Title page
Klebsiella pneumoniae Liver Abscess: A New Invasive Syndrome
L. Kristopher Siu, Kuo-Ming Yeh, Jung-Chung Lin, Chang-Phone Fung, Feng-Yee Chang
Institute of Infectious Diseases and Vaccinology, National Health Research Institutes, Miaoli, Taiwan, ROC (L. K. Siu Ph.D.); Graduate Institute of Basic Medical Science, China Medical University, Taichung, Taiwan, ROC (L. K. Siu Ph.D.); Division of Infectious Diseases and Tropical Medicine, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, ROC (K.-M. Yeh MD, J.-C. Lin MD, F.-Y. Chang MD); Taiwan Centers for Disease control, Taipei, Taiwan, ROC (F.-Y. Chang MD); Section of Infectious Diseases, Department of Medicine, Taipei Veterans General Hospital and National Yang-Ming University, Taipei, ROC (C.-P. Fung MD).
Correspondence to:
Dr Feng-Yee Chang, Division of Infectious Diseases and Tropical Medicine, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, 325. Sec. 2, Cheng-Kung Rd., Taipei, 114, Taiwan Republic of China
[email protected] 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Word count of summary: 145 words Word count of text: 2369 words Reference count: 67
File name: Klebsiella-Chang-Revised Date: 2012/4/16 1 2 3 4 5 6 7
Summary
Klebsiella pneumoniae has been well described as a human pathogen in nosocomial
infections. Community-acquired infections have been mostly reported for pneumonia and urinary tract infection. However, a distinct invasive syndrome of liver abscess has been frequently reported in Asia, and this syndrome is emerging as a global disease. We have reviewed large patient series from Asia and Western countries and systematically summarized the clinical presentation and therapeutic management as well the microbiological features of this invasive disease. Specific characteristics of the host and bacteria including diabetes and specific capsules may predispose patients to the development of liver abscess and metastatic complications of bacteremia, meningitis, endophthalmitis, and necrotizing fasciitis. Appropriate antimicrobial therapy combined with percutaneous drainage of liver abscess has resulted in a low mortality rate. In addition to clinical assessment, rapid detection of this hypervirulent strain permits earlier diagnosis, thus minimizing complications and improving outcome. 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Introduction
Klebsiella pneumoniae is an established human pathogen. However, a distinct invasive
syndrome has appeared in Southeast Asia over the past two decades. Liver abscess occurring in patients infected with K. pneumoniae was first described in the 1980s in anecdotal reports and case series, all emanating from Taiwan. Extrahepatic complications resulting from bacteremic dissemination including endophthalmitis,3 meningitis,4 necrotizing fasciitis,5 and other illnesses6 were also manifested. The invasive syndrome was subsequently reported throughout Southeast Asia, including Singapore, Hong Kong, Korea, and Vietnam. Notably, few cases were reported from China.15 A meta-analysis revealed that the prevalence of K.
pneumoniae infection has been increasing since the late 1980s, and it is currently the
predominant etiological cause of liver abscess in Korea.11
The reasons for the predominance of this syndrome in individuals of Asian descent remain unclear. In 2002, Ko et al. found that the major factor was the microbe itself. K. pneumoniae isolated from specimens of patients with the invasive syndrome had distinct phenotypic and genotypic features including unusual virulence in a mouse model compared to that of K.
pneumoniae isolated from bacteremic patients outside Asia.16 Moreover, a genotype strongly associated with this highly invasive disease is widespread. 17-19
In the past two decades, this syndrome has been described in anecdotal reports from North America. Most patients with invasive Klebsiella syndrome outside Asia were of Asian 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
descent. However, cases occurring in patients of non-Asian descent are now being reported, and the isolated Klebsiella strains have been classified as serotypes K1 and K2.
In this systematic review,, we assess current studies on the pathophysiology, epidemiology, clinical manifestations, diagnosis, and treatment of K. pneumoniae liver abscess. We aim to provide comprehensive knowledge about this emerging disease.
Definition of the Invasive Syndrome
Through an extensive reference review, we propose a case definition for “invasive Klebsiella syndrome” to more clearly identify other cases occurring elsewhere. As knowledge about this distinct aspect of Klebsiella accumulates, this definition may be modified.
Clinical Definition:
(1) Invasive Klebsiella syndrome-Definite: K. pneumoniae liver abscess with extrahepatic complications, especially central nervous system (CNS) involvement, necrotizing fasciitis, or endophthalmitis.
(2) Invasive Klebsiella syndrome-Probable: K. pneumoniae liver abscess as the sole presenting clinical manifestation.
Microbiological Definition:
(1) K. pneumoniae liver abscess caused by the K1/K2 serotype. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
formation of a viscous string > 0.5 cm in length stretched by the inoculation loop (Fig. 1).
The invasive nature of certain K. pneumoniae strains includes a hypermucoviscous phenotype associated with serotypes K1/K2 and the regulator of mucoid phenotype A gene (rmpA). A loss or reduction of capsule synthesis will simply reduce the virulence due to the loss of the anti-phagocytic effect against macrophages and neutrophils.22,23 Almost all severe cases with bacteremia, liver abscess, and extrahepatic infections are due exclusively to K1/K2 K.
pneumoniae, but not all K1/K2 serotypes of K. pneumoniae result in liver abscess with
extrahepatic infection. Fulfillment of both the clinical and microbiological definitions of the invasive syndrome portends a poor prognosis and warrants immediate and more aggressive therapy.
