Almond consumption improved glycemic control and lipid profiles in
patients with type 2 diabetes mellitus
Sing-Chung Li
a,1, Yen-Hua Liu
a,1, Jen-Fang Liu
a, Wen-Hsin Chang
a,
Chiao-Ming Chen
b, C.-Y. Oliver Chen
c,⁎
aSchool of Nutrition and Health Science, Taipei Medical University, Taipei City, 110, Taiwan
bDepartment of Food Science, Nutrition and Nutraceutical Biotechnology, Shih Chien University, Taipei City, 110, Taiwan cAntioxidants Research Laboratory, Jean Mayer USDA Human Nutrition Research Center on Aging, Tufts University, Boston, MA 02111, USA
Received 13 January 2010; accepted 12 April 2010
Abstract
Almond consumption is associated with ameliorations in obesity, hyperlipidemia, hypertension, and hyperglycemia. The hypothesis of this 12-week randomized crossover clinical trial was that almond consumption would improve glycemic control and decrease the risk for cardiovascular disease in 20 Chinese patients with type 2 diabetes mellitus (T2DM) (9 male, 11 female; 58 years old; body mass index, 26 kg/m2) with mild hyperlipidemia. After a 2-week run-in period, patients were assigned to either a control National Cholesterol Education
Program step II diet (control diet) or an almond diet for 4 weeks, with a 2-week washout period between alternative diets. Almonds were added to the control diet to replace 20% of total daily calorie intake. Addition of approximately 60 g almonds per day increased dietary intakes of fiber, magnesium, polyunsaturated fatty acid, monounsaturated fatty acid, and vitamin E. Body fat determined with bioelectrical impedance analysis was significantly lower in patients consuming almonds (almonds vs control: 29.6% vs 30.4%). The almond diet enhanced plasmaα-tocopherol level by a median 26.8% (95% confidence intervals, 15.1-36.6) compared with control diet. Furthermore, almond intake decreased total cholesterol, low-density lipoprotein cholesterol, and the ratio of low-density lipoprotein cholesterol to high-density lipoprotein cholesterol by 6.0% (1.6-9.4), 11.6% (2.8-19.1), and 9.7% (0.3-20.9), respectively. Plasma apolipoprotein (apo) B levels, apo B/apo A-1 ratio, and nonesterified fatty acid also decreased significantly by 15.6% (5.1-25.4), 17.4% (2.8-19.9), and 5.5% (3.0-14.4), respectively. Compared with subjects in the control diet, those in the almond diet had 4.1% (0.9-12.5), 0.8% (0.4-6.3), and 9.2% (4.4-13.2) lower levels of fasting insulin, fasting glucose, and homeostasis model assessment of insulin resistance index, respectively. Our results suggested that incorporation of almonds into a healthy diet has beneficial effects on adiposity, glycemic control, and the lipid profile, thereby potentially decreasing the risk for cardiovascular disease in patients with type 2 diabetes mellitus.
© 2010 Elsevier Inc. All rights reserved.
1. Introduction
More than 20 million people have type 2 diabetes mellitus (T2DM) in the United States and 135 million worldwide, and the number unfortunately keeps growing mainly because of a prevalence of overweight and obese populations. The burden of health issue related to the DM patients is beyond that resulting from diabetes-related complications. Because
cardiovascular risk factors cluster in T2DM, these patients have greater risk for cardiovascular disease (CVD) than nondiabetic equivalents even when blood glucose levels are under control[1]. The main components of T2DM include hyperglycemia, oxidative stress, chronic mild inflammation, and dyslipidemia; and they all are associated with increased risk of CVD. The standard treatment for T2DM patients is to control blood glucose and lipid profile in the recommended ranges. Health-promoting lifestyle and dietary practices may also help better manage diabetes-related complications, particularly CVD because it accounts for greater than 70% morbidity and mortality[2].
Tree nuts have become a healthy food, with support from a growing body of epidemiologic evidence showing a strong association of nut consumption to lower risk of CVD and
Available online at www.sciencedirect.com
Metabolism Clinical and Experimental xx (2010) xxx–xxx
www.metabolismjournal.com
Institutional approval: The study protocol was approved by the Institutional Review Board of the Taipei Medical University, and written consent was obtained from each participant prior to participation in the study.
⁎ Corresponding author.
E-mail address:[email protected](C.-Y.O. Chen).
