ users. In the Sri Lankan community, the fractions of individual domains for dependence were consistently greater among TA-BQ chewers than among TF-BQ chewers.
and Indonesian TA-BQ/TF-BQ chewers) were a cluster of users closely related to the dependence domains of ‘tolerance’ and ‘withdraw’ (lower right quadrant, Fig. 1). The BQ chewers from Sri Lanka and Malaysia formed another cluster that is more related to ‘craving’ (upper-right quadrant). The two Chinese TF-BQ users formed an independent cluster (upper-left quadrant) with ‘time spent chewing’ being the most important dependency domain (Table 2).
Table 3 shows the BQ-D rate among chewers who consumed different ingredient-included TF-BQ. To obtain robust results, we evaluated only BQ products used by a minimum of 5% of chewers. Aside from Sri Lanka, all TF-BQs were prepared with slaked limes. A higher aBQ-D rate was found in Taiwanese chewers who used unripe AN wrapped with betel leaf/inflorescence than that for Mainland Chinese chewers who used dried areca husk with favorites. Among the eight dependence domains, Taiwanese chewers endorsed more ‘craving’ and ‘tolerance’ than Mainland Chinese chewers. In Sri Lankan chewers, AN wrapped betel leaf with slaked limes conferred a higher rate of developing aBQ-D, compared to that without limes. The chewers who used lime-contained TF-BQ claimed more ‘unsuccessful cut-down’ than those who used TF-BQ without limes (39.1% vs. 5.6%, P=0.001).
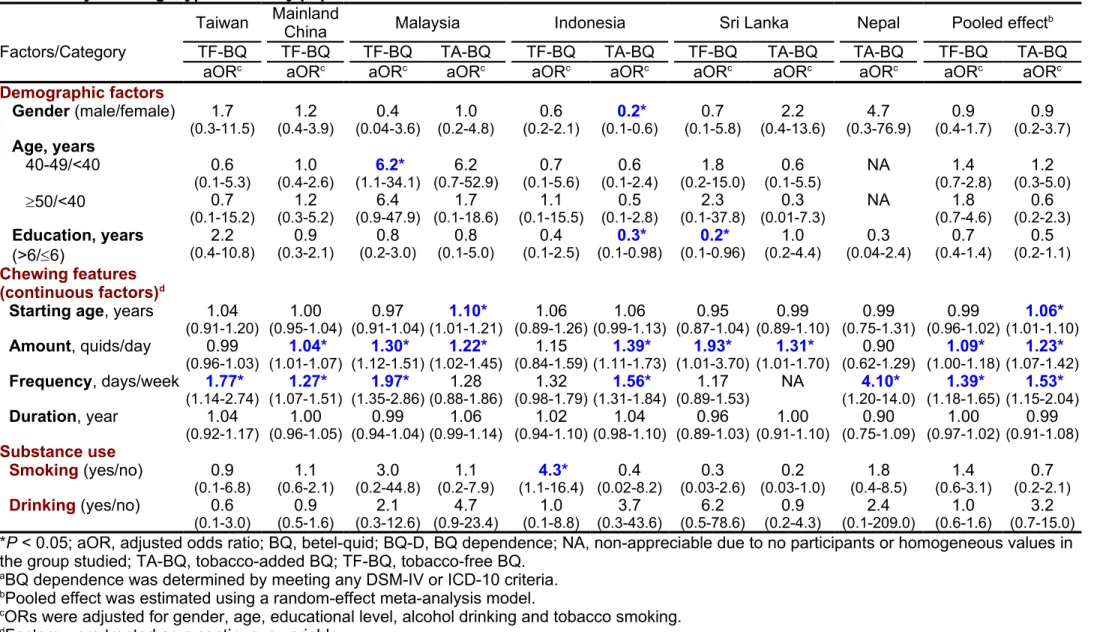
The effects of demographic factors, chewing patterns, and concomitant substance use on aBQ-D are shown in Table 4. In the Indonesian community, female TA-BQ users were more likely to develop dependence, whereas those with high educational achievement were less likely to have this syndrome. As shown in the combined results, the amount (aOR; 1.09 for TF-BQ and 1.23 for TA-BQ) and the frequency (aOR; 1.39 for TF-BQ and 1.53 for TA-BQ) of BQ consumption were the primary predictors of dependence. Among Mainland Chinese, Malaysian and Sri Lankan chewers, and Indonesian TA-BQ chewers, a one-quid increase in consumption was associated with a
1.04 to 1.93-fold risk of aBQ-D, whereas a one-day increase in the intake frequency was linked to a 1.27 to 4.10-fold dependence risk among TF-BQ chewers in Taiwan, Mainland China and Malaysia, and among TA-BQ chewers in Indonesia and Nepal. In Indonesian, a significant association between the concomitant use of cigarettes in TF-BQ chewers and aTF-BQ-D was found.
