and C-Reactive Protein Levels in Asymptomatic Patients With
Heterozygous Familial Hypercholesterolemia
Zhong-Xuan Ye, MD
a,b,c, Hao-Ming Cheng, MD
a,b, Kuan-Rau Chiou, MD
b,d,
Po-Hsun Huang, MD
a,b, Shing-Jong Lin, MD, PhD
a,b, and Min-Ji Charng, MD, PhD
a,b,*
The extent of coronary artery calcium (CAC) is correlated with coronary artery disease prognosis. However, the relation of CAC to endothelial function and high-sensitivity C-reactive protein (hs-CRP) in patients with asymptomatic heterozygous familial hyper-cholesterolemia (FH) requires clarification. The study aim was to investigate the relations among CAC, endothelial function, and hs-CRP in patients with asymptomatic heterozy-gous FH. Thirty-two patients with asymptomatic heterozyheterozy-gous FH (mean age 42 years) and 34 healthy control subjects (mean age 36 years) were enrolled. We measured CAC by electron-beam computed tomography and endothelial function by flow-mediated dilation of the brachial artery. A higher percentage of patients with FH had a positive CAC score compared with the control group. Comparing the FH group with detectable CAC (CAC score >0) and undetectable CAC (CAC score of 0), we found higher hs-CRP levels (0.29ⴞ 0.23 vs 0.07ⴞ 0.08 mg/dl, p ⴝ 0.001) and reduced flow-mediated dilation (0.04 ⴞ 0.03 vs 0.08 ⴞ 0.03, p ⴝ 0.005) in the detectable CAC group. Multivariate analysis showed an independent correlation of hs-CRP with detectable CAC (relative risk 5.034, 95% confi-dence interval 1.525 to 16.613, pⴝ 0.04). In conclusion, FH subjects with positive CAC scores have decreased flow-mediated dilation and increased hs-CRP levels. Furthermore, hs-CRP level is the only independent predictor of the presence of CAC. © 2007 Elsevier Inc. All rights reserved. (Am J Cardiol 2007;100:1119 –1123)
Familial hypercholesterolemia (FH) is an inherited autoso-mal dominant disorder that affects approximately 1 in 500 persons worldwide and is the most common inborn error of cholesterol metabolism.1 Coronary artery calcium (CAC),
measured by electron-beam computed tomography, has been widely used to assess the extent of atherosclerosis and predict the prognosis of coronary artery disease.2Hoffmann
et al3 have demonstrated that CAC is more extensive in
cases of coronary artery disease in patients with FH, pre-sumably resulting from a long history of increased low-density lipoprotein cholesterol (LDL-C) levels. However, the pathophysiology of vascular calcium deposition is un-clear, and its relation to inflammation markers needs further clarification.4,5In the present study, we tested the
hypothe-sis that a high cholesterol burden would lead to increased high-sensitivity C-reactive protein (hs-CRP) and endothelial dysfunction, and could thereby contribute to CAC in asymptomatic patients with heterozygous FH.
Methods
Patients with LDL-C levels⬎190 mg/dl and positive family history of hypercholesterolemia were enrolled in a genetic screening program for FH in Taiwan. Methodology used for mutation detection has been described before.6 Family
members who were genetically verified as not carrying an FH-related mutation allele and with LDL-C levels ⬍130 mg/dl were enrolled as the control group. The exclusion criteria were age ⬎55 years and history of medication for dyslipidemia, hypertension, or hyperglycemia. Patients with history of angina or coronary artery disease were also ex-cluded. The study protocol was approved by the institu-tional review board, and informed consent was obtained from each patient.