Epidemiology and Risk Factors
Thirty-eight patients were diagnosed with K. pneumoniae liver abscess in two case series in the US. Korea has the second highest prevalence of K. pneumoniae liver abscess, trailing only Taiwan; in total, 321 patients were identified in two national studies. We reviewed the demographic and clinical characters of 512 cases from four large-scale studies in Taiwan (Table 1).25-28 Virtually all cases have been community-acquired.
The patients in the US were more ethnically diverse, with 50% of patients being non-Asian (Table 1). Diabetes mellitus appears to be a risk factor for the invasive Klebsiella syndrome 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
(Table 1), and it is significantly associated with poor visual outcome in patients with endophthalmitis.34 Strict glycemic control may prevent the development of metastatic complications caused by serotype K1/K2 K. pneumoniae.35 A liver abscess is usually a solitary abscess located in the right lobe (Table 1). The global mortality rate was 5.3% (43/813) (Table 1).
Different studies have showed that tThe source of invasive K. pneumoniae appears to be the gastrointestinal tract.36 (CP Fung et al., Fung C-P, Lin Y-T, Lin J-C, Chen T-L, Yeh
K-M, Chang F-Y, et al. Klebsiella pneumoniae in gastrointestinal tract and pyogenic liver abscess. Emerg Infect Dis [serial on the Internet]. 2012 Aug [date cited]. http://dx.doi.org/10.3201/eid1808.111053). Fung et al., has observed that K. pneumoniae strains isolated from liver abscess patients and from healthy carriers had an identical PFGE profile with the same virulence-associated genes and similar LD50 values. This observation indicates that the healthy adults carried the virulent strains in
their intestines. Liver abscess may occur when bacterial translocation across the intestinal epithelium occurs. A previous animal study has provided evidence that K. pneumoniae strains had the ability to cross the intestinal barrier and cause liver abscess (Tu YC et al., Genetic requirements for Klebsiella pneumoniae-induced liver abscess in an oral infection model.
Infect Immun. 2009;77:2657-71.) Fecal-oral transmission, gastrointestinal colonization, and environmental exposure are possible routes of acquisition. Liver abscess may develop due to 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
the leakage of K. pneumoniae colonizing the bowel that subsequently spreads to the liver via the portal circulation.
Seroepidemiology on fecal carriage of K. pneumoniae in healthy Chinese and overseas Chinese adults in Asian countries has shown carriage rate of K. pneumoniae in healthy adults was 75% with a high prevalence (23 %) of serotype K1/K2 isolates among typeable strains in Taiwan (Lin YT, Siu LK, Lin JC, Chen TL, Tseng CP, Yeh KM, Seroepidemiology of
Klebsiella pneumoniae colonizing the intestinal tract of healthy Chinese and overseas
Chinese adults in Asian countries. BMC Microbiol. 2012;12:13). In European studies, Carriage rate of K. pneumoniae have differed considerably. The rate of detection in fecal samples from healthy persons ranged from 19.4% to 38% (Thom BT. Klebsiella in faeces.
Lancet. 1970;2(7681):1033; Smith GW, Blackwell CC, Nuki G. Faecal flora in
spondyloarthropathy. Br J Rheumatol. 1997;36:850-4). Thus, The high carriage of virulent K.
pneumoniae strains in Asian descent is probably the reason why there are high prevalence of K. pneumoniae liver abscess.
Virulence Factors of Klebsiella
Several virulence factors have been described in K. pneumoniae: the capsular serotype, mucoviscosity-associated gene A (magA), rmpA, and aerobactin (Table 2).37 Klebsiella strains expressing capsular type K1 or K2 antigen are particularly virulent. These serotypes have a high prevalence of resistance to phagocytosis and intracellular killing by neutrophils and 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
serum killing by bactericidal complements. Mutants without a capsule are highly susceptible to phagocytosis and serum killing and exhibit reduced virulence in mice. Although serotype K1/K2 Klebsiella isolated from patients with liver abscess usually exhibit hypermucoviscosity, hypermucoviscosity is not confined to only these two serotypes only.17 This extreme mucoid phenotype may reflect the degree of capsular polysaccharide expression, which is related to resistance to phagocytosis. In animal models, the resistance of K1/K2 strains to intracellular killing by neutrophils and serum may promote inflammation and dissemination.