1 This authors contributed equally to this work.
0026-0495/$– see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.metabol.2010.04.009
diabetes[3-5]. This benefit may underlie the nut nutrients that comply with the recommended dietary guidelines for Americans and fit very well into a heart-healthy diet. Particularly, nuts are rich sources of unsaturated fats, fiber, minerals, and proteins[6]. Furthermore, epidemiologic and clinical evidence has shown that their consumptions were associated with improved hyperlipidemia and insulin sensitivity, decreased inflammation and oxidative stress, and reduced/maintained body weight [7]. The American Diabetes Association also recommends inclusion of nuts into the diet of diabetes to treat or manage CVD risk[8].
Almonds are the most consumed tree nut, with per capita nut consumption at 1 lb/y in the United States[9]. Almonds may be cardioprotective because they are excellent sources of monounsaturated fats,α-tocopherol, dietary fiber, copper, magnesium, arginine, plant sterols, and polyphenols[6,10]. Most almond studies in the literature have illustrated the hypolipidemic effect of almonds in healthy subjects or hypercholesterolemic patients. Regarding glycemic control, Jenkins et al[11]found that almonds lowered postprandial glucose excursion in healthy individuals. However, Lovejoy et al[12]had found that almonds incorporated into a low- or high-fat diet did not affect glycemia and lipid profiles of American T2DM patients. In this controlled feeding study, we aim to investigate the extent by which incorporation of almonds into the National Cholesterol Education Program (NCEP) [13] step II diet improves insulin sensitivity and lipid profile in Chinese T2DM patients.
2. Materials and methods 2.1. Subjects
Thirty Chinese T2DM patients previously diagnosed by a physician were recruited from the Endocrine Clinic of the Taipei Medical University Hospital, Taiwan. Among them, 8 patients were not qualified for the study because they did not meet all of the following eligibility criteria. The eligibility criteria included (1) serum cholesterol greater than 200 mg/dL or triglycerol greater than 150 mg/dL, free of dietary restrictions/food allergies; (2) not receiving insulin therapy; (3) not using medications or supplementations known to alter lipid metabolism; (4) stable blood lipid and sugar levels within 3 months before study; (5) no clinical history of cardiovascular, hepatic, gastrointestinal, or renal disease; (6) no alcoholism; and (7) no recent history of smoking. All women were postmenopausal, and all subjects were taking oral hypoglycemic agents. All participants were asked to stay with the same medications and refrain from nuts and supplements. Three-day dietary record, including 2 weekdays and 1 weekend day, was collected weekly from the subjects to monitor dietary compliance and assess nutrient intakes. The study protocol was approved by the Institutional Review Board of the Taipei Medical University, and written consent was obtained from each participant before participation in the study.
2.2. Study design
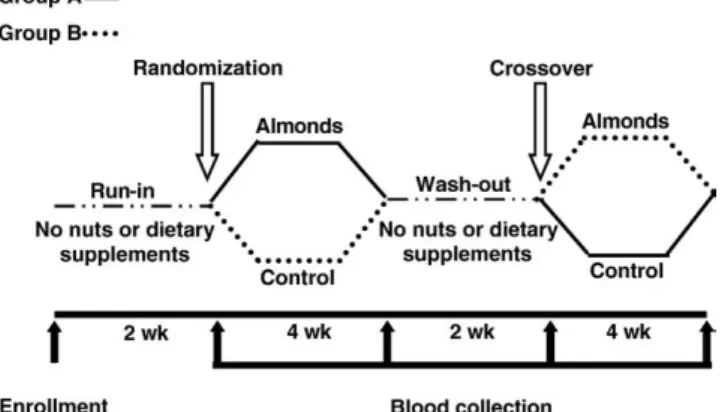
In a 12-week randomized crossover trial with a 2-week washout between alternative diets, subjects were assigned to receive control or almond diet for 4 weeks after a 2-week run-in period (Fig. 1). To diminish the impact of background diet on study outcomes, patients consumed meals prepared by the metabolic kitchen of Taipei Medical University Hospital during dietary interventions. During run-in and washout periods, the subjects consumed their habitual diets without nuts; and a daily diet diary was used to monitor the compliance. A registered dietitian instructed all participants on how to select appropriate foods during run-in and washout periods and prepare dietary records. Four overnight-fast blood samples and anthropometric data were collected from each participant before and after each dietary treatment.
