The Association of Caveolin-1 Genotypes with Oral Cancer Susceptibility in Taiwan
Da-Tian Bau1,4,5*, Ming Hsui Tsai1,2*, Yung-An Tsou1,2*, Chung-Hsing Wang1, Chia-Wen
Tsai1, Shung-Shung Sun1, Chun-Hung Hua1,2, Song-Kun Shyue5 and Ru-Yin Tsai1
Departments of 1Terry Fox Cancer Research Laboratory and 2Otolaryngology, China
Medical University Hospital, Taichung; 4Graduate Institute of Clinical Medical Science,
China Medical University, Taichung, Taiwan. 5Institute of Biomedical Sciences, Academia
Sinica, Taipei, Taiwan.
*These authors contributed equally to this study
Correspondence to: Da-Tian Bau, Ru-Yin Tsai, Terry Fox Cancer Research Laboratory,
China Medical University Hospital, 2 Yuh-Der Road, Taichung, 404 Taiwan. Tel: +886-422052121 Ext. 1523, Fax: +886-422053366
e-mail: [email protected]; [email protected]
Key Words: Cav-1, polymorphism, oral cancer, metastasis.
ABSTRACT
Background.
Caveolin-1, which has been proposed as a candidate tumor suppressor, plays a regulatory role in several signaling pathways. The aim of this study is to evaluate the association between oral cancer susceptibility and Cav-1 genotypes. In this hospital— based case—control study, the association of Cav-1 polymorphisms with oral cancer risk in a Central Taiwanese population was investigated.Methods. Six hundred patients with oral cancer and 620 age- and gender-matched healthy
controls recruited were genotyped and analyzed by PCR-RFLP method.
Results. There were significant differences between oral cancer and control groups in the
distributions of their genotypes (P=1.7*10-18 and 2.6*10-4) and allelic frequencies (P=3.3*10-19 and 9.5*10-6) in the Cav-1 G14713A (rs3807987) and T29107A (rs7804372) polymorphisms, respectively. As for the combined genotype analysis, those who had GG/AT or GG/AA at Cav-1 G14713A/T29107A showed a 0.72-fold (95% confidence interval=0.52-0.99) decreased risk of oral cancer compared to those with GG/TT, while those of any other combinations were of increased risk. The presence of metastasis was also correlated to both Cav-1 G14713A AA and Cav-1 T29107A TT genotypes.
Conclusions. This is the first report providing evidence that Cav-1 being involved in oral
cancer, the A allele of the Cav-1 G14713A is risky, the A allele of the Cav-1 T29107A is protective, and AA/TT on these two polymorphisms may be the most risky combined
genotype for the development of oral cancer and may be novel risky markers for early detection and prediction of distant metastasis.
INTRODUCTION
Oral cancer incidence has increased more than 15% from the mid 1970s until the latest (2007) National Cancer Institute Survey. In 2007, the estimated incidence of oral cancer in the United States was 10.3 cases per 100,000 persons, with a mortality rate of 2.5 per 100,000 persons.1 It is estimated that there will be 36,540 new cases of oral cancer
diagnosed in the United States in 2010 and 7,880 deaths due to this disease.2 Oral cancer is
more common in men than in women and accounts for 3% of new cancer cases in American male.2 In Taiwan, where the oral cancer density is highest worldwide, oral
cancer is a fatal disease accounting for the fourth highest incidence of malignancy in males and the seventh in females.3 The relatively high prevalence of oral cancer in Taiwan is
mainly because there is a high-risk group of 2.5 million people with the habit of smoking, alcohol drinking and betel nut chewing, while the genomic etiology of oral cancer is of great interest but largely unknown.
Caveolae are found primarily in terminally differentiated mesenchymal cells and caveolin proteins (caveolin-1, caveolin-2, and caveolin-3) serve as the structural components of caveolae and also function as scaffolding proteins, which are capable of recruiting numerous signaling molecules to caveolae and regulating their activity. Studies in caveolin-deficient mice have indicated that caveolae and caveolins participate in human disease processes, including diabetes, cancer, cardiovascular disease, atherosclerosis,
pulmonary fibrosis, and a variety of degenerative muscular dystrophies.4 Caveolin-1
(Cav-1), a 22- to 24-kDa protein of 178 amino acids, initially was identified as a major substrate for tyrosine phosphorylation in Rous sarcoma virus-transformed chicken embryonic fibroblasts, suggesting that its role of being a candidate tumor suppressor gene.5
It has been demonstrated that cav-1 is down-regulated in sarcoma, lung carcinoma, and ovarian carcinoma.6-8 However, elevated expression of cav-1 has been associated with the
metastasis of esophageal squamous cell carcinoma and prostate cancer and negatively correlated with patient survival.9, 10 These findings indicate that the role of cav-1 may vary
considerably, depending on the tissue involved.
