Date 2014/August/16
Type of manuscript: Original article
Manuscript title: Actively using clopidogrel correlates with an increased risk of acute pancreatitis in Taiwan
Running head: clopidogrel and acute pancreatitis Authors' full names:
Shih-Wei Lai1,2, Cheng-Li Lin3,4, Kuan-Fu Liao5,6
1School of Medicine, China Medical University and 2Department of Family Medicine, China Medical University Hospital, Taichung, Taiwan
3Department of Public Health, China Medical University and 4Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan
5Graduate Institute of Integrated Medicine, China Medical University and 6Department of Internal Medicine, Taichung Tzu Chi General Hospital, Taichung, Taiwan
Corresponding author: Kuan-Fu Liao, Department of Internal Medicine, Taichung Tzu Chi General Hospital, No.66, Sec. 1, Fongsing Road, Tanzi District, Taichung City, 427, Taiwan
Phone: 886-4-2205-2121 Fax: 886-4-2203-3986
E-mail: [email protected]
ABSTRACT
Objectives. The aim of this study is to assess whether there is an association between clopidogrel use and risk of acute pancreatitis in Taiwan.
Methods. We conducted a case-control study using the database of the Taiwan National Health Insurance Program from 2000 to 2011. There were 5644 subjects aged 20-84 years with a first-time attack of acute pancreatitis as the case group and 22576 randomly selected sex-matched and age-matched subjects without acute pancreatitis as the control group. We defined clopidogrel use as “actively using” if the final clopidogrel
prescription was filled between 0-7 days before the date of diagnosing acute pancreatitis, or “not actively using” if the final clopidogrel prescription was filled 8 days ≧ before the date of diagnosing acute pancreatitis, respectively. Subjects who never used clopidogrel were defined as never use. The multivariable logistic regression model was used to calculate the odds ratio (OR) and 95% confidence interval (CI) of acute pancreatitis associated with clopidogrel use.
Results. Comparison of subjects actively using clopidogrel to those with never use of clopidogrel, the adjusted OR of acute pancreatitis was 8.46 (95%CI 5.25, 13.7). The adjusted OR decreased to 1.16 among subjects not actively using clopidogrel (95%CI 0.95, 1.43).
Conclusions. Persons actively using clopidogrel are at an increased risk of acute pancreatitis. Further studies are necessary to prove the causal relationship.
INTRODUCTION
Acute pancreatitis is a life-threatening condition characterized by acute inflammation of the pancreas. The epidemiological studies have revealed that gallstones and alcoholism account for 75-80% of all cases of acute pancreatitis. In addition, a growing body of evidence shows that many drugs have been reported to be associated with acute pancreatitis, with estimation of 2% of all cases.
Clopidogrel is an antiplatelet agent commonly used in cardiovascular disease with significant benefits. However, bleeding is the major adverse event of clopidogrel therapy, which may frequently result in discontinuation or noncompliance of this agent.
So far, no case of acute pancreatitis associated with clopidogrel use has been published, whereas U.S. Food and Drug Administration (FDA) has reported that from 1999 to 2012,
240 persons (0.36%) had acute pancreatitis among 67298 persons reporting to have adverse events when using clopidogrel. Since the causal relationship between
clopidogrel use and risk of acute pancreatitis remains uncertain in U.S. FDA report, we conducted a population-based case-control study using the database of the Taiwan National Health Insurance Program to assess whether there is an association between clopidogrel use and risk of acute pancreatitis.
MATERIALS AND METHODS
A case-control study was conducted to use the database of the Taiwan National Health Insurance Program. Briefly speaking, the insurance program started in March 1995 and it provided outpatient, hospitalization and emergency services. Nearly, 99% of 23 million citizens living in Taiwan were covered. In this program, diseases were diagnosed based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9 codes). The program details can be found in previous studies. This study was approved by the Institutional Review Board (IRB) of China Medical University and
Hospital in Taiwan (CMU-REC-101-012).
