Long-term follow-up of superior mesenteric venous thrombosis
233 Kaohsiung J Med Sci May 2003 • Vol 19 • No 5
L
ONG
-
TERM
F
OLLOW
-
UP
OF
P
ARTIAL
T
HROMBOSIS
OF
THE
S
UPERIOR
M
ESENTERIC
V
EIN
IN
A
C
IRRHOTIC
P
ATIENT
WITH
H
EPATOCELLULAR
C
ARCINOMA
Men-Shun Hsieh, Zu-Yau Lin, Wan-Long Chuang, and Wen-Yu Chang
Hepatobiliary Division, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan.
Superior mesenteric venous thrombosis (SMVT) is an uncommon but potentially life-threatening disorder. We describe a cirrhotic patient with hepatocellular carcinoma who had partial SMVT for at least 28 months. Our experience may help in the management of such patients. The partial SMVT was not treated at the time of discovery because there was no evidence of bowel infarction. Moreover, the patient had a tendency to bleed severely and was in a poor condition. SMVT was followed using regular ultrasonography and the pattern of SMVT did not change significantly during the follow-up period. A symptom that may have been related to SMVT was abdominal colic pain after meals, which was sometimes followed by diarrhea and/or nausea and vomiting. There was no evidence of bowel ischemia or infarction during follow-up. Abdominal discomfort can be successfully treated using anticholinergic drugs with or without analgesia.
Key Words: superior mesenteric venous thrombosis, liver cirrhosis, hepatocellular carcinoma
(Kaohsiung J Med Sci 2003;19:233–7)
Received: September 17, 2002 Accepted: March 4, 2003 Address correspondence and reprint requests to: Dr. Zu-Yau Lin, Hepatobiliary Division, Department of Internal Medicine, Kaohsiung Medical University Hospital, 100 Shih-Chuan 1st Road, Kaohsiung 807, Taiwan.
E-mail: [email protected]
Superior mesenteric venous thrombosis (SMVT) is an uncommon disorder [1–3], with no specific clinical symptoms and signs. Early diagnosis is based on the physician’s awareness of the disorder. SMVT is clinically important because it has the potential to cause life-threatening bowel ischemia [1–6]. SMVT m a y b e i d i o p a t h i c , s e c o n d a r y t o i n h e r i t e d thrombophilic conditions, or acquired [2–6]. Liver cirrhosis and hepatocellular carcinoma (HCC), which are very common in Taiwan, are two acquired causes of SMVT [2]. At autopsy [7] and peritoneoscopy [8–
10], macronodular cirrhosis coexists in 80–85% of patients with HCC. SMVT in cirrhotic patients with HCC may be caused by either portal hypertension or malignant invasion. The methods used to treat benign SMVT are quite different from those for malignant SMVT. Moreover, patients with liver cirrhosis usually demonstrate a tendency to bleed, caused by thrombocytopenia and coagulopathy. Therefore, it may be very difficult to decide on how to manage SMVT in cirrhotic patients with HCC. In this case report, we describe a cirrhotic patient with HCC who had partial SMVT for at least 28 months. Our experience may help in the management of such patients.
CASE PRESENTATION
A 50-year-old man with a medical history of liver cirrhosis and diabetes mellitus was admitted to our
Kaohsiung J Med Sci May 2003 • Vol 19 • No 5 M.S. Hsieh, Z.Y. Lin, W.L. Chuang, and W.Y. Chang
234
institution because of gastrointestinal hemorrhage. Blood pressure at admission was 126/72 mmHg and pulse rate was 104. Laboratory tests revealed a hemoglobin concentration of 7.5 g/dL, white blood cell count of 2,400/mm3
, platelet count of 33,000/mm3
, total bilirubin concentration of 6.5 mg/dL (direct bilirubin, 5.2 mg/dL), albumin of 2.7 g/mL, aspartate transaminase of 150 IU/L, alanine transaminase of 98 IU/L, prothrombin time of 16.5 seconds (control, 12 seconds), and serum alpha-fetoprotein concentration of 387 ng/mL. Upper gastrointestinal endoscopy showed rupture of the esophageal varices, which was successfully treated using continuous vasopressin therapy for 3 days in combination with two sessions of endoscopic ligation of the varices. Abdominal ultrasonography on the second day of hospitalization showed evidence of liver cirrhosis with massive ascites and a hepatic nodule measuring 3 cm at the right posterior inferior segment of the liver. The portal system was patent with no evidence of thrombosis. Aspiration biopsy of the hepatic nodule was not p e r f o r m e d b e c a u s e o f a s c i t e s . F o l l o w - u p ultrasonography 2 months after the first examination showed improvement in the ascites, slight enlargement of the hepatic nodule, and partial SMVT near the confluence with the splenic vein (Figure 1A). No hepatofugal portal blood flow was detected using color Doppler ultrasonography. Since the patient did not show evidence of peritonitis, was in a poor condition, and had a tendency towards severe bleeding, the SMVT was not treated. He was well informed about the possible symptoms of SMVT and was instructed to take a small amount of food only in each meal. Contrast-enhanced computerized tomography (CT) also showed partial SMVT and excluded the possibility of intestinal infarction (Figure 2). The hepatic nodule was diagnosed as HCC based on elevated serum alpha-fetoprotein and CT findings. The patient underwent regular follow-up for HCC and SMVT using ultrasonography at 3-month intervals. The HCC was treated using transcatheter arterial chemoembolization at five sessions over a period of 2 years. Prophylactic endoscopic ligation of the esophageal varices was performed over four sessions during follow-up. The ultrasonographic pattern of the partial SMVT did not change significantly for at least 28 months (Figure 1B). During the follow-up period, the patient frequently complained of colic pain around the umbilical area after meals. This symptom was
