Title: Lung Abscess Predicts the Surgical Outcome in Patients with Pleural Empyema
Short title: Lung abscess and pleural empyema
Authors: aHung-Che Huang, MD, aHeng-Chung Chen, MD, bHsin-Yuan Fang, MD, a
Yi-Chieh Lin, aChin-Yen Wu, aChing-Yuan Cheng, MD
Institution: Division of Thoracic surgery, Department of Surgery, Changhua
Christian Hospital,a Changhua, Taiwan; and Division of Thoracic surgery, Department
of Surgery, China Medical University Hospital, China Medical University,b Taichung,
Taiwan.
This study was supported by a grant from the foundation of Changhua Christian
Hospital and Chang Jung Christian University (97-CCH-CJCU-10), Taiwan.
Key Words: Pleural empyema; lung abscess; thoracoscopic surgery
Corresponding Author: Dr. Hsin-Yuan Fang; Division of Thoracic surgery,
Department of Surgery, China Medical University Hospital, China Medical
University, Taichung, Taiwan; Address: 2 Yude Road, Taichung, Taiwan 404;
ABSTRACT
Objectives: Most cases of pleural empyema are caused by pulmonary infections,
which are usually combined with pneumonia or lung abscess. The mortality of
patients with pleural empyema remains high (up to 20%). It also contributes to higher
hospital costs and longer hospital stays. We studied pleural empyema with combined
lung abscess to determine if abscess was associated with mortality.
Methods: From January 2004 to December 2006, we retrospectively reviewed 259
patients diagnosed with pleural empyema who received thoracscopic decortications of
the pleura in a single medical center. We evaluated their clinical data and analyzed
their chest computed tomography (CT) scans. Outcomes of pleural empyema were
compared between groups with and without lung abscess.
Results: Twenty-two pleural empyema patients had lung abscesses. Clinical data
showed significantly higher incidences in the lung abscess group of pre-operative
leukocytosis, need for an intensive care unit stay and mortality.
Conclusion: Patients with pleural empyema and lung abscess have higher ICU
admission rate, higher mortality during 30 days and overall mortality than patients
with pleural empyema. The Odds ratio of lung abscess is 4.685. Physician shall pay
more attention on high risk patient of lung abscess for early detection and
BACKGROUND
Pleural empyema is one of the serious complications of pneumonia, and
increases the morbidity and mortality due to pneumonia [1-3]. About 5% of patients
with pneumonia suffer from pleural empyema [4, 5]. About 65,000 patients in the
United State and the United Kingdom suffer annually from pleural empyema or a
complicated parapneumonic effusion. The mortality of patients with pleural empyema
is up to 20% and contributes to higher hospital costs. Inflammatory mechanisms and
alterations in the balance of pleural fibrinolysis have been implicated in the
pathophysiology of infectious pleural effusion. Pleural empyema is associated with
fibrin deposition over pleural surfaces due to inhibition of the fibrinolysis system [6,
7]. Parapneumonic effusions progress through exudative and fibrinopurulent stages
and terminate in empyema in the organized stage. The clinical courses of patients with
parapneumonic effusions or pleural empyema are varied. Lung abscess is defined as a
circumscribed collection of pus in the lung, which leads to formation of a cavity. It
develops when a localized area of parenchymal infection becomes necrotic and then
cavitates. It most commonly occurs secondary to aspiration in patients with poor
dentition or as a complication of necrotizing pneumonia. Lung abscess has previously
been thought to be a rare condition of empyema and parapneumonic effusions. About
Surgical resection of lung abscess is rare when medical treatments fail.
Pleural empyema and lung abscess are both a part of low respiratory tract
infection. According to the clinical observation, pleural empyema and lung abscesses
may happen on the same patient. However, the strategies of these two diseases are so
different. It is interesting whether the surgical results are the same of empyema
patients with and without lung abscesses. We compared the clinical presentations and
METHODS
Patients
This was a retrospective cohort study conducted in evaluation the impact of lung
abscess on the surgical results of patients with pleural empyema.From January 2004
to December 2006, 259 patients were diagnosed with pleural empyema and received
thoracoscopic decortication of pleural in Changhua Christian Hospital in central
Taiwan. The diagnosis for all the patients was based initially on a chest X-ray
followed by a computed tomography (CT) scan or ultrasound. All of the operations
were performed by one of four qualified thoracic surgeons in our hospital. Pleural
empyema was classified according to the American Thoracic Society staging; stage I
is exudative pleuresia, stage II is fibrinopurulent and stage III is organized.
