應用中藥板藍根於放射線黏膜炎之研究; Application of Ban-Lan-Gen (Radix of Isatis indigoaca) in Radiation-Induced Mucositis
99
0
0
全文
(2) 應用中藥板藍根於放射線黏膜炎之研究. 摘要. 本品為十字花科植物菘藍的根,是一種常用於涼血止血、清熱解 毒、涼血利咽的常用中藥。根據現代藥學研究,板藍根主要成分含靛 藍、靛玉紅等成分,具有抗病毒、清熱、解毒和抗發炎功效,並且毒 性與副作用都很小。放射線口腔炎是頭頸部癌症病人接受放射治療期 間最主要的急性副作用,目前主要的治療藥物其藥效有限,病人常需 要暫停放射治療來緩和症狀。我們的目的是應用板藍根以降低放射性 口腔炎並且評估其臨床效果,並探討可能的作用機轉,以期可在臨床 廣泛的應用。 方法: 分為二部分:(1). 應用板藍根於降低放射線口腔炎的臨床試驗: 針對頭頸部癌症病人接受放射治療時,將病人分成兩組,一組為口服 板藍根組,另ㄧ組為對照組(口服生理食鹽水),進行臨床觀察並評估 放射性口腔炎的嚴重程度;(2). 小鼠在經放射線照射後投與板藍根, 評估其抗發炎的效果:以 8 週 BALB/c 公鼠,經連續三天以放射線 9 MeV 照射全身共 5.4 Gy 的劑量,投與板藍根ㄧ周後犧牲,評估 BALB/c 公鼠體內的發炎指標。 i.
(3) 結果: 在臨床試驗部分,ㄧ共有 20 位病人進行板藍根的臨床試驗,其 中板藍根組 11 位,對照組 9 位。臨床試驗證明,板藍根組相對於對 照組可有效降低放射線口腔炎(P=0.01)、厭食(P =0.002)和對於病人因 放射線口腔炎而引起的吞嚥困難(P =0.02)能顯著改善。病人接受放射 治療所需的休息天數也能下降,但未達到顯著意義(P =0.06)。板藍根 組的病人血清中的炎性細胞素 IL-6 與對照組相比,在放射治療第 1、 5、7 週有顯著下降。在動物實驗方面,投與板藍根能顯著降低放射 線對於免疫器官的損傷,增加免疫器官的重量,並且使老鼠體內的血 球數量如白血球、淋巴球等顯著上升,並且呈現劑量關係。發炎細胞 素 IL-1β、IL-6 與腫瘤壞死因子 TNF-α則顯著下降,並且呈現劑量關 係。 結論: 臨床試驗及動物實驗結果顯示,板藍根可有效降低因放射線所引 起的細胞損傷,降低放射性黏膜炎傷害,對於細胞激素的調節有明顯 的作用,本研究發現板藍根可成為放射治療之緩解患者因放射性黏膜 炎之不適,其機轉應該是經由發炎細胞激素的調節。 關鍵字: 板藍根、放射性黏膜炎、臨床試驗、動物模式、發炎細胞 激素。. ii.
(4) Abstract Radiotherapy plays major role in the treatment of malignancy. However, acute side effects such as radiation mucositis often cause oral pain and dysphagia of the patients, resulting in poor nutrition status. These disabilities usually influence the effect of radiotherapy. In this study, we evaluated the effect of Ban-Lan-Gen (BLG, radix of Isatis indigotica FORT) on acute mucositis and dermatitis induced by radiation. Methods: In clinical trial there were total 20 head and neck cancer patients were randomized into two groups: 1. Control group with only normal saline, 2. BLG group: We prophylactic application of BLG consisted of gargling and then swallowing the BLG preparation on the irradiated oral mucosa as radiotherapy was being carried out. This was compared with control patients who received routine conventional analgesics and skin care. Therapeutic application was started on the first day of radiotherapy. We evaluated of acute radiation mucositis and dermatitis according to the gold standard scale proposed by RTOG.. In. animal study, total 57 BALB/c mice were divided into six groups: three BLG groups with low (BLG-L, 0.195 g/kg/day), moderate (BLG-M, 0.585 g/kg/day) and high dose (BLG-H, 1.170 g/kg/day), glutamine group (1.950 g/kg/day), control group (RO water 10 ml/kg/day) and naïve group. All mice except naïve group were irradiated with 5.4 Gy in three days and then treated according to each group’s regimen for one week. Results: The clinical trial showed BLG can reduce the severity of radiation mucositis (P=0.01), anorexia (P=0.002) and swallowing iii.
(5) (P=0.002).. Although the result of resting days needed between groups. without significant (P=0.06), but quiet difference still was noted (mean days 1.64±2.46 versus 5.89±6.7). Serum IL-6 was significant lower in BLG group in 1st, 5th and 7th weeks. In animal study, increased thymus and spleen weight were found in BLG groups and in dose-dependent relationship. Blood contents such as leukocyte, lymphocyte, granulocyte and monocyte showed the same result. Serum TNF-α, IL-1β and IL-6 were also significantly lower in BLG groups and in dose-dependent relationship. Histopathology assessments of intestine were done and villi number was increased in BLG-H group and glutamine group only. Conclusion: BLG can improve radiation mucositis clinically. Animal study also showed its effects on immune organs preservations, increased cell subpopulation and down-regulated inflammatory cytokines expression. in. irradiated. mice.. We. suggested. that. BLG. has. anti-inflammatory ability to reduce the mucosal damage caused by radiation.. Keywords: Ban-Lan-Gen, radiation mucositis, clinical trials, animal study, inflammatory cytokines.. iv.
(6) Abbreviation BLG. Ban-Lan-Gen (radix of Isatis indigotica FORT). CDK. cyclin-dependent kinase. COX-2. cyclooxygenase-2. GM-CSF. Granulocyte-macrophage colony-stimulating factor. IL-1β. Interleukin-1beta. IL-6. Interleukin-6. MAPK. Mitogen-activated protein kinase. NF-κB. Nuclear factor-kappa B. PGE2. Prostaglandin E2. RT. Radiotherapy. RTOG. Radiation Therapy Oncology Group. ROS. Reactive oxygen species. SARS. Severe Acute Respiratory Syndrome. SWOG. Southwest Oncology Group. TNF-α. Tumor necrosis factor-alpha. v.
(7) Contents Chinese abstract --------------------------------------------------------------- i English abstract -------------------------------------------------------------iii Abbreviation -------------------------------------------------------------------v Chapter 1:. Introduction -------------------------------------------------1. Chapter 2:. Literature Review ------------------------------------------3. 2-1 Radiotherapy ----------------------------------------------------------3 2-2 Radiation mucositis --------------------------------------------------5 2-3 Current treatment of radiation mucositis ------------------------ 10 2-4 Previous clinical trials for radiation mucositis ----------------- 11 2-5 Cytokines and blood contents related to radiation damage --- 14 2-5 Ban-Lan-Gen (radix of Isatis indigotica FORT) ---------------- 17 2-6 Clinical trial of Ban-Lan-Gen for radiation mucositis--------- 19 Chapter 3:. Material and method ----------------------------------- 20. 3-1 Clinical trial of BLG in irradiated oral mucositis -------------- 20 3-2 Animal study of BLG in irradiated mice ------------------------ 30 Chapter 4:. Results ---------------------------------------------------- 36. 4-1 Clinical results of BLG -------------------------------------------- 36 4-2 Influence of BLG to immune organs in irradiated mice ----- 37. vi.
(8) 4-3 Influence of BLG to blood counts in irradiated mice---------- 37 4-4 Influence of BLG to cytokines in irradiated mice-------------- 37 4-5 Histopathologic assessment in animal model------------------- 38 Chapter 5:. Discussion-------------------------------------------------- 39. Chapter 6:. Conclusion ------------------------------------------------- 42. References -------------------------------------------------------------------- 43 Tables -------------------------------------------------------------------------- 54 Figures------------------------------------------------------------------------- 65 Appendix ---------------------------------------------------------------------- 87 感謝詞 ------------------------------------------------------------------------- 91. vii.
(9) Chapter 1: Introduction Ionizing radiation is one of the most important modalities for the treatment of human malignancies. However, the acute and late effects of radiation on normal tissues often limit the total dose that can be delivered safely.. Radiation mucositis is that condition wherein mucosa suffers toxic. damage from direct or indirect action of radiation insult at the layer of mucosal epithelium, on the luminal surface of the mucosa and on the cells between lumen and basement membrane [1]. Radiation mucositis is the most common seen acute side effect in head and neck cancer patients receiving radiotherapy. Thus, radiation mucositis usually acts as a major dose-limiting side effect that influences optimal delivery of radiation [2]. To days, there is no satisfied strategy for preventing mucosal injury or lowering its severity. The current major drug for the treatment of radiation mucositis are steroid and non-steroid anti-inflammation drugs (NSAIDs). Unfortunately, due to the limited effectiveness of drugs, patients often need to rest radiotherapy to relief. or. reduce. radiation. mucositis. symptoms.. Additionally,. radiation-induced mucosal damage influence other objective or subjective illness to qualify as mucositis such as pain, dysphagia and anorexia. In order to improve the therapeutic effects of radiotherapy, clinical physicians often increase total radiation dose and size of daily fractions. However,. acute. and. late. effects. of. ionizing. radiation. on. the. vascular-connective tissue of bone and cartilage in the head and neck region still limited the total radiation dose.. If it were possible to protect the oral. and pharyngeal mucous membranes from the acute effects of irradiation such as radiation mucositis, patient morbidity would be substantially improved. Nonetheless, radioprotection of mucous membranes would reduce morbidity and make possible the incensement of irradiation dose. 1. Besides, most.
(10) clinical trials showed great higher cure rate and local control rate in concomitants radiotherapy with chemotherapy. But these chemotherapeutics also cause acute desquamation of mucosal epithelium and exacerbate radiation mucositis [3]. Thus lowering of grade of mucositis caused from the acute effects of ionizing radiation and/or chemotherapeutic agents would reduce the dose-limiting toxicity of these two modalities and represent a therapeutic gain in the combined modality treatment of head and neck cancer. Isatis indigotica FORT is a kind of the blue cruciferous plants.. Its. root is a commonly used Chinese herb to remove toxic heat, to reduce heat in blood, and to relieve convulsions.. According to modern medical research,. the major components of radix of Isatis indigotica FORT (BLG) including indirubin, indigotone and indigo pigment contents, with anti-virus, fever detoxification and anti-inflammatory efficacy. are small.. Its toxicity and side-effects. The purpose of this study was to prove the efficiency of BLG to. reduce radiation mucositis in clinical trial, to discus the possible mechanism and to explore the possibility of widely clinical applications. 2.