Participants
From 2000 to 2011, subjects aged 20-84 with a first-time attack of acute pancreatitis were defined as the case group (ICD-9 code 577.0).We defined the index date for each case as the date of diagnosing acute pancreatitis. For each case with acute pancreatitis, we
randomly selected four subjects without acute pancreatitis from the same database as control group. Both groups were matched by sex, age (within five years), and index year of diagnosing acute pancreatitis. Subjects with chronic pancreatitis or pancreatic cancer before the date of diagnosing acute pancreatitis were excluded from this study.
Comorbidities potentially associated with acute pancreatitis risk
The comorbidities before the date of diagnosing acute pancreatitis potentially associated with acute pancreatitis risk were included as following: alcoholism, biliary
stone, chronic obstructive pulmonary disease, diabetes mellitus, hepatitis B infection, hepatitis C infection, hypertriglyceridemia, as well as cardiovascular disease including coronary artery disease, heart failure, cerebrovascular disease and peripheral
atherosclerosis. All comorbidities were diagnosed based on ICD-9 codes. Definition of clopidogrel exposure
Clopidogrel's active metabolite inhibits platelet adenosine diphosphate (ADP) receptor binding irreversibly. since platelet lifespan is about 7-10 days, we used the period of 7 days as a cut-point. We defined clopidogrel use as “actively using” if the final
clopidogrel prescription was filled between 0-7 days before the date of diagnosing acute pancreatitis, or “not actively using” if the final clopidogrel prescription was filled 8 ≧ days before the date of diagnosing acute pancreatitis, respectively. Subjects who never used clopidogrel were defined as never use.
Statistical Analysis
In the beginning, we used the Chi-square test to compare the differences between the case group and the control group for distributions of demographic profile, clopidogrel use and comorbidities. Then, all covariables were included in a univariable unconditional logistic regression model. Last, only those found significantly were further included in a
multivariable unconditional logistic regression model to calculate the odds ratio (OR) and 95% confidence interval (CI) for risk of acute pancreatitis associated with clopidogrel use and comorbidities. The probability value < 0.05 was considered statistically significant (SAS software version 9.1, SAS Institute Inc., Cary, North Carolina, USA).
RESULTS
Characteristics of the study population
pancreatitis as controls were included with equal distributions in sex and age (Table 1). The mean ages (standard deviation) were 53.59 (16.53) years in the case group and 53.13 (16.68) years in the control group. The cases tended to have higher proportions of clopidogrel use, alcoholism, biliary stone, cardiovascular disease, chronic obstructive pulmonary disease, diabetes mellitus, hepatitis B, hepatitis C and hypertriglyceridemia (P <0.001 for all ).
Odds ratio of acute pancreatitis associated with clopidogrel use and comorbidities After adjusted for adjusted for sex, age, alcoholism, biliary stone, cardiovascular disease , cardiovascular disease, diabetes mellitus, hepatitis B, hepatitis C and
hypertriglyceridemia, comparison of persons actively using clopidogrel to those with never use of clopidogrel, the adjusted OR of acute pancreatitis was 8.46 (95%CI 5.25, 13.7). The adjusted OR decreased to 1.16 among persons not actively using clopidogrel (95%CI 0.95, 1.43) (Table 2). In addition, alcoholism (OR 12.90, 95%CI 11.00,15.30), biliary stone (OR 12.29, 95%CI 10.99,13.73), cardiovascular disease (OR 1.32, 95%CI 1.21,1.45), chronic obstructive pulmonary disease (OR 1.30,95%CI 1.19, 1.42), diabetes mellitus (OR 1.98, 95%CI 1.81, 2.16), hepatitis B (OR 1.56, 95%CI 1.36, 1.79), hepatitis C (OR 2.03, 95%CI 1.70, 2.44) and hypertriglyceridemia (OR 1.40, 95%CI 1.29,1.51), were also significantly associated with risk of acute pancreatitis.