Thoracentesis was performed on these patients for a sample of pleural fluid to
determine pH, lactate dehydrogenase, glucose, protein levels, and blood cell count.
After the diagnosis was established, all the patients were treated with an appropriate
antibiotic therapy. The patients, who were classified into phase II or phase III pleural
empyema received video-assist thoracoscopic surgery (VATS) for decortications of
pleura. The operation was converted to open thoracotomy if it was failed by VATS.
The patients with pleural empyema and lung abscess received VATS decortications
chronology of initial signs and diagnoses; bacteriological and biochemical studies of
pleural fluids; and radiological and pre-operative findings. The vital signs were
recorded just before operation in the operation room. Lung abscess was defined as a
circumscribed collection of pus in the lung that led to cavity formation, which was
noted on chest radiograph, CT scan or intraoperative findings by the surgeon. In our
study, there was no any patient in lung abscess group received additional chest tube
insertion or abscess aspiration before or after operation. Figure 1 shows an example of
chest radiograph and CT scan for loculated pleural fluid collection and Figure 2 is an
example of chest radiograph and CT scan of pleural empyema accompanied by
abscess. Leukocytosis was defined as a white blood cell count > 10,000/µL (reference
value in Changhua Christian Hospital). The outcome measures were post-operative
complications and the length of hospitalization.
Surgical procedures
All patients were transferred to the operating room and underwent general anesthesia
with double-lumen endotracheal tube or single lumen endotracheal tube intubation. A
patient was placed in the true lateral decubitus position on the side opposite to the
empyema. Two ports were used (telescope and one instrument) after selective one
was difficult to perform. After a systematic sampling of fluid, abundant irrigation and
aspiration were performed. Extensive debridement and ablation of all septa allowed
the entire pleural cavity to be unified. Removal of the visceral and parietal pleural
peel was by VATS as complete as possible, with attention paid to the visceral pleura in
order to avoid air leakage. The lung re-expansion after decortication was confirmed
during operation by two lung ventilation. If failure, mini-thoracotomy was performed
for adequate decortication until full expansion of the lung was confirmed. Two chest
tubes (28 or 32 Fr) were positioned to the anterior and posterior. After the operation,
the chest tube was connected to one-bottle system that was set to a negative pressure
(15 cm H2O using an Emerson postoperative suction pump) regularly.
Statistical methods
Data are presented as median medians ± standard error for continuous
variables and number (percentage) for categorical variables. Continuous and
categorical variables were statistically compared by Mann-Whitney U test and
Fisher’s exact test. Survival curves were generated using the Kaplan-Meier method
and differences were determined using the log-rank test. A two-tailed P-value of ≤0.05
RESULTS
There were 259 patients who had pleural empyema from January 2004 to
December 2006 who underwent surgical interventions during the investigation period.
There were 202 men (78%) and 57 women (22%). Nineteen patients died during the
same admission.The surgical mortality rate was 7.34 % (19 of 259). All early and late
deaths were attributed to progressive uncontrolled sepsis.
The causes of pleural empyema included low respiratory infection (n = 239,
92%), lung cancer (n = 9, 3.5%), induced by deep neck infection (n=1, 0.39%),
post-traumatic empyema (n = 6, 2.3%) and post-operative complication (n = 4, 1.5%).
Two patients were converted to mini-thoracotomy (2 of 259, 0.77%). In abscess group,
there were nineteen phase II patients and three phase III patients. In non-abscess
group, there were six phase I patients, two hundred and seven phase II patients and
three phase III patients. There was no significant different between the two groups
(P=0.0516).
Bacteria culture were performed for the 259 patients during their operations
and microorganism growth was detected in 86 sets (86 of 259, 33.2%). There were
161 patients who had bacterial blood cultures and 25 positive results (15.5%); 173
patients had bacterial cultures of pleural effusion before surgery and only 42 positive
The mean hospital stay was 24.8±31.68 days and the mean post-operative
hospital stay was 17.5± 27.80days. The mean period of pre-operative antibiotic
therapy in the mortality group was 13.0 ± 11.5 days. The mean period of pre-operative
antibiotic therapy in the surviving group was 7.6 ± 9.8 days. There was a significant
different between the two groups (P=0.037). There were no significant differences in
clinical presentations, such as heart rate, body temperature, mean arterial pressure,
respiratory rates or co-morbidities.
