Long-term Health Outcomes of Chronic Hepatitis C Patients: a Review of Findings from REVEAL-HCV Cohort Study
Mei-Hsuan Lee, PhD., Hwai-I Yang, PhD., Chien-Jen Chen, Sc.D., for the R.E.V.E.A.L.-HCV Study Group*
From the Genomics Research Center, Academia Sinica, Taipei, (M.-H.L., H.-I.Y., C.-J.C.); the Molecular and Genomic Epidemiology Center, China Medical University Hospital, Taichung (H.-I.Y.); the Graduate Institute of Clinical Medical Science, China Medical University, Taichung (H.-I.Y.); and the Graduate Institute of Epidemiology, College of Public Health, National Taiwan University, Taipei, (C.-J.C.) all in Taiwan.
*Other members of the Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-Hepatitis C Virus (R.E.V.E.A.L.-HCV) study are listed in the Appendix
Corresponding Author: Prof. Chien-Jen Chen, Genomics Research Center, Academia Sinica, 128 Academia Road Section 2, Nankang, Taipei 11529, Taiwan. E-mail: [email protected]
Abstract
Chronic hepatitis C affects more than 180 million people worldwide. As one of the most important infectious diseases, it caused around 250,000 deaths per year. The long-term follow-up cohort study is essential for evaluating health outcomes associated with virus infection, and for exploring potential seromarkers which have high predictability for risk of developing various diseases. However, the prospective cohorts consisted of individuals with chronic HCV infection are still rare. The Risk Elevation of Viral Load Elevation and
Associated Liver Disease/Cancer in HCV (R.E.V.E.A.L.-HCV) study has followed a cohort of 1095 anti-HCV seropositive residents lived in seven townships in Tiawan for fifteen years. These anti-HCV seropositives were asymptomatic and relatively healthy than chornic
hepatitis C patients cared in clinics and hospitals. Most of them acquired HCV infection through iatrogenic transmission routes in study townships. The epidemiological
characteristics of HCV infection was very similar to those in countries with high prevalence such as Japan, Korea, Italy and India. As the participants in the R.E.V.E.A.L.-HCV study rarely received antiviral therapies, it provided an exceptional opportunity to study the natural history of chronic HCV infection. In this review article, we describe the details of participant enrollment, laboratory tests, follow-up procedures, and major recent findings. Anti-HCV seropositives with elevated serum HCV RNA levels were found to have an increasing risk of developing hepatocellular carcinoma in a dose-response relationship. In addition to the serum HCV RNA level, serum alanine aminotransferase levels and HCV genotype also had long-term predictability for the risk of hepatocellular carcinoma. Moreover, anti-HCV
seropositives with detectable serum HCV RNA levels had an increased mortality from extrahepatic diseases such as cerebrovascular and renal diseases. Our study revealed anti-HCV seropositives with detectable serum anti-HCV RNA levels had an increased risk of hepatic and extrahepatic diseases.
Hepatitis C virus (HCV) is recognized as a major cause of chronic liver disease. Liver cirrhosis eventuates in 20 to 30% patients with chronic HCV infection after 2 to 3 decades generally.1 Once cirrhosis occurs, hepatocellular carcinoma develops in 1 to 4% of theses patients per year.2 HCV was estimated to be attributable to one third of hepatocellular carcinoma cases globally,3 representing a great public health burden. Because its vaccine is not available and treatment options are still limited and expensive , the efforts of infection controls should be focused on the primary prevention. A long-term follow-up cohort may help evaluate the incidence and mortality of various diseases associated with chronic HCV infection. In this review article, we describe the study population, enrollment and follow-up procedures, recent findings and future perspectives of Risk Elevation of Viral Load Elevation and Associated Liver Disease/Cancer in HCV (R.E.V.E.A.L.-HCV) study.
R.E.V.E.A.L.-HCV Study Cohort
The R.E.V.E.A.L.-HCV study cohort was recruited from a community-based cancer screening program conducted in Taiwan during 1991-1992. There were seven townships selected as the study areas, including two northern townships (Sanchi and Chutung) and two southern townships (Potzu and Kaohsu) on main Taiwan Island, and three townships
(Makung, Huhsi, and Paihsa) on Penghu Islets.
There were 89,293 inhabitants aged 30-65 years old in the seven study townships invited to participate in the study, and 23,820 (11,973 males and 11,847 females) were enrolled with written informed consents. The vital status of the study participants were followed by the computerized linkage with the national cancer registration and death certification profiles. The nationalidentification number, date at birth, and sex were used as the linkingvariables to double-check the vital status and causes of deathof study participants. At the enrollment, the participants were personally interviewed using structured questionnaires by well trained
public health nurses. The information collected included the sociodemographic characteristics (age, sex, educational levels, occupation, etc.), habits of life styles (cigarette smoking,
alcohol consumption, and betel nut chewing), and personal and family history of major diseases. Anthropometric measurements including weight and height were also performed.