2.3. Diets
Meals for each patient were prepared to meet daily caloric requirement to maintain body weight by the metabolic kitchen of the Taipei Medical University Hospital. Caloric adjustments were made as needed to maintain body weight within 2 kg of each person's initial value. Based on the NCEP step II dietary guideline [13], the control diet was designed to provide daily calories from carbohydrate, protein, and fat at 56%, 17%, and 27%, respectively. Furthermore, calories from saturated and polyunsaturated fat were less than 7% and 10%, respectively; and cholesterol content was less than 200 mg. The almond diet was prepared by incorporating roasted, unsalted whole almonds with skins into meals to replace 20% calories of the control diet. Depending on the menus, almonds were either incorporated into entrees and deserts or consumed as snack. On average, a patient consumed 56 g of almonds a day. Almonds were sweet almonds containing small amounts of cyanogenic compounds [11]. They were generously provided by the Almond Board of California. A 5-day menu rotation was used to make food more appealing and palatable to the participants throughout the study. The participants were provided with all foods needed during the dietary
interven-Fig. 1. Study design. 2 S.-C. Li et al. / Metabolism Clinical and Experimental xx (2010) xxx–xxx
tion. All meals were packaged for takeout. To assist with compliance assessment, each participant completed a daily food diary in which the patient recorded the study foods not eaten, nonstudy foods eaten, and beverages consumed. Nutrient compositions of the almond and control diets were calculated using the Nutritional Chamberlain Line, Nutri-tionist Edition, version 2002 (E-Kitchen Business, Taichung City, Taiwan).
2.4. Anthropometric measurements
Body height, weight, and fat mass were assessed using a body composition analyzer (X-SCAN PLUS; Jawon Med-ical, Seoul, Korea). The subjects were dressed in light attire and bare feet. They were also asked to empty their bladders before the measurements to minimize the measurement errors. This device uses the bioelectrical impedance method with 8 electrodes placed on hands and feet (or ankles) and multifrequency (1, 5, 50, 250, 550, 1000 kHz). The percentage of body fat was estimated up to 0.1% using the built-in experimentally derived algorithm. Body mass index (BMI) was calculated as weight/height2 (in kilograms per square meter). After more than 10 minutes of rest in a quiet room, blood pressure was determined using the automatic blood pressure monitor FT-500 R (Jawon Medical). 2.5. Sample preparation and storage
After an overnight fast, blood was withdrawn with and without anticoagulants (EDTA and NaF). Subsequently, plasma was collected after centrifugation at 1400g for 10 minutes at 4°C. Aliquots of plasma and serum were prepared and stored in−80°C for following biochemical measurements. 2.6. Glycemic control and lipid profiles
Glucose in NaF plasma was determined by an enzymatic assay using a clinical chemistry analyzer (SYNCHRON LX 20; Beckman Coulter, Fullerton, CA). Insulin level in serum was determined by an immunoassay (Mercodia, Uppsala, Sweden). Insulin sensitivity was estimated using the homeostasis model assessment (HOMA-OR) based on the following formula: insulin × glucose/22.5, with insulin expressed in microunits per milliliter and glucose in millimoles per liter. Lipid profiles in serum were determined with enzymatic assays using a clinical chemistry analyzer (SYNCHRON LX 20).
Concentrations of apolipoprotein (apo) A-1 and apo B in serum were measured using immunoturbidimetric immu-noassays (Randox Laboratories, Antrim, United Kingdom). Nonesterified fatty acids in EDTA plasma were determined by an enzymatic assay (Randox Laboratories).
2.7. Plasmaα-tocopherol
α-Tocopherol in EDTA plasma was determined using a reverse-phase high-performance liquid chromatography system equipped with a LiChroCART C-18 column (4 × 250 nm, 4μm; Perkin-Elmer, West Lafayette, IN) based on
the method of Bieri et al [14]. The concentration was quantified at 292 nm after isocratic elution with the mobile phase (1% H2O in methanol with 10 mmol/L lithium
perchlorate) at 1.0 mL/min. 2.8. Statistical analysis
Results are expressed as mean ± standard error (SE). Between-diet differences are expressed as median percentage change and 95% confidence intervals. A Student t test was performed to assess nutrients between the almond and control diet. A Student paired t test was performed to evaluate the difference between the baseline and washout values of study outcomes, and the results showed that there were differences between them. A repeated-measures analysis was performed to analyze significance between treatment using PROC GLM with treatment (almond vs control), sequence (almond-control vs (almond-control-almond), period (1 vs 2), and subject as variable. The effect of sex and its interaction with other independent variables were insignificant; thus, they were excluded in the model. Furthermore, LSMEANS was performed to evaluate the significance in differences between almond and control diet. Significance was considered at P≤ .05 (2-tailed). All statistical analyses were performed using SAS 9.1 (SAS Institute, Cary, NC).