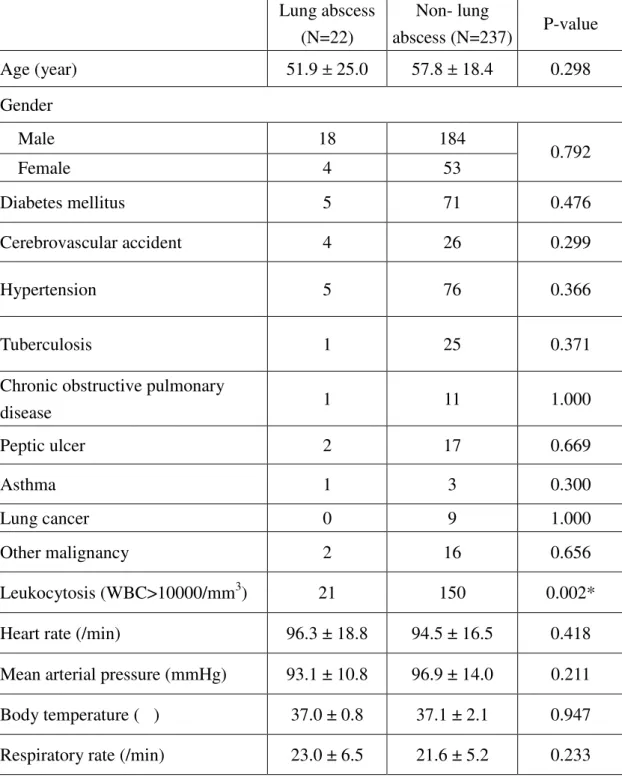
There were 22 patients with lung abscesses based on image studies or by the
findings during surgery. Pre-operative leukocytosis (P=0.002), need for intensive care
unit stays (P=0.032), 30 days mortality (P=0.003; Figure 3, upper panel) and overall
mortality (P=0.004; Figure 3, lower panel) were significantly different between the
abscess group and the no abscess group (Table 1). Patients with lung abscess
formation might require additional surgical procedures for residual empyema
(P=0.081).
14 patients were cared in intensive care unit before operation due to
respiratory failure or unstable vital signs. In abscess group, there was only one patient
cared in intensive care unit. In non-abscess group, there were 13 patients cared in
intensive care unit. Excluding patients cared in intensive care unit (ICU) before
non-abscess group. The rate of admission to ICU after operation had significant
different between the groups (P= 0.02).
The data of alcohol use of 194 patients were available. It was collected from
patient himself, nurse record and medical chart. There were 24 patients use alcohol
sometimes and 3 patients had abscess formations. 14 patients used alcohol everyday
but no one had abscess formation. By the available data, the patient number of alcohol
use or alcohol abuse had no significant difference between the abscess and
non-abscess group (P=0.625). There was also no significant difference between the
DISCUSSIONS
About 20% of cases of paraneumonic effusion progress to pleural empyema
despite the effective antibiotics and drainage of pleural effusion[3]. Early diagnosis
and prompt drainage of pleural space infections are crucial, as delay increases
morbidity. Pleural empyema can occur as a complication of pneumonia, tuberculosis
or surgical procedures. In our study, the majority of our cases resulted from
respiratory tract infection, as the same as other reports. An appropriate treatment for
pleural empyema will include sepsis control, restoration of pulmonary function and
prevent lung entrapment after the fibrous peel [9, 10].
A lung abscess is a thick-walled cavity that contains purulent material and can
occur at any age [11]. About ninety percent of patients with lung abscesses were cured
by simply antibiotics therapy [8, 12]. It is rarely necessary to resect the lung abscesses.