Up to now, to our knowledge, there was no report about the association of Cav-1 with oral oncology. Thus, the objectives of the current study were to determine the genotypic frequency of six polymorphisms of the Cav-1 gene at C239A (rs1997623), G14713A (rs3807987), G21985A (12672038), T28608A (rs3757733), T29107A (rs7804372), and G32124A (rs3807992). In addition, the correlations of Cav-1 genotypes with clinicopathological data, such as recurrence, metastasis, and survival outcome were also investigated. To the best of our knowledge, this is the first study carried out to evaluate the contribution of Cav-1 genotypes in oral oncology all over the world.
Six hundred and twenty patients diagnosed with oral cancer were recruited at the outpatient clinics of general surgery between 1998-2009 at the China Medical University Hospital, Taichung, Taiwan, Republic of China. The mean age of the oral cancer patients and the controls were 65.5 (SD = 9.7) and 63.5 (SD = 8.5) years, respectively. All patients voluntarily participated, completed a self-administered questionnaire and provided peripheral blood samples. The questionnaire administered to the subjects included questions on history and frequency of alcohol consumption, betel quid chewing and smoking habits. Self-reported alcohol consumption, betel quid chewing and smoking habits were evaluated and classified as categorical variables. Information on these factors was obtained as more then twice a week for years as ‘‘ever’’. The same amounts of non-oral cancer healthy people as controls were selected by matching for age and gender after initial random sampling from the Health Examination Cohort of the hospital. Our study was approved by the Institutional Review Board of the China Medical University Hospital and written-informed consent was obtained from all participants.
Genotyping Conditions
Genomic DNA was prepared from peripheral blood leucocytes using a QIAamp Blood Mini Kit (Blossom, Taipei, Taiwan) and further processed according to our previous papers.11-17 Briefly, the following primers were used for Cav-1 C239A (rs1997623):
5’-GTGTCCGCTTCTGC TATCTG-3’ and 5’-GCCAAGATGCAGAAGGAG TT-3’; for
Cav-1 G14713A (rs3807987): 5’-CCTTCCAGTAAGCAAGCTGT-3’ and
5’-CCTCTCAATCTTGCCATAGT-3’; for Cav-1 G21985A (12672038):
5’-GGTGTCAGCAAGGCTATGCT-3’ and 5’-CCAGACACTCAGAATGTGAC-3’; for
Cav-1 T28608A (rs3757733): 5’-GCTCAACCTCATCTGAGGCA-3’ and
5’-GGCCTATTGTTGAGTGGATG-3’; for Cav-1 T29107A (rs7804372):
5’-GCCTGAATTGCAATCCTGTG-3’ and 5’-ACGGTGTGAACACGGACATT-3’; and
for Cav-1 G32124A (rs3807992): 5’-GGTGTCTTGCAGTTGAATG-3’ and
5’-ACGGAGCTACTCAGTGCCAA-3’. The following cycling conditions were performed: one cycle at 94oC for 5 min; 35 cycles of 94oC for 30 s, 55oC for 30 s, and 72oC for 30 s;
and a final extension at 72oC for 10 min. The PCR products were studied after digestion
with Avr II, Bfa I, Hae III, Tsp509 I, Sau3AI and Nla III, restriction enzymes for Cav-1 C239A (cut from 485 bp C type into 170+315 bp T type), Cav-1 G14713A (cut from 268 bp A type into 66+202 bp G type), Cav-1 G21985A (cut from 251+43 bp A type into 153+98+43 bp G type), Cav-1 T28608A (cut from 298 bp T type into 100+198 bp A type),
Cav-1 T29107A (cut from 336 bp A type into 172+164 bp T type), and Cav-1 G32124A
(cut from 213+142+67 bp A type into 142+118+95+67 bp T type), respectively. Ten percent of the samples both in control and patient groups were analyzed of their genotypes by PCR direct sequencing (Genomics BioSci & Tech Co., Taipei).
Sample Preparation and Western Blotting Analysis of Cav-1
The tissues of tumor sites and distal sites (as the internal control for each patient) from oral cancer patients at early stage collected from 2009 to 2010 were homogenized in RIPA lysis buffer (Upstate, USA, Inc), the homogenates were centrifuged at 10,000 g for 30 min at 4 , and℃ the supernatants were used for Western blotting. The protein concentration of the samples was determined by the BCA method (Pierce, Thermo Fisher Scientific Inc, Waltham, MA) using bovine serum albumin as the standard. Equal amounts of total protein (20 μg) were adjusted to a similar volume with loading buffer (10% SDS, 20% glycerin, 125 mM Tris, 1 mM EDTA, 0.002% bromophenol blue, 10% β-mercaptoethanol), denatured by heating at 95℃ for 10 min, then separated on a 10% SDS-PAGE gel, and transferred to a nitrocellulose membrane (Bio-Rad). The membrane was blocked with 5% non-fat milk and incubated overnight at 4℃ with polyclonal rabbit anti-human Cav-1 (Abcam, Cambridge, UK), then with the corresponding horseradish peroxidase-conjugated goat anti-rabbit IgG secondary antibody (Chemicon, Temecula, CA) for 1 h at room temperature. After reaction with ECL solution (Amersham, Arlington Heights, USA), bound antibody was visualized using a chemiluminescence imaging system (Syngene, Cambrdge, UK). Finally, the blots were incubated at 56℃ for 18 min in stripping buffer (0.0626 mol/L Tris-HCl, pH 6.7, 2% SDS, 0.1 mol/L mercaptoethanol) and re-probed with a monoclonal mouse anti-β-actin antibody (Sigma, Missouri, USA) as the loading control.
