INTERESTING IMAGE
Title: Rare Breast and Adrenal Gland Metastases From Small-Cell Neuroendocrine Carcinoma of Uterine Cervix
Authors: Te-Chun Hsieh, MD,*† Yu-Chin Wu, MD,*‡ Shung-Shung Sun, MD,*† Chun-Fan Yang, MD,§ Kuo-Yang Yen, BS,*† Ji-An Liang, MD,¶ and Chia-Hung Kao, � MD* �
Abstract: A 46-year-old woman was initially diagnosed with rare small-cell
neuroendocrine carcinoma of uterine cervix with regional lymph node metastases. She hesitated to undergo the suggested concurrent chemoradiation therapy and was lost to follow-up for 4 months. Then, a FDG PET/CT scan was requested for restaging her disease and disclosed other abnormal findings in the breast and adrenal gland that probably indicated malignancies. The following pathologic examination confirmed the diagnosis of rare breast and adrenal gland metastases from small-cell neuroendocrine carcinoma of uterine cervix.
Key Words: small-cell neuroendocrine carcinoma, uterine cervix, FDG PET/CT, breast metastasis, adrenal gland metastasis
From the *Department of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung, Taiwan; †Department of Biomedical Imaging and Radiological
Science, China Medical University, Taichung, Taiwan; ‡Departmentof Nuclear Medicine, National Taiwan University Hospital Hsin-Chu Branch, Hsin-Chu, Taiwan; Departments of §Pathology and ¶Radiation Oncology, China Medical University Hospital, Taichung, Taiwan; and School of Medicine, China Medical University, � Taichung, Taiwan.
Conflicts of interest and sources of funding: none declared.
Reprints: Chia-Hung Kao, MD, and Shung-Shung Sun, MD, Department of Nuclear Medicine and PET Center, China Medical University Hospital, No. 2, Yuh-Der Rd, Taichung 404, Taiwan. E-mail: d10040@mail.cmuh.org.tw and
FIGURE 1. A 46-year-old woman presented with intermittent vaginal spotting, dysmenorrhea, and menorrhagia for 2 months. The blood test disclosed abnormal carcinoembryonic antigen (10.39 ng/mL). The pelvic examination for the uterine cervix revealed a bulky, endophytic, necrotic tumor with easy contact bleeding. Histopathologic examination of the tumor showed small neoplastic cells with very scant cytoplasm, round/oval nuclei, finely granular chromatin, inconspicuous nucleoli (A, B), and positive immunohistochemical stain for synaptophysin (C). These features confirmed the
diagnosis of small-cell neuroendocrine carcinoma (SCNC).
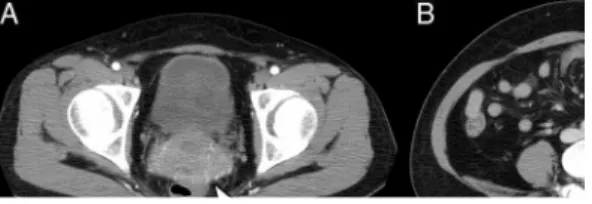
FIGURE 2. Subsequently, contrast-enhanced computed tomography (CT) of the
abdomen and pelvis for routine staging workup revealed not only the cervical tumor (A; white arrowhead) but also many enlarged lymph nodes in the peritumoral areas as well as bilateral internal iliac and left common iliac lymphatic regions (B; black arrowhead). These findings suggested cervical cancer with pelvic lymph node metastases. However, she chose to receive alternative herbal therapy, not suggested concurrent chemoradiation therapy.
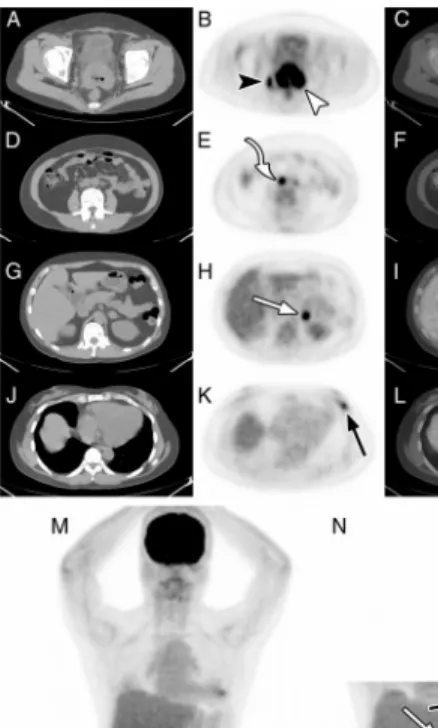
FIGURE 3. Four months later, treatment failure and disease progression were suspected because of gradually increasing carcinoembryonic antigen (116.25 ng/mL). Then, she underwent fluorodeoxyglucose positron emission tomography (FDG PET)/CT for restaging. Besides the known cervical tumor and metastatic lymph nodes in the pelvis (A–C, M, and N; white and black arrowheads), FDG PET/CT demonstrated new
metastatic lymph nodes in the right common iliac region and bilateral para-aortic region (D–F, M, and N; curved arrow). In addition, there were unexpected FDG-avid lesions in the left adrenal gland (G–I, M, and N; white straight arrows) and left breast (J–L, M, and N; black straight arrows) that were also suspected as malignancies.