MagA has been described as the causative gene for K. pneumoniae liver abscess and septic
metastatic complications.40 Similarly to mutants lacking a capsule, the magA mutant does not exhibit an extreme mucoid phenotype (Fig. 1). It is now clear that magA functions as a polymerase involved in capsule synthesis, and this function is only restricted to the capsular gene cluster of serotype K1. Silencing of genes surrounding magA (Fig. 1) in the same cluster of genes required for capsular polysaccharide synthesis resulted in the same phenomenon of loss of hypermucoviscosity and virulence.23
RmpA has been proposed as a virulent factor in addition to magA and capsular serotypes
K1/K2 in 2006.44 rmpA is not an independent factor contributing to liver abscess but facilitates the expression of the virulent complex as mentioned above for capsule synthesis.7 One report revealed that all the K. pneumoniae strains causing liver abscess and abscess at 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
other sites are rmpA-positive.44 rmpA has been confirmed as a major gene that regulates capsular polysaccharide synthesis. Ablation of this gene results in the loss or thinning of the
K. pneumoniae capsule and weak positivity to the anti-serum antibody due to extremely low
capsule synthesis. One significant phenotype of rmpA-negative strains is the loss of hypermucovisity or a negative string test result as defined above (Fig. 1). Aerobactin genes in combination with rmpA play an important role in the virulence of non-serotype K1/K2 isolates. Mucoid phenotype frequently concomitant with aerobactin production (Yu VL et., al., EID 2007. 13:986-993). Since aerobactin (siderophore) is involving in iron acquisition, the growth of bacteria in host is limited on the supplying of iron if lacking of siderophore. Thus, bacteria produce siderophore were more virulence. The contribution of aerobactin in virulence has been confirmed in several studies (Fung CP et al., EID. 2012 Aug [date cited]. http://dx.doi.org/10.3201/eid1808.111053; Yu VL EID 2007. 13:986-993; and Yeh KM et al., JCM 2007. 45(2): 466-71) Non-serotype K1/K2 isolates that express rmpA and aerobactin genes exhibit similar virulence as serotype K1/K2 isolates from patients with liver abscess.45
Clinical Manifestations and Diagnosis
The most common presenting clinical manifestations of K. pneumoniae liver abscess are fever, chills, and abdominal pain. 25-28 Most patients had fever and chills, about two-third of them abdominal pain, and one-forth nausea/vomiting. 25-28 However, these symptoms are not 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
pathognomonic for K. pneumoniae invasive syndrome. Leukocytosis, thrombocytopenia, increased level of C-reactive protein, glucose and abnormal results of liver function tests were common.27
Clinical clue: Clinical diagnosis: In Asian patients or patients with diabetes who present with
Klebsiella pneumoniae bacteremia, endophthalmitis, meningitis, or other extrahepatic infections, a search for an occult liver abscess is indicated. CT scans are more sensitive than sonography in diagnosing liver abscess. 46
Microbiological clue: Microbiological diagnosis: A Klebsiella isolate isolated from blood or liver abscess with the hypermucoviscous phenotype is suggestive of an “invasive Klebsiella strain,” and a warning should be sent to the clinician. Multiplex PCR may be a useful rapid test for detection of the serotype of confirming the diagnosis of the invasive Klebsiella
syndromeK. pneumoniae causing liver abscess.47
The lungs, CNS, and eyes were the most common metastatic sites (Lee SS et al., CID, 2008. 47:p642-650; Lee HC et al., J of Intern. Med., 2006. 259:606-614 and Feng-CT et al., Fang-CT et al., Clin Infect Dis. 2007 Aug 1;45(3):284-93). Only one-third of metastatic infections could be noted on admission and most of metastatic infections are diagnosed within 3 days after presentation. Meningitis and endophthalmitis are two major metastatic infection followed by septic pulmonary emboli or empyema. High mortality was seen in liver abscess associated with meningitis (Tang LM epidemiol infect 1997; 119:135-42). K. pneumoniae
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
endophthalmitis, often occurring in patients with diabetes mellitus, may initially present without hepatic involvement.48 A relative poor outcome with a high mortality was also seen
on patients with septic pulmonary emboli or empyema (Yang PW . J Chin Med Assoc 2008. 71:442-447). Thus, diagnosis with CT scan in liver abscess patient with abnormal chest x-ray may have a value in early notice on the development of complications.
Management
Because of the potential for metastatic infection, clinicians must monitor for such complications when the clinical response is poor. Strict glycemic control may prevent the development of metastatic complications. 35
The selection of antimicrobial therapy should be based on susceptibilities and clinical response. Cephalosporins are the antibiotic mainstay of antibiotic therapy in Asia (Table 3). Patients in the US were treated successfully with combination therapy (Table 3). Those antibiotics in various combinations included aminopenicillins (16·7%), antipseudomonal penicillins (16·7%), first/second- (8·3%) and third-generation (50·0%) cephalosporins, carbapenems (2·8%), fluoroquinolones (27·8%), aminoglycosides (16·7%), and metronidazole (30·6%) (Table 3).
Although liver abscess caused by extended spectrum β-lactamase (ESBL)-producing K.
pneumoniae has been reported in Taiwan, it is a rare occurrence. Carbapenems are the drug
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
of choice for ESBL producers. Carbapenem-resistant K. pneumoniae, such as strains producing New Delhi metallo-β-lactamase-1 (NDM-1), is of serious concern because of the limited treatment options for these hyperresistant strains.50 Further community investigation of the drinking water and sewage water in New Delhi revealed the presence of the NDM-1 gene, indicating heavy contamination of this gene in the community.51 If the incidence of community acquisition of this gene increases in the Asia-Pacific region, then clinicians should be alerted to the possible emergence of hyperresistant and hypervirulent K.
pneumoniae in community-acquired infections, defined as disease onset occurring in the
community or not in 3 days of hospital admission, such as liver abscess.