The optic density of each specific band was measured using a computer-assisted imaging analysis system (Gene Tools Match software, Syngene, Cambridge, UK). The expression level of Cav-1 in the tumor sites from the patients were normalized by the ratio to each distal control sites and listed in Table IV.
Clinical Outcome Survey
All the patients received regular follow up for 10 years or till the patient expired. Clinical stages were determined according to the criteria used for oral cavity cancer as recommended by AJCC 5th edition of 2002. Histology grading was performed according to
the 1991 world health organization grading scheme. We had grouped the patients according to their genotypes in the clinical outcome analysis. Poor outcome was defined as if the patient had any of the following case: a) expired within one year due to persisted tumor after treatment; b) occurrence of distant metastasis within half year; c) tumor recurrence after finishing treatment within half year.
Statistical Analyses
Only those matches with all genotyping data (case/control =620/620) were selected into final analyzing. To ensure that the controls used were representative of the general population and to exclude the possibility of genotyping error, the deviation of the genotype
frequencies of Cav-1 single nucleotide polymorphisms (SNP) in the control subjects from those expected under the Hardy-Weinberg equilibrium was assessed using the goodness-of-fit test. Pearson’s chi-square test or Fisher’s exact test (when the expected number in any cell was less than five) was used to compare the distribution of the Cav-1 genotypes between cases and controls. Cancer risk associated with the genotypes was estimated as odds ratio (ORs) and 95% confidence intervals (CIs) using unconditional logistic regression. The analysis of survival outcome was performed by the Kaplan-Meier analysis and log rank test for calculating the significance. Any data was recognized as significant when the statistical P-value was less than 0.05.