FIGURE 4. SCNC of the uterine cervix with metastases to the breast and adrenal gland was rare, and primary malignancy in the breast was much more frequent. Therefore, pathologic confirmation seemed necessary. Biopsy of the left breast lesion showed similar features (A, B) as SCNC of the uterine cervix. Based on serial clinical, radiologic,
and pathologic findings, a diagnosis of SCNC of uterine cervix with lymph node, breast, and adrenal gland metastases was made.
Extrapulmonary small-cell carcinoma (SCC) accounts for only 5% of all SCC,1
most common in the gastrointestinal tract, genitourinary system, and of unknown origin.2– 6 SCC of uterine cervix is diagnosed based on hematoxylin and eosin stain alone,
regardless of its neuroendocrine differentiation.7 Histologically, SCC of uterine cervix
resembles SCC in other sites, with the characteristic features as small cells with hyperchromatic nuclei, scant cytoplasm, inconspicuous nucleoli, frequent mitoses, and necrosis. Immunohistochemical neuroendocrine markers are present in up to 80% of SCC of uterine cervix.8 SCNC of uterine cervix is rare (less than 5% of all cervical cancers)7
and usually considered as an extrapulmonary variant of pulmonary SCC. Because of the extremely aggressive behavior and relatively poor prognosis in comparison with other subtypes of cervical cancers,7,9 –12 the nodal and distant metastases of SCNC of uterine
cervix are frequently observed during the period of initial diagnosis or early post-treatment follow-up. However, there are only sporadic reports mentioned about 7,10,13,14
and adrenal gland14 metastases from SCNC of uterine cervix.
Clinically, SCNC of uterine cervix is seldom curable and usually needs more intensive adjuvant chemotherapy to improve the survival. The 5-year survival rate, even for patients with early-stage disease, ranges from 30% to 60%.7,9,10,14 Although the prognosis
remains poor, concurrent chemoradiation therapy to treat patients with advanced-stage diseases has been tried.11 Currently, there is still lack of optimal chemotherapy for
SCNC.14 However, extrapolation of the regimen for pulmonary SCC has been regarded as
Our report demonstrates the clinical scenario to diagnose a rare aggressive primary malignancy with metastases to unusual sites. FDG PET/CT is useful for systemic survey of a known malignancy but may also disclose other lesions with uncertain etiologies. Pathologic confirmation of these lesions is helpful to determine further therapeutic strategy properly.
References:
1. Richardson RL, Weiland LH. Undifferentiated small cell carcinomas in extrapulmonary sites. Semin Oncol. 1982;9:484–496.
2. Haider K, Shahid RK, Finch D, et al. Extrapulmonary small cell cancer: a Canadian province’s experience. Cancer. 2006;107:2262–2269.
3. Sayed MH, Farghaly HR, Nguyen NC, et al. Interesting image. Extrapulmonary small cell carcinoma in prostate: detection with F-18 FDG PET/CT. Clin Nucl Med.
2010;35:38 –39.
4. Yilmaz M, Celen Z, Sevinc A, et al. Widespread metastases in small cell carcinoma of the prostate on FDG PET/CT. Clin Nucl Med. 2009;34:598– 600.
5. Jones K, Subramaniam RM, Durnick DK, et al. F-18-FDG-PET/CT imaging of small cell carcinoma of the colon. Clin Nucl Med. 2008;33:645– 646.
6. Tulchinsky M. F-18 FDG PET/CT in primary gastric small cell carcinoma. Clin Nucl Med. 2009;34:44–47.
7. Viswanathan AN, Deavers MT, Jhingran A, et al. Small cell neuroendocrine carcinoma of the cervix: outcome and patterns of recurrence. Gynecol Oncol. 2004;93:27–33. 8. Sevin BU, Method MW, Nadji M, et al. Efficacy of radical hysterectomy as treatment for patients with small cell carcinoma of the cervix. Cancer. 1996;77:1489 –1493. 9. Crowder S, Tuller E. Small cell carcinoma of the female genital tract. Semin Oncol. 2007;34:57– 63.
10. Chan JK, Loizzi V, Burger RA, et al. Prognostic factors in neuroendocrine small cell cervical carcinoma: a multivariate analysis. Cancer. 2003;97:568– 574.
neuroendocrine carcinoma of the uterine cervix treated surgically: results of a multi-center retrospective Korean study. Ann Oncol. 2008;19: 321–326.
12. McCusker ME, Cote TR, Clegg LX, et al. Endocrine tumors of the uterine cervix: incidence, demographics, and survival with comparison to squamous cell carcinoma. Gynecol Oncol. 2003;88:333–339.
13. Shin HJ, Caraway NP. Fine-needle aspiration biopsy of metastatic small cell carcinoma from extrapulmonary sites. Diagn Cytopathol. 1998;19:177–181.
14. Chang TC, Lai CH, Tseng CJ, et al. Prognostic factors in surgically treated small cell cervical carcinoma followed by adjuvant chemotherapy. Cancer. 1998;83:712–718. 15. Hoskins PJ, Swenerton KD, Pike JA, et al. Small-cell carcinoma of the cervix: fourteen years of experience at a single institution using a combined-modality regimen of involved-field irradiation and platinum-based combination chemotherapy. J Clin Oncol. 2003;21:3495–3501.
16. Brennan SM, Gregory DL, Stillie A, et al. Should extrapulmonary small cell cancer be managed like small cell lung cancer? Cancer. 2010;116: 888–895.