In addition to the questionnaire interview, the 10 mL blood samples were collected from each participant at study entry. The blood samples were obtained using disposable needles and heparinized vacuum syringes. They were fractioned on the day of collection and stored at -70C until assayed. Serum samples of all participants were tested for HBsAg by
radioimmunoassay (Abbott Laboratories, North Chicago, IL, USA), anti-HCV by enzyme immunoassay (Abbott Laboratories), serum levels of aspirate aminotransferase (AST) and alanine aminotransferase (ALT) by serum chemistry autoanalyzer (Model 736, Hitachi, Tokyo, Japan) using commercial reagents (Biomerieux, Marcy L’Etoile, France).
Participants who were seropositive for anti-HCV were further examined for serum HCV RNA levels by polymerase chain reaction using the COBAS TaqMan HCV test, v2.0 (Roche Diagnostics, Indianapolis, NJ, USA), an in vitro nucleic acid amplification test for the
quantification of HCV RNA. The quantification method used the high pure system viral nucleic acid kit for manual specimen preparation and the COBAS TaqMan 48 Analyzer for automated amplification and detection. The manufacturer’s procedures for sample
preparation to extract HCV RNA, automated reverse transcription of the target RNA to generate complementary DNA, and amplification of target cDNA were followed. In any test procedure, a replicate of negative, low-positive, and high-positive controls were included in each run for HCV RNA quantification. The HCV RNA titer was expressed in International Units (IU)/mL according to the WHO International Standard for HCV RNA NAT assays, and the linear range for the COBAS TaqMan HCV test was from 25 to 3.9108 IU/mL.
by melting curve analysis, which could effectively differentiate different HCV genotypes by showing different melting temperatures.4 In the R.E.V.E.A.L.-HCV study, the HCV
genotype-1 and HCV genotype non-1 were differentiated.
Participants seropositive for HBsAg or anti-HCV were invited to receive regular health examinations. The health examinations included abdominal ultrasonography examinations and blood tests. The certified hepatologists performed the high-resolution real-time
abdominal ultrasonography and interpreted according to a standardized protocol. Liver cirrhosis was determined based on a quantitative scoring system which was derived from the appearance of liver surface (normal, irregular, undulated), liver parenchymal texture (normal, heterogeneous, coarse), intrahepatic blood vessel size (normal, obscure, narrowing) and splenic size (normal, enlarged). The serological tests included serum levels of AST, ALT and -fetoprotein. To ensure all study participants received standard care, those who had
abnormal serum levels of ALT and/or -fetoprotein levels and ultrasonographic findings were referred to hepatologists in medical centers for further clinical managements.
There were 1095 participants seropositive for anti-HCV but seronegative for HBsAg. Among them, 975 (89%) had adequate retrievable serum samples for HCV RNA test. Comparing those who had adequate serum samples (n=975) and those without adequate serum samples for HCV RNA test (n=120), there were no significant differences in the distributions of baseline characteristics except for gender. However, for the 975 anti-HCV seropositives with adequate samples for HCV RNA test, the proportion of gender was similar to that of all 1,095 anti-HCV seropositives.
Seroprevalence of Anti-HCV by Age and Gender
There were 1313 participants seropositive for anti-HCV, giving the seroprevalence of 5.5% in our study population. The seroprevalence increased with the advanced age. For
females, the seroprevalence of HCV was 3.0%, 3.6%. 4.2%, 6.8%, 7.3%, 9.7% and 9.8%, respectively, for the age group of 30-34, 35-39, 40-44, 45-49, 50-54, 55-59, and 60-65 years old. The corresponding seroprevalence for males was 2.7%, 3.7%, 3.2%, 5.2%, 5.6%, 6.4%, and 6.1%, respectively. As shown in Figure 1, females had higher age-specific anti-HCV seroprevalence than males with the overall seroprevalence of 6.2% vs. 4.8%, respectively,