Demographic and clinical parameters including age, height, weight, body mass index, waist circumference, sys-tolic blood pressure, diassys-tolic blood pressure, and smoking habits were collected. After 12 to 14 hours overnight fast-ing, total plasma cholesterol, high-density lipoprotein cho-lesterol, and triglyceride were measured using commer-cially available kits (Roche, Mannheim, Germany). LDL-C was calculated according to the formula of Friedewald et al.7
The concentrations of apolipoprotein A1 and apolipoprotein B were measured by nephelometry (Behring Diagnostic,
Mar-aDivision of Cardiology, Department of Medicine, Taipei Veterans
General Hospital, Taipei; bCardiovascular Research Center, National
Yang-Ming University, Taipei; cDivision of Cardiovascular Medicine,
School of Medicine, Taipei Medical University, Wan-Fang Hospital, Taipei; anddDivision of Cardiology, Department of Medicine, Kaohsiung
Veterans General Hospital, Kaohsiung, Taiwan, Republic of China. Manu-script received February 12, 2007; revised manuManu-script received and ac-cepted May 8, 2007.
This work was supported by Grant NSC 95-2314-B-075-033 from the National Science Council of Taiwan, Research Grant V95C1-046 from Taipei Veterans General Hospital, and Grant V96ER2-003 from Genomic Medicine Research Center, Taipei Veterans General Hospital, Taipei, Taiwan.
*Corresponding author: Tel: 886-2-2875-7507; fax: 886-2-2875-6849.
E-mail address: [email protected] (M.J. Charng).
0002-9149/07/$ – see front matter © 2007 Elsevier Inc. All rights reserved. www.AJConline.org doi:10.1016/j.amjcard.2007.05.034
burg, Germany). Blood glucose was measured using an en-zymatic method. A highly sensitive latex-based immunoassay (Dade Behring, Milton Keynes, United Kingdom) was used for hs-CRP. Cholesterol–year score, which is dependent on cho-lesterol exposure duration and severity in people with FH, was selected to reflect the total burden of hypercholesterolemia.8
The score is computed by multiplying the initial serum cho-lesterol value (in milligrams per deciliter) by the age at diag-nosis and then adding the annually determined total cholesterol values.
Endothelium dependent flow-mediated dilation was as-sessed using a 7.5-MHz linear array transducer (Sonos 5500; Hewlett-Packard; Andover, Massachusetts) to scan the brachial artery in longitudinal section. All subjects were asked to fast, refrain from smoking, and withhold all med-ications for 12 hours. The procedure was performed in a quiet, air-conditioned room (22°C to 25°C). The left arm was stabilized with a cushion, and a sphygmomanometric cuff was placed on the forearm. A baseline image was acquired, and blood flow was estimated by time-averaging the pulsed Doppler velocity signals obtained from a sample volume at the middle of the artery. The cuff was then inflated to ⱖ50 mm Hg greater than systolic pressure to occlude the arteries for 5 minutes and released abruptly. Postocclusion diameters were obtained at 60, 80, 100, and 120 seconds after deflation. Flow-mediated dilation was calculated as the maximum postocclusion diameter relative to the average diameter before occlusion. A mid-artery pulsed Doppler signal was obtained immediately after cuff release and no later than 15 seconds after cuff deflation to assess hyperemic velocity.4
Electron-beam computed tomography was performed to measure CAC. A C-150 LXP scanner (Imatron, South San
Francisco, California) calibrated daily with air and water phantoms and twice monthly with contrast medium and resolution phantoms was used. Images were obtained using a 40- to 50-slice (3-mm thickness) protocol with image acquisition triggered to 60% to 80% of the electrocardio-graphic RR interval while respirations were held. Scans were interpreted by an experienced radiologist blinded to the participant’s group using the scoring method of Agat-ston et al.9A focus of coronary calcium was defined as the
presence of ⱖ4 contiguous pixels with ⬎130 Hounsfield units. Total CAC score was determined as the sum of individual scores of 4 major epicardial coronary arteries.10
All results were expressed as means with SDs for continuous variables and proportions for categorical vari-ables. Comparisons between groups were performed us-ing the Wilcoxon 2-sample test. Logarithmically trans-formed hs-CRP values were used in statistical analysis to achieve a normal distribution. Spearman correlation coeffi-cients were determined to assess association among CAC score, flow-mediated dilation, plasma lipid profile, lipopro-tein, blood pressure, and hs-CRP. To test whether variables had an independent effect on hs-CRP and CAC, stepwise logistic regression analysis was performed. All tests were 2-sided, and p values ⬍0.05 were considered statistically significant.
