Kaohsiung J Med Sci December 2004 • Vol 20 • No 12 W.M. Li, C.H. Huang, C.M. Su, et al
612
E
XTRA
-
ADRENAL
P
HEOCHROMOCYTOMA
P
RESENTING
WITH
L
IFE
-
THREATENING
V
ENTRICULAR
T
ACHYCARDIA
:
A C
ASE
R
EPORT
Wei-Ming Li, Chun-Hsiung Huang, Chin-Ming Su, Chee-Yin Chai,1
Wen-Jeng Wu, and Yii-Her Chou
Departments of Urology and 1Pathology, Kaohsiung Medical
University Hospital, Kaohsiung, Taiwan.
Extra-adrenal pheochromocytoma develops in paraganglion chromaffin cells of the sympathetic nervous system. It probably represents at least 15% of adult and 30% of childhood pheochromocytomas. Although electrocardiographic abnormalities occur in up to 75% of patients with pheochromocytoma, there are only three other reported cases of pheochromocytoma that initially presented with ventricular tachycardia. In this report, we describe a 64-year-old woman with an abdominal para-aortic extra-adrenal pheochromocytoma who presented with pulseless ventricular tachycardia and needed electrical defibrillation initially to keep vital signs. The 24-hour urine vanillylmandelic acid was 35.8 mg. Computerized tomography showed a left retroperitoneal mass. The postoperative course was uneventful. Pheochromocytoma was proved by histologic study.
Key Words: pheochromocytoma, ventricular tachycardia, arrhythmia (Kaohsiung J Med Sci 2004;20:612–5)
Received: June 17, 2004 Accepted: September 15, 2004 Address correspondence and reprint requests to: Dr. Chun-Hsiung Huang, Department of Urology, Kaohsiung Medical University, 100 Shih-Chuan 1st Road, Kaohsiung 807, Taiwan.
E-mail: [email protected]
© 2004 Elsevier. All rights reserved.
Extra-adrenal pheochromocytoma develops in paragan-glion chromaffin cells of the sympathetic nervous system. It probably represents at least 15% of adult and 30% of childhood pheochromocytomas [1]. It most commonly occurs in the second or third decade of life [2]. Patients with extra-adrenal pheochromocytoma commonly present with the classic triad of headache, palpitation, and sweating [2]. Cardiac arrhythmias are common with pheochromocyto-ma. Nevertheless, ventricular tachycardia has been reported in only three cases [3]. We report a rare case of pulseless ventricular tachycardia caused by extra-adrenal pheo-chromocytoma in an adult.
C
ASEP
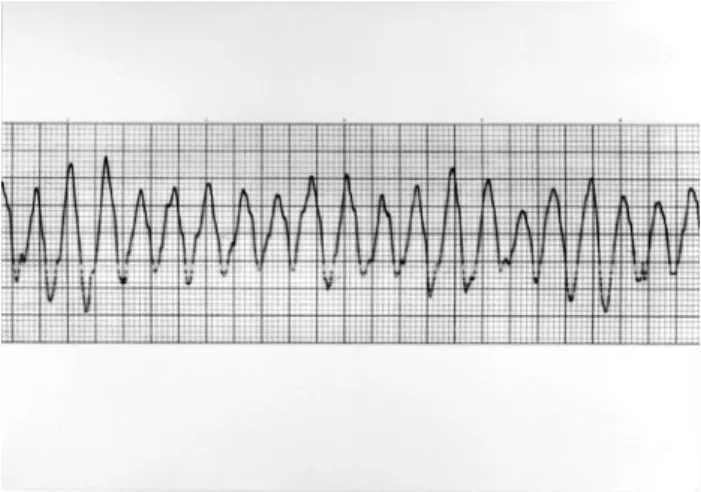
RESENTATIONA 64-year-old female had had hypertension under drug control (amlodipine 2.5 mg/day and bisoprolol 5 mg/day) for 2 years. She was sent to our emergency department due to cold sweating, headache, palpitation, and hypertension (245/119 mmHg). She lost consciousness and had pulse-less ventricular tachycardia (Figure 1) after arrival. After electrical defibrillation (200 J), she recovered consciousness. Electrocardiography (ECG) showed sinus tachycardia and inverted T waves. Blood pressure was 237/160 mmHg. Due to unstable hemodynamics, she was admitted and received advanced survey.