The major risk factors of HCV infection in the R.E.V.E.A.L.-HCV study population were iatrogenic risk factors including blood transfusion, hemodialysis, medical injections and dental procedures. In our previous reports, more than 80% HCV infection could be
attributable to iatrogenic factors.5,6 People with older age had an increased chance to receive
multiple medical injections and had an increased cumulative risk of HCV infection in their lifetime. The gender difference in the seroprevalence of HCV infection might be expalined by 1) Females might be more concerned about their minor illness and more likely to receive the glucose-based nutrient or vitamin injections than males, which were frequently prescribed to sick people; or 2) Males infected with HCV might have a higher mortality rate than infected females, thus the anti-HCV prevalence in males would more likely to be lower than females due to a faster attrition of the HCV-infected.7
HCV RNA Seropositive Rate and its Associated Baseline Characteristics
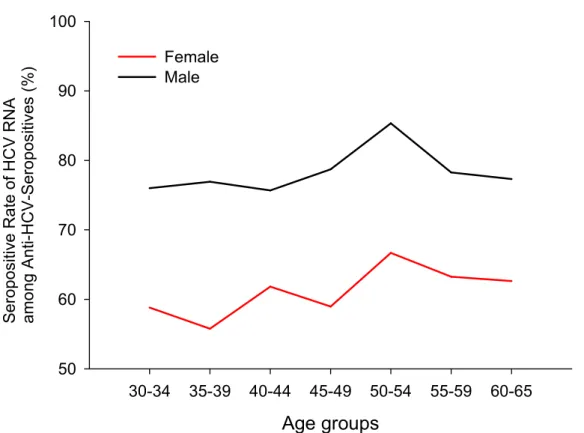
Serum HCV RNA level was undetectable in 299 (30.7%) and detectable in 676 (69.3%) anti-HCV seropositives in the R.E.V.E.A.L.-HCV study cohort. Table 1 shows the HCV RNA seropositive rate by baseline characteristics. The HCV RNA seropositive rate was 78.8% in males and 62.0% in females, suggesting females were more likely to have
spontaneous seroclearance of HCV RNA. Participants with the habit of cigarette smoking or alcohol consumption had a higher HCV RNA seropositive rate than those without the habit. However, the associations might result from the higher proportions of cigarette smokers and
alcohol drininkers in males than females. After adjustment for gender, there was no
association between the HCV RNA seropositivity and habits of cigarette smoking and alcohol drinking. There was no significant association with HCV RNA seropositivity for body mass index (BMI) and history of diabetes.
Participants with increasing serum ALT levels had elevated HCV RNA seropositive rates. In comparison to those with serum ALT levels 15 U/L as the referent, the sex-adjusted odds ratio (95% confidence interval) of having detectable serum HCV RNA levels was 3.69 (2.69-5.06) and 10.18 (5.58-18.60), respectively, for serum ALT levels of 15-45 U/L and higher than 45 U/L. Males had a 2.26 folds (95% confidence interval, 1.66-3.07) risk of having detectable serum HCV RNA levels after adjustment for serum ALT levels. It is interesting to note that females had a higher anti-HCV seroprevalence as shown in Figure 1, but a lower HCV RNA seropositive rate among anti-HCV seropositives than males as shown in Figure 2. It suggests the serum HCV RNA level might be a seromarker to be considered in
management of anti-HCV seropositives. However, the importance and significance of this seromarker should be further evaluated by comparing the health outcomes between HCV RNA seronegative and seropositive participants who were seropositive for anti-HCV.
Incidence of Hepatocellular Carcinoma by Baseline Characteristics
There were 101 newly developed HCC cases occurred after 17,944 person-years of follow-up, giving the incidence rate of 562.9 per 100,000 person-years. Table 2 shows the number of participants, person-years of follow-up, number of HCC cases, and the incidence rate of HCC by baseline characteristics. Individuals with older age, habit of cigarette smoking or alcohol consumption, increased BMI (25 kg/m2), elevated serum ALT levels and
detectable serum HCV RNA levels had an increased incidence of HCC among the 1,095 anti-HCV seropositives who were seronegative for HBsAg. The baseline characteristics which
were significantly associated with increased HCC risk in univariate analyses were included in the subsequent multivariate analyses. Participants with older age, habit of cigarette smoking and alcohol consumption, increased BMI still had a significantly increased HCC risk after adjustment for each other. But no significant association was observed for habit of cigarette smoking and alcohol consumption after further adjustment for serum levels of ALT and HCV RNA.