Because Sri Lankan TA-BQ chewers have shown a higher aBQ-D rate than TF-BQ chewers, we examined how chewing characteristics influence the disparity. The TA-BQ chewers had a 6.2-year earlier age at initiating BQ chewing than TF-BQ chewers (supplementary Fig. 2 and Table 5). However, this chewing feature only explained 9.6% of the excess risk of dependence in TA-BQ chewers. We observed similar findings for the duration of use. The average amount and frequency of BQ consumption in TA-BQ users were both higher than those in TF-BQ users. Of those, the quantity of BQ consumed accounted for 90.5% of the excess risk of aBQ-D.
DISCUSSION
Among the various ingredients used to prepare BQ, specific BQ products, particularly those with lime and tobacco added, contribute to BQ-D syndrome. We also found quantity and frequency to be two chewing characteristics closely related to BQ dependent use.
Several neuroactive alkaloids, including arecoline, arecaidine, guvacine and guvacoline, have been identified from the AN . Arecoline exerts neurobiological actions on numerous neurotransmitters (principally on cholinergic neurons) to affect the reactions of autonomic and central nervous systems . The physiological responses
reported by AN users are actually compatible to the neurobiological observations from this alkaloid . Alternatively, by way of the GABA reuptake restraint, arecaidine shows relaxation through its anxiolytic effects . In recent psychiatric investigations, chronic BQ users have clearly endorsed the dependence symptoms of tolerance and withdrawal . A case report of a pregnant woman with prolonged BQ consumption showed that not only arecoline was identified in her placenta, but further neonatal withdrawal syndrome was diagnosed in her infant .
Despite the varying BQ preparations, most chewers overwhelmingly use slaked lime-included BQ . This Asian cooperative study found that an appreciably higher proportion of chewers who consumed lime-containing TF-BQ developed aBQ-D (23.3%) than those who consumed lime-free TF-BQ (4.0%). Calcium hydroxide accelerates the extraction of AN-derived alkaloids during mastication, thus improving the psychoactive effects of these alkaloids on AN chewers . The existence of slaked lime, arecoline and guvacoline in AN could correspondingly be hydrolyzed into arecaidine and guvacine (two strong inhibitors of GABA uptake), and consequently exert GABAnergic functions . Our study found that such neurobiological actions were partially expressed in the dependence domain of ‘unsuccessful cut-down’, which was significantly endorsed by lime-containing TF-BQ users (39.1%, Table 3). Experimental studies have shown that AN-derived alkaloids are quickly absorbed into the buccal mucosa, and produce neurobiological activity within 5 minutes of administration and prolong for 15-20 minutes .
Our study showed that Taiwan and Hunan BQ chewers both significantly endorsed the dependency domain of ‘time spent chewing’. Because most BQ users were blue-collar workers (e.g., bus/taxi drivers), they typically chewed BQ for long-time to remain
attentive and to heighten alertness at work . We also found that Taiwanese chewers who used a whole unripe AN wrapped with a betel leaf/inflorescence have a higher dependence rate (46.1%) and endorse more ‘craving’ (40.5%) and ‘tolerance’ (27.1%) than Hunan chewers who used a halved dried areca husk (not the solid AN) with favorites (32.7%, 18.6% and 11.1%). Biomedical studies have indicated that betel leaf and inflorescence contain aromatic phenolic compounds that stimulate the release of catecholamines in vitro . These findings suggest that, compared with the areca husk, AN-contained BQ combined with betel leaf/inflorescence confers stronger neurobiological actions associated with craving and tolerance because these two dependence indicators were significantly endorsed by chewers of this BQ type.