A 24-hour Holter monitor revealed sinus rhythm with intermittent junctional escape rhythms. Heart ultrasono-graphy showed mild tricuspid regurgitation, right ven-tricular dilation, and septal hypertrophy. The patient also underwent coronary angiographic evaluation, which was normal. The 24-hour urine vanillylmandelic acid was 35.8 mg (normal, 2–9 mg/24 hours). Other laboratory studies revealed: normal thyroid function; serum ionized calcium,
Ventricular tachycardia in extra-adrenal pheochromocytoma
613
Kaohsiung J Med Sci December 2004 • Vol 20 • No 12
4.9 mg/dL; normal serum electrolyte; blood urea nitrogen, 27 mg/dL; and creatinine, 1.2 mg/dL. Computerized tomography showed a left retroperitoneal mass which compressed the left ureter, resulting in mild obstructive uropathy (Figure 2). 131I-metaiodobenzylguanidine scan
revealed abnormal tracer uptake in the left abdomen. After admission, blood pressure and arrhythmia were well con-trolled with labetalol, a non-selective α- and β-adrenergic blocker. Preoperatively, the patient was taking 200 mg labetalol three times daily, titrated to 200 mg twice daily according to blood pressure when surgery was arranged.
The tumor was totally excised through a para-midline transperitoneal incision. An operative ECG-blood pres-sure monitor taped several hypertensive and hypoten-sive episodes without ventricular rhythm disturbance. Histopathologic examination of the tumor confirmed pheochromocytoma (weight, 32 g; 62 × 39 × 28 mm) (Fig-ure 3). Postoperatively, blood press(Fig-ure remained stable and within the normal range. She was discharged on postoperative day 14.
D
ISCUSSIONElectrocardiographic abnormalities are common and occur in up to 75% of patients with pheochromocytoma, including sinus tachycardia, premature ventricular complex, T-wave inversion, premature atrial complex, ST elevation, parox-ysmal supraventricular tachycardia, atrial fibrillation, prolonged QT interval, painless myocardial infarction, and left ventricular hypertrophy [3]. However, pheochromo-cytoma that initially presents with ventricular tachy-cardia is rare and only three cases have been reported in the literature [4]. We report another case of extra-adrenal pheochromocytoma that presented with pulseless ven-tricular tachycardia and needed electrical defibrillation.
Cardiac arrhythmias are probably due to the sudden release of catecholamines. Ceremuzynski et al found increased plasma catecholamine concentrations in anes-thetized dogs during acute myocardial ischemia and a relationship between blood catecholamine concentration and the severity of ventricular arrhythmias [5]. Daugherty et al showed that increases in plasma catecholamine concentrations during coronary artery ligation in pentobarbitone-anesthetized rats were prevented by either acute adrenalectomy or chronic adrenal demedullation, but these procedures did not protect against ventricular arrhythmias [6]. Thus, plasma catecholamines are not obligatory mediators of arrhythmogenesis, but these results do not exclude the possibility that catecholamines released locally to the ischemic myocardium may be important arrhythmogenic mediators.
Other neurohumoral agents may be associated with cardiac arrhythmia. Neuropeptide Y levels are increased in the plasma and tumors of patients with pheochromocytoma. Neuropeptide Y has potent direct and indirect cardio-vascular effects [7]. The presence and degree of circulatory disturbance, in particular tachycardia and left heart failure, are strongly related to increased plasma concentrations of neuropeptide Y in coronary care patients [8].
Figure 1. Ventricular tachycardia on electrocardiography.
