Short Communication
Mosaic trisomy 12 at amniocentesis: prenatal diagnosis and molecular genetic
analysis
Chih-Ping Chen a,b,c,d,e,f,g *, Yi-Ning Su h, Jun-Wei Su a,i, Schu-Rern Chern b, Yu-Ting Chen b, Li-Feng
Chen a and Wayseen Wang b,j
a Department of Obstetrics and Gynecology, Mackay Memorial Hospital, Taipei, Taiwan b Department of Medical Research, Mackay Memorial Hospital, Taipei, Taiwan
c Department of Medicine, Mackay Medical College, New Taipei City, Taiwan d Department of Biotechnology, Asia University, Taichung, Taiwan
e School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan f Institute of Clinical and Community Health Nursing, National Yang-Ming University, Taipei, Taiwan g Department of Obstetrics and Gynecology, School of Medicine, National Yang-Ming University, Taipei, Taiwan
h Department of Obstetrics and Gynecology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan
i Department of Obstetrics and Gynecology, China Medical University Hospital, Taichung, Taiwan j Department of Bioengineering, Tatung University, Taipei, Taiwan
* Correspondence to: Chih-Ping Chen, MD
Department of Obstetrics and Gynecology, Mackay Memorial Hospital 92, Section 2, Chung-Shan North Road, Taipei, Taiwan
Tel: +886-2-25433535; Fax: +886-2-25433642, +886-2-25232448 E-mail: [email protected]
Abstract
Objective: This study aims at prenatal diagnosis of mosaic trisomy 12 and reviewing the literature.
Materials, Methods and Results: A 34-year-old woman underwent amniocentesis at 17 weeks of gestation because of advanced maternal age. Cytogenetic analysis of cultured amniocytes revealed a karyotype of 47,XX,+12[9]/46,XX[14]. She was referred to the hospital for genetic counseling. Repeated amniocentesis was performed at 22 weeks of gestation. Array comparative genomic hybridization (aCGH), interphase fluorescence in situ hybridization (FISH) and quantitative fluorescent polymerase chain reaction (QF-PCR) were applied on uncultured amniocytes, and conventional cytogenetic analysis was applied on cultured amniocytes. The aCGH analysis on uncultured amniocytes revealed a small genomic gain in chromosome 12. Interphase FISH analysis on uncultured amniocytes using a 12q11-q12-specific probe of RP11-496H24 (spectrum green) showed three green signals in 17.8% (8/45 cells) of uncultured amniocytes. QF-PCR analysis on uncultured amniocytes using chromosome 12-specific microsatellite markers excluded uniparental disomy 12. Cytogenetic analysis of cultured amniocytes revealed a karyotype of 47,XX,+12[5]/ 46,XX[25]. The parents decided to continue the pregnancy. A healthy 3,270-g female baby was delivered at 39 weeks of gestation with no phenotypic abnormalities. Cytogenetic analysis of cord blood revealed a karyotype of 46,XX in 40/40 cultured lymphocytes. The neonate was normal in growth and psychomotor development at 6 months of age. Interphase FISH analysis on uncultured urinary cells revealed 5% (1/20 cells) mosaicism for trisomy 12.
Conclusion: Prenatal diagnosis of mosaic trisomy 12 at amniocentesis should alert a clinically significant aneuploidy. Interphase FISH and aCGH on uncultured amniocytes are useful for rapid confirmation of low-level trisomy 12 mosaicism at repeated amniocentesis.
Introduction
Mosaic trisomy 12 is one of the commonly described mosaicism at amniocentesis that has been well described in the literature [1-20]. Postnatally diagnosed trisomy 12 mosaicism has variable phenotype, and the reported phenotypic abnormalities include developmental delay, pigmentary dysplasia, congenital heart defects, microcephaly, facial asymmetry, prominent ears, hypotonia, hemihyperplasia, intestinal malrotation, retinopathy and sensorineural hearing loss [11,21-28]. Herein, we present our experience of prenatal diagnosis of mosaic trisomy 12 by amniocentesis and a review of the literature.