(11) Chapter 2: Literature Review 2-1 Radiotherapy 2-1-1 Introduction Radiotherapy is a kind of treatment for cancer using radiation. Radiotherapy has experienced more than a century of history. Mr. Rontgen first discovered X-ray and his wife discovered radium respectively in 1895, then human soon used radiation in clinical treatment for skin cancer one year after. With advance in medical research and technique, non-invasive treatment became to be dominant in modern cancer treatment. Till now, approximately 70% of cancer patients in need of cancer treatment with radiotherapy and about 40% of the pain can undergo in curative purpose. The role and status of radiotherapy in the treatment of cancers had become increasingly prominent. Radiotherapy was used in the treatment of malignancies which are radiosensitive such as lymphomas or Kaposi's sarcoma among others. Some tumors, such as the epithelial cancers of the upper aero-digestive tract, including the oral cavity, are moderately radiosensitive. Ionizing radiation to the head and neck regions is administered by means of external beams of X-ray, gamma rays or external beams of electrons directed to the tumor or by local implantation (brachytherapy) of radioactive needles of cesium, radium, gold, palladium or other metals which also emit x-rays or gamma rays. Most of the irradiative treatments for head and neck cancers consist of a total dose of 50 to 80 Grays (Gy) distributed in fractioned doses of 10 Gy per week during five weeks, at a rate of 2.0 Gy every 24 hours during a 5 day period (1.0 Gy = 100 rads).. 3.
(12) 2-1-2 Mechanism of radiation-induced cell damage (1) Direct injury: Major role in the direct rays resulting from organic elements pertaining to the DNA elements appear fractured and overlapping. (2) Indirect damage: Organization of ionizing water with energy-derived photons produced larger oxidative free radicals by using radiation on the human body. These large molecules interact with the DNA elements, usually correlate with irreversible damage.. 4.
(13) 2-2 Radiation mucositis 2-2-1 Structure of oral mucosa The structure of oral mucosa is composed of stratified squamous epithelium that overlies the lamina propria and connective tissue, which consists of fibroblasts small blood vessels, inflammatory cells and extra-cellular matrix (ECM). The oral mucosa is a kind of constantly renewing tissue.. Proliferating cells in the basal epithelial layer mitosis and. produce daughter cells that then migrate to the mucosal surface [Figure 1].. 2-2-2 Introduction of radiation mucositis Radiation-induced damages are non-selective, and therefore may even trigger skin injury or mucositis, and even other fatal complications regardless of normal cells or malignant cells. Those side effects often limit the radiation dose to use in cancer treatment and therefore influence the therapeutic effects.. Some side effects can be mitigated by medication. methods. One major complication of radiation therapy is the damage that occurs in the mucosal lining of the gastrointestinal tract, especially to the oral and oropharyngeal mucosa.. This damage is called radiation mucositis.. Severe oral mucositis is especially common among patients who receive radiation therapy as treatment for cancers of the oral cavity, oropharynx, nasopharynx and salivary glands [2]. Radiation mucositis is a painful inflammatory reaction of the oral mucosa to radiation therapy. The effect of radiation on the oral mucosa is one of cessation of the rapid proliferation of normal epithelial cells with 5.
(14) consequent cellular atrophy followed by necrosis, epithelial sloughing and ulceration.. The exposed underlying connective tissue becomes an open. door to infection which will be more marked in those patients which have undergone full body radiation and are in immune suppression patients. The degree of radiation mucositis varies, depending on the dose and portal of the beam.. Besides, age and general health of the patients affect. the severity of radiation mucositis. The first reaction is usually noted during the second week of a 5 or 6 week treatment and consists of diffuse erythematic change, followed by desquamation and ulceration.. Xerostomia. adds to the discomfort and usually persists indefinitely to some degree. An alteration in taste often precedes the mucosal reaction and may persist, depending on the dose.. 2-2-3 Mechanism of radiation mucositis The mechanism of radiation mucositis was been postulated as occurring in four phases: initiation, cellular message generation and signal amplification, ulceration and healing.. 2-2-3-1 Initiation phase High energy photons can cause direct or indirect damage to cells. Mostly, indirect damages play major role in cell killing. Energy-derived photons interacted with water and generate reactive oxygen species (ROS), free radicals that can cause DNA strand breaks in the epithelium and submucosa. Cellular responses occur very soon, usually few milliseconds immediately after direct or indirect damages to DNA or other cellular 6.
(15) components by radiation insult. These responses initiate a cascade of other downstream biological events.. 2-2-3-2 Cellular message generation and signal amplification Cellular responses to radiation-induced DNA damage activate several transcription factors that affect a number of genes modulating protein synthesis and cell signaling. Among those numerous transcription factors which activated by radiation insult, one of the most important is nuclear factor-kappa B (NF-κB).. This nuclear regulatory molecule coordinate. nearly 200 genes involved with radiation mucositis.. Some of those genes. encode and regulate pro-inflammatory cytokines such as interleukin-6 (IL-6) and cell adhesion molecules [4, 5]. Elevated activity of synthesis of the cytokines interleukin-1β (IL-1β) and IL-6 were seen in the irradiated mucosa. Other enzymes activated by radiation, and sequential ROS include ceramide synthase and sphingomyelinases that can increase the rate of apoptosis. These transcription factors, cytokine and other substances together contribute to trigger a variety of destructive processes that can be lethal damage to epithelial cells and surrounding fibroblasts. After initial cellular message generation, the next step involves feedback loops that further amplify the number and level of activating signals [Figure 2]. Following radiation damage, some pro-inflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α), not only directly result in tissue injury but also further increase the activity of other signaling factors such as NF-κB and mitogen-activated protein kinase (MAPK) [4]. Then there is an ongoing cycle of amplification of cellular messages for radiation injury that persists well after the initial insult of radiation, 7.
(16) recruiting inflammation reaction cells. However, few symptoms are apparent in spite of all these cellular changes occurring during the initial stages of mucositis interestingly.. 2-2-3-3 Mucosal ulceration The advanced stage next to cycles of amplification of cellular message, mucosal ulceration occurs. The ulcer penetrates through the epithelium into the submucosa. The ulcerated mucosal surface often was infected by oral bacteria. The infection can produce toxins and recruit acute inflammatory cells such as macrophage, which release additional inflammatory cytokines and angiogenesis factors. This ulcerative phase takes great part of the main clinical symptoms of mucositis, such as oral pain, erymanthos inflammation, and dysfunction of swallowing.. 2-2-3-4 Healing In response to worse ulcer formation, mucosa starts healing process. Epithelial cells grow, migrate, and differentiate to form a wound under the stimulation of signals secreted by the extra-cellular matrix. These signals are then down-regulated to avoid hyperplasia.. With the healing process. under way, symptoms begin to abate.. 2-2-4 Clinical course and severity grades of radiation of mucositis During a course of fractionated external radiotherapy for head and neck cancer, the rapidly dividing mucosal epithelium is progressively 8.
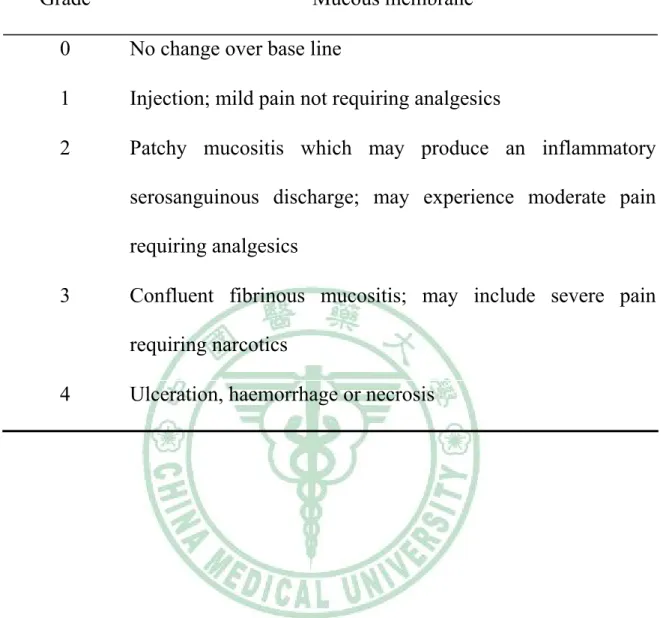
(17) depleted with each succeeding radiation fraction. An acute radiation-induced mucositis usually begins during the third week of fractionated external irradiation, gradually increases in intensity until the end of irradiation, and then subsides over several weeks after. Erythema characterizes the early mucosal reaction, erythema and patchy ulceration the intermediate, and erythema and confluent ulceration. The Radiation Therapy Oncology Group (RTOG) classified five grades to be a gold standard clinical guideline for physicians to objectively inspect and evaluate radiation-induced mucositis [Table 1].. 9.
(18) 2-3 Current treatment of radiation mucositis Till now, there are no proven effective agents for prophylaxis of radiation mucositis, and thus no “gold standard” method exists. Many traditional forms of treatment, such as mouthwashes and chlorhexidine, have been largely ineffective. Medical intervention such as analgesics, steroids and antibiotics showed therapeutic benefits for symptoms improvement. But these methods have not demonstrated consistent efficacy in preventing and treating oral mucositis. Antimicrobial agents benefit but a few patients who develop a confluent exudative ulceration of the mucous membranes during irradiation. A far more common problem is the early appearance of a burning sensation and beefy red mucosa with or without the gray white plaques characteristic of candidiasis. Yeast can be documented by KOH smears or culture in roughly one quarter of patients undergoing irradiation for head and neck cancer and successfully treated with topical antifungal agents. Antimicrobial and antifungal agents successfully treat superimposed bacteria or fungal infection but do little to protect mucous membranes from the acute effects of irradiation. Although limited success was observed in pain moderation and improvements in inflammation with some of these procedures, to date, no agent has been granted a priori approval as a prevention or therapy for cytotoxic mucositis. Thus newer approaches or agents are needed to improve both prophylaxis and therapy in patients receiving radiation therapy.. 10.
(19) 2-4 Previous trials for radiation mucositis Strategies to reduce the incidence and severity of acute radio mucositis include the use of antimicrobial and antifungal agents as well as thiol and prostaglandin radio-protectors. In the past, the use of chlorhexidine [6] sucralfate [7] and benzydamine hydrochloride [8] oral rinses for prevention of radiation induced oral and pharyngeal mucositis have been tried but only benzydamine hydrochloride has been shown to reduce the severity of mucositis when compared with placebo. To date, some ended clinical trials and agents are listed below.. 2-4-1 benzydamine hydrochloride Epstein reported a reduction in mucositis severity from a score of 3.2 ±0.51 for eighteen placebo patients to 2.20±0.56 for the 25 benzydamine hydrochloride patients (P=0.01) [8].. Benzydamine not only attenuates. pro-inflammatory cytokines but also scavenges reactive oxygen species (ROS) [9].. 2-4-2 aminothiols (WR-2721) There are sulfhydryl compounds that protect from the effects of ionizing radiation mainly by scavenging free radicals. Charged with protecting military and civilian populations from radiation or chemical warfare the Defense Department undertook an extensive program to develop thiol radio-protectors based on the early work of Bacq and Herve [10]. The most. effective. radio-protector. proved. to. be. S-2-(3-amino-propyl. amino)-ethyl phosphorothioic acid (WR-2721). WR-2721 has proven 11.