Figure 2. A left retroperitoneal mass (arrow) on computerized
Kaohsiung J Med Sci December 2004 • Vol 20 • No 12 W.M. Li, C.H. Huang, C.M. Su, et al
614
In addition, cardiac abnormalities occur commonly in patients with pheochromocytomas, including myocarditis, acute myocardial infarction, cardiac arrhythmias, and cardiomyopathy. Catecholamines released from pheo-chromocytomas cause myocardial necrosis, focal myofibrillar degeneration, and subsequent fibrous scar formation [9,10].
The preoperative use of phenoxybenzamine, a non-selective α-adrenergic blocker, has a mostly theoretical pharmacologic basis. The β-blocker propranolol is used when tachycardia or catecholamine-induced arrhythmias are present, and should only be started after α-blockade has been established to avoid life-threatening hypertension. Labetalol has the advantage of being a β-blocker with additional α-adrenergic blocking properties. However, it may interfere with diagnostic studies, restricting its use to patients in whom the diagnosis of pheochromocytoma is already firm [1,7]. The optimal length of preoperative adrenergic blockade is variable and primarily depends on the time required for the patient to manifest hemodynamic stability. In our case, the patient was placed on labetalol 2 weeks preoperatively to control hypertension and tachycardia.
Pheochromocytoma should be kept in mind even in an elderly hypertensive patient. In our opinion, while the di-agnosis of extra-adrenal pheochromocytoma is established by biochemical examination and image studies, it is best to use continuous ECG monitoring. Although life-threatening cardiac arrhythmias are rare in extra-adrenal pheo-chromocytoma, cardiopulmonary resuscitative facilities and
Figure 3. Microscopic findings of the retroperitoneal mass: (A) tumor cells are arranged in a nest bounded by delicate fibrovascular stroma, the
so-called Zellballen (hematoxylin & eosin, × 40); (B) the nuclei are round or oval with finely granular cytoplasm, and there is hyperchromasia with occasional nucleoli (hematoxylin & eosin, × 400).
medications must be easily available to prevent morbidity and cardiac arrest.
R
EFERENCES1. Whalen RK, Althausen AF, Daniels GH. Extra-adrenal pheochromocytoma. J Urol 1992;147:1–10.
2. Goldfarb DA, Novick AC, Bravo EL, et al. Experience with extra-adrenal pheochromocytoma. J Urol 1989;142:931–6. 3. Michaels RD, Hays JH, O’Brian JT, et al. Pheochromocytoma
associated ventricular tachycardia blocked with atenolol.
J Endocrinol Invest 1990;13:943–7.
4. Petit T, de Lagausie P, Maintenant J, et al. Thoracic pheo-chromocytoma revealed by ventricular tachycardia. Eur J
Pediatr Surg 2000;10:142–4.
5. Ceremuzynski L, Staszewska-Barczak J, Herbaczynska-Cedro K. Cardiac rhythm disturbances and the release of catechol-amines after acute coronary occlusion in dogs. Cardiovasc Res 1969;3:190–7.
6. Daugherty A, Frayn KN, Redfern WS, et al. The role of catecholamines in the production of ischaemia-induced ventricular arrhythmias in the rat in vivo and in vitro. Br J
Pharmacol 1986;87:265–77.
7. Bravo EL, Tagle R. Pheochromocytoma: state-of-the-art and future prospects. Endocr Rev 2003;24:539–53.
8. Hulting J, Sollevi A, Ullman B, et al. Plasma neuropeptide Y on admission to a coronary care unit: raised levels in patients with left heart failure. Cardiovasc Res 1990;24:102–8.
9. Van Vliet PD, Burchell HB, Titus JL. Focal myocarditis associated with pheochromocytoma. N Engl J Med 1966;274: 1102–8.
10. Bravo EL. Pheochromocytoma: new concepts and future trends.
Ventricular tachycardia in extra-adrenal pheochromocytoma
615