Nepalese and Indonesian chewers were shown to have the highest aBQ-D rates (86.4-99.3%), and aggregately endorse the dependence domains of ‘tolerance’ and ‘withdrawal’ (Fig. 1). Because these two indicators are major biological modules for dependence syndrome , this partially explains why the highest aBQ-D rates were in this cluster.
Malaysian and Sri Lankan chewers endorsed craving as the major BQ-D indicator, which is supported by an appreciably higher proportion of TA-BQ users in Sri Lanka who reported more craving than that for TF-BQ users. TA-BQ users in an observational study in India were also detected to have higher craving than TF-BQ users after BQ abstinence (33.9-48.7% vs. 72.2-80.8%). These findings show craving to be an important indicator for BQ-D determination, particularly for TA-BQ use.
Epidemiological studies have shown that larger amounts of BQ consumption and increased intake frequency significantly predict the likelihood of developing BQ-D .
Comparable results were found in our multi-culture Asian populations, regardless of tobacco use. Using the modified Cigarette Dependence Scale and Smokeless Tobacco Dependence Scale to measure BQ-D, an Indian study showed that higher frequency of BQ chewing is positively correlated with severe dependence among TF-BQ users . In the Sri Lankan community, we found that chewing quantity and frequency explained the largest proportions of the excess risk of aBQ-D (36.4-90.5%) in TA-BQ users, compared to TF-BQ users. Similar findings were found among the BQ chewers in Malaysia and Indonesia (data not shown). Alternatively, because dependence risk for TA-BQ use was considerably attenuated by adjusting the amount of BQ consumed (5.1-fold significant risk reduced to 1.4-fold non-significant risk, Table 5), this chewing characteristic could act as an intermediate between the psychoactive effect of tobacco and the development of BQ-D in Sri Lankan chewers.
In our countries under study, BQ is a socially sanctioned substance, thus the degree of under-reporting of BQ dependent use and dependence symptoms among chewers should be limited. However, several limitations must be considered when interpreting the findings in this investigation. First, the cross-sectional findings only present a snapshot of the BQ-D degree among chewers and preclude clarifying causal, intermediate and non-causal scenarios. Second, the results should not be extended to other regions within individual countries because the pattern of BQ chewing may vary by region and cultural group. However, the study method and system could be applied to countries or areas where BQ chewing is widespread.
Given inadequate awareness and latent addictive effects of BQ use, screening for BQ-D is important for monitoring and preventive activities of BQ-related diseases. BQ-D is a multifaceted factor contributing to sustained BQ consumption, and is a principal syndrome associated with clinical managements of chewers. Understanding the
association of BQ ingredients and practice behavior with BQ-D symptoms and syndrome, as well as related genetic susceptibility , may enable the development of clinical therapy for addiction cessation.
In conclusions, tobacco additive increases the addictive potential of TA-BQ use. TF-BQ confers an independent effect on TF-BQ-D, which could act through the slaked lime additive to extract areca-derived alkaloids and exert their psychoactive dependence. Tolerance and withdrawal are the most important dependence symptoms among chewer groups with a high rate of BQ-D, and craving could be an indicator for BQ-D development.
ACKNOWLEDGMENTS
We would like to thank Jennifer Ko, the staff of the CEEM, for her great assistance in helping to organize the various centers’ principal investigators. We would also like to express our appreciation to the study staff members, including Bang-Liang Yin, Zhi-Wen Liu, Wen-Hui Li, Zhi-Wen Liu, Wen-Hui Li, Sanjeevani Jayshankar, Dipak Sapkota, Norain Abu Talib, Helen Ng Lee Ching, Tah Geok Mooi, Zaiton Tahir, Nurshaline Pauline Hj Kipli, Tian-You Ling, Ekamaya, Aris Istianah, SKM, Lutviana, Sriana Herman, Nuril, Taufig, Herman, and Arifin, for their diligent work and excellent endeavors in this international cooperative study.
REFERENCES
1. IARC Betel-quid and areca-nut chewing and some areca-nut derived nitrosamines, IARC Monogr Eval Carcinog Risks Hum 2004, 85, 1-334.
2. IARC A Review of Human Carcinogens: Personal Habits and Indoor Combustions, IARC Monogr Eval Carcinog Risks Hum 2012, 100E, 333-372. 3. MARSHALL, M. An overview of drugs in Oceania. In: Lindstrom L, editor. Drugs in
Western Pacific societies: relations of substance. Association for Social Anthropology in Oceania Monograph 11. Lanham (MD): University Press of America; p.15-21., 1987.