In comparison to those with serum ALT levels 15 U/L as the referent group, the adjusted-hazard ratio (95% confidence interval) was 1.78 (1.01-3.14) and 2.98 (1.65-5.40), respectively, for serum ALT levels of 16-44 U/L and 45 U/L. Individuals with detectable serum HCV RNA level had 5.67 times risk to occur HCC than those with undetectable HCV RNA levels. In our recent study, we found that serum levels of ALT and HCV RNA and HCV genotype had long-term predictability for HCC. These seromarkers had predictability five years or earlier than the occurrence of HCC After 15 years of follow-up, the cumulative HCC risk was only 0.4% for participants seronegative for anti-HCV. There was an increasing cumulative HCC risk for anti-HCV-seropositive participants with undetectable, low and high serum HCV RNA levels (1.1%, 6.4% and 14.7%, respectively, p<0.001 for trend). Among participants seropositive for anti-HCV, the cumulative HCC risk was 1.7%, 4.2%, and 13.8% for serum ALT levels of persistently 15 U/L, ever >15 but never >45 U/L, and ever 45 U/L, respectively (p<0.001 for trend). Among participants with detectable serum HCV RNA levels, the cumulative HCC incidence was 12.6% for HCV genotype 1 and 4.5% for genotype non-1 (p<0.001).8 Moreover, the increasing HCC risk by the elevating serum levels of HCV RNA was found not only in men but also in women.9
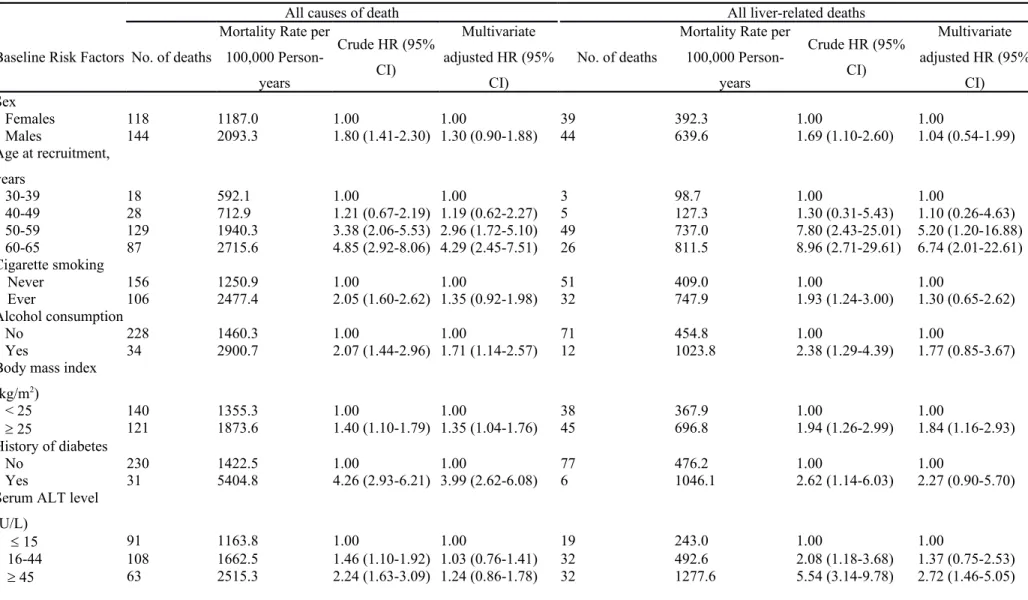
All Causes and Liver-related Mortality by Baseline Characteristics
for each baseline characteristic. The all-causes mortality rate was 1557.7 per 100,000 person-years and the liver-related mortality rate was 493.5 per 100,000 person-person-years, respectively. The cumulative mortality from all causes of death was 30.1% and 12.8% after 17 years of follow-up for participants with detectable and undetectable serum HCV RNA levels, respectively. Similarly, those with detectable serum HCV RNA levels had an increased cumulative mortality from liver-related diseases compared with those with undetectable serum HCV RNA levels, with the cumulative mortality of 12.8% and 1.6%.10 Generally, male gender, older age, habits of cigarette smoking and alcohol consumption, BMI 25 kg/m2,
history of diabetes, elevated serum ALT levels, and detectable serum HCV RNA levels were associated with an increased mortality form all-causes and liver-related deaths. After
adjustment for potential risk factors, participants with detectable serum HCV RNA levels had an increased risk for all-causes of death and hepatic-related deaths with the adjusted hazard ratio (95% confidence interval) of 2.78 (1.56-3.33) and 6.53 (2.32-18.37), respectively. It implies that participants with detectable serum HCV RNA levels might die from other extrahepatic diseases in addition to hepatic diseases. Our findings indicated the serum HCV RNA level was an important marker for management of individuals seropositive for anti-HCV.