(20) radio-protective for a variety of normal tissues but its clinical usefulness has been limited by nausea, vomiting and hypotension [11].. 2-4-3 Granulocyte-macrophage colony-stimulating factor (GM-CSF) GM-CSF has been postulated as one of the most promising agents for the prevention of radiation-induced mucositis on the basis of same preliminary reports [12-14].. GM-CSF is a glycoprotein with a molecular. weight of 22 kD. It is a potent growth factor for the myeloid lineage of hematopoietic cells. GM-CSF enhances colony formation of granulocytes, macrophages, and eosinophils and also regulates several functions of mature leukocytes, macrophages, and dendritic cells in the dermis and submucosa [15-17], was shown to have the ability of reduces the severity of radiation-induced mucositis.. 2-4-4 glutamine Glutamine, a nonessential amino acid, is the key fuel for rapidly dividing cells, such as enterocytes, renal tubular cells, lymphocytes, and malignant cells [18-19].. During critical illness, the balance of glutamine. metabolism switches to favor enhanced use, leading to a state of total body glutamine depletion and a catabolic state [20-21]. Concentrations of glutamine are found to be decreased during stress, starvation, metabolic acidosis, postoperative stress, and advanced malignant states [22]. It has been shown previously to reduce the extent of intestinal injury from radiation and chemotherapy in laboratory rats [23]. Mechanism by which 12.
(21) glutamine may help decrease mucous membrane injury induced by radiation is by altering the inflammatory response. Glutamine has been shown to be a regulator of glutathione, a ubiquitous antioxidant [24]. Glutathione is an antagonist to prostaglandin E2 (PGE2) production, which is a strong inflammatory mediator. A trial conducted by Huang and colleagues [25] in 2000 examined whether oral glutamine could also inhibit radiation-induced mucositis. A total of 17 patients were randomized to receive oral glutamine suspension (2.0 g/30 ml) versus placebo.. Objective responses were noted, with. decreased duration of grade 3 and 4 mucositis as well as decreased severity in degree of mucositis (mean, 1 grade). These early results certainly warrant further investigation. But recently, a large randomized, double-blind, placebo-controlled study (SWOG-9908) in American conducted by Southwest Oncology Group (SWOG) showed that glutamine had no significant benefit to improve radiation mucositis.. 13.
(22) 2-5 Cytokines and blood contents effect related to radiation damage Some cytokines such as TNF-α, IL-1β and IL-6 was found to be often elevated during radiotherapy. To date, a number of circulating cytokine levels have been measured in patient serum and appear to have clinical relevance: TNF-α [26-28], IL-1 [29-30], IL-6 [31-32] and IL-8 [33-35]. These cytokines are inflammatory or pro-inflammatory mediators, related to radiation-induced tissue damage, such as radiation mucositis [36]. Tumor necrosis factor-α could well provide a marker for both tissue damage and the induction of inflammatory processes. Circulating levels of these cytokines will be used as a measure of primary damage and activation. Moreover, several studies showed these cytokines also take part of fatigue and thus influence the life quality of cancer patients.. Bower and. colleagues [37-40] compared breast cancer survivors with persistent fatigue to a control group of non-fatigued survivors. Fatigued survivors showed significant elevations in several markers of pro-inflammatory cytokine activity compared to non-fatigued controls. Fatigued survivors also reported behavioral changes consistent with pro-inflammatory cytokine activity, including depressed mood, sleep disturbance, decreased activity, and cognitive disturbance [37-40].. 2-5-1 Tumor necrosis alpha (TNF-α) TNF-α in particular has been shown to be of primary importance in pulmonary fibrosis following injury and has been demonstrated to coordinate and network secondary, down-stream cytokines and chemokines, recruiting and amplifying inflammatory cells and components [41, 42]. This 14.
(23) network ultimately leads to the expression of radiation-induced late effects.. 2-5-2 Interleukin-1alpha and beta (IL-1α, IL-1β) IL-1 procedure by monocytes and macrophages, activate CD4 helper T-cell. It can promote T-cell proliferation. IL-1 alpha (IL-1α) is a kind of cytokine expressed on cell plasma membrane. IL-1α that may secreted by astrocytes, fibroblasts, hepatocytes, keratinocytes, type II Greater alveolar cells, brown fat adipocytes, thymic myoid cells, T cells, eosinophils, monocytes, and dendritic cells, especially by macrophages, endothelial cells, dendritic cells and fibroblast.. The cells which can express IL-1β are. astrocytes, adrenal cortical cells, NK cells, macrophages, monocytes, endothelial. cells,. keratinocytes,. megakaryocytes,. platelets,. neurons,. neutrophils, oligodendroglia, osteoblasts, Schwann cells, trophoblasts, T cells and fibroblasts.. 2-5-3 Interleukin-6 (IL-6) IL-6 is a pro-inflammatory cytokine secreted by T cells and macrophages to stimulate immune response to trauma, especially burns or other tissue damage leading to inflammation. Pons et al. reported that IL-6 gene expression was increased by irradiation [43].. 2-5-4 Hemoglobin (Hgb) The Radiation Therapy Oncology Group (RTOG) analyzed 521 patients treated as part of RTOG 85-27, showed that patients with anemia 15.
(24) (defined as hemoglobin <14.5 mg/dl for men and < 13.0 mg/dl for women) had significantly worse overall survival (P=0.0003).. A trend was noticed. with respect to local-regional control, with anemic patients having a worse outcome (P=0.065).. Of note, there was also a trend toward fewer late. complications in anemic patients (P=0.054); it is unclear whether this could reflect hypoxia in normal tissues as well as tumor or whether this finding was an artificial result of anemic patients having shorter survival and thus less time to develop late complications [44].. 2-5-5 Neutrophils Activated neutrophils can lead to microvascular injury resulting in increased permeability, hemorrhage, and thrombosis [36].. Activation of. neutrophils was by cytokines such as IL-1 and TNF-α [45].. Mucosal. damage observed with infection is thought to be caused by cytokine activated neutrophils [46].. 16.
(25) 2-6. Radix of Isatis indigotica FORT. 2-6-1 Introduction Radix of Isatis indigotica, also known as Ban-Lan-Gen (BLG), derived from the root of the isatis plant, which is a source of indigo dye. Its roots were widely used as a kind of traditional Chinese medicine herb. Indigo plant is used in China for infections associated with heat.. The. purified extracts of BLG have been utilized to make various preparations which can be used in clinical practice for treatment of influenza, epidemic hepatitis, epidemic encephalitis B, carbuncle, erysipelas [47, 48]. purported uses are bronchitis, chest congestion and fever.. It’s main. It is used in. combination with other herbs to treat the common cold, sore throat, mumps, respiratory aliments, other febrile diseases and malignant tumors [48-51]. In several studies, it appears that indigo plant root has immune stimulating and anti-inflammatory activity. Recent anecdotal reports indicate that BLG can be used in Severe Acute Respiratory Syndrome (SARS) [52], because BLG has antiviral activities. [53]. 2-6-2 Constituents and possible mechanism of actions Many chemical compounds have been isolated from BLG, including indigotin, indirubin, isatin, isatan A, isatan B, trytanthrin, purin, isaindigotidione, polysaccharides, organic acids and many amino acids [54].. 17.
(26) These isolated components can be roughly divided to water-soluble and insoluble groups. Mainly polysaccharides organic acids. Water-soluble compounds:. and amino acids take great part of the water-soluble compounds. Polysaccharide from indigowoad was shown to have immune-stimulatory effects by enhancing reticuloendothelial system function, especially lymphocyte, monocyte and NK cells.. The organic acids in BLG had in. vitro anti-endotoxic action and antiviral action [55]. Indirubin, an active component of. Water-insoluble compounds:. BLG, is a potent inhibitor of cyclin-dependent kinases (CDK) [56]. chemical structure of indirubin was analyzed and shown below.. The. Indirubin. was proved to have cyclooxygenase-2 (COX-2) inhibitory-like effects [57]. Indirubin also had been proved an anti-cancer activity in the treatment of chronic granulocytic leukemia [56].. Recently, it was found that indigotin. and indirubin were potent aryl hydrocarbon receptor (AhR) agonists [58, 59] and the alkaloid isaindigotone from BLG was reported to be a scavenger of superoxide generated [60].. 18.
(27) 2-7. Clinical trial of BLG in radiation mucositis Radiotherapy plays major role in cancer treatment. However, radiation mucositis is the most often acute side effect in head and neck cancer patients receiving radiotherapy.. The current major drug for the. treatment of radiation mucositis is steroid and non-steroid anti-inflammation drug (NSAIDs).. Unfortunately, due to the limited effectiveness of drugs,. patients often need to rest radiotherapy to relief reduce radiation mucositis symptoms. BLG is a commonly used Chinese medicine to remove toxic heat, to reduce heat in blood, and to relieve convulsions. According to modern medical research, the major components of BLG including indirubin, indigotone and indigo pigment contents, with anti-virus, fever detoxification and anti-inflammatory efficacy.. Its toxicity and side-effects are small.. Indirubin is the most important component. It is water-insoluable. The ethanol-extract part of BLG was proved to have major anti-inflammatory activity [61] However, there was no clinical trial to use BLG in radiation mucositis till now. The purpose of this study was to prove the efficiency of BLG to reduce radiation mucositis in clinical trial, to discus the possible mechanism and to explore the possibility of widely clinical applications.. 19.
(28) Chapter 3: Materials and methods. Divided into two parts: (1) Application of BLG in radiation-induced mucositis clinical trials. (2) Assessment of BLG for the immune system after exposure to radiation effects.. 3-1 Clinical trial: application of BLQ in Radiation-induced Mucositis 3-1-1 Inclusion criteria: (1) Patients must have be victims of head and neck cancer (T1-T4, Any N, M0) (2) Patients must be scheduled to receive (according to institutional standards) high dose radiation therapy (XRT) of at least 6,000 cGy with a daily dose of 180-200 cGy. Intensity Modulated Radiation Therapy (IMRT) may be substituted for standard XRT. XRT must be planned to begin 7 to 28 days after registration. (3) Patients must have a Kornofsky performance score ≧ 70。 (4) No other malignancy is allowed except for the following: adequately treated basal cell or squamous cell skin cancer, in situ cervical cancer, adequately treated Stage I or II cancer from which the patient is currently in complete remission, or any other cancer from which the patient has been disease-free for five years.. 20.