4. NORTON, S. A. Betel: consumption and consequences, J Am Acad Dermatol
1998, 38, 81-8.
5. BOUCHER, B. J. & MANNAN, N. Metabolic effects of the consumption of Areca
catechu, Addict Biol 2002, 7, 103-10.
6. GUPTA, P. C. & WARNAKULASURIYA, S. Global epidemiology of areca nut usage, Addict Biol 2002, 7, 77-83.
7. GUPTA, P. C. & RAY, C. S. Epidemiology of betel quid usage, Ann Acad Med Singapore 2004, 33, 31-6.
8. SECRETAN, B., STRAIF, K., BAAN, R., GROSSE, Y., EL GHISSASSI, F., BOUVARD, V.
et al. A review of human carcinogens--Part E: tobacco, areca nut, alcohol, coal smoke, and salted fish, Lancet Oncol 2009, 10, 1033-4.
9. KO, Y. C., HUANG, Y. L., LEE, C. H., CHEN, M. J., LIN, L. M. & TSAI, C. C. Betel
quid chewing, cigarette smoking and alcohol consumption related to oral cancer in Taiwan, J Oral Pathol Med 1995, 24, 450-3.
10. LEE, C. H., KO, Y. C., HUANG, H. L., CHAO, Y. Y., TSAI, C. C., SHIEH, T. Y. et al.
The precancer risk of betel quid chewing, tobacco use and alcohol consumption in oral leukoplakia and oral submucous fibrosis in southern Taiwan, Br J Cancer 2003, 88, 366-72.
11. LEE, C. H., LEE, J. M., WU, D. C., HSU, H. K., KAO, E. L., HUANG, H. L. et al.
Independent and combined effects of alcohol intake, tobacco smoking and betel quid chewing on the risk of esophageal cancer in Taiwan, Int J Cancer 2005, 113,
475-82.
12. CHIANG, S. L., CHEN, P. H., LEE, C. H., KO, A. M., LEE, K. W., LIN, Y. C. et al.
Up-regulation of inflammatory signalings by areca nut extract and role of cyclooxygenase-2 -1195G>a polymorphism reveal risk of oral cancer, Cancer
Res 2008, 68, 8489-98.
13. LEE, C. H., LEE, K. W., FANG, F. M., WU, D. C., SHIEH, T. Y., HUANG, H. L. et al.
The use of tobacco-free betel-quid in conjunction with alcohol/tobacco impacts early-onset age and carcinoma distribution for upper aerodigestive tract cancer, J
Oral Pathol Med 2011, 40, 684-692.
14. LEE, C. H., LEE, K. W., FANG, F. M., WU, D. C., TSAI, S. M., CHEN, P. H. et al. The
neoplastic impact of tobacco-free betel-quid on the histological type and the anatomical site of aerodigestive tract cancers, Int J Cancer 2012, 131, E733-43. 15. LIN, C. F., WANG, J. D., CHEN, P. H., CHANG, S. J., YANG, Y. H. & KO, Y. C.
Predictors of betel quid chewing behavior and cessation patterns in Taiwan aborigines, BMC Public Health 2006, 6, 271-8.
16. YANG, M. S., CHANG, F. T., CHEN, S. S., LEE, C. H. & KO, Y. C. Betel quid
chewing and risk of adverse pregnancy outcomes among aborigines in southern Taiwan, Public Health 1999, 113, 189-92.
17. YANG, M. S., LEE, C. H., CHANG, S. J., CHUNG, T. C., TSAI, E. M., KO, A. M. et al.
The effect of maternal betel quid exposure during pregnancy on adverse birth outcomes among aborigines in Taiwan, Drug Alcohol Depend 2008, 95, 134-9. 18. SINGH, P. N., NATTO, Z., YEL, D., JOB, J. & KNUTSEN, S. Betel quid use in relation
to infectious disease outcomes in Cambodia, Int J Infect Dis 2012, 16, e262-7. 19. LORD, G. A., LIM, C. K., WARNAKULASURIYA, S. & PETERS, T. J. Chemical and
analytical aspects of areca nut, Addict Biol 2002, 7, 99-102.