The role of surgery for lung abscess is to manage the complications, including pleural
empyema and bronchopleural fistula. Some patients had pleural empyema and lung
abscess at the same time. In this study, the patient characteristics showed no
significant differences between the two groups such as co-morbidity and clinical
presentation, but leukocytosis (Table 1). There were more patients with leukocytosis
abscess group. Only 150 patients (63.3%) had leukocytosis of the patients in the no
abscess group. However, leukocytosis may be related to inflammation or infection,
but the number of white cell counts does not reflect the severity of inflammation or
infection. Although the difference between the two group has statistical significant
(P=0.002), it is rough to conclude the diagnosis and severity according to the white
cell count.
The leading cause of pleural empyema in our study was low respiratory tract
infection and the incidence was 92.8%, and 22 of these patients (8.5%) had abscesses.
Previous studies also identified bronchopulmonary infection as an important cause of
empyema [13]. Lung malignancy, post-trauma, post-operative complications and deep
neck infection were the other causes of pleural empyema in our study. Our study
showed less post-traumatic pleural empyema rate than previous study. The low
incidence may be due to early chest tube drainage when traumatic patients had related
pleural effusion in our department [14].
Lung abscess have been associated with alcohol abuse. However, in our study,
the patient number of alcohol use or alcohol abuse had no significant difference
difference between the mortality and survive group (P=0.557). However, the data
was limited by the patient number of abscess group, the accuracy of medical record
and nurse record, as well as the different definition of alcohol use and alcohol abuse.
The mean periods of pre-operative antibiotic therapy in the mortality group
was longer than in the surviving group, respectively (P=0.037). According to these
results, early surgery after diagnosis appears to decrease the mortality. Some studies
showed that early decortication of the pleura by VATS was a safe, curative treatment
of pleural empyema with low morbidity [15, 16]. However, some patients in our
study were admitted for other diseases or were given antibiotics for other infection
sources before pleural empyema was diagnosed. Longer antibiotics period may be
due to poor infection control or nosocomial infection. The delay or increase duration
of preoperative antibiotics may result from delaying diagnosis of empyema or lung
abscess. There are many patients with low respiratory infection complicated with
pleural empyema. The diagnosis shall be kept in mind. According to Coote et al and
Petrakis et al, once pleural empyema is diagnosed, early and adequate drainage as
well as early operation, especially the less invasive operation, VATS, is helpful to
Bacterial cultures of the pleural empyema were performed in all patients.
However, there were only 33.2% positive results from all these cultures. There were
161 patients who had bacterial blood cultures and only 25 positive results (15.5%);
173 patients had bacterial cultures of pleural effusions before surgery and only 42
positive results (24.3%). There was no significant difference for mortality based on
the results of bacterial cultures. Echo guidance aspiration for pleural effusion is
helpful to distinguish the quality of pleural effusion which is a guide of management.
As Nyambat et al suggested in 2008, due to the low culture rate, culture may not be a
sufficiently sensitive diagnostic method to determine the etiology in the majority of
cases. The cost-effectiveness of pre-operative pleural effusion culture or blood
culture shall be discussed after further study.
The abscess group also showed a higher frequency to enter the ICU after
surgery (P= 0.032). After excluding the patients in ICU before operation (one in
abscess group and thirteen in no abscess group), the frequency to enter the ICU after
surgery still has significant difference (P=0.02). The indications for admission to an
ICU were unstable vital signs, unstable respiratory patterns and previous ICU stays.
The result revealed that the patients with pleural empyema and lung abscess were
However, there was no statistical difference in the length of ICU stays, lengths
of admission or length of post-operative stays. This may have been due to the large
capacity of the respiratory care center or respiratory care ward. All the patients could
be transferred to these units after sepsis or bronchopulmonary infections were
controlled, and then transferred to a nursing home if conditions became stable and
necessary. It also may be due to the failure to calculate the length of stay in other
hospital before transferring to our hospital. In our study, the length of stay for patients
in pleural empyema was 21.4 days and the length of stay after surgery was 12.8 days.
The length of stay was longer than previous data. This may resulted from
co-morbidity, delayed diagnosis of pleural empyema or a delay in surgical
intervention. Some studies showed that early surgical intervention was the most
optimal and cost-effective initial modality for the treatment of empyema [19].
Five patients died after their operations in the abscess group (23%) within 30
days of surgery or during the same admission. The mortality rate of the no abscess
group was only 5.9%, consistent with overall mortalities observed in previous series
studies [13, 19, 20]. Patients with abscess had a higher mortality rate than patients
confidence interval = 1.057-14.56). Furthermore, patients in the abscess group also
had a trend to receive second decortications of the pleura (P=0.081). The multiple
logistic regressions revealed lung abscess was not an independent predictor of death.