Materials, Methods and Results
A 34-year-old, gravida 3, para 1, woman underwent amniocentesis at 17 weeks of gestation because of advanced maternal age. Cytogenetic analysis of cultured amniocytes revealed a karyotype of 47,XX,+12[9]/46,XX[14]. She was referred to the hospital for genetic counseling. The parental karyotypes were normal, and prenatal ultrasound findings were unremarkable. Repeated amniocentesis was performed at 22 weeks of gestation. Array comparative genomic hybridization (aCGH), interphase fluorescence in situ hybridization (FISH) and quantitative fluorescent polymerase chain reaction (QF-PCR) were applied on uncultured amniocytes, and conventional cytogenetic analysis was applied on cultured amniocytes. The aCGH analysis using CytoChip Oligo Array (BlueGnome, Cambridge, UK) on uncultured amniocytes revealed a small genomic gain in chromosome 12 (Fig. 1). Interphase FISH analysis on uncultured amniocytes using a 12q11-q12-specific probe of RP11-496H24 (spectrum green) showed three green signals in 17.8% (8/45 cells) and two green signals in 82.2% (37/45 cells) of uncultured amniocytes (Fig. 2). QF-PCR analysis on uncultured amniocytes using chromosome 12-specific microsatellite markers revealed a 1:1 biparental diallelic pattern for chromosome 2 and thus excluded uniparental disomy (UPD) 12 (Fig. 3). Cytogenetic analysis of cultured amniocytes revealed a karyotype of 47,XX, +12[5]/46,XX[25]. Of 30 colonies of cultured amniocytes, five colonies (16.7%) had the karyotype of 47,XX,+12 (Fig. 4), whereas the other 25 colonies (83.3%) had the karyotype of 46,XX. The parents decided to continue the pregnancy. A healthy 3,270-g female baby was delivered at 39 weeks of gestation with no phenotypic abnormalities. Cytogenetic analysis of cord blood revealed a karyotype of 46,XX in 40/40 cultured lymphocytes. The neonate was normal in growth and psychomotor development at 6 months of age. Interphase FISH analysis on uncultured urinary cells at the age of 6 months using 12q11-q12-specific probe of RP11-496H24 (spectrum
green) showed three green signals in 5% (1/20 cells) and two green signals in 95% (19/20 cells) of urinary cells, indicating 5% mosaicism for trisomy 12 in the urinary cells.
Discussion
Molecular cytogenetic techniques such as aCGH, interphase FISH and QF-PCR on uncultured amniocytes for rapid positive confirmation of trisomy mosaicism have been well described [29-34]. The present case shows that in case of trisomy 12 at amniocentesis interphase FISH on uncultured amniocytes is useful for rapid confirmation of low-level mosaicism, aCGH on uncultured amniocytes is useful for confirmation of the presence of about 20% mosaicism, and QF-PCR assay on uncultured amniocytes is useful for rapid exclusion of UPD. The present case also provides evidence for a correlation of low-level trisomy 12 mosaicism in uncultured amniocytes with a favorable fetal outcome. In the present case, the first amniocentesis revealed 39.1% (9/23 colonies) mosaicism for trisomy 12 in cultured amniocytes, and the second amniocentesis revealed 16.7% (5/30 colonies) mosaicism for trisomy 12 in cultured amniocytes and 17.8% (8/45 colonies) mosaicism for trisomy 12 in uncultured amniocytes detected by interphase FISH. Different amniocenteses have been reported to result in inconsistent trisomy 12 mosaicism levels in cultured amniocytes and make genetic counseling difficult [7,9,13,20]. For examples, Frohlich and Falk [7] reported 7% vs. 0%, Cartolano et al [9] reported 26.7% vs. 0%, Spiro et al [13] reported 7.5% vs. 48%, and Gentilin et al [20] reported 17.6% vs. 62.5% mosaicism for trisomy 12 between two different amniocenteses. We think that interphase FISH on uncultured amniocytes in repeated amniocentesis is very practical for determining the real mosaicism level under such a circumstance.