21. CHU, N. S. Effects of Betel chewing on the central and autonomic nervous
systems, J Biomed Sci 2001, 8, 229-36.
22. CHU, N. S. Neurological aspects of areca and betel chewing, Addict Biol 2002, 7,
111-4.
23. BENEGAL, V., RAJKUMAR, R. P. & MURALIDHARAN, K. Does areca nut use lead to
dependence?, Drug Alcohol Depend 2008, 97, 114-21.
24. BHAT, S. J., BLANK, M. D., BALSTER, R. L. & NICHTER, M. Areca nut dependence
among chewers in a South Indian community who do not also use tobacco,
Addiction 2010, 105, 1303-10.
25. LEE, C. H., KO, A. M., WARNAKULASURIYA, S., YIN, B. L., SUNARJO, ZAIN, R. B. et
al. Intercountry prevalences and practices of betel-quid use in south, southeast and eastern asia regions and associated oral preneoplastic disorders: An international collaborative study by asian betel-quid consortium of south and east Asia, Int J Cancer 2011, 129, 1741-51.
26. LEE, C. H., KO, A. M., WARNAKULASURIYA, S., LING, T. Y., SUNARJO, RAJAPAKSE, P.
S. et al. Population burden of betel quid abuse and its relation to oral premalignant disorders in South, Southeast, and East Asia: an Asian Betel-quid Consortium Study, Am J Public Health 2012, 102, e17-24.
27. LEE, C. H., KO, A. M., YEN, C. F., CHU, K. S., GAO, Y. J., WARNAKULASURIYA, S. et
al. Betel-quid dependence and oral potentially malignant disorders in six Asian countries, Br J Psychiatry 2012, 201, 383-391.
28. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (4th edn) (DSM-IV). APA, 1994.
29. World Health Organization. International Statistical Classification of Diseases and Related Health Problems (ICD-10). WHO, 1992.
30. First MB, Spitzer RL, Gibbon M, Williams JBW. Structured Clinical Interview for DSM-IV Axis I Disorders. American Psychiatric Press, 2005.
31. World Health Organization. Schedules for Clinical Assessment in Neuropsychiatry (SCAN). WHO, 1994.
32. STATACORP LP (2013) Stata Survey Data Reference Manual, Release 13
(College Station Texas: Stata Press Publication).
33. BRANCATI, F. L., KAO, W. H., FOLSOM, A. R., WATSON, R. L. & SZKLO, M. Incident
type 2 diabetes mellitus in African American and white adults: the Atherosclerosis Risk in Communities Study, JAMA 2000, 283, 2253-9.
34. LOPEZ-VILCHEZ, M. A., SEIDEL, V., FARRE, M., GARCIA-ALGAR, O., PICHINI, S. &
MUR, A. Areca-nut abuse and neonatal withdrawal syndrome, Pediatrics 2006, 117, e129-31.
35. SENN, M., BAIWOG, F., WINMAI, J., MUELLER, I., ROGERSON, S. & SENN, N. Betel
nut chewing during pregnancy, Madang province, Papua New Guinea, Drug
Alcohol Depend 2009, 105, 126-31.
36. CHU, N. S. Cardiovascular responses to betel chewing, J Formos Med Assoc
1993, 92, 835-7.
37. KO, Y. C., CHIANG, T. A., CHANG, S. J. & HSIEH, S. F. Prevalence of betel quid
chewing habit in Taiwan and related sociodemographic factors, J Oral Pathol
Med 1992, 21, 261-4.
38. HO, M. C. & WANG, C. K. The effect of betel nut chewing on contour and object
masking, Atten Percept Psychophys 2011, 73, 2583-93.
39. HO, M. C., CHANG, C. F., LI, R. H. & TANG, T. C. Attentional biases for betel nut
cues in heavy and light chewers, Psychol Addict Behav 2013, 27, 1044-9.
40. MIRZA, S. S., SHAFIQUE, K., VART, P. & ARAIN, M. I. Areca nut chewing and
dependency syndrome: is the dependence comparable to smoking? a cross sectional study, Subst Abuse Treat Prev Policy 2011, 6, 23.