3. Results
3.1. Participant characteristics
Twenty-two participants signed consent forms and began the protocol; 20 patients completed the study with full compliance. Two subjects were excluded from the study because of noncompliance in consuming the study meals. The characteristics of 20 subjects completing the study are illustrated in the Table 1. All patients took hypoglycemia agents but not insulin. Sex did not affect study outcomes. 3.2. Study diet
The nutrients of control and almond diet for an 1800-kcal diet are illustrated in Table 2. The percentage of calories from proteins was not different between the 2 diets. However, the almond diet had 9.8% less calories from carbohydrate and 9.9% more from fat than the control diet. Particularly, the almond diet had 104% more monounsatu-rated fatty acid (MUFA) calories. Furthermore, the almond diet contained 64.8% and 400% more magnesium and α-tocopherol than the control diet, respectively.
3.3. Anthropometry
Body weight and BMI were not altered by the diets, as well as systolic and diastolic blood pressure. The body fat was decreased by a median 1.8% (95% confidence intervals, 1.1-4.8) in the T2DM patients consuming the almond diet for 4 weeks compared with those taking the control diet (P = .002) (Table 3).
3 S.-C. Li et al. / Metabolism Clinical and Experimental xx (2010) xxx–xxx
3.4. Blood biochemistries
Because almonds are rich inα-tocopherol, the change in plasmaα-tocopherol serves as an index of compliance. The almond diet enhanced plasmaα-tocopherol level by 26.8% (15.1-36.6) compared with the control diet (Table 3).
The almond diet significantly decreased fasting insulin and glucose by 4.1% (0.9-12.5) and 0.8% (0.4-6.3), respectively, as compared with the control diet. At the end of the almond phase, HOMA-IR was 9.2% (4.4-13.2) lower than that at the control phase.
Lipid profiles of the patients were improved by the almond diet. The almond diet decreased total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and LDL-C to high-density lipoprotein cholesterol (HDL-C) ratio by 6.0% (1.6-9.4), 11.6% (2.8-19.1), and 9.7%
(0.3-20.9), respectively, as compared with the control diet. Furthermore, plasma apo B level and apo B/apo A-1 ratio were decreased significantly by 15.6% (5.1-25.4) and 17.4% (2.8-19.9), respectively. Plasma nonesterified fatty acid level was significantly (5.5%, 3.0-14.4) lower in the patients consuming the almond diet than those taking the control diet.
4. Discussion
Epidemiologic evidence has suggested that consumption of nuts is associated with lower risk of CVD [4,5], purportedly because their incorporation into a choles-terol diet improved lipid profile beyond the effect of a low-cholesterol dietary plan[15]. Our study provides another line of evidence showing the benefits of almond consumption in CVD-prone T2DM patients.
Our study showed that incorporation of almonds into Chinese cuisine prepared following the NCEP step II dietary guideline decreased TC, LDL-C, and the LDL-C/HDL-C ratio, but did not affect TG and HDL-C, in Chinese T2DM patients. Our results are in line with other previous studies with either hypercholesterolemic patients or healthy subjects
[16-18]. Notably, the LDL-C level in our study was decreased by 11% in subjects consuming 60 g/d almonds, which is slightly better than the suggested 1% decrease by 7 g[16]. The improvements in lipid profiles were further substantiated by the reductions in apo B and the apo B/apo A-1 ratio. However, Jia et al[19]did not find that almond consumption at 84 or 168 g/d for 4 weeks altered TC and TG in young male Chinese smokers with normal cholesterol levels. Similar to the Jia et al study[19], Lovejoy et al[12]did not find that
Table 1
Demographics and baseline values of blood biochemistries of the subjects Subject no. 20 (9 M/11 F)
Age (y) 58 ± 2
Diabetic history (y) 8 ± 1 Use of oral hypoglycemia medication (n) 20 Insulin treatment (n) 0 BMI (kg/m2) 26.0 ± 0.7
Body fat (%) 30.6 ± 1.5 Systolic blood pressure (mm Hg) 131.0 ± 3.7 Diastolic blood pressure (mm Hg) 73.1 ± 2.6 Fasting glucose (mmol/L) 8.7 ± 0.7 Fasting insulin (μU/mL) 15.3 ± 2.1
HOMA-IR 5.71 ± 0.76
Total triglycerides (mmol/L) 1.6 ± 0.2 TC (mmol/L) 5.7 ± 0.2 LDL-C (mmol/L) 3.5 ± 0.1 HDL-C (mmol/L) 1.3 ± 0.2 LDL-C/HDL-C 3.1 ± 0.3 Apo B (mg/dL) 137.8 ± 6.5 Apo A-1 (mg/dL) 124.0 ± 11.5 Apo B/apo A-1 0.06 ± 0.03 Nonesterified fatty acid (mmol/L) 0.73 ± 0.06 Plasmaα-tocopherol (μmol/L) 27.8 ± 2.5 Data are expressed as mean ± SE.