As ESBL-producing K. pneumoniae has been detected only very rarely in patients with liver abscess, antibiotics including ampicillin/sulbactam, a third-generation cephalosporin, aztreonam, or a quinolone may be used. We prefer to give a third-generation cephalosporin instead of a first-generation cephalosporin for 2–4 weeks for a solitary abscess or as long as 6 weeks for multiple abscesses.6 We often add an aminoglycoside unless a third-generation cephalosporin is used, although there is no randomized controlled trial evaluating the success rates of the combination regimen. The precise duration of therapy can be determined by ultrasonagraphic progress and resolution of fever and leukocytosis. Drainage of the abscess is often needed for a clinical response. Although percutaneous drainage was more widely used due to the progress of interventional radiology, aggressive hepatic resection resulted in a 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
better outcome than conventional percutaneous drainage for patients with APACHEII scores ≥ 15.53
Metastatic infections involving CNS and eyes are devastating and difficult to treat. In the absence of ESBL production, third-generation cephalosporins are the drugs of choice for K.
pneumoniae meningitis given their superior penetration into the cerebrospinal fluid.54 Both cefotaxime and ceftriaxone have proven effective for meningitis.55 Large doses are traditionally used for both cefotaxime (up to 2 g every 4 h) and ceftriaxone (2 g twice per day). Three weeks of therapy has been recommended due to relapse rates in those treated with shorter courses of therapy. Imipenem and meropenem are alternatives to third-generation cephalosporins.56
The prognosis for endophthalmitis caused by K. pneumoniae is extremely poor; more than 85% of reported patients experienced a severe visual deficit. Prognosis for visual recovery is improved if a diagnosis is made early with expeditious antibiotic therapy. K. pneumoniae endophthalmitis may present days after appropriate treatment for K. pneumoniae bacteremia and hepatic abscess has been started.57 Both intravitreal and intravenous routes should be used for endophthalmitis. Intravenous ceftazidime plus amikacin has been the most widely used combination. Combination intravitreal therapy with cephalosporins (cefazolin 2 gm and ceftazidime 2·25 gm) and aminoglycosides (gentamicin 4 gm, amikacin 0.5 gm) has been used successfully. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
The penetration of systemically given antibiotics into the eye is variable; however, third-generation cephalosporins can achieve peak vitreous levels of at least 2 mg/L.62 Aminoglycosides penetrate the vitreous reasonably well after repetitive systemic dosing.63 Oral ciprofloxacin can achieve vitreous concentrations of 0·2–0·5 mg/L. A single dose of 0·5 g of imipenem resulted in a mean vitreous concentrations of 0·2 mg/L 2–4 h after infusion; concentrations increased to approximately 2 mg/L after a 1-g dose.66
Conclusion
The invasive syndrome appears to be spreading to countries outside Asia. Presentation of liver abscess with bacteremia in patients infected with K. pneumoniae strains displaying a positive string test result (Fig. 1) may be the first clinical clue. Rapid diagnosis followed by appropriate therapy should improve patient outcome and prevent metastatic complications, which are severe. Further research should include determining the basis for predilection in Asians especially Taiwanese (the incidence in China is low), confirming that gastrointestinal colonization is the mechanism for infection, and elucidating the reason for the appearance of K1/K2 serotype in North America and Europe. More studies are necessary to elucidate the source or environmental reservoir for these highly virulent K1/K2 K. pneumoniae strains. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Contributors
LKS and FYC conceived and designed the review. LKS and KMY wrote the drafts of the review. JCL critically reviewed the draft. CPF proofread and edited the review.
Conflicts of interest
We declare that we have no conflicts of interest.
Acknowledgments
This work was supported by grants from the National Science Council of Taiwan (NSC 98-2341-B-016-024-MY3, NSC 99-2314-B-016-007-MY3, and NSC 100-2314 -B-016-013-MY3).
Search Strategy and Selection Criteria
We searched PubMed for papers published between Jan 1970 and June 2012 by using combinations of the following keywords: Klebsiella pneumoniae, liver abscess, endophthalmitis, and meningitis. We selected articles published in English or Chinese. Reports of large case series were selected for inclusion in this review in favor of anecdotal reports, which were numerous. Data surveyed included race and ethnicity, underlying diseases, clinical manifestations, therapeutic measures and outcome.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Serotype K1 Serotype K2
Figure. String tests of K1 and K2 Klebsiella pneumoniae strains
Wild type, WT, K. pneumoniae with normal capsule expression exhibited positive string test results. Loss of extreme mucoid phenotype mutants, capsular polymerase gene mutant (Δwzy or ΔmagA), capsular glycosyltransferase gene mutant (ΔrfbP), and regulator of mucoid phenotype A gene mutant (ΔrmpA) exhibited negative string test results.
Wild-type Δwzy(magA) ΔrfbP ΔrmpA 1 2 3 4 5 6 7 8 9 10 11
Table 1. Demographic and clinical characteristics of patients with K. pneumoniae liver abscess in the US, Korea, and Taiwana
United States (n=20,21 1824) Korea (n=263,11 5812) Taiwan (n=84,25 147,26 110,27 17128)
Age (mean, years) 53·6 59·9 57·4
Male 68·4% (26/38) 42·4% (136/321) 62·7% (321/512)
Race
Asian or Asian descent 50·0% (16/32)b 100% (58/58)d 100% (512/512)
Hispanic 25·0% (8/32)b African American 12·5% (4/32)b Caucasian 9·3% (3/32)b Underlying diseases Diabetes mellitus 28·9% (11/38) 38·0% (122/321) 63·1% (323/512 ) Hepatobiliary disease 18·4% (7/38) 19·9% (64/321) 24·8% (127/512 ) Malignancy 2·6% (1/38) 6·2% (20/321) 7·4% (38/512) Alcoholism 0 15·6% (50/321) 7·8% (40/512)
Chronic renal failure 0 0·3% (1/321) 3·1% (16/512)
Bacteremia 73·7% (28/38) 47·7% (153/321) 60·9% (312/512)
Number and location of abscess
Solitary 73·7% (28/38) 61·7% (198/321) 76·6% (392/512)
Multiple 26·3% (10/38) 38·3% (123/321) 23·4% (120/512)
Right hepatic lobe 64·9% (24/37)c 63·8% (37/58)e 65·0% (333/512)
Left hepatic lobe 24·3% (9/37)c 24·1% (14/58)e 25·2% (129/512)
Both lobes 10·8% (4/37)c 12·1% (7/58)e 9·8% (50/512)
Metastatic infection 23·7% (9/38) 8·1% (26/321) 14·5% (62/428)g
Lung 15·8% (6/38) 3·4% (2/58)e 3·7% (16/428)g
Eye 10·5% (4/38) e 4·2% (18/428)g
Central nervous system 7·9% (3/38) 1·7% (1/58)e 4·9% (21/428)g
Muscular and skeletal system 2·6% (1/38) e 2·1% (9/428)g
Urinary system 2·6% (1/38) e 0·2% (1/428)g
Mortality 7·9% (3/38) 3·8% (10/263)f 5·9% (30/512)
aThe denominator do not add up to the total in some cohorts, because of missing data in some patients.