Table 1 Types and ingredients of betel-quid (BQ) consumed in current-chewers, stratified by study population
Factors/Category Taiwan MainlandChina Malaysia Indonesia Lanka NepalSri
Participants, no. 74 297 296 839 194 378 BQ types Tobacco-free BQ, % 100.0 100.0 53.6 27.1 71.5 0.0 BQ with lime-included Areca nut + betel leaf 88.8 0.0 50.3 13.8 31.6 0.0 + betel inflorescence 6.5 0.0 0.3 10.7 0.9 0.0 + local favorites 4.8 0.0 3.1 2.6 0.0 0.0
Areca husk + favoritesa 0.0 100.0 0.0 0.0 0.0
BQ without lime-included
Areca nut + betel leaf 0.0 0.0 0.0 0.0 39.0 0.0
Tobacco-added BQ with
lime-included, % 0.0 0.0 46.4 72.9 28.5 100.0
Table 2 BQ dependence domains and syndromes among BQ chewers, stratified by BQ usage type and study population
Factors/Category Taiwan
Mainland
China Malaysia Indonesia Sri Lanka Nepal
TF-BQ n=74 TF-BQn=297 P a value TF-BQn=173 TA-BQn=123 P a value TF-BQn=250 TA-BQn=589 P a value TF-BQn=135 TA-BQn=59 P a value TA-BQn=378 Dependence domain, % [1] Tolerance 26.7 11.1 0.003 23.4 16.2 0.167 79.5 33.2 <0.001 6.8 22.6 0.042 99.3 [2] Withdrawal 22.7 18.1 0.709 65.2 68.4 0.561 91.0 88.4 0.390 5.1 18.6 0.045 99.3 [3] Larger intake 24.3 31.2 0.678 21.4 24.1 0.622 38.4 26.9 0.144 15.5 56.3 <0.001 0.0 [4] Unsuccessful cut-down 37.1 28.1 0.168 0.0 0.0 NA 57.3 66.9 0.227 20.9 53.0 0.001 99.3
[5] Time spent chewing 60.5 48.9 0.099 17.2 21.5 0.653 26.8 15.7 0.097 5.8 36.8 0.001 0.0
[6] Given up activities 33.6 24.6 0.110 13.9 9.1 0.130 81.3 79.2 0.480 5.9 10.1 0.643 0.0
[7] Continued despite problems 29.1 30.6 0.879 14.8 28.0 0.190 74.9 53.6 0.040 8.3 40.0 <0.001 93.3
[8] Craving 37.1 18.6 0.006 70.3 77.9 0.864 89.2 90.4 0.704 68.0 95.6 0.001 0.0
No. of domain,b meanSE 2.70.3 2.10.1 0.035 2.30.2 2.50.2 0.812 5.40.2 4.50.1 0.001 1.40.1 3.30.3 <0.001 3.90.03
Dependence syndrome, %
DSM-IV criteria 40.4 31.5 0.115 24.0 25.7 0.926 92.3 84.2 0.099 9.6 44.7 <0.001 99.3
ICD-10 criteria 35.0 24.3 0.221 36.8 49.2 0.413 88.0 61.7 0.004 10.1 47.9 <0.001 93.3
Both criteriac 33.1 23.0 0.138 22.7 23.6 0.740 87.7 59.5 0.005 7.3 44.7 <0.001 93.3
Any criteriad 42.4 32.7 0.178 38.0 51.3 0.392 92.6 86.4 0.212 12.5 47.9 0.001 99.3
*P < 0.05; BQ, betel-quid; NA, Non-appreciable; TA-BQ, tobacco-added BQ; TF-BQ, tobacco-free BQ.
aP values for proportional differences between Taiwanese and Mainland Chinese TF-BQ chewers, and between TF-BQ and TA-BQ chewers in
Malaysia, Indonesia and Sri Lanka, respectively. P values were adjusted for gender, age, year of schooling, alcohol drinking and tobacco smoking.
bThe number of those satisfying dependence domains [1] to [8].
cBQ dependence was determined by meeting both DSM-IV and ICD-10 criteria. dBQ dependence was determined by meeting any DSM-IV or ICD-10 criteria.