Table 2
Nutrients of the control and almond diet, based on 1800 kcal/d
Nutrients Control diet Almond diet P valuea Energy (kcal) 1802.3 ± 5.2 1801.8 ± 4.2 NS Protein (% of energy) 16.6 ± 0.6 16.5 ± 0.3 NS Carbohydrate (% of energy) 56.8 ± 0.4 47.0 ± 0.2 ≤.0001 Fat (% of energy) 26.6 ± 0.7 36.5 ± 0.2 ≤.0001 Saturated fat (% of energy) 6.1 ± 0.5 6.1 ± 0.4 NS Monounsaturated fat
(% of energy)
8.1 ± 0.5 16.5 ± 0.4 ≤.0001 Polyunsaturated fat (% of energy) 9.4 ± 0.3 10.5 ± 0.1 ≤.05 Fiber (g) 24.6 ± 0.9 26.9 ± 0.7 ≤.05 Cholesterol (mg) 162.7 ± 17.0 130.1 ± 13.6 NS α-Tocopherol (mg) 3.8 ± 0.2 19.1 ± 0.1 ≤.0001 Magnesium (mg) 201.9 ± 4.8 332.7 ± 3.9 ≤.0001 Nutrients were calculated using E-Kitchen program. Data are expressed as mean ± SE. NS indicates not significant (PN .05).
a P value tested by a Student t test.
Table 3
Changes in BMI, blood pressure, body fat, glycemia control, lipid profile, and plasmaα-tocopherol of the T2DM patients consuming either control or almond diet for 4 weeks
Control diet Almond diet P valuea BMI (kg/m2) 25.7 ± 0.7 25.8 ± 0.8 .56
Blood pressure (systolic/diastolic) (mm Hg)
125.6/72.8 124.1/70.6 .48/.16 Body fat (%) 30.4 ± 1.5 29.6 ± 1.6 .002 Fasting glucose (mmol/L) 8.6 ± 0.6 8.3 ± 0.6 .0238 Fasting insulin (μU/mL) 13.8 ± 1.2 12.7 ± 1.1 .0184 HOMA-IR 5.2 ± 0.6 4.6 ± 0.5 .0039 Total triglycerides (mmol/L) 1.6 ± 0.2 1.5 ± 0.2 .7569 Total cholesterol (mmol/L) 5.5 ± 0.2 5.2 ± 0.2 .0025 LDL-C (mmol/L) 3.4 ± 0.1 3.0 ± 0.2 .0117 HDL-C (mmol/L) 1.2 ± 0.1 1.2 ± 0.2 .83 LDL-C/HDL-C 3.3 ± 0.2 3.0 ± 0.3 .0128 Apo B (mg/dL) 133.7 ± 6.5 110.8 ± 6.5 .0046 Apo A-1 (mg/dL) 121.2 ± 10.3 121.2 ± 11.3 .99 Apo B/apo A-1 0.06 ± 0.03 0.05 ± 0.03 .0084 Nonesterified fatty acids (mmol/L) 0.73 ± 0.06 0.66 ± 0.06 .008 Plasmaα-tocopherol (μmol/L) 25.8 ± 2.0 31.8 ± 2.5 ≤.0001 Data are expressed as mean ± SE.
a
P value for comparison between treatments tested by LSMEANS in the PROC GLM model.
4 S.-C. Li et al. / Metabolism Clinical and Experimental xx (2010) xxx–xxx
incorporation of almonds into a low-fat or high-fat diet altered TC and LDL-C in T2DM patients. Almond dosage (current study vs Lovejoy: 20% vs 10% of energy), background diet (Asian vs Western), and ethnicity (Chinese vs American) might be accountable for the underlying factors for the discrepancy in the benefits of almond consumption in diabetes. Fiber, phytosterols, polyphenolics, and a high unsaturated to saturated fat ratio[6,10]may be accountable for the hypocholesterolemic effect of almonds.