(29) (5) All patients must be informed of the investigational nature of this study and must sign and give written informed consent in accordance with institutional and federal guidelines.. 3-1-2 Objectives (1) Primary Compare the efficacy of BLG versus placebo, in terms of maximum mucositis toxic effects and worst reported mouth pain during and after high-dose radiotherapy, in patients with head and neck cancer. (2) Secondary a. Compare the duration of severe mucositis in patients treated with BLG. b. Compare the radiotherapy delay in patients treated with BLG. c. Compare weight loss in patients treated with BLG. d. Compare the toxic effects of BLG in these patients. e. Compare patient-reported mouth pain success rate in patients treated with BLG. f. Determine the compliance of patients treated with BLG.. 3-1-3 Pretreatment evaluation. 21.
(30) (1) Complete history and physical examination (2) Document extent of tumor tissue biopsy (previous treatment) (3) CBC with differential, platelet count, blood chemistries (SMA-12), liver profile. (4) Chest X-ray. (5) Pregnancy test for women of child-bearing potential.. 3-1-4 Registration procedure (1) Patients can be registered only after pretreatment evaluation is completed and eligibility criteria are met. (2) The patient will be registered to the clinical trial and a case number will be assigned and confirmed. (3) The Eligibility Checklist must be completed in its entirety prior to calling chairman. (4) The completed, signed, and dated Checklist used at study entry must be retained in the patient’s study file.. 3-1-5 Radiation therapy (1) Physical Factors a. Equipment: Linear accelerators with appropriate photon and electron energies for supplemental boosting to the nodes. 22.
(31) b. Selection of appropriate photon energy should be based on optimizing the RT dose distribution within the target volume and minimizing the dose to the normal tissue. c. Treatment distance must be S.A.D for isocentric techniques. (2) Localization Requirements a. Simulation: Simulation of all fields is mandatory. must be reproducibly immobilized.. Patients. The use of customized. blocks to shape the treatment fields is recommended. Simulation films of each field, initial port films, and the calculation form will be sent to RTOG Headquarters in the first week of therapy, together with the treatment prescription for radiation therapy quality assurance review. b. Verification: Beam verification (port) films must be obtained for each field.. This should be done at least once in the first. week of treatment and whenever any field adjustments are made.. Port films of each field must be submitted to RTOG. Headquarters. (3) Target Volume Irradiation Portals a. Standard three-field techniques using two parallel opposed lateral fields will be used for the primary tumor site at the discretion of the investigator for the case.. A single anterior. A-P field will be used to treat the neck below the fields for the primary tumor.. When there is (are) positive node(s) in the. lower neck, an additional posterior field may be necessary to deliver a supplemental dose to the positive node (s). All fields 23.
(32) must be treated on each treatment day.. The lower neck and. supraclavicular field should abut the primary field at the skin. For patients with short necks, right and left superior inferior oblique fields or any other standard techniques may be used. For oropharynx primaries, a midline block 2 cm wide and at least 2 cm in length on the skin surface will be placed in the anterior lower neck field to shield the larynx and the spinal cord in the junction region. For larynx and hypopharynx primaries, a lower lateral block, 2 cm in height, should be placed in the lateral upper neck fields to shield the areas from potential overlap of diverging beams over the spinal cord. Use of right and left superior – inferior oblique fields technique is also acceptable. used.. Appropriate bolus around the stoma is to be. The primary treatment fields should encompass the. primary tumors with adequate margins along with sites of known and/or suspected lymph node disease in the upper neck. There should be a minimum 2-3 cm margin around the primary tumor and positive node(s) and should include upper neck nodes to be irradiated electively for the initial target volume. Appropriate field reductions are to be made at the discretion of the treating radiation oncologist. The maximum spinal cord dose should not be more than 45 Gy-46 Gy. (4) Oropharynx: a. The upper border of the field includes the nodes in the upper jugular region and should be placed at the level of the zygomatic arch, to include the parotids in the field. b. The ipsilateral posterior cervical nodes must be irradiated if the 24.
(33) primary tumor is T3 or T4. c. Both the ipsilateral and contralateral posterior cervical nodes must be irradiated if there are clinically positive cervical nodes in the anterior chain. (5) Supraglottic larynx: a. The upper border of the field includes the nodes in the upper jugular region and should be placed at the level of the zygomatic arch to include the parotids in the field. b. The lower border of the field encompasses the larynx usually at or below the level of C5. c. The ipsilateral posterior nodes should be treated for T3 and T4 lesions. d. Both ipsilateral and contralateral posterior nodes should be treated if there are clinically positive nodes in the anterior chain. (6) Hypopharynx: a. The superior border is placed at the level of the zygomatic arch, to include the base of skull (above C1) and the retropharyngeal nodes. Nodes in the upper jugular region and posterior triangle are included. b. The lower border of the field encompasses the lower border of the cricoid cartilage. (7) Lower neck: 25.
(34) a. A single anterior lower neck field will be used to treat the neck and the supraclavicular fossa below the fields for the primary tumor. When there is (are) positive node (s) in the lower neck, an additional posterior field may be necessary to deliver a supplemental dose to the positive node (s). b. The lower border of the field will be just below the clavicle or 1 cm below the clavicle when there are positive nodes in the supraclavicular fossa. (8) Dose Calculation a. Dose to the supraclavicular field is calculated at 3 cm depth or d Max depending on the clinical situation and at the discretion of the treating Radiation Oncologist. Cumulative isodose distributions at the level of the tumor center, a copy of the treatment record indicating cumulative doses, and boost field simulation and portal films must be submitted at the completion of radiotherapy. b. Missing tissue equivalent compensators should be used to ensure homogeneity of dose distribution so that variation within the target volume does not exceed 10% of the target dose. c. Boost doses will be specified at the actual site(s) of gross primary and nodal disease. (9) Standard Fractionation a. Treatment to the primary tumor and upper neck will be given at 1.8 Gy per fraction, once a day, five days a week to a total 26.
(35) dose of 54-70 Gy in 27-35 fractions in five and a half to seven weeks. Fields must be reduced to exclude the spinal cord at 38-44 Gy at the mid-plane.. However, the entire neck must be. irradiated to a dose of 54 Gy (even NO stage) as the anatomical levels of lymph node spread, usually 2-4 cm below the skin surface. Clinically positive neck nodes should receive a dose of 62-70 Gy in 31-35 fractions in 6-7 weeks. To supplement the dose to the posterior neck and clinically positive nodes, boost techniques may include additional electron beam (9 MeV) to the posterior neck. The anterior lower neck field will be treated at 2 Gy per fraction at 3 cm depth, once a day, to a total dose of 54 Gy in 22 fractions in 5.5 weeks.. The total dose to the. primary tumor and clinically positive nodes will be 62-70 Gy in 31-35 fractions in 6-7 weeks. b. Radiation treatment is to be started within 4-6 weeks of surgery. c. Wedge-pair techniques to boost the primary tumor can only be used if it does not interfere with the shielding of the transferred submandibular salivary gland in the submental space. 3-1-6 Radiation Therapy Toxicity Adjustments (1) Treatment Interruptions: Interruptions in radiation therapy may be necessitated by skin reactions, mucositis, ulceration, edema, or other acute complications. Radiation therapy will be continued without interruption if at all possible. Any interruption of radiation. therapy. for. whatever. 27. reason. (pain,. machine.
(36) malfunction, illness, lack of transportation or social obligation) must be clearly indicated in the treatment record. (2) CBC is required to be done before radiation therapy or during the first week of radiation therapy. Radiation mucositis judgments are according to RTOG classification of mucositis as Table 1.. 3-1-7 Toxicity Reporting Guidelines (1) For acute radiation effect, through day 90 of treatment, the NCI CTC Version 2.0 will be used. (2) Late radiation effects will be evaluated and scored per the RTOG/EORTC Late Effects Scale. (3) All fatal toxicities (grade 5) resulting from protocol treatment must be reported by telephone to the Group Chairman, to ACR Headquarters Data Management and to the Study Chairman within 24 hours of discovery. (4) Required data forms, and, if requested, a written report, must be submitted to Headquarters within 10 working days of the telephone report.. 3-1-8 Preparation the BLG According to the textbook records of BLG, we prepared scientific Chinese medicine BLG powder manufactured by Sun-Ten Pharmaceutical 28.
(37) Co. Ltd.. This BLG powder was composed of radix isatidis concentrated. extracts and radix isatidis powder with absorption ratio to 2:1.. 3-1-9 Clinical usage of BLG We dissolve the concentrated powder of BLG in RO reverse water with daily dose 1.5 g in 90 ml solution. We educated our patients how to use it: mouthwash, gargle over throat and then swallow it, 30 ml per time and three times a day. (0.5 g BLG per time, 1.5 g per day) During whole course of radiotherapy, we will give medication according to WHO three steps guideline (step 1: NSAIDs, step 2: partial narcotics, step 3: narcotics). BLG was supplied as adjuvant medication to lower radiation mucositis.. 3-1-10 Statistical analysis Parameters were documented at the beginning of radiotherapy until completion of radiotherapy: (1) grade of mucositis each fraction (from patient’s subjective complaint and evaluation of physician.. We used F-test. to compare age, body weight, and treatment time between the two arms. Mean maximum grade of mucositis, mean maximum WHO step, mean body weight change, and mean fraction number of Grade 0-4 mucositis were compared by the Mann-Whitney U test. considered to indicate statistical significance.. 29. P-values less than 0.05 were.
(38) 3-2 Assessment of BLG for the immune system after exposure to radiation effects. 3-2-1 Animals Total 57 BALB/c mice strain aged 5-6 week and weighing between 20~25 g, , purchase from the National Laboratory Animal Breeding and Research Center, Taipei, Taiwan, will housing in plastic cage with Ventilated Micro Isolator System (VMIS) and provide with steriled Purina rodent chow and water ad libitum. A 12-hour light/dark cycle was set. Animals were acclimated for a minimum of 48 hours prior to radiation to minimize the effects of stress due to shipping.. All animals were weighed. prior to radiation and monitored daily for survival. All protocols were approved by the Standing Committee on Animal Use of the China Medical University.. 3-2-2 Regimen dosing In animal study, total 57 BALB/c mice were divided into six groups: three BLG groups with low (BLG-L, 0.195 g/kg/day), moderate (BLG-M, 0.585 g/kg/day) and high dose (BLG-H, 1.170 g/kg/day), glutamine group (1.950 g/kg/day), control group (RO water 10 ml/kg/day) and naïve group. Each group was assigned the different test regimens (feed immediately after irradiation for seven days before sacrificed) as following:. 30.