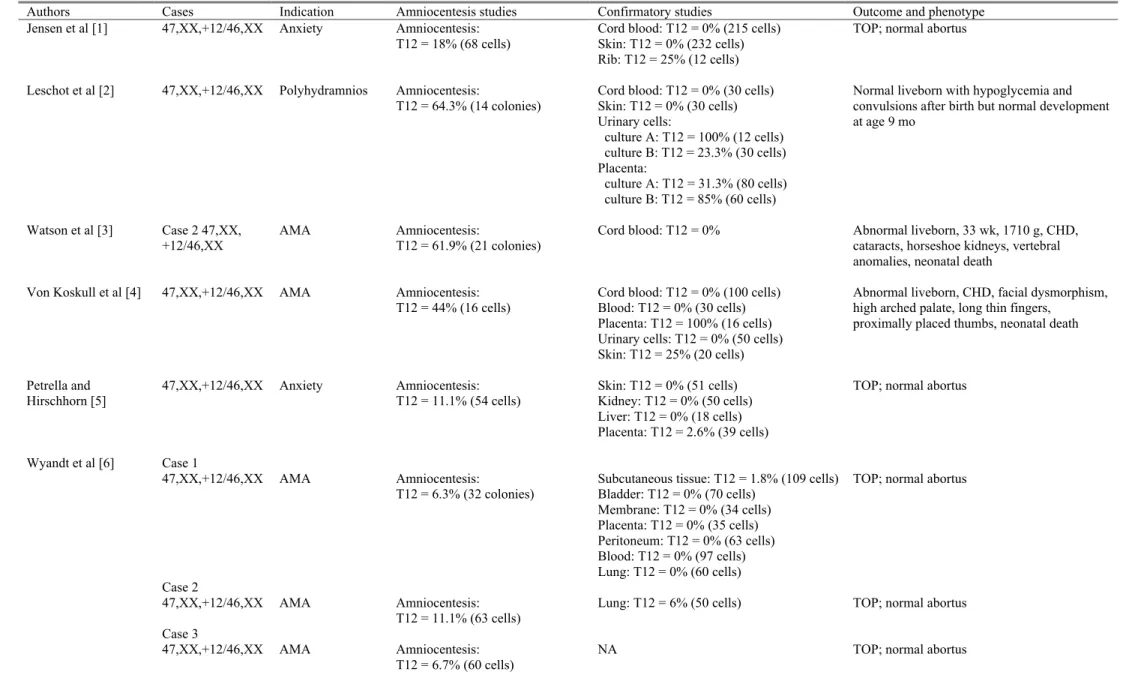
To date, at least 32 cases of mosaic trisomy 12 detected by amniocentesis have been reported (Table 1). Of these, at least 9 cases (9/32 = 28.1%) [3,4,11,14,16,17,19] were associated with prominent phenotypic abnormalities, suggesting that the malformation risk should be concerned in prenatal diagnosis of mosaic trisomy 12 by amniocentesis. In nine cases with an apparently abnormal outcome, the percentage of trisomic cells in cultured amniocytes varied from 4.3% to 61.9% (with five cases > 34%). In 23 cases with a normal outcome, the percentage of trisomic cells in cultured amniocytes varied from 6.1% to 64.3% (with three cases > 34%). These findings indicate a correlation between a higher trisomy 12 mosaicism level and an abnormal fetal outcome. Table 1 shows that the male: female sex ratio for fetal mosaic trisomy 12 is 0.103 (3 males/29
females), indicating a female preponderance in fetal mosaic trisomy 12 and a natural selection against male mosaic trisomy 12 conceptuses. Table 1 also shows that mosaic trisomy 12 can prenatally be associated with elevated maternal serum -fetoprotein [14], elevated maternal serum human chorionic gonadotrophin [12], abnormal maternal serum screening [12,14] and abnormal ultrasound findings [2,11,12]. Table 1 additionally shows that the reported abnormal ultrasound findings associated with mosaic trisomy 12 at amniocentesis include polyhydramnios, intrauterine growth restriction, single umbilical artery, congenital heart defects, hydronephrosis and absence of stomach image.