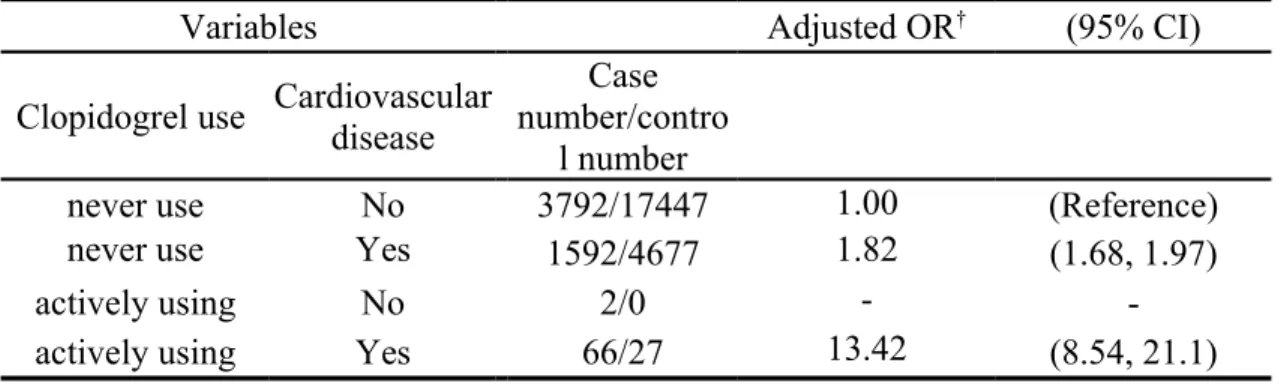
Interaction effect between actively using clopidogrel and cardiovascular disease on risk of acute pancreatitis
In further analysis, as a reference of persons without cardiovascular disease and with never use of clopidogrel, The adjustedOR of acute pancreatitis was 1.82 among persons with cardiovascular disease and those who never used clopidogrel (95%CI 1.68, 1.97) and the adjustedOR significantly increased to 13.42 among persons with cardiovascular disease and those actively using clopidogrel (95%CI 8.54, 21.1) (Table 3).
DISCUSSION
To the best of our knowledge, this is the first pharmacoepidemiological study using the population-based claim data to assess the association between clopidogrel use and risk of acute pancreatitis. No such data exist to be compared with. During the study period, among 5644 cases with acute pancreatitis, 260 persons (4.6%) ever used clopidogrel. We
found that only persons actively using clopidogrel were at an 8.46-fold increased odds for acute pancreatitis. If not actively using clopidogrel, the risk would decrease. In further analysis, as a reference of persons without cardiovascular disease and with never use of clopidogrel, The adjusted OR of acute pancreatitis was 1.82 among persons with cardiovascular disease and with never use of clopidogrel (95%CI 1.68, 1.97) and the
adjusted OR significantly increased to 13.42 among persons with cardiovascular disease
and those actively using clopidogrel (95%CI 8.54, 21.1). This means that cardiovascular disease is associated with the risk for acute pancreatitis, which is compatible with Bexelius et al’s study. Actively using clopidogrel would markedly enhance the risk of acute pancreatitis among persons with cardiovascular disease. Because the subject number was too small, no estimation could be shown among persons actively using clopidogrel and without cardiovascular disease. Therefore, we cannot notice whether actively using clopidogrel alone is associated with the risk for acute pancreatitis among those without cardiovascular disease.