Almonds are high-fat, energy-dense food. However, observational and clinical studies have shown that almond consumption was not associated with a higher BMI or weight gain[20]. Consistent with the Fraser et al [21] study that sowed that consumption of 56 g/d almonds (providing 320 kcal/d) for 6 months did not lead to a significant weight gain in healthy people, our results showed that the almond diet did not cause weight gain in Chinese T2DM patients. An interesting finding of our study is that the almond diet lowered body fat significantly by 0.8% as compared with the control diet even though caloric intakes in this controlled feeding trial were similar between the 2 diets. This observation is in line with the Salas-Salvado et al [22]
study that showed that 30 g/d mixed nuts added to a Mediterranean diet decreased central adiposity in patients with metabolic syndrome in the absence of body weight changes. Although the mechanisms for this reduction in body fat remain to be examined, it is plausible that bioaccessibility and bioavailability of almond lipids were diminished by a physical barrier of cell walls [23]. Furthermore, absorbed almond oleic acid might facilitate fat utilization by enhancing mitochondrial fatty acid oxidation and thermogenesis through up-regulation of uncoupling protein genes[24].
High postprandial glucose and insulin levels are a particular concern for diabetic patients [25-28]. Although almonds are rich in fat, they possess a low-glycemic index and could alter the glycemic index of co-consumed foods
[11,29]. Jenkins et al[30]had reported in a clinical trial that almond consumption decreased insulin secretion in nondi-abetic hyperlipidemic patients. Thus, almond consumption might not impose risk of high postprandial glucose level on diabetic patients. However, to date, only 4 studies have been reported that examined the effect of nuts on glucose and insulin levels in T2DM or metabolic syndrome patients
[12,31-33]. Tapsell et al[31]reported that in T2DM patients, long-term supplementation of walnuts decreased fasting insulin levels, but did not alter hemoglobin A1c.
Further-more, Casas-Agustench et al[32]reported that a healthy diet supplemented with 30 g/d of raw nuts (15 g walnuts, 7.5 g almonds, and 7.5 g hazelnuts) for 12 weeks improved insulin and HOMA-IR in metabolic syndrome patients as compared with the healthy control diet. However, Lovejoy et al [12]
found that almond supplementation at 10% of daily caloric intake in either a low-fat (25% calories from fat) or high-fat (37%) diet did not alter glucose tolerance and insulin status in T2DM patients. The potential improvement in glycemic
control might be offset by increased body weight with almond consumption. In the other study, Scott et al [33]
compared the effect of a high–protein and MUFA diet with almonds as the MUFA source (44%, 22%, and 25% calories from fat, MUFA, and protein, respectively) to a contempo-rary American Heart Association diet (30%, 15%, and 15% calories from fat, MUFA, and protein, respectively) on glycemic control and CVD risk factors in 17 patients with metabolic syndrome or T2DM diabetes. They found that the patients in both treatment groups improved their glycemic control, possibly related to the weight loss observed with both treatments. In this study, we found that almonds replacing 20% calories of the control diet improved glycemic control in Chinese T2DM patients, but did not reduce glucose level to the unimpaired range (110-125 mg/dL [6.1-6.9 mmol/L]). Subject ethnicity, background diet, and almond dosage could somewhat contribute to the discrep-ancy. Magnesium, fiber, MUFA, and polyphenols in almonds are potential underlying contributors to the improvement in glycemic control[34-37].
There are 3 limitations in the study. First, the sample size is relatively small in this controlled feeding trial, so that our results might not be readily generalized to the diabetic population. Second, although almonds decreased fasted blood glucose and insulin in the patients, an oral glucose tolerance test is required to confirm their effect on insulin actions. Third, because meaningful changes in hemoglobin A1cneed a study duration of more than 1 month, its change
was not assessed in this study.
Because increased postprandial stress is a risk factor that is associated with complications of insulin resistance, future studies are warranted to assess the benefits of almond consumption on lipid profiles and glycemic control after a fat-rich meal. The mechanism of reduction in circulating insulin level by almond consumption was not studied. It will be worthwhile to determine C-peptide excretion, which is a biomarker of insulin production.
Our study confirms the hypocholesterolemic effect of almonds. We further demonstrate that incorporation of almonds into an NCEP step II diet improved glycemic control and decreased body fat in Chinese T2DM patients with a borderline-high LDL-C level. Further studies are warranted to examine whether such benefits are dependent upon background diet, lifestyle, and ethnicity, as well as the mechanism(s) contributing to improving glycemic control.
Acknowledgment
S-CL, C-YOC, and J-FL designed research; Y-HL, W-HC, and C-MC conducted research; Y-HL and W-HC analyzed the data; S-CL, C-YOC, and J-FL wrote the paper; C-YOC and J-FL had the primary responsibility for the final content. All authors read and approved the final manuscript. We would like to express our gratitude to the Almond Board of California for providing the almonds.