RESULTS
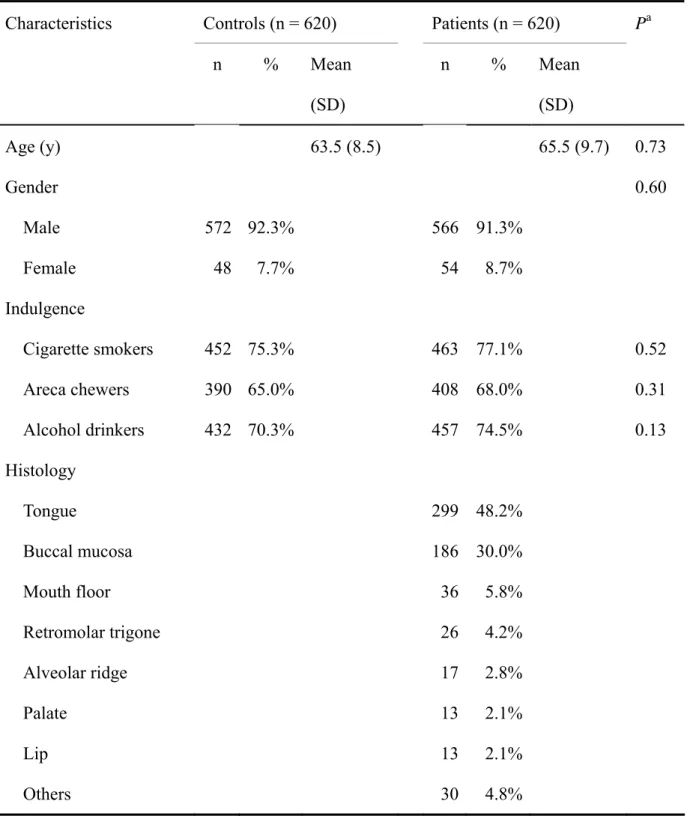
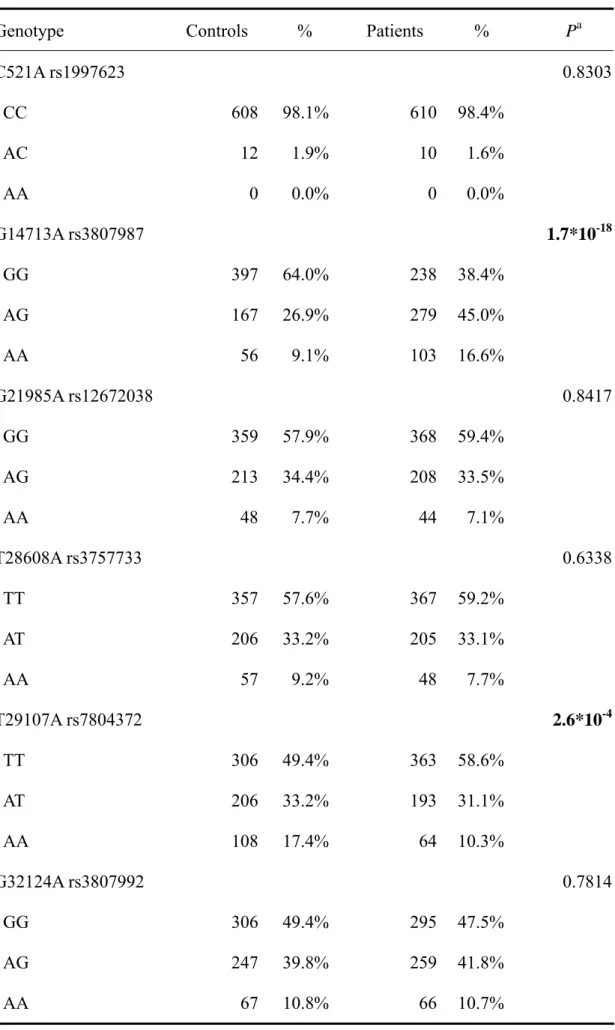
The patient group was composed of 566 men and 54 women between age 25 and 87 years old. There were 100 clinical stage I, 224 stage II, 121 stage III and 175 stage IV oral cancer patients diagnosed by the AJCC 5th edition. The primary tumor sites were tongue, buccal mucosa, mouth floor, retromolar trigone, alveolar ridge, palate, lip, and other site in 299, 186, 36, 26, 17, 13, 13 and 30 patients. There were no significant differences between both groups in their age, sex, and environmental factors (Table I). The frequencies of the genotypes for the Cav-1 C239A, G14713A, G21985A, T28608A, T29107A and G32124A between controls and oral cancer patients is shown in Table II. Genotype distribution of various genetic polymorphisms of Cav-1 G14713A and T29107A were significantly different between oral cancer and control groups (P=1.7*10-18 and 2.6*10-4, respectively), while those for Cav-1 C239A, G21985A, T28608A and G32124A were not significant (P>0.05) (Table II). To sum up, the polymorphism of Cav-1 G14713A and T29107A are associated with oral cancer risk and may be a biomarker for oral cancer detection. The representative PCR-based restriction analyses for the Cav-1 G14713A and T29107A polymorphisms were shown in Figure 1.
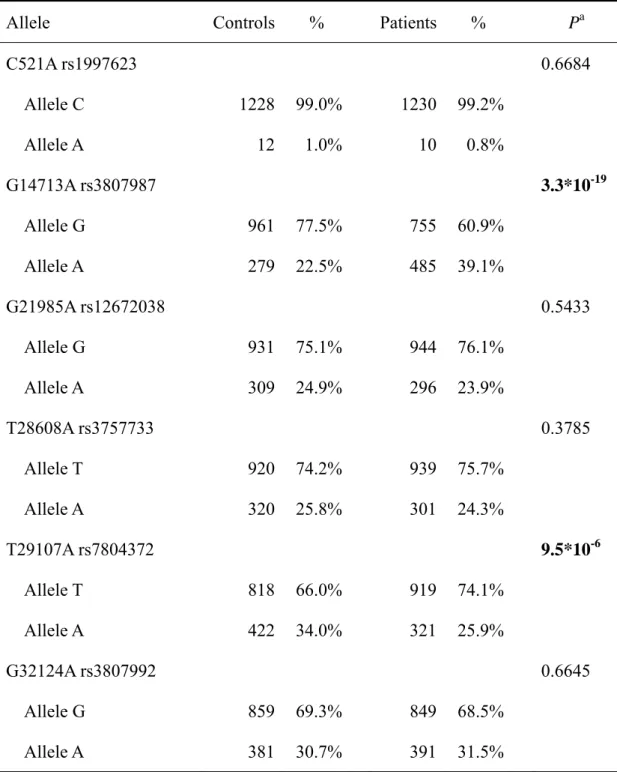
The frequencies of the alleles for the Cav-1 C239A, G14713A, G21985A, T28608A, T29107A and G32124A between controls and oral cancer patients are shown in Table III. The two SNPs of Cav-1 found to be associated with oral cancer in Table II, G14713A and T29107A, are also found to be associated with higher oral cancer susceptibility in their allele frequency
significantly different in controls and oral cancer patients (Table III).