Although it appears that this study examined a novel hypothesis, several issues need to be considered in the interpretation of the results obtained. First, though smoking is found to be associated with acute pancreatitis, smoking status was not recorded in this database. We used chronic obstructive pulmonary disease as an indirect variable instead of
smoking. Second, the exact cause of acute pancreatitis could not be documented in this database. Whether the association between actively using clopidogrel and acute pancreatitis is causal remains unclear. Therefore, interpretation of our results should be more cautious. Third, because no case report of acute pancreatitis associated with clopidogrel use has been published, the pathological mechanism cannot be completely clarified from this observational study. Therefore, whether clopidogrel has a direct effect on the pancreas or persons actively using clopidogrel have other unfound factors to be associated with acute pancreatitis needs further investigation. Forth, another limitation of this study is the inability to incorporate considerations of current and cumulative dosage of clopidogrel use due to lack of data from this database. Fifth, other drugs prescribed to patients with cardiovascular disease may confer risk for acute
pancreatitis, but this possibility was not examined in this study. Last, the diagnosis accuracy of diseases based on ICD-9 codes, such as acute pancreatitis, bililary stone,
diabetes mellitus, hepatitis B infection, hepatitis C infection and hypertriglyceridemia, has been validated in previous studies.
We conclude that persons actively using clopidogrel are at an increased risk of acute pancreatitis. Further studies remain necessary to prove the causal relationship.
Funding
This study was supported in part by Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW103-TDU-B-212-113002). The funding agency did not influence the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Specific author contributions
Shih-Wei Lai: (1) substantially contributed to the conception of this article; (2) planned and conducted the study; (3) initiated the draft of the article and critically revised the article.
Cheng-Li Lin: (1) conducted data analysis; (2) critically revised the article. Kuan-Fu Liao: (1) planned and conducted the study; (2) participated in data interpretation; (3) critically revised the article.
Conflict of Interest Statement
REFERENCES
[1] Cappell MS. Acute pancreatitis: etiology, clinical presentation, diagnosis, and therapy. Med Clin North Am. 2008;92:889-923, ix-x.
[2] Ksiadzyna D. Drug-induced acute pancreatitis related to medications commonly used in gastroenterology. Eur J Intern Med. 2011;22:20-5.
[3] Nitsche CJ, Jamieson N, Lerch MM, Mayerle JV. Drug induced pancreatitis. Best Pract Res Clin Gastroenterol. 2010;24:143-55.
[4] Mangalpally KK, Kleiman NS. The safety of clopidogrel. Expert Opin Drug Saf. 2011;10:85-95.
[5] eHealthMe study from FDA and social media reports. Review: could Plavix cause Pancreatitis acute? http://www.ehealthme.com/print/ds16470672. [cited in 2014 April].
[6] Liao KF, Lai SW, Li CI, Chen WC. Diabetes mellitus correlates with increased risk of pancreatic cancer: a population-based cohort study in Taiwan. J Gastroenterol Hepatol. 2012;27:709-13.
[7] Lai SW, Liao KF, Liao CC, Muo CH, Liu CS, Sung FC. Polypharmacy correlates with increased risk for hip fracture in the elderly: a population-based study. Medicine (Baltimore). 2010;89:295-9.
[8] Lai SW, Muo CH, Liao KF, Sung FC, Chen PC. Risk of acute pancreatitis in type 2 diabetes and risk reduction on anti-diabetic drugs: a population-based cohort study in Taiwan. Am J Gastroenterol. 2011;106:1697-704.
[9] Chang MC, Su CH, Sun MS, Huang SC, Chiu CT, Chen MC, et al. Etiology of acute pancreatitis--a multi-center study in Taiwan. Hepatogastroenterology. 2003;50:1655-7. [10] Bexelius TS, Ljung R, Mattsson F, Lagergren J. Cardiovascular disease and risk of acute pancreatitis in a population-based study. Pancreas. 2013;42:1011-5.
[11] Ellis KJ, Stouffer GA, McLeod HL, Lee CR. Clopidogrel pharmacogenomics and risk of inadequate platelet inhibition: US FDA recommendations. Pharmacogenomics. 2009;10:1799-817.
[12] Bates ER, Lau WC, Angiolillo DJ. Clopidogrel-drug interactions. J Am Coll Cardiol. 2011;57:1251-63.
[13] Sadr-Azodi O, Andren-Sandberg A, Orsini N, Wolk A. Cigarette smoking, smoking cessation and acute pancreatitis: a prospective population-based study. Gut. 2012;61:262-7.