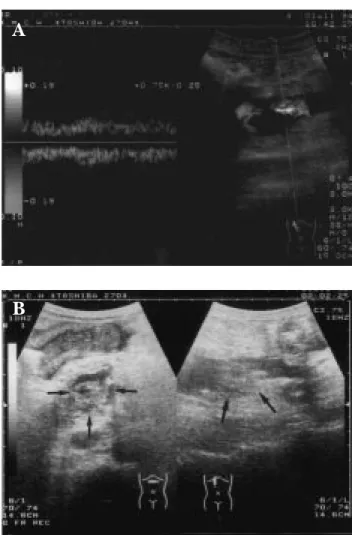
Figure 1. (A) Color Doppler ultrasonography shows partial
thrombosis of the superior mesenteric vein. There is turbulent blood flow around the thrombus. (B) B-mode real-time ultrasonography performed 28 months after the color Doppler ultrasonogram shows no significant change in the thrombus (arrows).
A
B
sometimes followed by diarrhea and/or nausea and vomiting. There was no evidence of bowel ischemia or infarction during follow-up. Abdominal discomfort was successfully treated with anticholinergic drugs, with or without analgesia. The patient died 32 months after the first admission to our institution due to cellulitis of the legs caused by Vibrio vulnificus.
DISCUSSION
SMVT caused by inherited thrombophilic conditions such as protein C and protein S deficiencies, antithrombin III deficiency, dysfibrinogenemia, and factor V Leiden deficiency is usually observed in young
Long-term follow-up of superior mesenteric venous thrombosis
235 Kaohsiung J Med Sci May 2003 • Vol 19 • No 5
patients [2,6]. The patient in this case report was 50 years old and had no medical history of venous thrombosis. Moreover, the pattern of SMVT did not change significantly over time, indicating that it was not caused by an inherited thrombophilic condition.
Focal or generalized abdominal inflammation, abdominal surgery or trauma, portal hypertension, invasion by malignant tumor, and oral contraceptive use can cause acquired SMVT [2,3]. The SMVT in the present case was not caused by tumor invasion as the HCC nodule was far away from the SMVT. Moreover, there was no hepatofugal portal blood flow and other parts of the portal system were free of thrombosis. The SMVT in our case was considered to be benign because there was no significant change in its pattern during long-term follow-up.
Endoscopic sclerotherapy with and without continuous vasopressin therapy may also cause SMVT [4]. Vasopressin therapy reduces portal blood flow via reversible vasoconstriction of splanchnic arterial blood vessels. This may cause stasis of portal blood flow in patients with severe portal hypertension. The clot induced by sclerotherapy may thus extend from the varices to the portal system when vasopressin therapy is used continuously for several days. When sclerotherapy is used without continuous vasopressin therapy, SMVT may be caused by the injected s c l e r o s a n t a n d / o r d i s t u r b a n c e i n p o r t a l hemodynamics. In the present case, endoscopic ligation therapy rather than sclerotherapy was used for
hemostasis. Although the patient also received continuous vasopressin therapy for 3 days, there was no evidence of thrombosis in other parts of the portal system. Therefore, the SMVT in our case was not caused by the extension of a clot from the varices to the portal system. Endoscopic ligation therapy alone was not considered to be a cause of SMVT because prophylactic ligation therapy did not cause further extension of the SMVT. The actual mechanism for the development of SMVT in our case remains unknown.
SMVT can be classified into acute and chronic presentations. Patients with acute SMVT present with symptoms of less than 4 weeks’ duration. Patients presenting with symptoms of more than 4 weeks’ duration but without bowel infarction, or those with SMVT diagnosed incidentally from clinically insignificant findings on abdominal imaging, can be classified as having chronic SMVT [2]. The patient in our case had chronic SMVT.
The symptoms of SMVT are not specific. They include abdominal pain, anorexia, diarrhea, nausea and vomiting, gastrointestinal bleeding, and even constipation [1–6]. The abdominal pain may vary from a mild and tolerable discomfort to severe and incapacitating distress. The most severe outcome of SMVT is intestinal infarction. In the present case, the symptom that may have been related to the thrombosis was frequent colic pain around the umbilical area of the abdomen after meals. Postprandial increase in portal blood flow, which needs to pass through the partially occluded superior mesenteric vein, may be the cause of this abdominal discomfort. Instructing the patient to eat only small meals may thus reduce the severity of this discomfort. Anticholinergic drugs with or without analgesia may be used in the management of such patients.