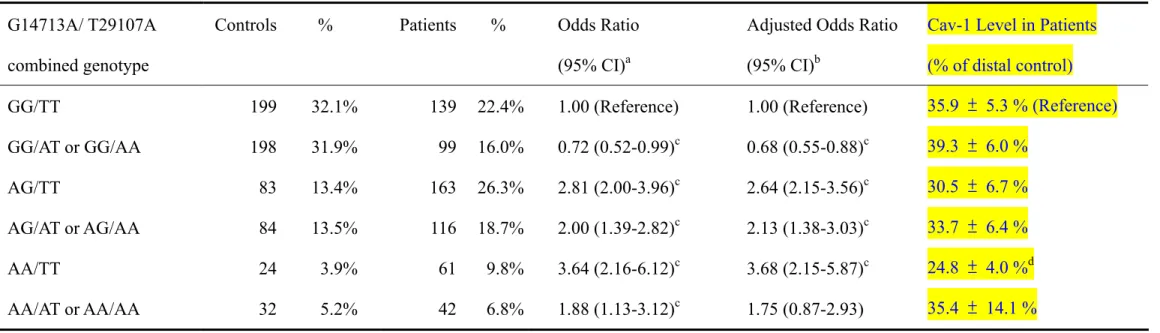
Considering potential interactions between the two significant SNPs of Cav-1 gene and oral cancer susceptibility, the risk of oral cancer related to combined genotype distributions of Cav-1 G14713A and T29107A were further analyzed (Table IV). Compared with GG/TT combined genotype of Cav-1 G14713A and T29107A, the GG/AT or GG/AA group has a 0.72-fold lower risk of oral cancer (95% CI=0.52-0.99). Other combinations of AG/TT, AG/AT or AG/AA, AA/TT, and AA/AT or AA/AA conferred 2.81-fold (95% CI=2.00-3.96), 2.00-fold (95% CI=1.39-2.82), 3.64-fold (95% CI=2.16-6.12) and 1.88-fold (95% CI=1.13-3.12) increased risks compared to the GG/TT combined genotype, respectively (Table IV). The expression levels of Cav-1 in the patients of each combined genotype were also summarized in Table IV. In all patients, the Cav-1 levels were much lower in their tumor sites than the distal control sites. The average protein levels were 35.9%, 39.3%, 30.5%, 33.7%, 24.8% and 35.4% of the expression levels in their distal control sites for GG/TT, GG/AT or GG/AA, AG/TT, AG/AT or AG/AA, AA/TT, and AA/AT or AA/AA groups, respectively. The Cav-1 level of AA/TT group was found to be statistically significant lower than that of GG/TT group (P=0.0012) in the tumor sites. The sample sizes for each genotype group were 10, 8, 10, 9, 5, and 3, respectively (Table IV).
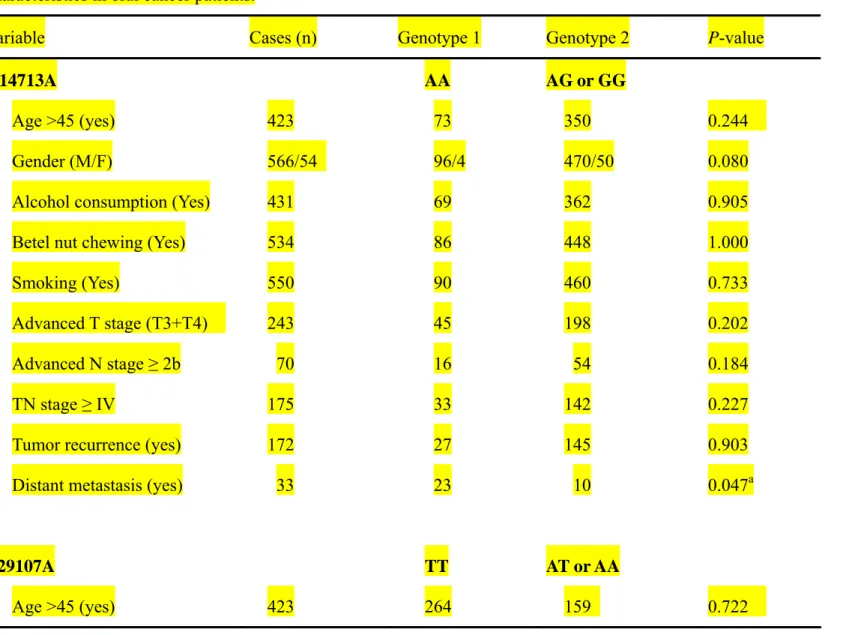
We have also analyzed the correlation between the Cav-1 genotypes and the clinicalpathological and behavioral characteristics of oral cancer patients, including age, gender, alcohol consumption, betel nut chewing, smoking, advanced stages, tumor recurrence and distant
genotype and Cav-1 T29107A TT genotype were correlated to the distant metastasis (P=0.047 and 0.050, respectively) (Table VII). The other clinical parameters such as age, gender, advanced T stage (T3+T4), advanced N stage (≥ 2b), advanced tumor stage (stage IV), tumor recurrence within half year were not significant clinical parameters which may correlate to the Cav-1 G14713A AA or T29107A TT genotypes. The effects of Cav-1 genotypes on 10-year survival rates were also investigated, and it was found that oral cancer patients with G14713A AA and T29107A TT genotypes, but not others, had poor 10-year survival outcomes (P=0.006 and 0.037, respectively) (Figure 2).