HCV Infection and Deaths from Extrahepatic Diseases
The mortality from extrahepatic diseases was 1064.2 per 100,000 person-years for the participants in R.E.V.E.A.L.-HCV cohort. Among participants seronegative for HBsAg, the cumulative mortality from extrahepatic diseases after 17 years of follow-up was 12.2% for anti-HCV seronegatives and 17.7% for anti-HCV seropositives, respectively. In other words, participants seropositive for anti-HCV had 1.4 folds risk of dying from extrahepatic diseases after adjustment for age and sex. Anti-HCV seropositives had an increased mortality from
either extrahepatic cancers or extrahepatic diseases other than cancers with age-sex-adjusted hazard ratio (95% confidence interval) of 1.23 (0.92-1.65) and 1.43 (1.19-1.73), respectively. Figure 3 shows the associations between extrahepatic deaths and HCV infection. The HCV infection was associated with an inceased mortality from circulatory diseases. Based on the long-term follow-up design of R.E.V.E.A.L.-HCV study, there was a correct causal
temporality for the HCV-induced atherosclerotic diseases.11 Moreover, the increasing serum HCV RNA levels were found to be associated with the mortality from cerebrovascular disease in a dose-response relationship after adjustment for conventional risk factors for cerebrovascular disease. Compared with participants seronegative for anti-HCV as the referent group, the multivariate-adjusted hazard ratio (95% confidence interval) of dying from cerebrovascular disease was 1.43 (0.63-3.23), 2.29 (1.38-3.82) and 2.81 (1.25-6.35), respectively, for anti-HCV-seropositive participants with undetectable, low and high serum levels of HCV RNA (p<0.001 for trend). However, there was no significant association between HCV genotype and mortality from cerebrovascular disease.12 In addition, HCV infection was associated with an increased mortality from renal disease and cancers of the esophagus, prostate, and thyroid cancer; and the mortality was even higher for those with detectable serum levels of HCV RNA.10
Advantages and Limitations of R.E.V.E.A.L.-HCV Study
Chronic hepatitis C patients in Taiwan rarely received antiviral treatment with interferon due to its high cost and adverse effects until November 2003, when patients with abnormal serum ALT levels (>82 U/L) and moderate fibrosis proven by liver biopsy could be
reimbursed for treatment by the National Health Insurance. Therefore this cohort study may be considered as a natural history study of chronic hepatitis C. To ensure study participants to receive standard care, those who had abnormal serum levels of ALT and -fetoprotein or
abnormal ultrasonographic findings were referred to medical centers for further clinical managements in this study. This cohort consisted of 1,000 anti-HCV seropositives provided an exceptional opportunity to examine the seromarker changes and liver disease occurrence of anti-HCV seropositives during the natural course of HCV infection.
The R.E.V.E.A.L.-HCV cohort enrolled participants lived in the community. Unlike other cohorts enrolled patients with experiences of drug injections13 or HCV-contaminated vaccinations,14,15 the exact time of HCV infection was unavailable for our participants. As the
major risk factors of HCV infection in the R.E.V.E.A.L.-HCV cohort were iatrogenic factors, it was difficult to obtain the exact time at HCV infection, the information on advanced fibrosis or mild cirrhosis was not available in this community-based cohort because it is not practical to have the asymptomatic participants examined by liver biopsy. Liver cirrhosis is an intermediate clinical outcome before the occurrence of HCC among chronic hepatitis C patients. Based on the abdominal ultrasonographic examination and serial tests of serum levels of AST and ALT, more than 80% of newly-developed HCC cases in participants seropositive for anti-HCV had liver cirrhosis detected by ultrasonography and/or an increased ratio between serum levels of AST and ALT.
Summary
Based on R.E.V.E.A.L.-HCV cohort study, we found that anti-HCV seropositives with detectable serum HCV RNA levels had an increased risk of both hepatic and extrahepatic diseases. Anti-HCV seropositives with undetectable serum HCV RNA levels had cumulative HCC risk similar to anti-HCV seronegatives (1.1% vs. 0.4%), implying antiviral treatment to seroclear HCV RNA may have benefits to patients. In addition, the findings suggests clinical patients experienced sustained virologic response after receiving antiviral therapy may have reduced HCC risk and improved survival.16 Recent trials showed use of direct-acting antiviral
agents may achieve sustained virologic response among patients who had not had a response to prior therapy.17,18 Our study provides evidence that patients with HCV infection, particular
for those with active HCV infection (seropositive for HCV RNA), should be encouraged for intensive management because they had an increased risk of HCC and mortality from hepatic or extrahepatic diseases. We also found the prevalence of anti-HCV in a community was associated with HCV RNA seropositive rate among anti-HCV seropositives in the community, suggesting anti-HCV seropositives with detectable serum HCV RNA levels played a major role in the transmission of the virus in the community.7 For the control of hepatic or extraheptic diseases and virus infection, anti-HCV seropositives should be tested for serum HCV RNA levels by a sensitive assay. Those with active HCV infection should be instructed to be aware of HCV-related health outcomes and HCV transmission routes as well as the need to take actions for HCV RNA seroclearance.
Future Perspectives
Recently, human genetic variants predicting successful treatments have been identified by genome-wide association study (GWAS) from several independent study groups.19-21 They studied different ethnic populations and found genetic variants near IL28B gene were
associated with antiviral response in patients infected with HCV genotype 1. Two single nucleotide polymorphisms (SNPs) near gene interleukin 28B (IL28B, also called IFN3), rs12979860 and rs8099917, were associated with antiviral treatment response in chronic hepatitis C patients.19-21 The C allele of the SNP (rs12979860) was found to be associated with the spontaneous clearance of HCV in a follow-up study.22 These findings imply host genetic factors may be involved in the natural course of HCV infection and the pathogenesis of liver diseases. IL28B polymorphism (T allele) seems to be involved in the development of HCV-induced HCC and the course of HCV recurrence after liver transplantation in a recent
study.23 In Taiwan, most chronic hepatitis C patients carried the favorable genotype
associated with better treatment responses and the minor allele frequency (T of rs12979860 and G of rs8099917) were very rare.24-26 To better understand the associations between the SNPs near IL28B and the risk of liver cirrhosis or HCC, a study with a large sample size is needed. Moreover, host genetic variants other than IL28B might also be associated with liver diseases in chronic hepatitis C patients. It will be interesting to discover these genetic variants to further understand the pathogenesis of liver disease progression or to apply them as
diagnostic or risk predictive biomarkers. Although high-throughput technologies to discover human genetic variants have developed rapidly to accelerate the genotyping, validation of genetic markers in other external populations is still essential and functional studies are needed. Collaborative studies to better understand the diseases associated with HCV infection and to promote appropriate clinical managements of chronic hepatitis C patients are in urgent need.