Systemic anticoagulation, transcatheter clot lysis, and surgical management are methods that can be used to treat benign SMVT [1–3,5,6,11–14]. They are usually applied immediately after the diagnosis is made. Systemic anticoagulation is usually the first choice for the treatment of benign SMVT because it is not difficult to perform. Transcatheter clot lysis may also be employed, but must be carried out by trained professionals. These methods carry a high risk of hemorrhage in patients with thrombocytopenia and/ or coagulopathy. Surgical intervention is mandatory for cases with localized or diffuse peritonitis [2], but it
Figure 2. Contrast-enhanced computerized tomography shows partial thrombosis of the superior mesenteric vein (arrow). There is no evidence of edema of the bowel wall.
Kaohsiung J Med Sci May 2003 • Vol 19 • No 5 M.S. Hsieh, Z.Y. Lin, W.L. Chuang, and W.Y. Chang
236
carries a high operative risk. Regular follow-up may be the treatment of choice for patients with benign SMVT diagnosed incidentally from clinically insignificant findings on abdominal imaging [3]. Local irradiation therapy and/or systemic chemotherapy may be considered in patients with malignant SMVT. Irradiation therapy carries the risk of irradiation enteritis. Systemic chemotherapy usually has severe side effects, especially in bone marrow suppression. In the present case, it was not possible to determine whether the SMVT was benign or malignant at the time of discovery because it was impossible to obtain specimens for pathologic examination. Moreover, the patient had a tendency towards severe bleeding and did not show evidence of peritonitis. Therefore, he received conservative treatment with regular follow-up using ultrasonography rather than aggressive treatment.
C
ONCLUSIONThe present case shows that partial SMVT in a cirrhotic patient with HCC may remain in a static condition for a long period. In clinical practice, it is impossible to predict at the time of discovery whether the partial SMVT will progress to complete occlusion. It may also be very difficult to determine the nature of SMVT in a cirrhotic patient with HCC at the time of discovery. R e g u l a r f o l l o w - u p o f p a r t i a l S M V T u s i n g ultrasonography may be one choice for patients with a tendency towards severe bleeding. Aggressive management of partial SMVT should be started in p a t i e n t s d e m o n s t r a t i n g p r o g r e s s i o n o f t h e thrombosis.
R
EFERENCES1. Gertsch P, Matthews J, Lerut J, et al. Acute thrombosis of the splanchnic veins. Arch Surg 1993;128:341–5.
2. Rhee RY, Gloviczki P. Mesenteric venous thrombosis. Surg
Clin North Am 1997;77:327–38.
3. Warshauer DM, Lee JK, Mauro MA, White GC. Superior mesenteric vein thrombosis with radiologically occult cause: a retrospective study of 43 cases. AJR Am J Roentgenol 2001; 177:837–41.
4. Thatcher BS, Sivak MV Jr, Ferguson R, Petras RE. Mesenteric venous thrombosis as a possible complication of endoscopic sclerotherapy: a report of two cases. Am J Gastroenterol 1986; 81:126–9.
5. Choudhary AM, Grayer D, Nelson A, Roberts I. Mesenteric venous thrombosis: a diagnosis not to be missed. J Clin
Gastroenterol 2000;31:179–82.
6. Skinner LJ, O’Donnell MJ, Kelly J, Cotter P. Causes of the acute abdomen: add thrombophilia to your list. Hosp Med 2000;61: 740–1.
7. Lin WSJ. Hepatoma in Taiwan: a pathologic study. Trans
Gastroenterol Soc ROC 1980;9:3–5.
8. Chen DS, Wang TH, Lai MY, Sung JL. Peritoneoscopic diagnosis in hepatoma. J Formos Med Assoc 1978;77:764–5. 9. Liu JD. Peritoneoscopic diagnosis of hepatocellular carcinoma.
Gastroenterol Endosc 1982;24:3–12.
10. Lin DY, Liaw YF, Chu CM, et al. Hepatocellular carcinoma in non-cirrhotic patients. Cancer 1984;54:1466–8.
11. Yankes JR, Uglietta JP, Grant J, Braun SD. Percutaneous transhepatic recanalization and thrombolysis of the superior mesenteric vein. AJR Am J Roentgenol 1988;151:289–90. 12. Poplausky MR, Kaufman JA, Geller SC, Waltman AC.
Mesenteric venous thrombosis treated with urokinase via the superior mesenteric artery. Gastroenterology 1996;110:1633–5. 13. Klempnauer J, Grothues F, Bektas H, Pichlmayr R. Results of portal thrombectomy and splanchnic thrombolysis for the surgical management of acute mesentericoportal thrombosis.
Br J Surg 1997;84:129–32.
14. Sze DY, O’Sullivan GJ, Johnson DL, Dake MD. Mesenteric and portal venous thrombosis treated by transjugular mesenteric thrombolysis. AJR Am J Roentgenol 2000;175:732–4.