Mosaic trisomy 12 detected postnatally has been described in nine cases (2 males/7 females) [11,21-28]. Schinzel [35] concluded that there is no clinical pattern due to trisomy 12 mosaicism. Richer et al [21] first reported a 31-year-old phenotypically normal infertile man with 7% mosaicism for trisomy 12 in 157 peripheral blood lymphocytes and Kartagener syndrome of situs inversus, chorionic sinusitis, bronchitis and immotile spermatozoa. Patil et al [22] reported a 36-year-old moderately mentally retarded female with a karyotype of 47,XX,+12[7]/46,XX[49] in peripheral blood, facial dysmorphisms, short stature, microcephaly, muscle stiffness, areflexia limited extension of joints, waddling gaits and scoliosis. English et al [23] reported a 7-year-old mentally normal girl with a karyotype of 47,XX,+12[6]/46,XX[50] in skin fibroblasts, short stature, scoliosis, pigmentary dysplasia and atrial septal defect. Bischoff et al [11] reported a male newborn with a karyotype of 46,XY in skin fibroblasts, a karyotype of 47,XY,+12[4]/ 46,XY[19] in chorionic villi, 5% (10/200) mosaicism for trisomy 12 in spleen, intrauterine growth restriction, oligohydramnios, Potter sequence, low-set ears, lung and kidney hypoplasia, and neonatal death. Aughton et al [24] reported a 9-year-old girl with a karyotype of 47,XX,+12[19]/48,XX, +12,+20[2]/46,XX[29] in skin fibroblasts, asymmetric fullness of the soft tissues of the face, trunk and extremities, normal growth and low-normal development. DeLozier-Blanchet et al [25] reported a 2-month-old girl with a karyotype of 47,XX,+12[7]/46,XX[38] in skin fibroblasts, congenital heart defects (large patent ductus arteriosus, dysplastic pulmonary and tricuspid valves), facial dysmorphisms, a two-vessel cord, widely spaced nipples, camptodactyly, overlapping fingers, pigmentary dysplasia and neonatal death. Boulard et al [26] reported a 15-year-old girl with 80% mosaicism for trisomy 12 in ovarian fibroblasts, pituitary stalk interruption, polycystic ovary syndrome, facial dysmorphisms, hypotonia, strabismus, conducting hearing loss and atrial
septal defect. Parasuraman et al [27] reported a female newborn with a karyotype of 47,XX, +12[18]/46,XX[52] in cord blood, polyhydramnios, echogenic bowel and dilated cardiomyopathy on prenatal ultrasound, edema and low-set ears at birth, and neonatal death. Al-Hertani et al [28] reported a 25-month-old girl with a karyotype of 47,XX,+12[4]/46,XX[17] in the skin fibroblasts from hyper-pigmented and hypo-pigmented regions, facial dysmorphisms, developmental delay, microcephaly, unilateral sensorineural hearing loss, intestinal malrotation, hemihyperplasia, pigmentary dysplasia, retinopathy and a vascular ring.
In summary, we present prenatal diagnosis and molecular cytogenetic analysis of mosaic trisomy 12 using uncultured and cultured amniocytes in a pregnancy with a favorable fetal outcome. We demonstrate the usefulness of analyses of uncultured amniocytes by interphase FISH and aCGH for rapid confirmation of low-level trisomy 12 mosaicism at amniocentesis, and by QF-PCR for rapid exclusion of UPD.
Acknowledgements
This work was supported by research grants NSC-99-2628-B-195-001-MY3 and NSC-101-2314-B-195-011-MY3 from the National Science Council and MMH-E-101-04 from Mackay Memorial Hospital, Taipei, Taiwan.
References
1. Jensen PKA, Hahnemann N, Rehder H, Schwinger E, Friedrich U. Prenatal diagnosis of a 46,XX/47,XX,+12 mosaic. Prenat Diagn 1984; 4: 307-9.
2. Leschot NJ, Wilmsen-Linders EJM, Van Geijn HP, Samsom JF, Smit LME. Karyotyping urine sediment cells confirms trisomy 12 mosaicism detected at amniocentesis. Prenat Diagn 1988; 8: 135-9.
3. Watson JD, Ward BE, Peakman D, Henry G. Trisomy 16 and 12 confined chorionic mosaicism in liveborn infants with multiple anomalies. Am J Hum Genet 1988; 43(Suppl): A252 (Abstract #1006). 4. Von Koskull H, Ritvanen A, Ammala P, Gahmberg N, Salonen R. Trisomy 12 mosaicism in amniocytes
and dysmorphic child despite normal chromosomes in fetal blood sample. Prenat Diagn 1989; 9: 433-7. 5. Petrella R, Hirschhorn K. Trisomy 12 mosaicism detected by mid-trimester amniocentesis. Prenat Diagn
1990; 10: 781-5.
6. Wyandt HE, Maher T, Fisher NL, Patil SR, Osella P, Luthardt FW, et al. Trisomy 12 mosaicism in phenotypically normal fetuses following prenatal detection. Prenat Diagn 1990; 10: 569-74.
7. Frohlich GS, Falk RE. Trisomy 12 mosaicism. Prenat Diagn 1991; 11: 881.
8. Park PM, Dermet MK, Moeschler JB, Wurster-Hill DH. Prenatal diagnosis and confirmation of trisomy 12 mosaicism. Prenat Diagn 1991; 11: 741.
9. Cartolano R, Guerneri S, Fogliani R, Galimberti A, Nicolini U. Prenatal confirmation of trisomy 12 mosaicism by fetal skin biopsy. Prenat Diagn 1993; 13: 1057-9.
10.Meck JM, Kozma C, Tchabo JG, King JC, Lencki S, Pinckert TL. Prenatal diagnosis of trisomy 12 mosaicism: physical and developmental follow-up. Prenat Diagn 1994; 14: 878-83.