DISCUSSION
Although several investigations have shown that Cav-1 plays a critical role in many tumors,6-10 few data are available which consider Cav-1 for genetic predisposition to cancers.18, 19 In 2004, the inactivation of Cav-1 by mutation models or via reducing its expression was found to involve in the pathogenesis of oral cancer.19 In that study, the exon 1 and 3 sequences of Cav-1 were investigated in 74 oral squamous cell carcinomas and 15 oral cancer cell lines, and the expression of Cav-1 was examined. It was reported that only five mutations (1 missense and 4 silent mutations) of Cav-1 were identified in so many cases, and they were all found in exon 3.19 Since sequencing of exonic and promoter regions had not revealed and variants in Cav-1 that might have been directly involved in disease risk, we selected intronic SNPs from the NCBI
to be associated with oral cancer risk.
Our study revealed that the Cav-1 G14713A (rs3807987) and T29107A (rs7804372) polymorphisms were associated with the susceptibility to oral cancer (Table II and III), while the other four polymorphisms were not. Although these genetic variations do not direct result in amino acid coding change, it is plausible to suspect the alternative spicing, intervention, modification, determination or involvement of these SNPs influence the expression level or stability of the Cav-1 protein.
The down-regulated expression of Cav-1 observed in the current study was similar to that reported in studies of mucoepidermoid carcinoma of the salivary glands, sarcoma, lung carcinoma, and ovarian carcinoma.6-8, 20 In addition, it has been suggested that transcriptional silencing through hypermethylation of the Cav-1 promoter may abrogate Cav-1 expression in human cancers.4 In our results, the protein levels of tumor sites of early stage oral cancer patients were much lower than the distal control sites, and this down-regulated Cav-1 expression supported the idea that the differential expression may be caused by Cav-1 genotypes. Furthermore, the combined AA/TT genotype at Cav-1 G14713A/T29107A was found to be of lower Cav-1 expression level than those patients of GG/TT genotype, which correlated well with higher odds ratio of oral cancer susceptibility (Table IV). It is interesting that the Cav-1 expression level may be reactivated in the aggressive esophageal squamous cell carcinoma and prostate cancer.9, 10 The patient sample size with both genotype (620) and protein expression
elucidate the role of Cav-1 in the near future.
There was no correlation among either Cav-1 G14713A or T29107A genotypes with elder age, gender, alcohol consumption, betel nut chewing, smoking, advanced stages, or tumor recurrence. However, the risky AA genotype of G14713A and TT genotype of T29107A were both correlated with higher distant metastasis rates (Table V). These two risky genotypes were also correlated to poorer 10-year survival outcome among the oral cancer patients (Figure 2). Thus, these two SNP sites, Cav-1 G14713A and T29107A, may be novel and potential oral cancer early detection biomarkers for Taiwanese. In the future, studies in other ethics may examine their application as worldwide oral cancer early detection biomarkers.
Environmental factors including cigarette smoking, alcohol consumption and betel quid chewing, were reported to be closely related to oral carcinogenesis. In this study, the joint effects of Cav-1 gene and individual behaviors including smoking, alcohol drinking and betel quid chewing habits were also analyzed, but no significance interaction was observed (Table V). The large enough sample size and similar trends of significant data after age- and behavior-adjustments strengthen the accuracy and reliability of our findings, and the frequencies of Cav-1 polymorphisms variant alleles were similar to those reported in the NCBI website in other Asian population studies. For instance, the minor A allele frequencies of Cav-1 G14713A are 22.5% in our control group, close to those of 16.7% for Beijing and 22.2% for Tokyo populations in NCBI, which strongly suggest no selection bias for the subject’s enrolments in
studies is not so necessary.
Using a candidate gene approach, this present study provided evidence supporting the oral tumorigenic contribution of Cav-1, of which the genotypes of G14713A and T29107A were the most significantly associated. We have also revealed its correlation with clinicopathological and behavioral indexes. Additional functional analyses of the gene and polymorphisms are worthy to explore the mechanisms by which Cav-1 and its regulated proteins affect oral cancer risk. In conclusion, this is the first report to investigate the association between Cav-1 polymorphisms and oral cancer. Our findings suggested that Cav-1 G14713A and T29107A, but not C239A, G21985A, T28608A, or G32124A, were associated with higher susceptibility, higher metastasis, and poorer survival rates of oral cancer. The Cav-1 G14713A AA and Cav-1 T29107A TT genotypes might become potential biomarkers for the oral oncology early detection and prediction.
ACKNOWLEDGEMENTS
We are grateful to Wen-Shin Chang, Hsiu-Min Hsieh and the Tissue Bank in China Medical University Hospital for their technical assistance. This study was supported by research grants from the China Medical University and Hospital (DMR-99-049, DOH99-TD-C-111-005), and the National Science Council (NSC 98-2320-B-039-010-MY3).
REFERENCES
1. Altekruse SF, Kosary CL, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2007. Bethesda, Md. National Cancer Institute. 2010.
2. American Cancer Society. Cancer Facts and Figures 2010. Atlanta, Ga. American Cancer
Society. 2010.
3. Department of Health, Taiwan. Cancer registration system annual report. Taiwan,
Department of Health. 2009.