Appendix
Other Members of the R.E.V.E.A.L.-HCV Study Group: National Taiwan University Hospital: C. Y. Hsieh, H.S. Lee, P. M. Yang, C. H. Chen, J. D. Chen, S. P. Huang,
C. F. Jan. National Taiwan University: T. H. H. Chen. National Defense Medical Center: C. A. Sun. Taipei City Psychiatric Center: M. H. Wu. Tzu Chi University: S. Y. Chen. Shin Kong Wu Ho-Su Memorial Hospital: K. E. Chu. Huhsi Health Center,
Penghu County: S. C. Ho, T. G. Lu. Provincial Penghu Hospital:W. P.Wu, T. Y. Ou. Sanchi Health Center, Taipei County: C. G. Lin. Provincial Chutung Hospital: K. C. Shih. Provincial Potzu Hospital: W. S. Chung, C. Li. Kaohsu Health Center, Pingtung County: C. C. Chen. Paihsa Health Center, Penghu County: W. C. How.
REFERENCES
1. Lauer GM, Walker BD. Hepatitis C virus infection.[see comment]. N Engl J Med. 2001;345(1):41-52.
2. Fattovich G, Stroffolini T, Zagni I, Donato F. Hepatocellular carcinoma in cirrhosis: Incidence and risk factors. Gastroenterology. 2004;127(5):S35-S50.
3. Parkin DM. The global health burden of infection-associated cancers in the year 2002. Int J Cancer. 2006;118(12):3030-3044.
4. Yeh SH, Tsai CY, Kao JH, et al. Quantification and genotyping of hepatitis B virus in a single reaction by real-time PCR and melting curve analysis. J Hepatol.
2004;41(4):659-666.
5. Sun CA, Chen HC, Lu CF, et al. Transmission of hepatitis C virus in Taiwan: prevalence and risk factors based on a nationwide survey. Journal of Medical Virology. 1999;59(3):290-296.
6. Sun CA, Chen HC, Lu SN, et al. Persistent hyperendemicity of hepatitis C virus infection in Taiwan: the important role of iatrogenic risk factors. Journal of Medical Virology. 2001;65(1):30-34.
7. Lee MH, Yang HI, Jen CL, et al. Community and personal risk factors for hepatitis C virus infection: a survey of 23,820 residents in Taiwan in 1991-2. Gut.
2011;60(5):688-694.
8. Lee MH, Yang HI, Lu SN, et al. Hepatitis C virus seromarkers and subsequent risk of hepatocellular carcinoma: long-term predictors from a community-based cohort study. J Clin Oncol. 2010;28(30):4587-4593.
9. Huang YT, Jen CL, Yang HI, et al. Lifetime risk and sex difference of hepatocellular carcinoma among patients with chronic hepatitis B and C. J Clin Oncol.
2011;29(27):3643-3650.
10. Lee MH, Yang HI, Lu SN, et al. Chronic hepatitis C virus infection increases mortality from hepatic and extrahepatic diseases: a community-based long-term prospective study. Journal of Infectious Diseases. 2012. (in press)
11. Lee MH, Yang HI, Wang CH, Chen CJ. Response to Letter by Lin et al Regarding Article, "Hepatitis C Virus Infection and Increased Risk of Cerebrovascular Disease". Stroke. 2011;42(6):e390-e391.
12. Lee MH, Yang HI, Wang CH, et al. Hepatitis C virus infection and increased risk of cerebrovascular disease. Stroke. 2010;41(12):2894-2900.
13. Hisada M, Chatterjee N, Kalaylioglu Z, Battjes RJ, Goedert JJ. Hepatitis C virus load and survival among injection drug users in the United States. Hepatology.
2005;42(6):1446-1452.
14. Wiese M, Berr F, Lafrenz M, Porst H, Oesen U. Low frequency of cirrhosis in a hepatitis C (genotype 1b) single-source outbreak in germany: a 20-year multicenter study. Hepatology. 2000;32(1):91-96.
15. Wiese M, Grungreiff K, Guthoff W, Lafrenz M, Oesen U, Porst H. Outcome in a hepatitis C (genotype 1b) single source outbreak in Germany--a 25-year multicenter study. J Hepatol. 2005;43(4):590-598.