11.Bischoff FZ, Zenger-Hain J, Moses D, VanDyke D, Shaffer L. Mosaicism for trisomy 12: Four cases with varying outcomes. Prenat Diagn 1995; 15: 1017-26.
12.Brosens JJ, Overton C, Lavery SA, Thornton S. Trisomy 12 mosaicism diagnosed by amniocentesis. Acta Obstet Gynecol Scand 1996; 75: 79-81.
13.Spiro R, Rita D, Jazmines L, Jones C, Booth CW. Trisomy 12/monosomy X/normal female mosaicism: prenatal detection and confirmation in a liveborn. Prenat Diagn 1996; 16: 734-40.
14.Hsu LYF, Yu M-T, Neu RL, Van Dyke DL, Benn PA, Bradshaw CL, et al. Rare trisomy mosaicism diagnosed in amniocytes, involving an autosome other than chromosomes 13, 18, 20, and 21: Karyotype/phenotype correlations. Prenat Diagn 1997; 17: 201-42.
15.Sikkema-Raddatz B, Bouman K, Verschuuren-Bemelmans CC, de Jong B. Trisomy 12 mosaicism in CVS culture confirmed in the fetus. Prenat Diagn 1999; 19: 1176-7.
16.Djalali M, Merk O, Storli K, Vogel W. Prenatally detected true double trisomy mosaic 12 and 13 not confirmed in fetal and placental tissues by conventional cytogenetic methods, but suggested by FISH analysis. Prenat Diagn 2000; 20: 934-5.
17.Flore LA, Ebrahim SA, Lee HM, Aatre R, Qureshi F, Johnson A, et al. Utilization of Fetal Skin Biopsy for Prenatal Confirmation of Trisomy 12 Mosaicism. Program Nr: 2380 from the 2000 ASHG Annual Meeting.
18.Staals JEA, Schrander-Stumpel CTRM, Hamers G, Fryns JP. Prenatal diagnosis of trisomy 12 mosaicism: normal development of a 3 years old female child. Genet Couns 2003; 14: 233-7.
19.Daniel A, Wu Z, Darmanian A, Malafiej P, Tembe V, Peters G, et al. Issues arising from the prenatal diagnosis of some rare trisomy mosaics--the importance of cryptic fetal mosaicism. Prenat Diagn 2004; 24: 524-36.
20.Gentilin B, Giardino D, Boschetto C Guerneri S, Fortuna R, Rizzuti T, et al. Limited value of echography to predict true fetal mosaicism for trisomy 12. Prenat Diagn 2006; 26: 1183-9.
21.Richer CL, Bleau G, Chapdelaine A. Trisomy 12 mosaicism in an infertile man. Can J Genet Cytol 1977; 19: 565-7.
22.Patil SR, Bosch EP, Hanson JW. First report of mosaic trisomy 12 in a liveborn individual. Am J Med Genet 1983; 14: 453-60.
23.English CJ, Goodship JA, Jackson A, Lowry M, Wolstenholme J. Trisomy 12 mosaicism in a 7 year old girl with dysmorphic features and normal mental development. J Med Genet 1994; 31: 253-4.
24.Aughton DJ, AlSaadi AA, Harper CE, Biesecker LG. Trisomy 12 mosaicism in a girl with multiple minor anomalies. Am J Hum Genet 1996; 59: A111.
25.DeLozier-Blanchet CD, Roeder E, Denis-Arrue R, Blouin JL, Low J, Fisher J, et al. Trisomy 12 mosaicism confirmed in multiple organs from a liveborn child. Am J Med Genet 2000; 95: 444-9. 26.Boulard S, Diene G, Barat R, Oliver I, Pienkowski C, Lacombe D, et al. A case of trisomy 12 mosaicism
with pituitary malformation and polycystic ovary syndrome. Genet Couns 2006; 17: 173-83.
27.Parasuraman R, Mercer C, Bascombe L, Maclachlan N, Gnanapragasam J, Howe DT. A case of trisomy 12 mosaicism presenting antenatally with fetal cardiomyopathy. J Obstet Gynaecol 2011; 31: 261-3. 28.Al-Hertani W, McGowan-Jordan J, Allanson JE. Novel clinical findings in a case of postnatally
diagnosed trisomy 12 mosaicism. Am J Med Genet 2012; 158A: 1452-4.