Table 3 BQ dependence syndrome and domains associated with diverse ingredients used by tobacco-free BQ chewers, stratified by study population
Taiwan Mainland China Indonesia Sri Lanka Malaysia
BQ with lime BQ with lime BQ with lime BQ withlime
BQ without
lime
BQ with lime
Factors/Category Areca fruit+
leaf/inflorescence Areca husk+ favorites Pa value AN+leaf AN+ inflorescence Pa
value AN+leaf AN+leaf
Pa value AN+leaf n=68 n=297 n=104 n=126 n=60 n=73 n=163 Dependence syndrome DSM-IV criteria 44.0% 31.5% 0.068 95.6% 87.6% 0.226 21.8% 0.0% 0.001b 25.0% ICD-10 criteria 38.1% 24.3% 0.034 94.8% 77.9% 0.051 17.9% 4.0% 0.002 38.7% Any criteriac 46.1% 32.7% 0.049 95.6% 88.3% 0.241 23.3% 4.0% 0.001 40.0% Significant domaind [1] Tolerance 27.1% 11.1% 0.006 [4] Unsuccessful cut-down 39.1% 5.6% 0.001 [8] Craving 40.5% 18.6% 0.001
AN, areca nut; BQ, betel-quid.
aP values for proportional differences between areca fruit chewers in Taiwan and areca husk chewers in Mainland China, and between
AN+leaf and AN+inflorescence chewers in Indonesia, and between BQ with and without lime chewers in Sri Lanka, respectively. P values were adjusted for gender, age, educational level, alcohol drinking and tobacco smoking.
bP value was calculated using the median unbiased estimates with the aid of exact logistic regression.
cBQ dependence was determined by meeting any DSM-IV or ICD-10 criteria.
Table 4 Effects of demographic factors, chewing features and concomitant substance use on BQ dependencea among BQ chewers,
stratified by BQ usage type and study population
Taiwan MainlandChina Malaysia Indonesia Sri Lanka Nepal Pooled effectb
Factors/Category TF-BQ TF-BQ TF-BQ TA-BQ TF-BQ TA-BQ TF-BQ TA-BQ TA-BQ TF-BQ TA-BQ
aORc aORc aORc aORc aORc aORc aORc aORc aORc aORc aORc
Demographic factors Gender (male/female) 1.7 (0.3-11.5) (0.4-3.9)1.2 (0.04-3.6)0.4 (0.2-4.8)1.0 (0.2-2.1)0.6 (0.1-0.6) 0.2* (0.1-5.8)0.7 (0.4-13.6)2.2 (0.3-76.9)4.7 (0.4-1.7)0.9 (0.2-3.7)0.9 Age, years 40-49/<40 0.6 (0.1-5.3) (0.4-2.6)1.0 (1.1-34.1) 6.2* (0.7-52.9)6.2 (0.1-5.6)0.7 (0.1-2.4)0.6 (0.2-15.0)1.8 (0.1-5.5)0.6 NA (0.7-2.8)1.4 (0.3-5.0)1.2 50/<40 0.7 (0.1-15.2) (0.3-5.2)1.2 (0.9-47.9)6.4 (0.1-18.6)1.7 (0.1-15.5)1.1 (0.1-2.8)0.5 (0.1-37.8)2.3 (0.01-7.3)0.3 NA (0.7-4.6)1.8 (0.2-2.3)0.6 Education, years (>6/6) (0.4-10.8)2.2 (0.3-2.1)0.9 (0.2-3.0)0.8 (0.1-5.0)0.8 (0.1-2.5)0.4 (0.1-0.98) 0.3* (0.1-0.96)0.2* (0.2-4.4)1.0 (0.04-2.4)0.3 (0.4-1.4)0.7 (0.2-1.1)0.5 Chewing features (continuous factors)d
Starting age, years 1.04