[14] Lai SW, Sung FC, Lin CL, Liao KF. Use of Proton Pump Inhibitors Correlates with Increased Risk of Pancreatic Cancer: A Case-Control Study in Taiwan. Kuwait Medical Journal 2014;46:44-8.
Table 1. Characteristics between persons with and without acute pancreatitis Controls Number = 22576 Cases Number = 5644 n (%) n (%) P value† Sex 0.99 male 8404 37.23 2101 37.23 female 14172 62.77 3543 62.77
Age group (years) 0.99
20-39 5558 24.62 1390 24.63 40-64 10466 46.36 2616 46.35 65-84 6552 29.02 1638 29.02 Clopidogrel use* <0.001 never use 22124 98.00 5384 95.39 actively using 27 0.12 68 1.20
not actively using 425 1.88 192 3.40
Comorbidities before index date**
Alcoholism 217 0.96 583 10.33 <0.001
Biliary stone 554 2.45 1255 22.24 <0.001
Cardiovascular disease 5118 22.67 1845 32.69 <0.001
Chronic obstructive pulmonary disease 3529 15.63 1230 21.79 <0.001 Diabetes mellitus 3257 14.43 1543 27.34 <0.001 Hepatitis B 835 3.70 442 7.83 <0.001 Hepatitis C 389 1.72 295 5.23 <0.001 Hypertriglyceridemia 5285 23.41 2078 36.82 <0.001
Data are presented as the number of subjects in each group, with percentages given in parentheses.
†Chi-square test comparing subjects with and without acute pancreatitis
*We defined clopidogrel use as “actively using” if the final clopidogrel prescription was filled between 0-7 days before the date of diagnosing acute pancreatitis, or “not actively using” if the final clopidogrel prescription was filled 8 days ≧ before the date of diagnosing acute pancreatitis, respectively. Subjects who never used clopidogrel were defined as never use.
Table 2. Odds ratio and 95% confidence interval of acute pancreatitis associated with clopidogrel use and other comorbidities
Crude Adjusted†
Variable OR (95% CI) OR (95% CI)
Clopidogrel use (never use as a reference)
actively using 10.3 (6.62, 16.2) 8.46 (5.25, 13.7)
not actively using 1.86 (1.56, 2.21) 1.16 (0.95, 1.43)
Comorbidities before index date (yes vs. no)
Alcoholism 11.87 (10.13, 13.91) 12.90 (11.00,15.30)
Biliary stone 11.37 (10.23, 12.63) 12.29 (10.99,13.73)
Cardiovascular disease 1.66 (1.55, 1.77) 1.32 (1.21,1.45)
Chronic obstructive pulmonary disease 1.50 (1.40, 1.62) 1.30 (1.19, 1.42)
Diabetes mellitus 2.23 (2.08, 2.39) 1.98 (1.81, 2.16)
Hepatitis B 2.21 (1.96, 2.49) 1.56 (1.36, 1.79)
Hepatitis C 3.15 (2.70, 3.67) 2.03 (1.70,2.44)
Hypertriglyceridemia 1.91 (1.79, 2.03) 1.40 (1.29,1.51)
†Covariables which were significantly associated with the risk of acute pancreatitis in a univariable unconditional logistic regression model were further examined by a multivariable unconditional logistic regression model.
Additionally adjusted for sex, age, alcoholism, biliary stone, cardiovascular disease ,
cardiovascular disease, diabetes mellitus, hepatitis B, hepatitis C and hypertriglyceridemia
Table 3. Interaction effect between actively using clopidogrel and cardiovascular disease on risk of acute pancreatitis
Variables Adjusted OR† (95% CI)
Clopidogrel use Cardiovascular disease
Case number/contro
l number
never use No 3792/17447 1.00 (Reference)
never use Yes 1592/4677 1.82 (1.68, 1.97)
actively using No 2/0 -
-actively using Yes 66/27 13.42 (8.54, 21.1)