Why the lung abscess group required further procedures? According to our data, it
may be due to worse condition of the lung abscess group. The operator may stopped
the operation before the completely removal of the peel due to unstable vital signs
during operation. Bronchopleural fistula may also play a role in such a situation;
however we had only a little experience with bronchopleural fistula. The overall
CONCLUSION
Patients with pleural empyema and lung abscess have higher ICU admission
rate, higher mortality during 30 days and overall mortality than patients with pleural
empyema. The Odds ratio of lung abscess is 4.685. Physician shall pay more
REFERENCES
[1] Schopf LF, Fraga JC, Amantea SL, Sanches P, Muller A, Borowski S, Kulczynski
J, Costa E. Induction of pleural empyema in rats by thoracentesis with intrapleural
pressure monitoring. Pediatric surgery international 2004;20:515-519.
[2] Jess P, Brynitz S, Friis Moller A. Mortality in thoracic empyema. Scand J Thorac
Cardiovasc Surg 1984;18:85-87.
[3] Sahn SA. Management of complicated parapneumonic effusions. Am Rev Respir
Dis 1993;148:813-817.
[4] Bouros D, Plataki M, Antoniou KM. Parapneumonic effusion and empyema: best
therapeutic approach. Monaldi Arch Chest Dis 2001;56:144-148.
[5] Kunz CR, Jadus MR, Kukes GD, Kramer F, Nguyen VN, Sasse SA. Intrapleural
injection of transforming growth factor-beta antibody inhibits pleural fibrosis in
empyema. Chest 2004;126:1636-1644.
[6] Idell S, Girard W, Koenig KB, McLarty J, Fair DS. Abnormalities of pathways of
fibrin turnover in the human pleural space. Am Rev Respir Dis 1991;144:187-194.
[7] Agrenius V, Chmielewska J, Widstrom O, Blomback M. Pleural fibrinolytic
activity is decreased in inflammation as demonstrated in quinacrine pleurodesis
treatment of malignant pleural effusion. Am Rev Respir Dis 1989;140:1381-1385.
intrapulmonary air and fluid collections. Radiologic clinics of North America
2000;38:385-393.
[9] Jaffe A, Balfour-Lynn IM. Management of empyema in children. Pediatric
pulmonology 2005;40:148-156.
[10] Russell-Taylor M. Bacterial pneumonias: management and complication.
Paediatric respiratory reviews 2000;1:14-20.
[11] Patradoon-Ho P, Fitzgerald DA. Lung abscess in children. Paediatric respiratory
reviews 2007;8:77-84.
[12] Pena Grinan N, Munoz Lucena F, Vargas Romero J, Alfageme Michavila I,
Umbria Dominguez S, Florez Alia C. Yield of percutaneous needle lung aspiration in
lung abscess. Chest 1990;97:69-74.
[13] Hsieh MJ, Liu YH, Chao YK, Lu MS, Liu HP, Wu YC, Lu HI, Chu Y. Risk
factors in surgical management of thoracic empyema in elderly patients. ANZ journal
of surgery 2008;78:445-448.
[14] Scherer LA, Battistella FD, Owings JT, Aguilar MM. Video-assisted thoracic
surgery in the treatment of posttraumatic empyema. Arch Surg 1998;133:637-641;
discussion 641-632.
[15] Kosloske AM, Cushing AH, Shuck JM. Early decortication for anaerobic
[16] Gun F, Salman T, Abbasoglu L, Salman N, Celik A. Early decortication in
childhood empyema thoracis. Acta chirurgica Belgica 2007;107:225-227.
[17] Coote N. Surgical versus non-surgical management of pleural empyema.
Cochrane database of systematic reviews (Online) 2002:CD001956.
[18] Petrakis IE, Kogerakis NE, Drositis IE, Lasithiotakis KG, Bouros D,
Chalkiadakis GE. Video-assisted thoracoscopic surgery for thoracic empyema:
primarily, or after fibrinolytic therapy failure? American journal of surgery
2004;187:471-474.
[19] Schiza S, Siafakas NM. Clinical presentation and management of empyema, lung
abscess and pleural effusion. Current opinion in pulmonary medicine
2006;12:205-211.