bThe race of six patients was not reported in Reference 24.
cOne patient’s abscess location was not reported in Reference 24. dPatients’ race was not described in Reference 11.
eThe locations of liver abscess and number of patients with metastatic infection were not specifically provided in Reference 11.
1 2 3 4 5 6 7 8
fThere was no description of mortality in Reference 12. gMetastatic infection was not mentioned in Reference 25. 1
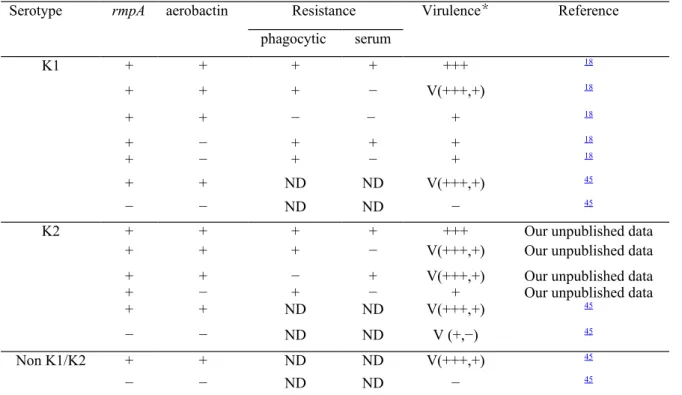
Table 2. Microbiological features associated with virulence
*(+++) Hypervirulent strains with LD50 < 1×103 CFU are more likely to induce complications in mice. (+)
Virulent strains with LD50 ≥ 1×103 CFU and < 1×106 CFU are less likely to induce complications in mice. (−)
Nonvirulent strains with LD50 ≥ 1×106 CFU and do not cause complications. V, variable; ND, no data
Serotype rmpA aerobactin Resistance Virulence* Reference
phagocytic serum K1 + + + + +++ 18 + + + − V(+++,+) 18 + + − − + 18 + − + + + 18 + − + − + 18 + + ND ND V(+++,+) 45 − − ND ND − 45
K2 + + + + +++ Our unpublished data
+ + + − V(+++,+) Our unpublished data
+ + − + V(+++,+) Our unpublished data
+ − + − + Our unpublished data
+ + ND ND V(+++,+) 45 − − ND ND V (+,−) 45 Non K1/K2 + + ND ND V(+++,+) 45 − − ND ND − 45 1 2 3 4
Table 3. Antibiotic treatment in patients with K. pneumoniae liver abscess and complications of endophthalmitis
Antibiotics Liver abscess Endophthalmitis
United States Korea11 Taiwan Yang et al.,67
Lederman et al.24 Pastagia et al.21 Lee et al.27 Chen et al.26 Cheng et al.6
Aminopenicillins 30·0% (6/20) 9·l% (2/22) Antipseudomonal penicillins 37·5% (6/16) 1st/2nd generation cephalosporins 12·5% (2/16) 5·0% (1/20) 94·5% (104/110) 70·2% (59/84) 55·1% (59/107) 18·2% (4/22) 3rd generation cephalosporins 43·8% (7/16) 55·0% (11/20) 82·5% (217/263) 3·6% (4/110) 17·8% (15/84) 44·9% (48/107) 72·7% (16/22) Carbapenems 6·3% (1/16) Fluoroquinolones 56·3% (9/16) 10% (2/20) 7·1% (6/84) 4·5% (1/22) Aminoglycosides 50·0% (8/16) 94·5% (104/110) 69·2% (74/107) 31·8% (7/22) Metronidazole 68·8% (11/16) 4·5% (1/22)
1st, 2nd generation cephalosporins: cefazolin, cefotetan
3rd generation cephalosporins: cefoperazone, cefotaxime, ceftazidime, ceftizoxime, ceftriaxone
Carbapenems: imipenem
Fluoroquinolones: levofloxacin, ciprofloxacin Aminoglycosides: amikacin, gentamicin, kanamycin 1
References
1. Chang FY, Chou MY, Fan RL, Shaio MF. A clinical study of Klebsiella liver abscess. Taiwan Yi Xue Hui Za Zhi. 1988; 87(3): 282-7.
2. Chang FY, Chou MY. Comparison of pyogenic liver abscesses caused by Klebsiella pneumoniae and non-K. pneumoniae pathogens. J Formos Med Assoc. 1995; 94(5): 232-7. 3. Liu YC, Cheng DL, Lin CL. Klebsiella pneumoniae liver abscess associated with septic endophthalmitis. Arch Intern Med. 1986; 146(10): 1913-6.