(39) Sample size. Radiation modeling. Treatment. No treatment. 10. ┼. ── (RO, 10 ml/kg/day). BLG-L. 10. ┼. BLG, 0.195 g/kg/day (1×). BLG-M. 10. ┼. BLG, 0.585 g/kg/day (3×). BLG-H. 10. ┼. BLG, 1.170 g/kg/day (5×). Glutamine. 9. ┼. Glutamine, 0.520 g/kg/day (1×). Control. 8. ─. ──. Group. 3-2-2 Irradiation Each groups except naïve group received whole body irradiation with 1.8 Gy/day for consecutive three days, total 5.4 Gy. We used Elekta Precision Linac to perform irradiation. High energy electron beam 9 MeV was applied with SSD technique (SSD, 110 cm).. 3-2-3 Immune organs and blood cells and differentiation measurement All 57 mice were sacrificed after consecutive feeding with testing regimens. The weight of immune organs, such as spleen, thymus and pancreas were measured. Red blood cells were removed by BD FACS Lysing Solution. Wash cells one time in cold wash buffer (DPBS/0.1% NaN3); and centrifuge at 350 ×g for 5 minutes. And then re-suspend cell pellet and adjust the cell concentration to 2×107 cells/ml.. Dilute primary fluorochrome-conjugated. 31.
(40) mAbs to predetermined optimal concentrations in wash buffer.. Deliver. 1×106 cells in 50 μl to each well already containing 50 μl of mAb.. Mix by. gently vortexing or tapping. dark.. Then Incubate at 4°C for 20-40 minutes in the. Wash two times with 3.0 ml of wash buffer.. After each. centrifugation, 350 ×g for 5 minutes, aspirate tube to remove supernatant. Vortex gently or tap plate to loosen pellet prior to adding next wash or diluted secondary reagent. Use 500 μl of analysis buffer (DPBS/0.1% NaN3/1.0% fetal bovine serum) to resuspend pellet in FACS tubes appropriate for flow cytometer. Acquire sample data on flow cytometer as soon as possible after staining. Live gate in 5000 cells for differentiate lymphocytes, monocytes and granulocytes in the dot plot of forward scatter (FSC) and side scatter (SSC).. 3-2-4 IL-1β and IL-6 by ELISA protocol The “Mouse cytokine ELISA Ready-SET-Go!” and “Human cytokine ELISA Ready-SET-Go!” “eBioscience” reagent set contains the necessary reagents, buffers and diluents for performing quantitative enzyme linked immunosorbent assays (ELISA). (1). Capture Antibodies and Detection Antibodies (biotin-conjugate) were pre-titrated, purified antibodies.. The clones list below in table:. 32.
(41) Cytokines. Capture antibody. Detection antibody. Sensitivity. Detection range. mTNF-α. 1F3F3D4. XT3/XT22. 8 pg/ml. 8-1000 pg/ml. mIL-1β. B122. Rabbit polyclone 8 pg/ml. 8-1000 pg/ml. mIL-6. MP5-20F3. MP5-32C11. 4 pg/ml. 4-500 pg/ml. hIL-1β. CRM56. CRM57. 8 pg/ml. 8-1000 pg/ml. hIL-6. MQ2-13A5. MQ2-39C3. 2 pg/ml. 2-200 pg/ml. (2).. Standard: Recombinant cytokine for generating standard curve and calibrating samples. (3).. Coating Buffer: 10× concentrated. (4).. Assay Diluent: 5× concentrated. (5).. Detection enzyme: pre-titrated Avidin-HRP. (6).. Substrate Solution: Tetramethylbenzidine (TMB) Substrate Solution. (7).. 96 Well Plate: Corning Costar 9018 or NUNC Maxisorp flat-bottom. (8).. Coat 96 well ELISA plate with 100 µl/well of capture antibody in Coating Buffer (dilute as noted on Certificate of Analysis, which is included with the reagent set).. Seal the plate and incubate overnight. at 4°C. (9).. Aspirate wells and wash 3 times with >300 µl/well Wash Buffer. Invert the plate and blot on absorbent paper to remove any residual buffer.. (10). Dilute 1 part 5× concentrated Assay Diluent with 4 parts DI water. 33.
(42) Do NOT add sodium azide.. Sodium azide inhibits HRP activity.. Block wells with 200 µl/well of 1× Assay Diluent.. Incubate at room. temperature (RT) for 1 hour. (11). Aspirate/wash as in step 9. (12). Add 100 µl/well of standard (dilute as noted on Certificate of Analysis) to the appropriate wells.. Perform 2-fold serial dilutions of the top. standards to make the standard curve. Add 100 μl/well of your samples to the appropriate wells.. Seal the plate and incubate at RT. for 2 hours. (13). Aspirate/wash as in step 9.. Repeat for a total of 5 washes.. (14). Add 100 µl/well of detection antibody diluted in 1× Assay Diluent (dilute as noted on Certificate of Analysis). Seal the plate and incubate at RT for 1 hour. (15). Aspirate/wash as in step 9.. Repeat for a total of 5 washes.. (16). Add 100 µl/well of Avidin-HRP diluted in 1× Assay Diluent (dilute as noted on Certificate of Analysis).. Seal the plate and incubate at RT. for 30 minutes. (17). Aspirate and wash as in step 9.. In this wash step, soak wells in Wash. Buffer for 1 to 2 minutes prior to aspiration.. Repeat for a total of 7. washes. (18). Add 100 µl/well of Substrate Solution to each well. room temperature for 15 minutes. (19). Add 50 µl/well of Stop Solution to each well.. 34. Incubate plate at.
(43) (20). Read plate at 450 nm by ELISA reader (Multiskan Spectrum, Thermo Electron Corporation, San Jose, CA, USA), and subtract the values of 570 nm from those of 450 nm and analyze data.. 3-2-5 Haematoxylin and Eosin Staining (HE stain) (1). Rinse sections to water. (2). Place sections in Mayers haematoxylin solution for 5 minutes. (3). Wash in tap water. (4). Place sections in 1% acid alcohol for a few seconds. (5). Wash in tap water. (6). Place sections in eosin (1%) for 5 minutes. (7). Wash in tap water. (8). Dehydration by serial concentrated alcohol (70%, 80%, 90%, 100%). (9). Mount sections and photograph record.. 35.
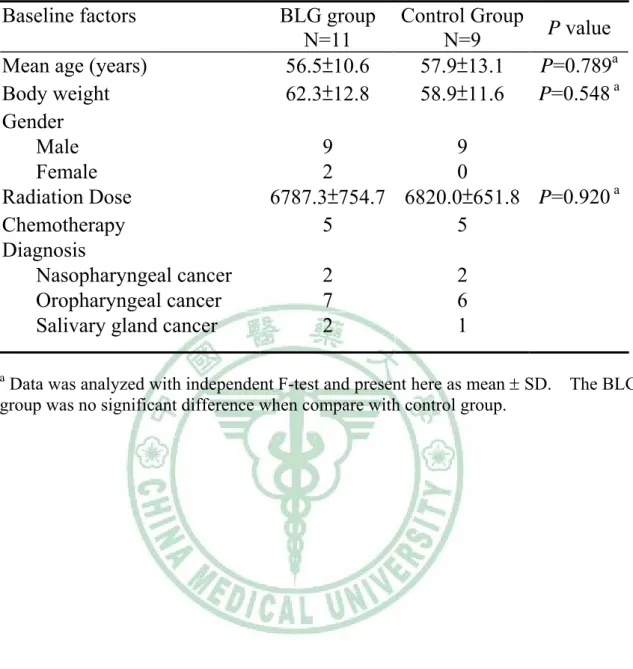
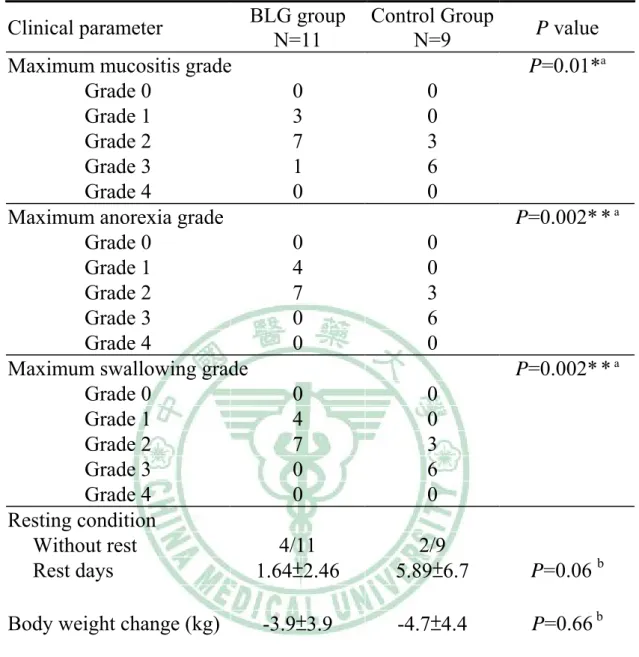
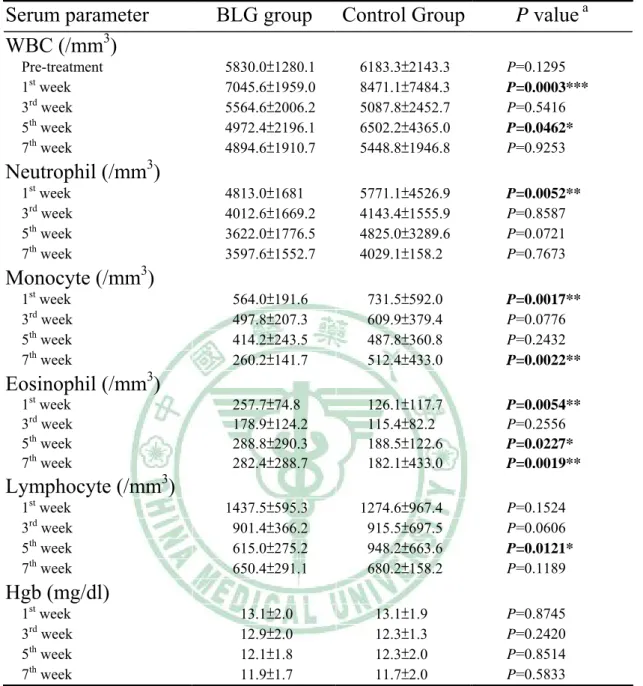
(44) Chapter 4: Results 4-1. Clinical results correlate to BLG Between October 2005 and May 2006, 20 patients were randomized. in clinical trial. Of these 20 patients, 11 were enrolled in the BLG group and 9 were enrolled in the placebo group. The distributions of patients according to age, body weight, gender, radiation dose, chemotherapy and diagnosis were similar between the two treatment groups [Table 4]. The clinical results of between two groups were listed in table 5. Our clinical trial showed that BLG improved objective symptomradiation mucositis (P=0.01). Lower the severity of clinical subjective symptoms such as anorexia (P=0.002) and swallowing difficulty (P=0.002). Most patients need to take rest during radiotherapy course because of severe radiation-induced mucositis and dermatitis. In our clinical trial, although patients’ resting day didn’t showed significance (P=0.06), we still can found that less rest were needed in BLG group and higher complete radiotherapy rate without rest (4/11 versus 2/9). The result of blood contents analysis in clinical trial was shown in Table 6. Less WBC counts was found in BLG group, especially in 5th weeks after start of radiotherapy (4972.4 ± 2196.1 vs. 6502.2 ± 4365.0 /mm3, P=0.046). Differential count of WBC disclosed that less eosinophils and lymphocytes. These results may explain why less WBC was found in 5th weeks. In contrary, absolute monocyte was higher in control group and showed significance in 7th week (P=0.0022).. Hemoglobin showed no. significant difference between BLG and control group. Serum cytokines analysis was analyzed by ELISA assay. The results. 36.