Results
A total of 32 untreated participants genetically verified as being heterozygous for FH (mean age 36⫾ 17.8 years, 56% male) and 34 family members (mean age 42.1 ⫾ 17.0 years, 50% male) genetically verified as not carrying an FH-related allele were enrolled in this study. All were of
Table 1
Comparison of subjects with or without heterozygous familial hypercholesterolemia (FH) mutation
Variable Control Group
(n⫽ 34) FH Group (n⫽ 32) p Value Age (yrs) 42.1⫾ 17.0 36.0⫾ 17.8 0.165 Men/women 17/17 18/14 0.618 Body weight (kg) 58.3⫾ 15.2 59.6⫾ 17.6 0.792
Body mass index (kg/m2) 23.4⫾ 3.9 22.1⫾ 4.9 0.243
Waist circumference (cm) 78.3⫾ 8.5 78.6⫾ 11.6 0.921
Systolic blood pressure (mm Hg) 109.5⫾ 11.0 115.8⫾ 14.4 0.106
Diastolic blood pressure (mm Hg) 65.0⫾ 9.8 67.3⫾ 10.8 0.448
Fasting blood glucose (mg/dl) 101.2⫾ 30.7 93.0⫾ 8.1 0.152
Total cholesterol (mg/dl) 196.6⫾ 38.1 299.7⫾ 73.7 ⬍0.001 Total triglyceride (mg/dl) 132.5⫾ 65.0 132.9⫾ 76.1 0.979 LDL-C (mg/dl) 120.0⫾ 38.1 218.4⫾ 66.1 ⬍0.001 HDL-C (mg/dl) 51.2⫾ 18.3 56.5⫾ 12.2 0.178 Total cholesterol/HDL-C 4.1⫾ 0.9 5.5⫾ 1.5 ⬍0.001 Cholesterol–year score 8,277.3⫾ 3,391.1 11,077.0⫾ 6,234.5 0.026 Apolipoprotein B (mg/dl) 99.2⫾ 30.3 151.5⫾ 41.2 ⬍0.001 Apolipoprotein A1 (mg/dl) 132.0⫾ 20.0 133.1⫾ 30.8 0.897 hs-CRP (mg/dl) 0.11⫾ 0.14 0.12⫾ 0.17 0.175 Flow-mediated dilation 0.08⫾ 0.03 0.06⫾ 0.04 0.023 CAC score 0.5⫾ 1.5 59.1⫾ 19.4 0.048
Patients with positive CAC score 3 (8.8%) 10 (31.2%) 0.022
Values presented as means⫾ SD where applicable. HDL-C⫽ high-density lipoprotein cholesterol.
Chinese descent. The characteristics of the mutations of the LDL receptor have been described before.6 None of the
participants had a history of cardiovascular disease, hyper-tension, or diabetes mellitus. Participant characteristics are listed in Table 1. Compared with healthy subjects, the FH subjects had significantly increased total cholesterol, LDL-C, and apolipoprotein B. The cholesterol–year scores were higher in the FH group. Subjects with FH had de-creased flow-mediated dilation and remarkably higher CAC scores. A higher percentage of subjects with FH in this series had a positive CAC score compared with the control group. Serum levels of hs-CRP were higher in the FH group, but the difference did not reach statistical signifi-cance.