29.Chen C-P, Lin M-H, Su Y-N, Chern S-R, Tsai F-J, Wu P-C, et al. Mosaic trisomy 9 at amniocentesis: Prenatal diagnosis and molecular genetic analyses. Taiwan J Obstet Gynecol 2010; 49: 341-50.
30.Chen C-P, Chen M, Pan Y-J, Su Y-N, Chern S-R, Tsai F-J, et al. Prenatal diagnosis of mosaic trisomy 8: Clinical report and literature review. Taiwan J Obstet Gynecol 2011; 50: 331-8.
31.Chen C-P, Su Y-N, Lin S-Y, Chern S-R, Chen Y-T, Lee M-S, et al. Prenatal diagnosis of mosaic trisomy 2: Discrepancy between molecular cytogenetic analyses of uncultured amniocytes and karyotyping of cultured amniocytes in a pregnancy with severe fetal intrauterine growth restriction. Taiwan J Obstet Gynecol 2011; 50: 390-3.
32.Chen C-P,Chang S-D, ChuehH-Y, Su Y-N, Su J-W, Chern S-R, et al. Rapid positive confirmation of trisomy 21 mosaicism at amniocentesis by interphase FISH, QF-PCR and aCGH on uncultured amniocytes. Taiwan J Obstet Gynecol 2012; 51: 475-80.
33.Chen C-P,Su Y-N, Chern S-R, Chen Y-T, Wu P-S, Su J-W, et al. Mosaic trisomy 2 at amniocentesis: prenatal diagnosis and molecular genetic analysis. Taiwan J Obstet Gynecol 2012; 51: in press.
34.Chen C-P, Su Y-N, Chern S-R, Chen Y-T, Su J-W, Pan C-W, et al. Prenatal diagnosis of trisomy 8 mosaicism. Taiwan J Obstet Gynecol 2012; 51: in press.
35.Schinzel A. Trisomy 12 mosaicism. In: Schinzel A. ed. Catalogue of Unbalanced Chromosome
Aberrations in Man, 2nd edn. Berlin: Water de Gruter, GmbH & Co. 2001; 541-2.
Figure Legends
Fig. 1. Array comparative genomic hybridization analysis on uncultured amniocytes demonstrates a small genomic gain in chromosome 12. (A) Whole genome view and (B) chromosome view.
Fig. 2. Interphase fluorescence in situ hybridization analysis on uncultured amniocytes using the a 12q11-q12-specific probe RP11-496H24 (spectrum green) shows (A) three green signals in a trisomy 12 cell and (B) two green signals in a disomy 12 cell.
Fig. 3. Representative electrophoretograms of quantitative fluorescent polymerase chain reaction assays on uncultured amniocytes. The markers D12S1301 and D12S376 show two peaks of equal fluorescent activity from two different parental alleles in uncultured amniocytes with a dosage ratio of 1:1 (paternal allele: maternal allele).
Table 1. Reported cases of mosaic trisomy 12 detected by amniocentesis
Authors Cases Indication Amniocentesis studies Confirmatory studies Outcome and phenotype Jensen et al [1] 47,XX,+12/46,XX Anxiety Amniocentesis:
T12 = 18% (68 cells)
Cord blood: T12 = 0% (215 cells) Skin: T12 = 0% (232 cells) Rib: T12 = 25% (12 cells)
TOP; normal abortus
Leschot et al [2] 47,XX,+12/46,XX Polyhydramnios Amniocentesis:
T12 = 64.3% (14 colonies)
Cord blood: T12 = 0% (30 cells) Skin: T12 = 0% (30 cells) Urinary cells: culture A: T12 = 100% (12 cells) culture B: T12 = 23.3% (30 cells) Placenta: culture A: T12 = 31.3% (80 cells) culture B: T12 = 85% (60 cells)
Normal liveborn with hypoglycemia and convulsions after birth but normal development at age 9 mo
Watson et al [3] Case 2 47,XX,
+12/46,XX AMA Amniocentesis:T12 = 61.9% (21 colonies) Cord blood: T12 = 0% Abnormal liveborn, 33 wk, 1710 g, CHD, cataracts, horseshoe kidneys, vertebral anomalies, neonatal death
Von Koskull et al [4] 47,XX,+12/46,XX AMA Amniocentesis:
T12 = 44% (16 cells) Cord blood: T12 = 0% (100 cells)Blood: T12 = 0% (30 cells) Placenta: T12 = 100% (16 cells) Urinary cells: T12 = 0% (50 cells) Skin: T12 = 25% (20 cells)
Abnormal liveborn, CHD, facial dysmorphism, high arched palate, long thin fingers,
proximally placed thumbs, neonatal death
Petrella and Hirschhorn [5] 47,XX,+12/46,XX Anxiety Amniocentesis: T12 = 11.1% (54 cells) Skin: T12 = 0% (51 cells) Kidney: T12 = 0% (50 cells) Liver: T12 = 0% (18 cells) Placenta: T12 = 2.6% (39 cells)
TOP; normal abortus
Wyandt et al [6] Case 1
47,XX,+12/46,XX AMA Amniocentesis:
T12 = 6.3% (32 colonies)
Subcutaneous tissue: T12 = 1.8% (109 cells) Bladder: T12 = 0% (70 cells) Membrane: T12 = 0% (34 cells) Placenta: T12 = 0% (35 cells) Peritoneum: T12 = 0% (63 cells) Blood: T12 = 0% (97 cells) Lung: T12 = 0% (60 cells)
TOP; normal abortus
Case 2
47,XX,+12/46,XX AMA Amniocentesis:
T12 = 11.1% (63 cells) Lung: T12 = 6% (50 cells) TOP; normal abortus Case 3
47,XX,+12/46,XX AMA Amniocentesis: T12 = 6.7% (60 cells)
Frohlich and Falk [7] 47,XX,+12/46,XX AMA Amniocentesis: T12 = 7% (86 cells) Retap: T12 = 0% (200 cells)
Blood: T12 = 0% (100 cells) Normal liveborn, normal development at age 5 mo
Park et al [8] 47,XX,+12/46,XX AMA Amniocentesis: T12 = 6.1% (98 cells)
Blood: T12 = 1% (98 cells) Skin: T12 = 3% (67 cells)
TOP; normal abortus Cartolano et al [9] 47,XX,+12/46,XX AMA Amniocentesis:
T12 = 26.7% (15 colonies) Retap: T12 = 0% (7 colonies)
Cord blood: T12 = 0% (100 cells) Skin: T12 = 6.7% (15 cells) Placenta: T12 = 43% (72 cells)
TOP; normal abortus
Meck et al [10] 47,XX,+12/46,XX AMA Amniocentesis:
T12 = 22.2% (36 colonies)
Cord blood: T12 = 0% (20 cells) Amnion: T12 = 0% (50 cells) Chorion: T12 = 0% (50 cells) Placenta: T12 = 0% (51 cells) Skin: T12 = 0% (100 cells)
Normal liveborn, normal development at age 5 yr Bischoff et al [11] Case D 47,XX,+12/46,XX AMA, ultrasound abnormalities Amniocentesis: T12 = 4.3% (47 cells)
Cord blood: T12 = 0% (20 cells) Cord: T12 = 46.7% (30 cells) Placenta: T12 = 18.6% (32 cells) Membrane: T12 = 0% (30 cells)
Ultrasound: CHD, single umbilical artery, hydronephrosis.
TOP; abnormal abortus, IUGR, single umbilical artery, hydronephrosis, facial dysmorphism, single palmar crease, truncus arteriosus
Brosens et al [12] 47,XX,+12/46,XX AMA, elevated MSAFP, elevated MShCG, Down risk = 1/25, ultrasound abnormalities Amniocentesis: T12 = 34.8% (69 cells) Blood: T12 = 0% (30 cells) Skin: T12 = 0% (45 cells) Placenta: T12 = 87.5% (16 cells)
Ultrasound: no fetal stomach image at 22 wk, polyhydramnios at 32 wk, preterm birth Abnormal liveborn, 32 wk, 1990 g, aortic coarctation, right ventricular hypertrophy, tracheo-esophageal fistula, bilateral pleural effusions, pericardial effusion, neonatal death Spiro et al [13] 47,XX,+12/45,X/
46,XX AMA Amniocentesis:T12 = 7.5% (40 cells) Retap: T12 = 48% (50 cells)
Cord blood: T12 = 0% (50 cells) Placenta: T12 = 20% (20 cells) Villi: T12 = 32.5% (40 cells) Cord: T12 = 85% (20 cells) Membrane: T12 = 41.7% (60 cells) Skin: T12 = 15% (20 cells)
Normal liveborn, mild physical dysmorphisms, hypotonia, delay in gross motor development , age- appropriate cognitive development at age 18 mo
Hsu et al [14] Case XI-1
47,XX,+12/46,XX AMA Amniocentesis:
T12 = 14.8% (27 colonies)