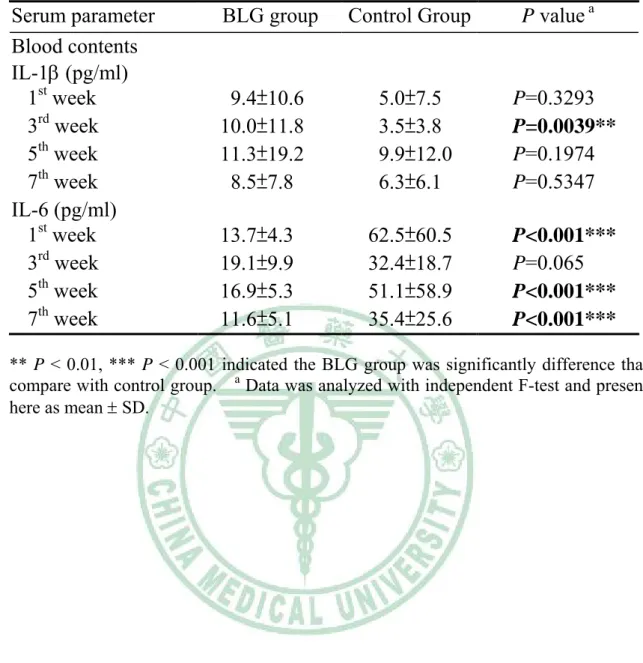
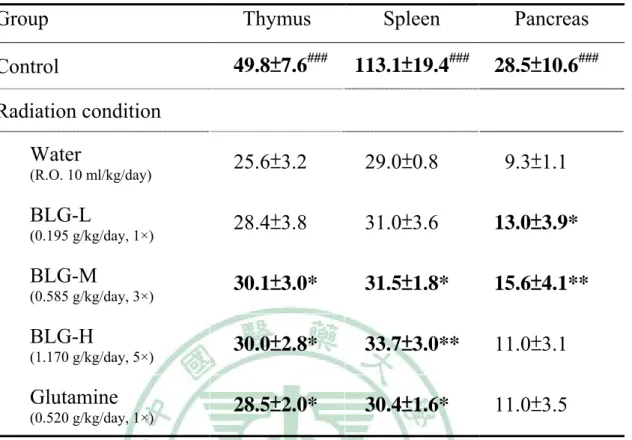
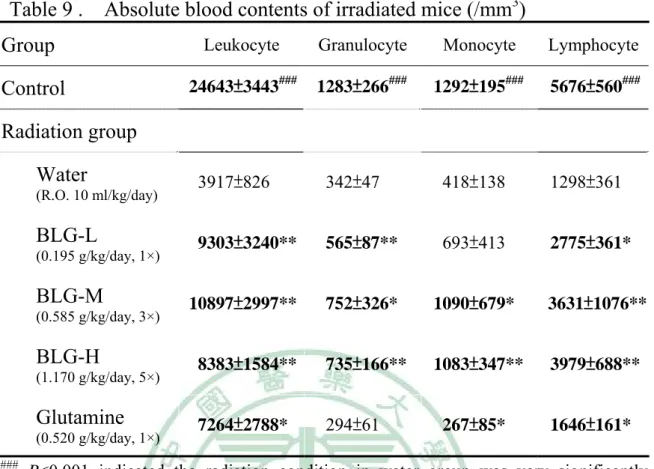
(45) were shown in Table 7. Pro-inflammatory cytokines IL-1β was lower in BLG group but didn’t showed significance except at 3rd weeks. Serum IL-6 level was much lower in BLG group at 1st, 5th and 7th week after radiotherapy and showed significantly difference when compared with control group.. 4-2. Influence of BLG to immune organs in irradiated mice As listed in Table 8, immune organs such as spleen, thymus and. pancreas were found to be significantly lower in irradiated control group compared with naïve group (0.0029±0.0008, 0.0256±0.0032 and 0.0093± 0.0011 vs. 0.1131 ± 0.0194, 0.0498±0.0076 and 0.0285±0.0106 g, respectively, P<0.001). That means this animal model was effective. Among BLG groups, BLG-M and BLG-H group showed higher immune organs preservation ability of thymus and spleen and in dose-dependent relationship. In contrary to spleen and thymus, BLG-M showed best preservation ability for pancreas (P<0.05).. 4-3. Influence of BLG to blood counts in irradiated mice The result of mice blood contents analysis was listed in Table 9.. Blood contents and its differentiation count such as granulocyte, monocyte and lymphocyte were found to be significantly lower in irradiated control group compared with naïve group that means this animal model was effective. BLG-treated groups had significantly higher lymphocyte, monocyte and granulocyte when compared to control group and in dose-dependent relationship. These results were corresponding to immune 37.
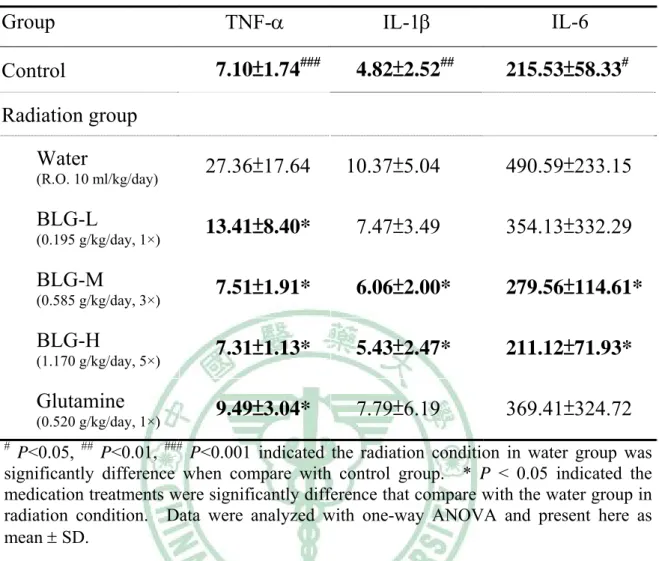
(46) organs preservation effect of BLG. Glutamine also has similar effects but not as well as BLG groups.. 4-5. Influence of BLG to cytokines in animal model Serum cytokines was quantitatively analysis its amount by ELISA. assay. TNF-α, IL-1β and IL-6 quantitative amount were made and these results were shown in Table 10. BLG groups takes great part in lowering serum TNF-α, IL-1β and IL-6, that were correlate with BLG dose. Higher BLG dose was correlated with lower serum pro-inflammatory cytokines in linear relationship. Glutamine has effect in lower TNF-α but plays no role in IL-1β and IL-6 (P=0.008, 0.331 and 0.352, respectively).. 4-6. Histopathologic assessment in animal model The results of histopathologic assessment in animal model were. listed in Table 11. Ileal villous number and height were found to be significantly lower in irradiated control group compared with naïve group (9.17 ± 0.98 and 0.32 ± 0.07 /mm vs. 12.67 ± 0.52 and 0.49 ± 0.09 mm, respectively, P <0.01 and P<0.001).. High dose BLG significantly showed. a increase in villi number but not villi height when compared with control group. Glutamine pretreatment before irradiation significantly prevented a decrease in villous number and height (10.83±0.75 vs. 9.17±0.98 mm, P=0.008).. 38.
(47) Chapter 5: Discussion Acute radiation mucositis is a result of mitotic cell death in the mucosa, disruption of the epithelial barrier, and mucosal inflammation. Pathogenesis of radiation mucositis is presumed to be an inflammatory process in which various mediators take place. The activation of inflammatory cells leads to the synthesis and release of certain cytokines, inflammatory mediators, and reactive oxygen metabolites. Among these cytokines, TNF-α and IL-6 are key pro-inflammatory mediators, which are often over-expression in cancer patients. TNF-α is produced after stimulation of mainly macrophages and monocytes. In addition, TNF-α binds to receptors on endothelial cells to initiate angiogenesis then produces vascular damage and the expression of IL-6 [62]. IL-6 is released by stimulation of T and B lymphocytes, macrophages, fibroblasts and endothelial cells. Radiation is found to induce TNF-α which may exacerbate the cytotoxic effects of radiation [63, 64]. Recent clinical studies have shown that the circulating serum level of IL-6 correlates with the disease progression and prognosis of cancer patients [65, 66]. Haveman et al. reported no increase in TNF-α level was observed while a significant radiation-induced rise in circulating IL-6 levels in experimental study [67]. However, Tang et al. evaluated the effect of pelvic irradiation on IL-6 and CRP levels in patients with cervical carcinoma and found no significant difference in patients treated with external beam RT [68].. The significance failure might have been a result of an inadequate. sample size.. In a recent clinical study, Akmansu et al. showed a significant. rise in TNF-α level with radiotherapy in all patients and also in IL-6 levels in patients treated with postoperative adjuvant radiotherapy [69].. Yuhchyau. et al. analyzed 24 lung cancer patients who received radiotherapy and 39.