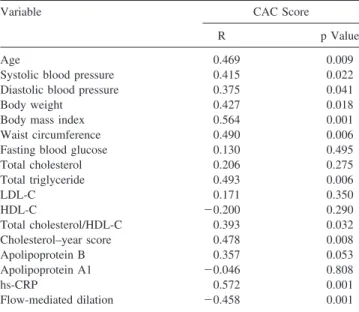
As the Spearman correlation analysis shows inTable 2, the CAC scores of patients with FH were correlated with
age, systolic blood pressure, cholesterol–year score, body weight, body mass index, waist circumference, total triglyc-eride, hs-CRP, and flow-mediated dilation. As presented in
Figure 1, cholesterol–year score was highly correlated with hs-CRP (r⫽ 0.574, p ⫽ 0.001). Cholesterol–year score was also correlated with CAC score (r ⫽ 0.478, p ⫽ 0.008), even though only 10 subjects with FH had detectable CAC. The 32 patients with FH-related mutations were further divided into 2 groups according to their CAC score: group 1 (n ⫽ 22) consisted of patients with FH without detectable CAC (CAC score of 0), and group 2 (n⫽ 10) consisted of patients with FH with detectable CAC (CAC score ⬎0).
Table 3compares baseline and clinical parameters between these 2 groups. The patients with FH with detectable CAC were older and had higher systolic/diastolic blood pressure and higher cholesterol–year scores than patients with unde-tectable CAC. The body weight, body mass index, and waist circumference were also increased in patients with detect-able CAC. As Figure 2 shows, patients with FH with de-tectable CAC had significantly increased hs-CRP values (p⬍0.001) and remarkably impaired flow-mediated dilation (p ⫽ 0.005). By stepwise logistic regression analysis ad-justed for age, total cholesterol, LDL-C, systolic/diastolic blood pressure, body mass index, waist circumference, and other conventional risk factors, hs-CRP value was an inde-pendent predictor for the presence of CAC in subjects with FH (relative risk 5.034, 95% confidence interval 1.525 to 16.613, p⫽ 0.04).
Discussion
In the present study, we demonstrated that subjects with asymptomatic heterozygous FH with positive CAC scores have decreased flow-mediated dilation and significantly in-creased levels of hs-CRP. On stepwise logistic regression analysis, hs-CRP is the only independent predictor for the presence of CAC in patients with FH.
Although CAC and hs-CRP are proven predictors of subclinical atherosclerosis,2,5the correlation between CAC
and hs-CRP results remains obscure.11–13 Huang et al4
re-ported that CAC was strongly related to endothelial dys-function but was not related to hs-CRP in patients with suspected coronary artery disease. Compared with partici-pants in other studies, our patients with FH were relatively healthy and untreated, and hypercholesterolemia was their only modifiable risk factor. Their atherosclerotic process, initiated by high cholesterol burden, was probably in the active inflammatory stage. In the absence of other con-founding cardiovascular risk factors, our study clearly showed that, in patients with FH, the CAC score corre-lated not only with cholesterol burden but also with hs-CRP values. Previous reports have also demonstrated the relations between inflammatory markers and vascular injury in FH.14,15In addition, stepwise logistic regression
analysis showed that the hs-CRP level was an indepen-dent predictor for the presence of CAC in FH. Zouridakis et al16demonstrated that increased C-reactive protein and
other mediators of inflammation signal rapid progression of coronary artery disease in patients with stable angina pectoris. Therefore, our study supports the notion that the mechanism for initiating coronary artery calcification in
Figure 1. Semi-log scatterplot for correlation between log hs-CRP (y axis) and cholesterol–year score (x axis). Cholesterol–year scores are correlated with hs-CRP (r⫽ 0.574, p ⫽ 0.001).
Table 2
Spearman correlation coefficients in 32 subjects with heterozygous familial hypercholesterolemia
Variable CAC Score
R p Value
Age 0.469 0.009
Systolic blood pressure 0.415 0.022
Diastolic blood pressure 0.375 0.041
Body weight 0.427 0.018
Body mass index 0.564 0.001
Waist circumference 0.490 0.006
Fasting blood glucose 0.130 0.495
Total cholesterol 0.206 0.275 Total triglyceride 0.493 0.006 LDL-C 0.171 0.350 HDL-C ⫺0.200 0.290 Total cholesterol/HDL-C 0.393 0.032 Cholesterol–year score 0.478 0.008 Apolipoprotein B 0.357 0.053 Apolipoprotein A1 ⫺0.046 0.808 hs-CRP 0.572 0.001 Flow-mediated dilation ⫺0.458 0.001 Abbreviation as inTable 1.