16. Velosa J, Serejo F, Marinho R, Nunes J, Gloria H. Eradication of hepatitis C virus reduces the risk of hepatocellular carcinoma in patients with compensated cirrhosis. Dig Dis Sci. 2011;56(6):1853-1861.
17. Lok AS, Gardiner DF, Lawitz E, et al. Preliminary study of two antiviral agents for hepatitis C genotype 1. N Engl J Med. 2012;366(3):216-224.
18. Zeuzem S, Andreone P, Pol S, et al. Telaprevir for retreatment of HCV infection. N Engl J Med. 2011;364(25):2417-2428.
19. Suppiah V, Moldovan M, Ahlenstiel G, et al. IL28B is associated with response to chronic hepatitis C interferon-alpha and ribavirin therapy. Nature Genetics.
2009;41(10):1100-U1174.
20. Tanaka Y, Nishida N, Sugiyama M, et al. Genome-wide association of IL28B with response to pegylated interferon-alpha and ribavirin therapy for chronic hepatitis C. Nature Genetics. 2009;41(10):1105-U1181.
21. Ge D, Fellay J, Thompson AJ, et al. Genetic variation in IL28B predicts hepatitis C treatment-induced viral clearance. Nature. 2009;461(7262):399-401.
22. Thomas DL, Thio CL, Martin MP, et al. Genetic variation in IL28B and spontaneous clearance of hepatitis C virus. Nature. 2009;461(7265):798-U752.
23. Eurich D, Boas-Knoop S, Bahra M, et al. Role of IL28B Polymorphism in the
Development of Hepatitis C Virus-Induced Hepatocellular Carcinoma, Graft Fibrosis, and Posttransplant Antiviral Therapy. Transplantation. 2012;93(6):644-649.
24. Huang CF, Huang JF, Yang JF, et al. Interleukin-28B genetic variants in identification of hepatitis C virus genotype 1 patients responding to 24 weeks
peginterferon/ribavirin. J Hepatol. 2012;56(1):34-40.
25. Lin CY, Chen JY, Lin TN, et al. IL28B SNP rs12979860 is a critical predictor for on-treatment and sustained virologic response in patients with hepatitis C virus genotype-1 infection. PLoS One. 20genotype-1genotype-1;6(3):egenotype-18322.
26. Yu ML, Huang CF, Huang JF, et al. Role of interleukin-28B polymorphisms in the treatment of hepatitis C virus genotype 2 infection in Asian patients. Hepatology. 2011;53(1):7-13.
Table 1. HCV RNA seropositive rates by baseline characteristis in R.E.V.E.A.L.-HCV study Baseline Characteristics Total n=975 HCV RNA Undetectable n=299 (30.7%) HCV RNA Detectable n=676 (69.3%) P value Sex Females 550 209 (38.0%) 341 (62.0%) <0.001 Males 425 90 (21.2%) 335 (78.8%) Age at recruitment, years 30-39 163 55 (33.7%) 108 (66.3%) 0.49 40-49 217 72 (33.2%) 145 (66.8%) 50-59 399 113 (28.3%) 286 (71.7%) 60-65 196 59 (30.1%) 137 (69.9%) Cigarette smoking Never 701 245 (35.0%) 456 (65.0%) <0.001 Ever 270 52 (19.3%) 218 (80.7%) Unknown 4 2 2 Alcohol consumption No 893 286 (32.0%) 607 (68.0%) 0.003 Yes 80 13 (16.2%) 67 (83.8%) Unknown 2 0 2
Body mass index
(kg/m2) < 25 589 170 (28.9%) 419 (71.1%) 0.12 25 385 129 (33.5%) 256 (66.5%) Unknown 1 0 1 History of diabetes No 930 285 (30.6%) 645 (69.4%) 0.78 Yes 42 12 (28.6%) 30 (71.4%) Unknown 3 2 1
Serum ALT level (U/L)
15 429 207 (48.3%) 222 (51.7%) <0.001
16-45 387 79 (20.4%) 308 (79.6%)
45 159 13 ( 8.2%) 146 (91.8%)
Table 2. Numbers of participants, person-years of follow-up, hepatocellular carcinoma case numbers and incidence rates by baseline characteristics
Baseline Risk Factors No. (%) of
Participants Pearson-years of Follow-up No. of Hepatocellular Carcinoma cases