4. Saccente M. Klebsiella pneumoniae liver abscess, endophthalmitis, and meningitis in a man with newly recognized diabetes mellitus. Clin Infect Dis. 1999; 29(6): 1570-1.
5. Hu BS, Lau YJ, Shi ZY, Lin YH. Necrotizing fasciitis associated with Klebsiella pneumoniae liver abscess. Clin Infect Dis. 1999; 29(5): 1360-1.
6. Cheng HP, Siu LK, Chang FY. Extended-spectrum cephalosporin compared to cefazolin for treatment of Klebsiella pneumoniae-caused liver abscess. Antimicrob Agents Chemother. 2003; 47(7): 2088-92.
7. Yeh KM, Kurup A, Siu LK, Koh YL, Fung CP, Lin JC, et al. Capsular serotype K1 or K2, rather than magA and rmpA, is a major virulence determinant for Klebsiella pneumoniae liver abscess in Singapore and Taiwan. J Clin Microbiol. 2007; 45(2): 466-71.
8. Yeoh KG, Yap I, Wong ST, Wee A, Guan R, Kang JY. Tropical liver abscess. Postgrad Med J. 1997; 73(856): 89-92.
9. Wong WM, Wong BC, Hui CK, Ng M, Lai KC, Tso WK, et al. Pyogenic liver abscess: retrospective analysis of 80 cases over a 10-year period. J Gastroenterol Hepatol. 2002; 17(9): 1001-7.
10. Lok KH, Li KF, Li KK, Szeto ML. Pyogenic liver abscess: clinical profile, microbiological characteristics, and management in a Hong Kong hospital. J Microbiol Immunol Infect. 2008; 41(6): 483-90.
11. Chung DR, Lee SS, Lee HR, Kim HB, Choi HJ, Eom JS, et al. Emerging invasive liver abscess caused by K1 serotype Klebsiella pneumoniae in Korea. J Infect. 2007; 54(6): 578-83.
12. Kim SB, Je BK, Lee KY, Lee SH, Chung HH, Cha SH. Computed tomographic differences of pyogenic liver abscesses caused by Klebsiella pneumoniae and non-Klebsiella pneumoniae. J Comput Assist Tomogr. 2007; 31(1): 59-65.
13. Chau NG, Bhatia S, Raman M. Pylephlebitis and pyogenic liver abscesses: a complication of hemorrhoidal banding. Can J Gastroenterol. 2007; 21(9): 601-3.
14. Sobirk SK, Struve C, Jacobsson SG. Primary Klebsiella pneumoniae Liver Abscess with Metastatic Spread to Lung and Eye, a North-European Case Report of an Emerging Syndrome. Open Microbiol J. 2010; 4: 5-7.
15. Li J, Fu Y, Wang JY, Tu CT, Shen XZ, Li L, et al. Early diagnosis and therapeutic 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37
choice of Klebsiella pneumoniae liver abscess. Front Med China. 2010; 4(3): 308-16.
16. Ko WC, Paterson DL, Sagnimeni AJ, Hansen DS, Von Gottberg A, Mohapatra S, et al. Community-acquired Klebsiella pneumoniae bacteremia: global differences in clinical patterns. Emerg Infect Dis. 2002; 8(2): 160-6.
17. Turton JF, Englender H, Gabriel SN, Turton SE, Kaufmann ME, Pitt TL. Genetically similar isolates of Klebsiella pneumoniae serotype K1 causing liver abscesses in three continents. J Med Microbiol. 2007; 56(Pt 5): 593-7.
18. Siu LK, Fung CP, Chang FY, Lee N, Yeh KM, Koh TH, et al. Molecular typing and virulence analysis of serotype K1 Klebsiella pneumoniae strains isolated from liver abscess patients and stool samples from noninfectious subjects in Hong Kong, Singapore, and Taiwan. J Clin Microbiol. 2011; 49(11): 3761-5.
19. Vila A, Cassata A, Pagella H, Amadio C, Yeh KM, Chang FY, et al. Appearance of Klebsiella pneumoniae liver abscess syndrome in Argentina: case report and review of molecular mechanisms of pathogenesis. Open Microbiol J. 2011; 5: 107-13.
20. Rahimian J, Wilson T, Oram V, Holzman RS. Pyogenic liver abscess: recent trends in etiology and mortality. Clin Infect Dis. 2004; 39(11): 1654-9.
21. Pastagia M, Arumugam V. Klebsiella pneumoniae liver abscesses in a public hospital in Queens, New York. Travel Med Infect Dis. 2008; 6(4): 228-33.
22. Lin JC, Chang FY, Fung CP, Xu JZ, Cheng HP, Wang JJ, et al. High prevalence of phagocytic-resistant capsular serotypes of Klebsiella pneumoniae in liver abscess. Microbes Infect. 2004; 6(13): 1191-8.
23. Yeh KM, Lin JC, Yin FY, Fung CP, Hung HC, Siu LK, et al. Revisiting the importance of virulence determinant magA and its surrounding genes in Klebsiella pneumoniae causing pyogenic liver abscesses: exact role in serotype K1 capsule formation. J Infect Dis. 2010; 201(8): 1259-67.
24. Lederman ER, Crum NF. Pyogenic liver abscess with a focus on Klebsiella pneumoniae as a primary pathogen: an emerging disease with unique clinical characteristics. Am J Gastroenterol. 2005; 100(2): 322-31.