Fetal tissue: T12 = 7.5% (40 cells) TOP; normal abortus, single umbilical artery Case XI-5
47,XY,+12/46,XY Abnormal maternal serum triple screen
Amniocentesis:
T12 = 6.3% (32 colonies) NA Normal liveborn Case XI-8
47,XY,+12/46,XY NA Amniocentesis:
T12 = 33% (30 cells) Fetal tissue: normal TOP; normal abortus Case XI-9
47,XX,+12/46,XX AMA Amniocentesis:
T12 = 46.7% (15 colonies)
NA TOP; normal abortus
Case XI-10
47,XX,+12/46,XX AMA Amniocentesis:
T12 = 50% (24 colonies) Retaps: T12 = 53%
T12 = 16%
NA Epstein anomaly, finger overlapping, normal psychomotor development at age 8 mo Case XI-11
47,XX,+12/46,XX Elevated MSAFP Amniocentesis:
T12 = 12.5% (16 colonies) Retaps: T12 = 1.6% (61 colonies)
NA Normal liveborn
Case XI-12
47,XX,+12/46,XX AMA Amniocentesis:
T12 = 20% (20 colonies) Cord blood: T12 = 0% (30 cells) Normal liveborn Case XI-13
47,XY,+12/46,XY Elevated MSAFP Amniocentesis:
T12 = 28.6% (14 colonies)
NA Normal liveborn
Case XI-14
47,XX,+12/46,XX Elevated MSAFP Amniocentesis:
T12 = 23.3% (43 colonies)
Cord blood: T12 = 0% (50 cells) TOP; abnormal abortus, facial dysmorphism, high arched palate, clinodactyly, transverse palmar creases, short colon, abnormal liver, CHD, large ovaries
Case XI-18
47,XX,+12/46,XX Elevated MSAFP Amniocentesis:
T12 = 32.1% (28 colonies) NA IUFD, IUGR, no gross abnormalities Sikkema-Raddatz et al [15] 47,XX,+12/46,XX AMA, mosaic trisomy 12 at CVS Amniocentesis: T12 = 6.9% (29 colonies) Cord: T12 = 0% T12 = 8% (100 cells) (FISH)
TOP; normal abortus
Djalali et al [16] 48,XX,+12,+13/ 46,XX
AMA Amniocentesis:
T12 and T13 = 17.7% (68 cells)
Skin: T12 = 1.3% (552 cells) (FISH) Rib: T12 = 2.8% (108 cells) (FISH)
TOP; abnormal abortus, facial dysmorphisms Flore et al [17] 47,XX,+12/46,XX AMA Amniocentesis:
mosaic T12 Blood: T12 = 0.6% (interphase cells)Placenta: T12 = 25% (cultured cells) Skin: T12 = 22% (cultured cells)
TOP; abnormal abortus, facial dysmorphisms, deep white matter microinfarct, subarachnoid congestion with focal hemorrhage, heterotopia of cerebellar white matter, broad and spaced hallices, prominent clitoris, poorly formed labia
Staals et al [18] 47,XX,+12/46,XX AMA Amniocentesis:
T12 = 18.2% (22 colonies)
NA Normal liveborn, normal development at age 3 yr
Daniel et al [19] Case 6
47,XX,+12/46,XX AMA Amniocentesis:
T12 = 45.2% (42 colonies) NA TOP; abnormal abortus, facial dysmorphisms, abnormal nipples, unlobar right lung, dysplastic tricuspid valve, pleural effusion Gentilin et al [20] 47,XX,+12/46,XX Anxiety Amniocentesis:
T12 = 17.6% (17 colonies)
Retap: T12 = 62.5% (40 colonies)
Skin: T12 = 2% (200 cells) Cartilage: T12 = 10% (200 cells)
TOP; normal abortus with mild micrognathia
Present case 47,XX,+12/46,XX AMA Amniocentesis:
T12 = 39.1% (23 colonies) Retap: T12 = 16.7% (30 colonies) interphase FISH: T12 = 17.8% (45 uncultured amniocytes)
Cord blood: T12 = 0% (40 cells) Urinary cells:
interphase FISH: T12 = 5% (20 cells)
Normal liveborn, normal development at age 6 mo
NA: not available, TOP: termination of pregnancy, T12: trisomy 12, MSAFP: maternal serum -fetoprotein, AMA: advanced maternal age, MShCG: maternal serum human chorionic gonadotrophin, CHD: congenital heart defect, IUFD: intrauterine fetal death, IUGR: intrauterine growth restriction, CVS: chorionic villus sampling, FISH: fluorescence in