4. Cohen AW, Hnasko R, Schubert W, Lisanti MP. Role of caveolae and caveolins in health and disease. Physiol Rev. 2004;84:1341-1379.
5. Glenney JR, Jr. Tyrosine phosphorylation of a 22-kDa protein is correlated with transformation by Rous sarcoma virus. J Biol Chem. 1989;264:20163-20166.
6. Belanger MM, Roussel E, Couet J. Caveolin-1 is down-regulated in human lung carcinoma and acts as a candidate tumor suppressor gene. Chest. 2004;125:106S.
7. Wiechen K, Diatchenko L, Agoulnik A, et al. Caveolin-1 is down-regulated in human ovarian carcinoma and acts as a candidate tumor suppressor gene. Am J Pathol. 2001;159:1635-1643.
8. Wiechen K, Sers C, Agoulnik A, et al. Down-regulation of caveolin-1, a candidate tumor suppressor gene, in sarcomas. Am J Pathol. 2001;158:833-839.
9. Yang G, Truong LD, Wheeler TM, Thompson TC. Caveolin-1 expression in clinically confined human prostate cancer: a novel prognostic marker. Cancer Res.
1999;59:5719-5723.
10. Kato K, Hida Y, Miyamoto M, et al. Overexpression of caveolin-1 in esophageal squamous cell carcinoma correlates with lymph node metastasis and pathologic stage.
Cancer. 2002;94:929-933.
11. Bau DT, Tseng HC, Wang CH, et al. Oral cancer and genetic polymorphism of DNA double strand break gene Ku70 in Taiwan. Oral Oncol. 2008;44:1047-1051.
12. Chang CH, Wang RF, Tsai RY, et al. Significant association of XPD codon 312 single nucleotide polymorphism with bladder cancer susceptibility in Taiwan. Anticancer Res. 2009;29:3903-3907.
13. Chiu CF, Tsai MH, Tseng HC, et al. A novel single nucleotide polymorphism in ERCC6 gene is associated with oral cancer susceptibility in Taiwanese patients. Oral Oncol. 2008;44:582-586.
14. Chiu CF, Tsai MH, Tseng HC, et al. A novel single nucleotide polymorphism in XRCC4 gene is associated with oral cancer susceptibility in Taiwanese patients. Oral Oncol. 2008;44:898-902.
15. Chiu CF, Wang CH, Wang CL, et al. A novel single nucleotide polymorphism in XRCC4 gene is associated with gastric cancer susceptibility in Taiwan. Ann Surg Oncol. 2008;15:514-518.
17. Wang HC, Chiu CF, Tsai RY, et al. Association of genetic polymorphisms of EXO1 gene with risk of breast cancer in Taiwan. Anticancer Res. 2009;29:3897-3901.
18. Conde MC, Ramirez-Lorca R, Lopez-Jamar JM, et al. Genetic analysis of caveolin-1 and eNOS genes in colorectal cancer. Oncol Rep. 2006;16:353-359.
19. Han SE, Park KH, Lee G, Huh YJ, Min BM. Mutation and aberrant expression of Caveolin-1 in human oral squamous cell carcinomas and oral cancer cell lines. Int J
Oncol. 2004;24:435-440.
20. Shi L, Chen XM, Wang L, Zhang L, Chen Z. Expression of caveolin-1 in mucoepidermoid carcinoma of the salivary glands: correlation with vascular endothelial growth factor, microvessel density, and clinical outcome. Cancer. 2007;109:1523-1531.
FIGURE LEGENDS
Fig 1. Genotyping analysis of the T29107A (A) and G14713A (B) polymorphisms of Cav-1 by PCR-RFLP (A and B) and double-checked by direct DNA sequencing (C-H). (A) M: 100 bp DNA size marker, A/A: indivisible homozygote, A/T: heterozygote, and T/T: divisible homozygote. (B) M: 100 bp DNA size marker, A/A: indivisible homozygote, A/G: heterozygote, and G/G: divisible homozygote. (C) TT genotype of T29107A. (D) AA genotype of T29107A. (E) AT genotype of T29107A. (F) AA genotype of G14713A. (G) GG genotype of G14713A. (H) AG genotype of G14713A.
Fig 2. Survival curves of oral cancer patients after diagnosis stratified by genotypes of Cav-1 T29107A (A) and G14713A (B). Statistical analysis was performed by the log-rank test.