(48) evaluated the correlation between serum cytokines and radiation pneumonitis, IL-lα and IL-6 were the only 2 cytokines that correlated significantly with radiation pneumonitis [70]. BLG is one of the plants in Cruciferae family. BLG was known to have antiviral effects to against influenza, hepatitis virus and Japanese encephalitis virus. Many chemical compounds were found in BLG, including indigotin, indirubin, isatin, isaindigotidione, organic acids and amino acids. In previous studies, water-insoluble component extracted by ethanol and chloroform was proved to have anti-endotoxic effect [61]. The indirubin and alkaloid isaindigotone are part of water-insoluble component from BLG. Alkaloid isaindigotone was first isolated in 1997 by Xiaoyun Wu and Guowei Qin et al. [71] and later found to be a scavenger of superoxide [72]. Indirubin was widely studied and reported to be one of most effective compounds in BLG, have anti-inflammatory and cyclin-dependent kinases (CDK) inhibitory reaction. However, the functional mechanisms of indirubin are still not very clear. According to Liu et al. study in 1997, meisoindigo was found to be a second-generation derivative of indirubin, could down-regulate the expression of c-myb mRNA, which is one of the transcriptional regulators for expression of interferon-γ mRNA [73]. Hoessel et al. studies indirubin in 1999 and reported that indirubin suppresses cyclin-dependent kinase (CDK) activities [56]. Animal study indicated that indirubin inhibit interferon-γ production from a low concentration at which indirubin did not affect cell growth and confirmed its anti-inflammatory activity [74]. Indirubin was also found to have inhibitory reaction on RANTES mRNA expression in influenza-infected bronchial epithelial cells [75]. In our clinical trial, BLG can effectively reduce the severity of 40.
(49) maximal mucositis (P=0.01), improved patients’ life qualities such as anorexia (P=0.002) and swallowing ability (P=0.002). Although less significance was found, BLG can lower the rest days (P=0.06), which most comment needed in illness patients who receive radiotherapy.. Serum IL-6. level was significantly lower in BLG group when compared with control group (P<0.001). According to the animal study of Liu et al, they used LPS to induce elevation of TNF-α and IL-6 then measured by ELISA method. Chloroform and butanol extracted fraction of BLG could lower endotoxin-induced TNF-α and IL-6 [76]. Later Lin et al. used similar mice model and further reported that chloroform and butanol extracted BLG can inhibit mitogen-activating-protein-kinases (MAPKs, p38) thus reduced LPS-induced TNF-α and IL-6 elevation [77].. In our animal study, the. similar result was found. Serum IL-1β and IL-6 are much lower in BLG groups.. It confirmed the anti-inflammatory effect of BLG.. Furthermore,. as higher dose of BLG and lower serum IL-1β and IL-6 was found to be linear-dose significance (P=0.012 and 0.001 respectively). In contrary to clinical study, our animal study disclosed BLG can increase immune organs weight; elevate blood leukocyte, granulocyte, and lymphocyte. But the possible mechanism is not clear. Several studies in China. Mainland. proposed. that. polysaccharides. of. BLG. have. immune-stimulating effect but the evidence was weak. This phenomenon remains further study in the future.. 41.
(50) Chapter 6: Conclusion BLG was used for thousands years in China and was recognized by our ancients to have anti-infection activity.. We used BLG to reduce. radiation mucositis clinically and in mice.. These data suggested the. anti-inflammatory effect and enhanced the immune cell proliferation. But the exact active compounds, mechanisms and pathways still need further analysis and evaluation.. 42.
(51) References [1].. Sonis ST, Fey EG. Oral complications of cancer therapy. Oncology (Williston Park) 2002;16:680-6.. [2].. Vissink A, Burlage FR, Spijkervet FK, Jansma J, Coppes RP. Prevention and treatment of the consequences of head and neck radiotherapy. Crit Rev Oral Biol Med 2003;14:213-25.. [3].. Knox JJ, Puodziunas AL, Feld R. Chemotherapy-induced oral mucositis. Prevention and management. Drugs Aging 2000;17:257-67.. [4].. Sonis ST. The pathobiology of mucositis. Nat Rev Cancer 2004;4:277-84.. [5].. Sonis ST, Elting LS, Keefe D, Peterson DE, Schubert M, Hauer-Jensen M, et al. Perspectives on cancer therapy-induced mucosal injury: pathogenesis, measurement, epidemiology, and consequences for patients. Cancer 2004;100:1995-2025.. [6].. Spijkervet FK, van Saene HK, Panders AK, Vermey A, van Saene JJ, Mehta DM, et al. Effect of chlorhexidine rinsing on the oropharyngeal ecology in patients with head and neck cancer who have irradiation mucositis. Oral Surg Oral Med Oral Pathol 1989;67:154-61.. [7].. Shenep JL, Kalwinsky DK, Hutson PR, George SL, Dodge RK, Blankenship KR, et al. Efficacy of oral sucralfate suspension in prevention and treatment of chemotherapy-induced mucositis. J Pediatr 1988;113:758-63.. [8].. Epstein JB, Stevenson-Moore P, Jackson S, Mohamed JH, Spinelli JJ. Prevention of oral mucositis in radiation therapy: a controlled study 43.
(52) with benzydamine hydrochloride rinse. Int J Radiat Oncol Biol Phys 1989;16:1571-5. [9].. Muller-Peddinghaus R. [Pathophysiology and pharmacology of reactive oxygen species in inflammation] Arzneimittelforschung 1987;37:589-600.. [10]. BACQ ZM, HERVE A. [A new protection against x-rays.] Schweiz Med Wochenschr 1952;82:1018-20. [11]. Kligerman MM, Glover DJ, Turrisi AT, Norfleet AL, Yuhas JM, Coia LR, et al. Toxicity of WR-2721 administered in single and multiple doses. Int J Radiat Oncol Biol Phys 1984;10:1773-6. [12]. Nicolatou O, Sotiropoulou-Lontou A, Skarlatos J, Kyprianou K, Kolitsi G, Dardoufas K. A pilot study of the effect of granulocyte-macrophage colony-stimulating factor on oral mucositis in head and neck cancer patients during X-radiation therapy: a preliminary report. Int J Radiat Oncol Biol Phys. 1998;42:551-6. [13]. Wagner. W,. Alfrink. M,. Haus. U,. Matt. J.. Treatment. of. irradiation-induced mucositis with growth factors (rhGM-CSF) in patients with head and neck cancer. Anticancer Res 1999;19:799-803. [14]. Lieschke GJ, Burgess AW. Granulocyte colony-stimulating factor and granulocyte-macrophage colony-stimulating factor (2). N Engl J Med 1992;327:99-106. [15]. Lieschke GJ, Burgess AW. Granulocyte colony-stimulating factor and granulocyte-macrophage colony-stimulating factor (2). N Engl J Med 1992;327:99-106.. 44.
(53) [16]. Bennett NT, Schultz GS. Growth factors and wound healing: biochemical properties of growth factors and their receptors. Am J Surg 1993;165:728-37. [17]. Braunstein S, Kaplan G, Gottlieb AB, Schwartz M, Walsh G, Abalos RM, Fajardo TT, Guido LS, Krueger JG. GM-CSF activates regenerative. epidermal. proliferation. in. human. growth skin. and in. stimulates. vivo.. J. keratinocytes. Invest. Dermatol. 1994;103:601-4. [18]. Souba WW. Glutamine and cancer. Ann Surg. 1993;218:715-28. [19]. Souba WW, Klimberg VS, Plumley DA, Salloum RM, Flynn TC, Bland KI, et al. The role of glutamine in maintaining a healthy gut and supporting the metabolic response to injury and infection. J Surg Res. 1990;48:383-91. [20]. Klimberg VS, Nwokedi E, Hutchins LF, Pappas AA, Lang NP, Broadwater JR, et al. Glutamine facilitates chemotherapy while reducing toxicity. JPEN J Parenter Enteral Nutr 1992;16:83-7S. [21]. Klimberg VS, Souba WW, Dolson DJ, Salloum RM, Hautamaki RD, Plumley DA, et al. Prophylactic glutamine protects the intestinal mucosa from radiation injury. Cancer 1990;66:62-8. [22]. Souba WW, Klimberg VS, Copeland EM 3rd. Glutamine nutrition in the management of radiation enteritis. JPEN J Parenter Enteral Nutr 1990;14:106-8S. [23]. Rouse K, Nwokedi E, Woodliff JE, Epstein J, Klimberg VS. Glutamine enhances selectivity of chemotherapy through changes in glutathione metabolism. Ann Surg 1995;221:420-6. 45.
(54) [24]. Gras G, Porcheray F, Samah B, Leone C. The glutamate-glutamine cycle as an inducible, protective face of macrophage activation. J Leukoc Biol 2006;80:1067-75. [25]. Huang EY, Leung SW, Wang CJ, Chen HC, Sun LM, Fang FM, et al. Oral glutamine to alleviate radiation-induced oral mucositis: a pilot randomized trial. Int J Radiat Oncol Biol Phys 2000;46:535-9. [26]. Thompson MM, Nasim A, Sayers RD, Thompson J, Smith G, Lunec J, et al. Oxygen free radical and cytokine generation during endovascular and conventional aneurysm repair. Eur J Vasc Endovasc Surg 1996;12:70-5. [27]. Katsuta T, Saito T, Shigemitsu Y, Kinoshita T, Shiraishi N, Kitano S. Relation between tumour necrosis factor alpha and interleukin 1beta producing capacity of peripheral monocytes and pulmonary complications following oesophagectomy. Br J Surg 1998;85:548-53. [28]. Nakashima J, Tachibana M, Ueno M, Miyajima A, Baba S, Murai M. Association between tumor necrosis factor in serum and cachexia in patients with prostate cancer. Clin Cancer Res 1998;4:1743-8. [29]. Fujiwaki R, Hata T, Miyazaki K, Kawamura T, Inada K. Elevation of serum interleukin-1 receptor antagonist levels in women with gynaecological cancers. Br J Obstet Gynaecol 1997;104:1407-8. [30]. Kabir S, Daar GA. Serum levels of interleukin-1, interleukin-6 and tumour necrosis factor-alpha in patients with gastric carcinoma. Cancer Lett 1995;95:207-12. [31]. De Vita F, Orditura M, Auriemma A, Infusino S, Roscigno A, Catalano G. Serum levels of interleukin-6 as a prognostic factor in 46.
(55) advanced non-small cell lung cancer. Oncol Rep 1998;5:649-52. [32]. Wojciechowska-Lacka A, Adamiak E, Stryczynska G, Lacki JK. Prognostic value of serial serum interleukin-6 level estimation in patients with lung cancer: a preliminary report. Yale J Biol Med 1997;70:139-48. [33]. Yokoe T, Iino Y, Takei H, Horiguchi J, Koibuchi Y, Maemura M, et al. Changes of cytokines and thyroid function in patients with recurrent breast cancer. Anticancer Res 1997;17:695-9. [34]. Ueda T, Shimada E, Urakawa T. Serum levels of cytokines in patients with colorectal cancer: possible involvement of interleukin-6 and interleukin-8. in. hematogenous. metastasis.. J. Gastroenterol. 1994;29:423-9. [35]. Orditura M, De Vita F, Catalano G, Infusino S, Lieto E, Martinelli E, et al. Elevated serum levels of interleukin-8 in advanced non-small cell lung cancer patients: relationship with prognosis. J Interferon Cytokine Res 2002;22:1129-35. [36]. Movat HZ, Cybulsky MI, Colditz IG, Chan MK, Dinarello CA. Acute inflammation in gram-negative infection: endotoxin, interleukin 1, tumor necrosis factor, and neutrophils. Fed Proc 1987;46:97-104. [37]. Bower JE, Ganz PA, Aziz N, Olmstead R, Irwin MR, Cole SW. Inflammatory responses to psychological stress in fatigued breast cancer survivors: Relationship to glucocorticoids. Brain Behav Immun 2006; 64: 604-11. [38]. Collado-Hidalgo A, Bower JE, Ganz PA, Cole SW, Irwin MR. Inflammatory biomarkers for persistent fatigue in breast cancer 47.