(0.91-1.20) (0.95-1.04)1.00 (0.91-1.04)0.97 (1.01-1.21) 1.10* (0.89-1.26)1.06 (0.99-1.13)1.06 (0.87-1.04)0.95 (0.89-1.10)0.99 (0.75-1.31)0.99 (0.96-1.02)0.99 (1.01-1.10) 1.06* Amount, quids/day 0.99 (0.96-1.03) (1.01-1.07) 1.04* (1.12-1.51) 1.30* (1.02-1.45) 1.22* (0.84-1.59)1.15 (1.11-1.73) 1.39* (1.01-3.70)1.93* (1.01-1.70) 1.31* (0.62-1.29)0.90 (1.00-1.18) 1.09* (1.07-1.42) 1.23* Frequency, days/week 1.77* (1.14-2.74) (1.07-1.51) 1.27* (1.35-2.86) 1.97* (0.88-1.86)1.28 (0.98-1.79)1.32 (1.31-1.84) 1.56* (0.89-1.53)1.17 NA (1.20-14.0)4.10* (1.18-1.65) 1.39* (1.15-2.04) 1.53* Duration, year 1.04 (0.92-1.17) 1.00 (0.96-1.05) 0.99 (0.94-1.04) 1.06 (0.99-1.14) 1.02 (0.94-1.10) 1.04 (0.98-1.10) 0.96 (0.89-1.03) 1.00 (0.91-1.10) 0.90 (0.75-1.09) 1.00 (0.97-1.02) 0.99 (0.91-1.08) Substance use Smoking (yes/no) 0.9 (0.1-6.8) (0.6-2.1)1.1 (0.2-44.8)3.0 (0.2-7.9)1.1 (1.1-16.4)4.3* (0.02-8.2)0.4 (0.03-2.6)0.3 (0.03-1.0)0.2 (0.4-8.5)1.8 (0.6-3.1)1.4 (0.2-2.1)0.7 Drinking (yes/no) 0.6 (0.1-3.0) (0.5-1.6)0.9 (0.3-12.6)2.1 (0.9-23.4)4.7 (0.1-8.8)1.0 (0.3-43.6)3.7 (0.5-78.6)6.2 (0.2-4.3)0.9 (0.1-209.0)2.4 (0.6-1.6)1.0 (0.7-15.0)3.2 *P < 0.05; aOR, adjusted odds ratio; BQ, betel-quid; BQ-D, BQ dependence; NA, non-appreciable due to no participants or homogeneous values in the group studied; TA-BQ, tobacco-added BQ; TF-BQ, tobacco-free BQ.
aBQ dependence was determined by meeting any DSM-IV or ICD-10 criteria. bPooled effect was estimated using a random-effect meta-analysis model.
cORs were adjusted for gender, age, educational level, alcohol drinking and tobacco smoking. dFactors were treated as a continuous variable.
Table 5 Adjusted odds ratios of BQ dependence and excess risk explained by chewing characteristics in Sri Lankan chewers
Factors/Category TF-BQ
n=135
TA-BQ n=59
P
for diff.a TA-BQ vs. TF-BQ Excess riskaORa (95% CI) explainedb
Dependence syndrome,c 12.5% 47.9% <0.001 5.1 (2.0-13.0) Reference
(base-model) Chewing features,
meanse
Starting age, year 31.11.4 24.91.6 0.001 4.7d (1.9-12.1) 9.6% Amount, quid/day 2.00.2 6.60.7 <0.001 1.4d (0.4-4.5) 90.5% Frequency, day/week 4.70.3 6.90.1 <0.001 3.6d (1.5-9.0) 36.4% Duration, year 19.61.7 31.42.3 <0.001 4.8d (1.9-12.1) 9.4% aOR, adjusted odds ratio; BQ, betel-quid; TA-BQ, tobacco-added BQ; TF-BQ, tobacco-free BQ.
aP values for proportion or mean differences and odds ratios were adjusted for gender, age,
year of schooling, alcohol drinking and tobacco smoking.
bExcess risk of BQ dependence in TA-BQ users explained by the chewing feature investigated. cBQ dependence was determined by meeting any DSM-IV or ICD-10 criteria.
Figure 1 Two-dimensional biplot of betel-quid dependence (BQ-D) domains and BQ
usage groups.
Note: Circles denote the eight BQ-D domains and arrows denote the nine BQ usage
groups. The BQ-D domains include [1] Tolerance, [2] Withdrawal, [3] Larger, [4] Unsuccessful cut down, [5] Time spent chewing, [6] Given up activities, [7] Continued despite problems and [8] Craving.
[1] [2] [3] [4] [5] [6][7] [8] TF-BQ/Mainland China TF-BQ/Taiwan TA-BQ/Sri Lanka TF-BQ/Sri Lanka TA-BQ/Malaysia TF-BQ/Malaysia TA-BQ/Indonesia TF-BQ/Indonesia TA-BQ/Nepal -1.5 -1.0 0.0 1.0 1.5 D im e ns io n 2 -2.0 -1.0 0.0 1.0 2.0 Dimension 1