Table I. Characteristics of oral cancer patients and controls
Characteristics Controls (n = 620) Patients (n = 620) Pa
n % Mean (SD) n % Mean (SD) Age (y) 63.5 (8.5) 65.5 (9.7) 0.73 Gender 0.60 Male 572 92.3% 566 91.3% Female 48 7.7% 54 8.7% Indulgence Cigarette smokers 452 75.3% 463 77.1% 0.52 Areca chewers 390 65.0% 408 68.0% 0.31 Alcohol drinkers 432 70.3% 457 74.5% 0.13 Histology Tongue 299 48.2% Buccal mucosa 186 30.0% Mouth floor 36 5.8% Retromolar trigone 26 4.2% Alveolar ridge 17 2.8% Palate 13 2.1% Lip 13 2.1% Others 30 4.8% a
Table II. Distribution of Cav-1 genotypes among oral cancer patients and controls
Genotype Controls % Patients % Pa
C521A rs1997623 0.8303 CC 608 98.1% 610 98.4% AC 12 1.9% 10 1.6% AA 0 0.0% 0 0.0% G14713A rs3807987 1.7*10-18 GG 397 64.0% 238 38.4% AG 167 26.9% 279 45.0% AA 56 9.1% 103 16.6% G21985A rs12672038 0.8417 GG 359 57.9% 368 59.4% AG 213 34.4% 208 33.5% AA 48 7.7% 44 7.1% T28608A rs3757733 0.6338 TT 357 57.6% 367 59.2% AT 206 33.2% 205 33.1% AA 57 9.2% 48 7.7% T29107A rs7804372 2.6*10-4 TT 306 49.4% 363 58.6% AT 206 33.2% 193 31.1% AA 108 17.4% 64 10.3% G32124A rs3807992 0.7814 GG 306 49.4% 295 47.5% AG 247 39.8% 259 41.8% AA 67 10.8% 66 10.7%
Table III. Distribution of Cav-1 alleles among oral cancer patients and controls
Allele Controls % Patients % Pa
C521A rs1997623 0.6684 Allele C 1228 99.0% 1230 99.2% Allele A 12 1.0% 10 0.8% G14713A rs3807987 3.3*10-19 Allele G 961 77.5% 755 60.9% Allele A 279 22.5% 485 39.1% G21985A rs12672038 0.5433 Allele G 931 75.1% 944 76.1% Allele A 309 24.9% 296 23.9% T28608A rs3757733 0.3785 Allele T 920 74.2% 939 75.7% Allele A 320 25.8% 301 24.3% T29107A rs7804372 9.5*10-6 Allele T 818 66.0% 919 74.1% Allele A 422 34.0% 321 25.9% G32124A rs3807992 0.6645 Allele G 859 69.3% 849 68.5% Allele A 381 30.7% 391 31.5% a
Table IV Distribution of Cav-1 G14713A/T29107A combined genotypes among oral cancer patients and controls G14713A/ T29107A
combined genotype
Controls % Patients % Odds Ratio
(95% CI)a
Adjusted Odds Ratio (95% CI)b
Cav-1 Level in Patients (% of distal control)
GG/TT 199 32.1% 139 22.4% 1.00 (Reference) 1.00 (Reference) 35.9 ± 5.3 % (Reference)
GG/AT or GG/AA 198 31.9% 99 16.0% 0.72 (0.52-0.99)c 0.68 (0.55-0.88)c 39.3 ± 6.0 %
AG/TT 83 13.4% 163 26.3% 2.81 (2.00-3.96)c 2.64 (2.15-3.56)c 30.5 ± 6.7 %
AG/AT or AG/AA 84 13.5% 116 18.7% 2.00 (1.39-2.82)c 2.13 (1.38-3.03)c 33.7 ± 6.4 %
AA/TT 24 3.9% 61 9.8% 3.64 (2.16-6.12)c 3.68 (2.15-5.87)c 24.8 ± 4.0 %d
AA/AT or AA/AA 32 5.2% 42 6.8% 1.88 (1.13-3.12)c 1.75 (0.87-2.93) 35.4 ± 14.1 %
a 95% CI, 95% confidence interval.
b 95% CI, 95% confidence interval, and date were calculated by unconditioned logistic regression and adjusted for age, gender, smoking, alcohol drinking and betel quid chewing behaviors.
Table V. Univariate analysis of Cav-1 G14713A and T29107A genotype with clinicopathological and behavioral characteristics in oral cancer patients.
Variable Cases (n) Genotype 1 Genotype 2 P-value
G14713A AA AG or GG
Age >45 (yes) 423 73 350 0.244
Gender (M/F) 566/54 96/4 470/50 0.080
Alcohol consumption (Yes) 431 69 362 0.905
Betel nut chewing (Yes) 534 86 448 1.000
Smoking (Yes) 550 90 460 0.733
Advanced T stage (T3+T4) 243 45 198 0.202
Advanced N stage ≥ 2b 70 16 54 0.184
TN stage ≥ IV 175 33 142 0.227
Tumor recurrence (yes) 172 27 145 0.903
Distant metastasis (yes) 33 23 10 0.047a
T29107A TT AT or AA
Gender (M/F) 566/54 361/29 205/25 0.184
Alcohol consumption (Yes) 431 278 153 0.240
Betel nut chewing (Yes) 534 341 193 0.231
Smoking (Yes) 550 347 203 0.318
Advanced T stage (T3+T4) 243 145 98 0.202
Advanced N stage ≥ 2b 70 40 30 0.296
TN stage ≥ IV 175 109 66 0.853
Tumor recurrence (yes) 172 110 62 0.781
Distant metastasis (yes) 33 28 5 0.009a