25. Chan KS, Yu WL, Tsai CL, Cheng KC, Hou CC, Lee MC, et al. Pyogenic liver abscess caused by Klebsiella pneumoniae: analysis of the clinical characteristics and outcomes of 84 patients. Chin Med J (Engl). 2007; 120(2): 136-9.
26. Chen SC, Wu WY, Yeh CH, Lai KC, Cheng KS, Jeng LB, et al. Comparison of Escherichia coli and Klebsiella pneumoniae liver abscesses. Am J Med Sci. 2007; 334(2): 97-105.
27. Lee SS, Chen YS, Tsai HC, Wann SR, Lin HH, Huang CK, et al. Predictors of septic metastatic infection and mortality among patients with Klebsiella pneumoniae liver abscess. Clin Infect Dis. 2008; 47(5): 642-50.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37
non-Klebsiella pneumoniae and Klebsiella pneumoniae. J Microbiol Immunol Infect. 2004; 37(3): 176-84.
29. Fung CP, Chang FY, Lee SC, Hu BS, Kuo BI, Liu CY, et al. A global emerging disease of Klebsiella pneumoniae liver abscess: is serotype K1 an important factor for complicated endophthalmitis? Gut. 2002; 50(3): 420-4.
30. Fung CP, Siu LK. Virulence of Klebsiella pneumoniae serotype K2 should not be underestimated in K. pneumoniae liver abscess. Clin Infect Dis. 2007; 45(11): 1530-1; author reply 2-3.
31. Lin JC, Siu LK, Fung CP, Yeh KM, Chang FY. Nosocomial liver abscess caused by extended-spectrum beta-lactamase-producing Klebsiella pneumoniae. J Clin Microbiol. 2007; 45(1): 266-9.
32. Yu WL, Chan KS, Ko WC, Lee CC, Chuang YC. Lower prevalence of diabetes mellitus in patients with Klebsiella pneumoniae primary liver abscess caused by isolates of K1/K2 than with non-K1/K2 capsular serotypes. Clin Infect Dis. 2007; 45(11): 1529-30; author reply 32-3.
33. Casanova C, Lorente JA, Carrillo F, Perez-Rodriguez E, Nunez N. Klebsiella pneumoniae liver abscess associated with septic endophthalmitis. Arch Intern Med. 1989; 149(6): 1467.
34. Sheu SJ, Kung YH, Wu TT, Chang FP, Horng YH. Risk factors for endogenous endophthalmitis secondary to klebsiella pneumoniae liver abscess: 20-year experience in Southern Taiwan. Retina. 2011; 31(10): 2026-31.
35. Lin JC, Siu LK, Fung CP, Tsou HH, Wang JJ, Chen CT, et al. Impaired phagocytosis of capsular serotypes K1 or K2 Klebsiella pneumoniae in type 2 diabetes mellitus patients with poor glycemic control. J Clin Endocrinol Metab. 2006; 91(8): 3084-7.
36. Chung DR, Lee H, Park MH, Jung SI, Chang HH, Kim YS, et al. Fecal carriage of serotype K1 Klebsiella pneumoniae ST23 strains closely related to liver abscess isolates in Koreans living in Korea. Eur J Clin Microbiol Infect Dis. 2011.
37. Podschun R, Ullmann U. Klebsiella spp. as nosocomial pathogens: epidemiology, taxonomy, typing methods, and pathogenicity factors. Clin Microbiol Rev. 1998; 11(4): 589-603.
38. Fung CP, Chang FY, Lin JC, Ho DM, Chen CT, Chen JH, et al. Immune response and pathophysiological features of Klebsiella pneumoniae liver abscesses in an animal model. Lab Invest. 2011.
39. Lin JC, Chang FY, Fung CP, Yeh KM, Chen CT, Tsai YK, et al. Do neutrophils play a role in establishing liver abscesses and distant metastases caused by Klebsiella pneumoniae? PLoS One. 2010; 5(11): e15005.
40. Fang CT, Chuang YP, Shun CT, Chang SC, Wang JT. A novel virulence gene in Klebsiella pneumoniae strains causing primary liver abscess and septic metastatic 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38
complications. J Exp Med. 2004; 199(5): 697-705.
41. Chuang YP, Fang CT, Lai SY, Chang SC, Wang JT. Genetic determinants of capsular serotype K1 of Klebsiella pneumoniae causing primary pyogenic liver abscess. J Infect Dis. 2006; 193(5): 645-54.
42. Struve C, Bojer M, Nielsen EM, Hansen DS, Krogfelt KA. Investigation of the putative virulence gene magA in a worldwide collection of 495 Klebsiella isolates: magA is restricted to the gene cluster of Klebsiella pneumoniae capsule serotype K1. J Med Microbiol. 2005; 54(Pt 11): 1111-3.
43. Yeh KM, Chang FY, Fung CP, Lin JC, Siu LK. magA is not a specific virulence gene for Klebsiella pneumoniae strains causing liver abscess but is part of the capsular polysaccharide gene cluster of K. pneumoniae serotype K1. J Med Microbiol. 2006; 55(Pt 6): 803-4.
44. Yu WL, Ko WC, Cheng KC, Lee HC, Ke DS, Lee CC, et al. Association between rmpA and magA genes and clinical syndromes caused by Klebsiella pneumoniae in Taiwan. Clin Infect Dis. 2006; 42(10): 1351-8.