Incidence Rate per 100,000 Person-years
Crude Hazard Ratio (95% CI)
Multivariate Adjusted Hazard
Ratio (95% CI) Sex
Females 630 (57.5) 10430 51 489.0 1.00 Not included
Males 465 (42.5) 7514 50 665.4 1.36 (0.92-2.01)
Age at recruitment, years
30-39 186 (17.0) 3148 3 95.3 1.00 1.00 40-49 243 (22.2) 4055 11 271.3 2.86 (0.80-10.26) 2.45 (0.68-8.80) 50-59 444 (40.6) 7196 56 778.2 8.32 (2.60-26.57) 5.70 (1.77-18.37) 60-65 222 (20.3) 3546 31 874.3 9.36 (2.86-30.62) 6.78 (2.05-22.39) Cigarette smoking Never 793 (72.7) 13092 65 496.5 1.00 1.00 Ever 298 (27.3) 4782 36 752.8 1.52 (1.01-2.29) 1.12 (0.70-1.80) Alcohol consumption No 1007 (92.1) 16540 87 526.0 1.00 1.00 Yes 86 (7.9) 1371 13 948.3 1.83 (1.02-3.28) 1.38 (0.69-2.76)
Body mass index (kg/m2)
< 25 663 (60.7) 11003 45 409.0 1.00 1.00
25 430 (39.3) 6906 56 810.9 2.01 (1.36-2.97) 1.76 (1.16-2.67)
History of diabetes
No 1043 (95.7) 17115 95 555.1 1.00 Not included
Yes 47 (4.3) 747 6 802.7 1.48 (0.65-3.37)
Serum ALT level (U/L)
15 495 (45.2) 8302 21 252.9 1.00 1.00
16-44 426 (38.9) 6950 43 618.7 2.49 (1.48-4.19) 1.78 (1.01-3.14)
45 174 (15.9) 2692 37 1374.4 5.66 (3.31-9.67) 2.98 (1.65-5.40)
Serum HCV RNA level (IU/mL)
25 (undetectable) 299 (30.7) 5040 5 99.2 1.00 1.00
>25 (detectable) 676 (69.3) 10943 86 785.9 8.08 (3.28-19.90) 5.67 (2.25-14.31)
Table 3. All-causes and liver-related mortality in patients with HCV infection by baseline characteristics
All causes of death All liver-related deaths
Baseline Risk Factors No. of deaths
Mortality Rate per 100,000 Person-years Crude HR (95% CI) Multivariate adjusted HR (95% CI) No. of deaths
Mortality Rate per 100,000 Person-years Crude HR (95% CI) Multivariate adjusted HR (95% CI) Sex Females 118 1187.0 1.00 1.00 39 392.3 1.00 1.00 Males 144 2093.3 1.80 (1.41-2.30) 1.30 (0.90-1.88) 44 639.6 1.69 (1.10-2.60) 1.04 (0.54-1.99) Age at recruitment, years 30-39 18 592.1 1.00 1.00 3 98.7 1.00 1.00 40-49 28 712.9 1.21 (0.67-2.19) 1.19 (0.62-2.27) 5 127.3 1.30 (0.31-5.43) 1.10 (0.26-4.63) 50-59 129 1940.3 3.38 (2.06-5.53) 2.96 (1.72-5.10) 49 737.0 7.80 (2.43-25.01) 5.20 (1.20-16.88) 60-65 87 2715.6 4.85 (2.92-8.06) 4.29 (2.45-7.51) 26 811.5 8.96 (2.71-29.61) 6.74 (2.01-22.61) Cigarette smoking Never 156 1250.9 1.00 1.00 51 409.0 1.00 1.00 Ever 106 2477.4 2.05 (1.60-2.62) 1.35 (0.92-1.98) 32 747.9 1.93 (1.24-3.00) 1.30 (0.65-2.62) Alcohol consumption No 228 1460.3 1.00 1.00 71 454.8 1.00 1.00 Yes 34 2900.7 2.07 (1.44-2.96) 1.71 (1.14-2.57) 12 1023.8 2.38 (1.29-4.39) 1.77 (0.85-3.67)
Body mass index
(kg/m2) < 25 140 1355.3 1.00 1.00 38 367.9 1.00 1.00 25 121 1873.6 1.40 (1.10-1.79) 1.35 (1.04-1.76) 45 696.8 1.94 (1.26-2.99) 1.84 (1.16-2.93) History of diabetes No 230 1422.5 1.00 1.00 77 476.2 1.00 1.00 Yes 31 5404.8 4.26 (2.93-6.21) 3.99 (2.62-6.08) 6 1046.1 2.62 (1.14-6.03) 2.27 (0.90-5.70)
Serum ALT level (U/L)
15 91 1163.8 1.00 1.00 19 243.0 1.00 1.00
16-44 108 1662.5 1.46 (1.10-1.92) 1.03 (0.76-1.41) 32 492.6 2.08 (1.18-3.68) 1.37 (0.75-2.53)
Level of HCV RNA (IU/mL)
25 (undetectable) 36 744.5 1.00 1.00 4 82.7 1.00 1.00
Figure 2. Seropositive rate of HCV RNA among anti-HCV-seropositives by age and gender
Age groups 30-34 35-39 40-44 45-49 50-54 55-59 60-65 S e ro p o si tiv e R a te o f H C V R N A a m o n g A n ti-H C V -S e ro p o si tiv es ( % ) 50 60 70 80 90 100 Female Male