FH is vascular inflammation induced by a high choles-terol burden.17
Although it is difficult to infer a causal relation without a longitudinal follow-up study, our results clearly indicate the association between risk factors of hypercholesterolemia and increased hs-CRP level and the intermediate outcomes of CAC and flow-mediated dilation in heterozygous patients with FH. Despite a relatively small sample size, we still identified close correlations between these measurements in patients with heterozygous FH.
In conclusion, compared with patients with FH without detectable CAC scores, subjects with asymptomatic het-erozygous FH with detectable CAC have increased hs-CRP
and impaired endothelial function. Furthermore, the hs-CRP level is the only independent predictor of the presence of CAC. CAC is correlated with hs-CRP and flow-mediated dilation in patients with asymptomatic heterozygous FH.11
1. Austin MA, Hutter CM, Zimmern RL, Humphries SE. Genetic causes of monogenic heterozygous familial hypercholesterolemia: a HuGE prevalence review. Am J Epidemiol 2004;160:407– 420.
2. Taylor AJ, Feuerstein IM, Wong H, Barko W, Brazaitis M, O’Malley PG. Do conventional risk factors predict subclinical coronary artery disease? Results from the Prospective Army Coronary Calcium Project. Am
Heart J 2001;141:463– 468.
3. Hoffmann U, Bodlaj G, Derfler K, Bernhard C, Wicke L, Herold CJ, Kostner K. Quantification of coronary artery calcification in patients with FH using EBCT. Eur J Clin Invest 2001;31:471– 475. 4. Huang PH, Chen LC, Leu HB, Ding PY, Chen JW, Wu TC, Lin SJ.
Enhanced coronary calcification determined by electron beam CT is strongly related to endothelial dysfunction in patients with suspected coronary artery disease. Chest 2005;128:810 – 815.
5. Arad Y, Goodman KJ, Roth M, Newstein D, Guerci AD. Coronary calcification, coronary disease risk factors, C-reactive protein, and atherosclerotic cardiovascular disease events: the St. Francis Heart Study. J Am Coll Cardiol 2005;46:158 –165.
6. Charng MJ, Chiou KR, Chang HM, Cheng HM, Ye ZX, Lin SJ. Identi-fication and characterization of novel low-density lipoprotein receptor mutations of familial hypercholesterolaemia patients in Taiwan. Eur
J Clin Invest 2006;36:866 – 874.
7. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concen-tration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 1972;18:499 –502. 8. Cheng HM, Ye ZX, Chiou KR, Lin SJ, Charng MJ. Vascular stiffness
in familial hypercholesterolaemia is associated with C-reactive protein and cholesterol burden. Eur J Clin Invest 2007;37:197–206. 9. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte MJ,
Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990;15:827– 832. 10. Mahoney LT, Burns TL, Stanford W, Thompson BH, Witt JD, Rost
CA, Lauer RM. Coronary risk factors measured in childhood and young adult life are associated with coronary artery calcification in young adults: the Muscatine Study. J Am Coll Cardiol 1996;27:277– 284.