(56) survivors. Clin Cancer Res 2006;12:2759-66. [39]. Bower JE, Ganz PA, Desmond KA, Bernaards C, Rowland JH, Meyerowitz BE, et al. Fatigue in long-term breast carcinoma survivors: a longitudinal investigation. Cancer 2006;106:751-8. [40]. Bower JE, Ganz PA, Aziz N, Fahey JL. Fatigue and proinflammatory cytokine activity in breast cancer survivors. Psychosom Med 2002;64:604-11. [41]. Zhang K, Gharaee-Kermani M, McGarry B, Remick D, Phan SH. TNF-alpha-mediated lung cytokine networking and eosinophil recruitment in pulmonary fibrosis. J Immunol 1997;158:954-9. [42]. Piguet PF, Collart MA, Grau GE, Kapanci Y, Vassalli P. Tumor necrosis factor/cachectin plays a key role in bleomycin-induced pneumopathy and fibrosis. J Exp Med 1989;170:655-63. [43]. Pons I, Gras G, Courberand S, Benveniste O, Dormont D. Consequences of gamma-irradiation on inflammatory cytokine regulation in human monocytes/macrophages. Int J Radiat Biol 1997;71:157-66. [44]. Lee WR, Berkey B, Marcial V, Fu KK, Cooper JS, Vikram B, et al. Anemia is associated with decreased survival and increased locoregional failure in patients with locally advanced head and neck carcinoma: a secondary analysis of RTOG 85-27. Int J Radiat Oncol Biol Phys 1998;42:1069-75. [45]. Sullivan GW, Carper HT, Novick WJ Jr, Mandell GL. Inhibition of the inflammatory action of interleukin-1 and tumor necrosis factor (alpha) on neutrophil function by pentoxifylline. Infect Immun 48.
(57) 1988;56:1722-9. [46]. Ambrus JL, Ambrus CM, Gastpar H. Studies on platelet aggregation with pentoxifylline: effect on neoplastic disorders and other new indications. J Med 1979;10:339-45. [47]. Jiangsu New Medical College. Dictionary of Chiuese Crude Drugs; Shanghai Scientific and Technological Press, Shanghai, 1985; p. 1250-52. [48]. Ministry of Public Health. Chinese Pharmacopeia, Part I; People's Health Press: Beijing, 1995; p. 171. [49]. Bensky D, Gamble A. Chinese Herbal Medicine: Materia Medica. Revised Ed. Seattle: Eastland Press; 1993. p. 875 [50]. Hocking G. A Dictionary of Natural Products. Medford (NJ): Plexus Publishing Inc; 1997. [51]. Ho YL, Chang YS. Studies on the antinociceptive, anti-inflammatory and anti pyretic effects of Isatis indigotica root. Phytomedicine 2002;9:419-24. [52]. Centers for Disease Control (CDC) Interim Guidance on Severe Acute Respiratory. Syndrome. (SARS).. http://www.cdc.. gov/ncidod/sars/ic-closecontacts.htm. [53]. Lin CW, Tsai FJ, Tsai CH, Lai CC, Wan L, Ho TY, et al. Anti-SARS coronavirus 3C-like protease effects of Isatis indigotica root and plant-derived phenolic compounds. Antiviral Res 2005;68:36-42. [54]. Hou HC, Liang SZ. [Determination of indirubin and indigo in Baphicacanthus cusia (Nees) Bremek byHPLC] Zhong Yao Cai 49.
(58) 2006;29:681-2. [55]. Li L, Liang HQ, Liao SX, Qiao CZ, Yang GJ, Dong TY. [Chemical studies of Strobilanthes cusia] Yao Xue Xue Bao 1993;28:238-40. [56]. Hoessel R, Leclerc S, Endicott JA, Nobel ME, Lawrie A, Tunnah P, et al. Indirubin, the active constituent of a Chinese antileukaemia medicine,. inhibits. cyclin-dependent. kinases.. Nat. Cell. Biol. 1999;1:60-7. [57]. Sethi G, Ahn KS, Sandur SK, Lin X, Chaturvedi MM, Aggarwal BB. Indirubin enhances tumor necrosis factor-induced apoptosis through modulation of nuclear factor-kappa B signaling pathway. J Biol Chem 2006;281:23425-35. [58]. Sugihara K, Kitamura S, Yamada T, Okayama T, Ohta S, Yamashita K, et al. Aryl hydrocarbon receptor-mediated induction of microsomal drug-metabolizing enzyme activity by indirubin and indigo. Biochem Biophys Res Commun 2004;318:571-8. [59]. Peter Guengerich F, Martin MV, McCormick WA, Nguyen LP, Glover E, Bradfield CA. Aryl hydrocarbon receptor response to indigoids. in. vitro. and. in. vivo.. Arch. Biochem. Biophys. 2004;423:309-16. [60]. Molina P, Tarraga A, Gonzalez-Tejero A, Rioja I, Ubeda A, Terencio MC, et al. Inhibition of leukocyte functions by the alkaloid isaindigotone from Isatis indigotica and some new synthetic derivatives. J Nat Prod 2001;64:1297-300. [61]. Yu CH, Wu QF, Sheng ZH, Zeng XY, Liu DH. [Study on the extraction of indirubin from Isatis indigotica Fort] Zhong Yao Cai 50.
(59) 2006;29:721-3. [62]. Moldawer LL, Copeland EM 3rd. Proinflammatory cytokines, nutritional support, and the cachexia syndrome: interactions and therapeutic options. Cancer 1997;79:1828-39. [63]. Peng RY, Gao YB, Chen HY, Fu KF, Ma JJ, Wang XM, et al. [The expression of TNF-alpha in the intestine of mice irradiated by neutron and gamma rays] Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi 2005;21:687-9. [64]. Liu L, Lu H, Ruebe CE, Ruebe CH. [TNF-alpha mRNA expression in lung cancer cell lines induced by ionizing radiation] Zhonghua Zhong Liu Za Zhi 2005;27:347-9. [65]. Rube CE, Wilfert F, Uthe D, Konig J, Liu L, Schuck A, et al. Increased expression of pro-inflammatory cytokines as a cause of lung toxicity after combined treatment with gemcitabine and thoracic irradiation. Radiother Oncol 2004;72:231-41. [66]. Barthelemy-Brichant N, Bosquee L, Cataldo D, Corhay JL, Gustin M, Seidel L, et al. Increased IL-6 and TGF-beta1 concentrations in bronchoalveolar lavage fluid associated with thoracic radiotherapy. Int J Radiat Oncol Biol Phys 2004;58:758-67. [67]. Haveman J, Geerdink AG, Rodermond HM. TNF, IL-1 and IL-6 in circulating blood after total-body and localized irradiation in rats. Oncol Rep 1998;5:679-83. [68]. Tang JT, Yamazaki H, Nishimoto N, Inoue T, Nose T, Koizumi M, et al. Effect of radiotherapy on serum level of interleukin 6 in patients with cervical carcinoma. Anticancer Res 1996;16:2005-8. 51.
(60) [69]. Akmansu M, Unsal D, Bora H, Elbeg S. Influence of locoregional radiation treatment on tumor necrosis factor-alpha and interleukin-6 in the serum of patients with head and neck cancer. Cytokine 2005;31:41-5. [70]. Chen Y, Williams J, Ding I, Hernady E, Liu W, Smudzin T, et al. Radiation pneumonitis and early circulatory cytokine markers. Semin Radiat Oncol 2002;12:26-33. [71]. Li B, Chen WS, Zhang HM, Zhang WD, Yang GJ, Qiao CZ. [A new alkaloids isolated from tetraploidy banlangen] Yao Xue Xue Bao 2003;38:430-2. [72]. Molina P, Tarraga A, Gonzalez-Tejero A, Rioja I, Ubeda A, Terencio MC, et al. Inhibition of leukocyte functions by the alkaloid isaindigotone from Isatis indigotica and some new synthetic derivatives. J Nat Prod 2001;64:1297-300. [73]. Liu XM, Wang LG, Li HY, Ji XJ. Induction of differentiation and down-regulation of c-myb gene expression in ML-1 human myeloblastic leukemia cells by the clinically effective anti-leukemia agent meisoindigo. Biochem Pharmacol 1996;51:1545-51. [74]. Kunikata T, Tatefuji T, Aga H, Iwaki K, Ikeda M, Kurimoto M. Indirubin. inhibits. inflammatory. reactions. in. delayed-type. hypersensitivity. Eur J Pharmacol 2000;410:93-100. [75]. Mak NK, Leung CY, Wei XY, Shen XL, Wong RN, Leung KN, et al. Inhibition of RANTES expression by indirubin in influenza virus-infected human bronchial epithelial cells. Biochem Pharmacol. 2004;67:167-74. 52.
數據
+7
Outline
相關文件
We then use Theorem 1 to show that a graph having neither articulation points nor similar pairs must have an induced subgraph isomorphic to some member of
the prediction of protein secondary structure, multi-class protein fold recognition, and the prediction of human signal peptide cleavage sites.. By using similar data, we
The loss of integrity of the gingival crevicular tissues, as a result of periodontitis and radiotherapy induced thinning of these tissues together with xerostomia, mucositis, altered
Children “are more sensitive to radiation (i.e., estimates of their lifetime risk for cancer incidence and mortality per unit dose of ionizing radiation are higher) and they have
The growth in the number of vanco- mycin-induced thrombocytopenia cases presently seen may be associated with the increased use of the drug, especially in multiresistant patients
Exclusion criteria were: 1) Lack of initial histological diagnosis; 2) follow-up period of less than one year; 3) lesion with clinical appearance or histological findings white,
Oral and maxillofacial metastasis of male breast cancer: Report of a rare case and literature review
Less than 1% of all breast cancers occur in male patients, and to date, only 8 cases of metastatic breast adeno- carcinoma to the oral and maxillofacial region in a male patient
Exposure to radiation causes damage to living tissue, resulting in skin burns, radiation sickness and death at high doses and cancer, tumors and genetic damage at low