5 S.-C. Li et al. / Metabolism Clinical and Experimental xx (2010) xxx–xxx
Supported by a grant from the Almond Board of California (C-YOC and J-FL) and LEARN weight management foundation in Taiwan ((J-FL). The contents of this publication do not necessarily reflect the views or policies of the USDA; nor does mention of trade names, commercial products, or organizations imply endorsement by the US government.
References
[1] Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, et al. Diabetes and cardiovascular disease: a statement for healthcare professionals from the American Heart Association. Circulation 1999; 100:1134-46.
[2] Heinig RE. The patient with diabetes: preventing cardiovascular complications. Clin Cardiol 2006;29(10 Suppl):II13-20.
[3] Jiang R, Manson JE, Stampfer MJ, Liu S, Willett WC, Hu FB. Nut and peanut butter consumption and risk of type 2 diabetes in women. JAMA 2002;288:2554-60.
[4] Sabaté J, Ang Y. Nuts and health outcomes: new epidemiologic evidence. Am J Clin Nutr 2009;89:1643S-8S.
[5] Sabaté J. Nut consumption, vegetarian diets, ischemic heart disease risk, and all-cause mortality: evidence from epidemiologic studies. Am J Clin Nutr 1999;70:500S-3S.
[6] Chen C-Y, Lapsley K, Blumberg JB. A nutrition and health perspective on almonds. J Sci Food Agric 2006;86:2245-50.
[7] Jenkins DJ, Hu FB, Tapsell LC, Josse AR, Kendall CW. Possible benefit of nuts in type 2 diabetes. J Nutr 2008;138:1752S-6S. [8] Bantle JP, Wylie-Rosett J, Albright AL, Apovian CM, Clark NG,
Franz MJ, et al. Nutrition recommendations and interventions for diabetes: a position statement of the American Diabetes Association. Diabetes Care 2008;31:S61-78.
[9] Buzby JC, Pollack SL. Almonds lead increase in tree nut consumption. [Internet]. USDA's Economic Research Service; 2008 [cited 2009 Nov 10]. Available from: http://www.ers.usda.gov/amberwaves/ june08/findings/almonds.htm.
[10] Chen C-Y, Blumberg JB. Phytonutrient composition of nuts. Asian Pacific J Clin Nutr 2008;17:329-32.
[11] Jenkins DJ, Kendall CW, Josse AR, Salvatore S, Brighenti F, Augustin LS, et al. Almonds decrease postprandial glycemia, insulinemia, and oxidative damage in healthy individuals. J Nutr 2006;136:2987-92. [12] Lovejoy JC, Most MM, Lefevre M, Greenway FL, Rood JC. Effect of
diets enriched in almonds on insulin action and serum lipids in adults with normal glucose tolerance or type 2 diabetes. Am J Clin Nutr 2002; 76:1000-6.
[13] National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106:3143-421. [14] Bieri JG, Tolliver TJ, Catignani GL. Simultaneous determination of
alpha-tocopherol and retinol in plasma or red cells by high pressure liquid chromatography. Am J Clin Nutr 1979;32:2143-9.
[15] Griel AE, Kris-Etherton PM. Tree nuts and the lipid profile: a review of clinical studies. Br J Nutr 2006;96:S68-78.
[16] Jenkins DJ, Kendall CW, Marchie A, Parker TL, Connelly PW, Qian W, et al. Dose response of almonds on coronary heart disease risk factors: blood lipids, oxidized low-density lipoproteins, lipoprotein(a), homocysteine, and pulmonary nitric oxide: a randomized, controlled, crossover trial. Circulation 2002;106:1327-32.
[17] Spiller GA, Jenkins DJ, Cragen LN, Gates JE, Bosello O, Berra K, et al. Effect of a diet high in monounsaturated fat from almonds on plasma cholesterol and lipoproteins. J Am Coll Nutr 1992;11:126-30.
[18] Hyson DA, Schneeman BO, Davis PA. Almonds and almond oil have similar effects on plasma lipids and LDL oxidation in healthy men and women. J Nutr 2002;132:703-7.
[19] Jia X, Li N, Zhang W, Zhang X, Lapsley K, Huang G, et al. A pilot study on the effects of almond consumption on DNA damage and oxidative stress in smokers. Nutr Cancer 2006;54:179-83.