11. Bowden DW, Lange LA, Langefeld CD, Brosnihan KB, Freedman BI, Carr JJ, Wagenknecht LE, Herrington DM. The relationship between Table 3
Comparisons of basic characteristics of patients with heterozygous familial hypercholesterolemia (FH) with versus without coronary artery calcium (CAC)
Variable Group 1 (CAC score of 0; n⫽ 22) Group 2 (CAC score⬎0; n ⫽ 10) p Value Age (yrs) 32.0⫾ 15.6 49.2⫾ 18.3 0.014 Men/women 12/10 6/4 0.878
Systolic blood pressure (mm Hg) 112.9⫾ 11.8 126.3⫾ 15.7 0.015
Diastolic blood pressure (mm Hg) 65.1⫾ 8.7 74.8⫾ 12.5 0.022
Body weight (kg) 54.3⫾ 14.2 73.2⫾ 18.8 0.004
Body mass index (kg/m2) 20.4⫾ 3.7 26.4⫾ 5.0 0.001
Waist circumference (cm) 75.0⫾ 9.8 87.8⫾ 11.0 0.003
Fasting blood glucose (mg/dl) 92.9⫾ 7.0 94.6⫾ 10.7 0.619
Total cholesterol (mg/dl) 288.8⫾ 76.0 329.7⫾ 70.9 0.180 Total triglyceride (mg/dl) 118.4⫾ 77.3 171.7⫾ 69.5 0.086 LDL-C (mg/dl) 210.2⫾ 64.7 240.4⫾ 67.6 0.270 HDL-C (mg/dl) 57.9⫾ 14.1 53.2⫾ 7.6 0.357 Total cholesterol/HDL-C 5.2⫾ 1.5 6.3⫾ 1.2 0.062 Cholesterol–year score 9597.0⫾ 5,397.5 15,924.0⫾ 5,890.0 0.008 Apolipoprotein B (mg/dl) 141.7⫾ 40.3 178.2⫾ 39.7 0.030 Apolipoprotein A1 (mg/dl) 136.0⫾ 32.0 132.6⫾ 29.4 0.786 hs-CRP (mg/dl) 0.07⫾ 0.08 0.29⫾ 0.23 ⬍0.001 Flow-mediated dilation 0.08⫾ 0.03 0.04⫾ 0.03 0.005
Values presented as means⫾ SD where applicable. Abbreviation as inTable 1.
Figure 2. Comparisons of hs-CRP and flow-mediated dilation between groups 1 and 2 in patients with heterozygous FH. Patients with FH with detectable CAC have significantly increased hs-CRP values (p⬍0.001) and remarkably impaired flow-mediated dilation (p⫽ 0.005). Group 1 (n ⫽ 22) comprises patients with no detectable CAC (CAC score of 0); group 2 (n⫽ 10) comprises those with detectable CAC (CAC score ⬎0).
C-reactive protein and subclinical cardiovascular disease in the Diabetes Heart Study (DHS). Am Heart J 2005;150:1032–1038. 12. Meng Q, Lima JA, Lai H, Vlahov D, Celentano DD, Margolick JB,
Lai S. Elevated C-reactive protein levels are associated with endo-thelial dysfunction in chronic cocaine users. Int J Cardiol 2003;88: 191–198.
13. Hunt ME, O’Malley PG, Vernalis MN, Feuerstein IM, Taylor AJ. C-reactive protein is not associated with the presence or extent of calcified subclinical atherosclerosis. Am Heart J 2001;141:206 –210. 14. Hovingh GK, Brownlie A, Bisoendial RJ, Dube MP, Levels JH,
Petersen W, Dullaart RP, Stroes ES, Zwinderman AH, de Groot E, et al. A novel apoA-I mutation (L178P) leads to endothelial dysfunction, increased arterial wall thickness, and premature coronary artery dis-ease. J Am Coll Cardiol 2004;44:1429 –1435.
15. Brown SL, Raal FJ, Panz VR, Stevens BA, Veller MG. High-dose atorvastatin therapy is required for significant improvement of endo-thelial function in heterozygous familial hypercholesterolaemic pa-tients. Cardiovasc J S Afr 2004;15:70 –75.
16. Zouridakis E, Avanzas P, Arroyo-Espliguero R, Fredericks S, Kaski JC. Markers of inflammation and rapid coronary artery disease pro-gression in patients with stable angina pectoris. Circulation 2004;110: 1747–1753.
17. Sangiorgi G, Rumberger JA, Severson A, Edwards WD, Gregoire J, Fitzpatrick LA, Schwartz RS. Arterial calcification and not lumen stenosis is highly correlated with atherosclerotic plaque burden in humans: a histologic study of 723 coronary artery segments using nondecalcifying methodology. J Am Coll Cardiol 1998;31:126 – 133.