[20] Molnar TF. Current surgical treatment of thoracic empyema in adults. Eur J
Figure 1: The chest radiograph and computed tomography scan showed pleural
empyema without lung abscess.
Figure 2: The chest radiograph and computed tomography showed pleural empyema
with lung abscess.
Figure 3: Survival curves after surgery. The survival curves used the Kaplan-Meier
method and differences were calculated using the log-rank test. Upper panel: The 30
days survival shows a significant difference (P=0.0031). Lower panel: The overall
post-operative survival between the 2 groups also shows a significant difference
Table 1: Characteristics of pleural empyema patients with and without lung abscess. Lung abscess (N=22) Non- lung abscess (N=237) P-value Age (year) 51.9 ± 25.0 57.8 ± 18.4 0.298 Gender Male 18 184 Female 4 53 0.792 Diabetes mellitus 5 71 0.476 Cerebrovascular accident 4 26 0.299 Hypertension 5 76 0.366 Tuberculosis 1 25 0.371
Chronic obstructive pulmonary
disease 1 11 1.000 Peptic ulcer 2 17 0.669 Asthma 1 3 0.300 Lung cancer 0 9 1.000 Other malignancy 2 16 0.656 Leukocytosis (WBC>10000/mm3) 21 150 0.002*
Heart rate (/min) 96.3 ± 18.8 94.5 ± 16.5 0.418
Mean arterial pressure (mmHg) 93.1 ± 10.8 96.9 ± 14.0 0.211
Body temperature (℃) 37.0 ± 0.8 37.1 ± 2.1 0.947
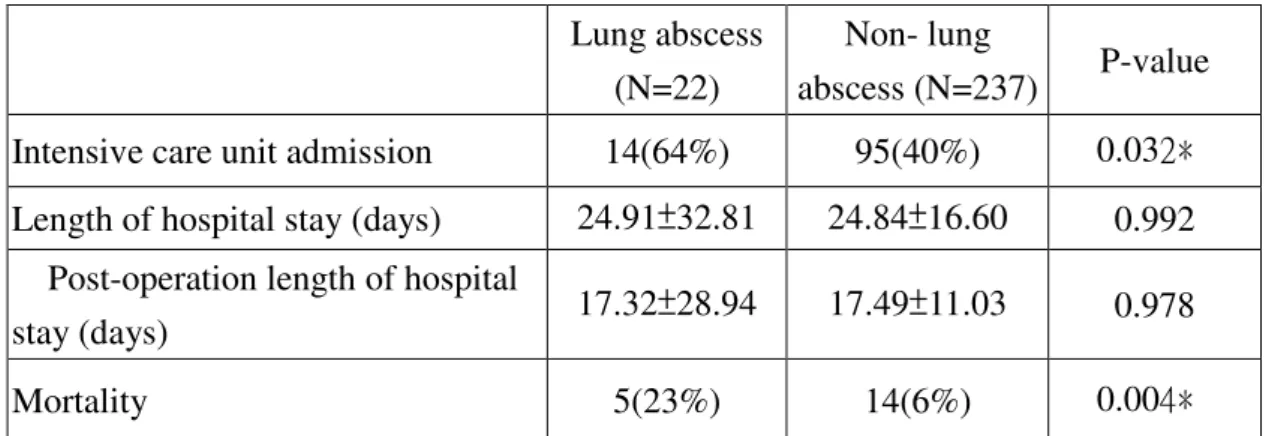
Table 2 outcomes of pleural empyema patients with and without lung abscess. Lung abscess
(N=22)
Non- lung
abscess (N=237) P-value
Intensive care unit admission 14(64%) 95(40%) 0.032﹡
Length of hospital stay (days) 24.91±32.81 24.84±16.60 0.992 Post-operation length of hospital
stay (days) 17.32±28.94 17.49±11.03 0.978
Mortality 5(23%) 14(6%) 0.004﹡
1. Values are medians ± standard error for continuous variables or # cases (%) for categorical variables.
2. P-values from Mann-Whitney U test (continuous variables) or Fisher exact test (categorical variables).
Additional file 1: table1.jpg, 101K
http://www.cardiothoracicsurgery.org/imedia/3906325314483615/supp1.jpeg Additional file 2: table2.JPG, 77K