[20] Rajaram S, Sabate J. Nuts, body weight and insulin resistance. Br J Nutr 2006;96:S79-86.
[21] Fraser GE, Bennett HW, Jaceldo KB, Sabaté J. Effect on body weight of a free 76 kilojoule (320 calorie) daily supplement of almonds for six months. J Am Coll Nutr 2002;21:275-83.
[22] Salas-Salvadó J, Fernández-Ballart J, Ros E, Martínez-González MA, Fitó M, Estruch R, et al. Effect of a Mediterranean diet supplemented with nuts on metabolic syndrome status: one-year results of the PREDIMED randomized trial. Arch Intern Med 2008;168:2449-58. [23] Ellis PR, Kendall CW, Ren Y, Parker C, Pacy JF, Waldron KW, et al.
Role of cell walls in the bioaccessibility of lipids in almond seeds. Am J Clin Nutr 2004;80:604-13.
[24] Rodríguez VM, Portillo MP, Picó C, Macarulla MT, Palou A. Olive oil feeding up-regulates uncoupling protein genes in rat brown adipose tissue and skeletal muscle. Am J Clin Nutr 2002;75:213-20. [25] Abbott WGH, Boyce VL, Grundy SM, Howard BV. Effects of
replacing saturated fat with complex carbohydrate in diets of subjects with NIDDM. Diabetes Care 1989;12:102-7.
[26] Fukagawa NK, Anderson JW, Hageman G, Young VR, Minaker KL. High-carbohydrate, high-fiber diets increase peripheral insulin sensi-tivity in healthy young and old adults. Am J Clin Nutr 1990;52:524-8. [27] Mayer-Davis EJ, Monaco JH, Hoen HM, Carmichael S, Vitolins MZ, Rewers MJ, et al. Dietary fat and insulin sensitivity in a triethnic population: the role of obesity. The Insulin Resistance Atherosclerosis Study (IRAS). Am J Clin Nutr 1997;65:79-87.
[28] Lovejoy JC. The influence of dietary fat on insulin resistance. Curr Diab Rep 2002;2:435-40.
[29] Josse AR, Kendall CW, Augustin LS, Ellis PR, Jenkins DJ. Almonds and postprandial glycemia–a dose-response study. Metabolism 2007; 56:400-4.
[30] Jenkins DJ, Kendall CW, Marchie A, Josse AR, Nguyen TH, Faulkner DA, et al. Effect of almonds on insulin secretion and insulin resistance in nondiabetic hyperlipidemic subjects: a randomized controlled crossover trial. Metabolism 2008;57:882-7.
[31] Tapsell LC, Batterham MJ, Teuss G, Tan SY, Dalton S, Quick CJ, et al. Long-term effects of increased dietary polyunsaturated fat from walnuts on metabolic parameters in type II diabetes. Eur J Clin Nutr 2009;63:1008-15.
[32] Casas-Agustench P, López-Uriarte P, Bulló M, Ros E, Cabré-Vila JJ, Salas-Salvadó J. Effects of one serving of mixed nuts on serum lipids, insulin resistance and inflammatory markers in patients with the metabolic syndrome. Nutr Metab Cardiovasc Dis 2009 [Epub ahead of print].
[33] Scott LW, Balasubramanyam A, Kimball KT, Aherns AK, Fordis Jr CM, Ballantyne CM. Long-term, randomized clinical trial of two diets in the metabolic syndrome and type 2 diabetes. Diabetes Care 2003;26: 2481-2.
[34] Lo Piparo E, Scheib H, Frei N, Williamson G, Grigorov M, Chou CJ. Flavonoids for controlling starch digestion: structural requirements for inhibiting human alpha-amylase. J Med Chem 2008;51:3555-61. [35] Paniagua JA, de la Sacristana AG, Sánchez E, Romero I, Vidal-Puig A,
Berral FJ, et al. A MUFA-rich diet improves postprandial glucose, lipid and GLP-1 responses in insulin-resistant subjects. J Am Coll Nutr 2007;26:434-44.
[36] Tierney AC, Roche HM. The potential role of olive oil-derived MUFA in insulin sensitivity. Mol Nutr Food Res 2007;51:1235-48. [37] Yokoyama J, Someya Y, Yoshihara R, Ishii H. Effects of
high-monounsaturated fatty acid enteral formula versus high-carbohydrate enteral formula on plasma glucose concentration and insulin secretion in healthy individuals and diabetic patients. J Int Med Res 2008;36: 137-46.
6 S.-C. Li et al. / Metabolism Clinical and Experimental xx (2010) xxx–xxx