45. Yu WL, Ko WC, Cheng KC, Lee CC, Lai CC, Chuang YC. Comparison of prevalence of virulence factors for Klebsiella pneumoniae liver abscesses between isolates with capsular K1/K2 and non-K1/K2 serotypes. Diagn Microbiol Infect Dis. 2008; 62(1): 1-6.
46. Lin AC, Yeh DY, Hsu YH, Wu CC, Chang H, Jang TN, et al. Diagnosis of pyogenic liver abscess by abdominal ultrasonography in the emergency department. Emerg Med J. 2009; 26(4): 273-5.
47. Turton JF, Baklan H, Siu LK, Kaufmann ME, Pitt TL. Evaluation of a multiplex PCR for detection of serotypes K1, K2 and K5 in Klebsiella sp. and comparison of isolates within these serotypes. FEMS Microbiol Lett. 2008; 284(2): 247-52.
48. Margo CE, Mames RN, Guy JR. Endogenous Klebsiella endophthalmitis. Report of two cases and review of the literature. Ophthalmology. 1994; 101(7): 1298-301.
49. Su SC, Siu LK, Ma L, Yeh KM, Fung CP, Lin JC, et al. Community-acquired liver abscess caused by serotype K1 Klebsiella pneumoniae with CTX-M-15-type extended-spectrum beta-lactamase. Antimicrob Agents Chemother. 2008; 52(2): 804-5.
50. Kumarasamy KK, Toleman MA, Walsh TR, Bagaria J, Butt F, Balakrishnan R, et al. Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study. Lancet Infect Dis. 2010; 10(9): 597-602. 51. Bradford PA, Bratu S, Urban C, Visalli M, Mariano N, Landman D, et al. Emergence of carbapenem-resistant Klebsiella species possessing the class A carbapenem-hydrolyzing KPC-2 and inhibitor-resistant TEM-30 beta-lactamases in New York City. Clin Infect Dis. 2004; 39(1): 55-60.
52. Walsh TR, Weeks J, Livermore DM, Toleman MA. Dissemination of NDM-1 positive 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37
environmental point prevalence study. Lancet Infect Dis. 2011; 11(5): 355-62.
53. Hsieh HF, Chen TW, Yu CY, Wang NC, Chu HC, Shih ML, et al. Aggressive hepatic resection for patients with pyogenic liver abscess and APACHE II score > or =15. Am J Surg. 2008; 196(3): 346-50.
54. Cherubin CE, Eng RH, Norrby R, Modai J, Humbert G, Overturf G. Penetration of newer cephalosporins into cerebrospinal fluid. Rev Infect Dis. 1989; 11(4): 526-48.
55. Cherubin CE, Corrado ML, Nair SR, Gombert ME, Landesman S, Humbert G. Treatment of gram-negative bacillary meningitis: role of the new cephalosporin antibiotics. Rev Infect Dis. 1982; 4 Suppl: S453-64.
56. Sentochnik DE, Eliopoulos GM, Ferraro MJ, Moellering RC, Jr. Comparative in vitro activity of SM7338, a new carbapenem antimicrobial agent. Antimicrob Agents Chemother. 1989; 33(8): 1232-6.
57. Chee SP, Ang CL. Endogenous Klebsiella endophthalmitis--a case series. Ann Acad Med Singapore. 1995; 24(3): 473-8.
58. Cheng DL, Liu YC, Yen MY, Liu CY, Wang RS. Septic metastatic lesions of pyogenic liver abscess. Their association with Klebsiella pneumoniae bacteremia in diabetic patients. Arch Intern Med. 1991; 151(8): 1557-9.
59. Chiu CT, Lin DY, Liaw YF. Metastatic septic endophthalmitis in pyogenic liver abscess. J Clin Gastroenterol. 1988; 10(5): 524-7.
60. Chou FF, Kou HK. Endogenous endophthalmitis associated with pyogenic hepatic abscess. J Am Coll Surg. 1996; 182(1): 33-6.
61. Liao HR, Lee HW, Leu HS, Lin BJ, Juang CJ. Endogenous Klebsiella pneumoniae endophthalmitis in diabetic patients. Can J Ophthalmol. 1992; 27(3): 143-7.
62. Sharir M, Triester G, Kneer J, Rubinstein E. The intravitreal penetration of ceftriaxone in man following systemic administration. Invest Ophthalmol Vis Sci. 1989; 30(10): 2179-83. 63. Barza M, Kane A, Baum J. Comparison of the effects of continuous and intermittent systemic administration on the penetration of gentamicin into infected rabbit eyes. J Infect Dis. 1983; 147(1): 144-8.
64. el Baba FZ, Trousdale MD, Gauderman WJ, Wagner DG, Liggett PE. Intravitreal penetration of oral ciprofloxacin in humans. Ophthalmology. 1992; 99(4): 483-6.
65. Keren G, Alhalel A, Bartov E, Kitzes-Cohen R, Rubinstein E, Segev S, et al. The intravitreal penetration of orally administered ciprofloxacin in humans. Invest Ophthalmol Vis Sci. 1991; 32(8): 2388-92.
66. Adenis JP, Mounier M, Salomon JL, Denis F. Human vitreous penetration of imipenem. Eur J Ophthalmol. 1994; 4(2): 115-7.
67. Yang CS, Tsai HY, Sung CS, Lin KH, Lee FL, Hsu WM. Endogenous Klebsiella endophthalmitis associated with pyogenic liver abscess. Ophthalmology. 2007; 114(5): 876-80. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38
1 2