Proofs of your article (Vol. 18, No. 7, cvi0422-10) from Clinical and Vaccine Immunology are available for
download
_______________________
Clinical and Vaccine Immunology Published by the American Society for Microbiology
Article title: Expression of CD25high Regulatory T Cells and PD-1 in Gastric Infiltrating CD4+ T
Lymphocytes in Patients with Helicobacter pylori Infection
Dear Author,
Please refer to the following URL:
http://rapidproof.cadmus.com/RapidProof/retrieval/index.jsp
Login: your e-mail address
Password:99jMkFDRVceW
The site contains 1 file. You will need to have Adobe Acrobat Reader software to read these files. This is
free software and is available for user downloading at
http://www.adobe.com/products/acrobat/readstep.html.
This PDF file contains:
*proofreading instructions
*proofreading marks guide
*page proofs for your article
*a query page (if applicable)
AFTER PRINTING THE FILE (within 48 hours after receipt of this e-mail), PLEASE READ THE
INSTRUCTIONS FIRST AND THEN THE PAGE PROOFS, AND:
1.Indicate changes or corrections, including any from coauthors, on a single copy of the hard-copy page
proof. Do NOT edit or alter the PDF file in any way.
2.Answer all queries (AQA, -B, -C, etc.) on the last page of the PDF proof. (Ignore any marginal mark
"Fn" that appears on the first page of the proofs.)
3.Sign and date the signature block on the first page of the proofs.
4.Send your signed, marked-up hard-copy version of the proof to the ASM Journals Department at the
address given below. Use mail or a courier service such as FedEx (a courier service is recommended).
Faxing is NOT recommended; ASM will not be responsible for errors caused by poor-quality faxes.
DO NOT SEND THE PROOF AS AN E-MAIL ATTACHMENT.
If you have any problems with your proofs or questions regarding changes you would like to make, please
contact me. PLEASE ALWAYS INCLUDE YOUR ARTICLE NO. ( cvi0422-10 ) WITH ALL
CORRESPONDENCE.
If you have problems accessing or viewing your PDF proofs, please contact Katie Gay of Cadmus
Professional Communications at 804-261-3155 (e-mail: [email protected]).
The proof contains 4 pages.
Clinical and Vaccine Immunology
To access the form and deadline information relating to PUBLICATION CHARGES AND REPRINT
ORDERS, and to provide billing instructions for your invoice, please go to the Author Billing System
(ABS) at https://authorbilling.asm.org within 1 week of receipt of this e-mail. If you have never created an
ASM eStore account, you will need to create a new account at the login screen of the ABS.
Sincerely,
Diane Smith
Production Editor
Clinical and Vaccine Immunology
Journals Department
American Society for Microbiology
1752 N St., N.W.
Washington, DC 20036-2904
Tel: 202-942-9288
Fax: 202-942-9355
INSTRUCTIONS FOR PROOFS
Mark all corrections, including any from coauthors, on a single copy of the proof that
you printed.
The final responsibility for correcting all errors is yours.
Special items that should be checked:
x
Accuracy of type, including Greek letters and any special characters
x
Wording of the running heads (Note: The page numbers on the proofs are
for easy reference only; they are not the actual page numbers that will be used
for the printed article.)
x
Tables and equations
x
Figures (See below for details.)
x
That all queries were answered
Checking figures:
x
Figures as they appear in the proofs are for validation of content and
placement, not quality of reproduction or color accuracy. Print output of
figures in the PDF page proofs will be of lower quality than the same figures
viewed on a monitor. Please avoid making changes to figures based on
quality of color or reproduction in proof.
x
See that each illustration is numbered correctly, is matched with the
appropriate legend, and is correctly oriented.
x
Check magnification (if appropriate) since the figure(s) may have been
resized.
x
Check that there are no missing or misaligned characters or labels.
(Some graphics applications, particularly PowerPoint, do not reliably handle
fonts or embedded images; thus, the file conversion may have resulted in
dropped characters, improperly converted characters, or shifting or obscuring
of various elements within the figure.)
Sending your marked-up proofs to ASM:
x
Sign and date the signature block on the bottom of the first page on the proof
x
Make a copy of the marked-up proof to keep in your file
x
Mail (or use a courier service such as FedEx) the signed, marked-up
hard-copy proof to the ASM Journals Department at the address given below.
Faxing is NOT recommended; ASM will not be responsible for errors caused
by poor-quality faxes. DO NOT SEND THE PROOF AS AN E-MAIL
ATTACHMENT.
Mailing address:
Journals
Department
American Society for Microbiology
1752 N St., NW
Washington, DC 20036-2904
General information:
The proof stage is not the time for revision, rewriting, rephrasing, addition of more recent
material, or any other significant change from the final edited manuscript. That is, the
manuscript that was approved by the editor should be the one printed; there should be no
major additions or deletions. In case of essential new information, you may send a short
“Addendum in Proof,” provided that the editor has given his or her consent. If references
to unpublished data or personal communications are added, it is expected that written
assurance granting permission for the citation will be included.
CLINICAL ANDVACCINEIMMUNOLOGY, July 2011, p. 000 Vol. 18, No. 7 1556-6811/11/$12.00 doi:10.1128/CVI.00422-10
Copyright © 2011, American Society for Microbiology. All Rights Reserved.
Expression of CD25
high
Regulatory T Cells and PD-1 in Gastric
Infiltrating CD4
⫹
T Lymphocytes in Patients with
Helicobacter pylori Infection
䌤
Yi-Ying Wu,
1,2†* Jiunn-Horng Chen,
3Jung-Ta Kao,
2,3Kuo-Ching Liu,
1,4Chih-Ho Lai,
5Yuan-Min Wang,
1,4Chin-Tung Hsieh,
6Jason T. C. Tzen,
4† and Ping-Ning Hsu
7,8†
Department of Medical Laboratory Science and Biotechnology, China Medical University, Taichung, Taiwan1; Graduate Institute of
Clinical Medical Science, China Medical University, Taichung, Taiwan2; Department of Internal Medicine, School of Medicine,
China Medical University Hospital and China Medical University, Taichung, Taiwan3; Graduate Institute of Biotechnology,
National Chung Hsing University, Taichung, Taiwan4; Department of Microbiology, School of Medicine, China
Medical University, Taichung, Taiwan5; Department of Pediatrics, Lotung Poh-Ai Hospital, I-Lan, Taiwan6;
Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan7; and
Graduate Institute of Immunology, China Medical University, Taichung, Taiwan8
Received 30 September 2010/Returned for modification 3 January 2011/Accepted 2 April 2011
We observed by flow cytometry that the frequency of both gastric infiltrating Tregs and PD-1-positive CD4 T cells is correlated with the density of Helicobacter pylori, suggesting that cellular immunity against this pathogen is inhibited.
Helicobacter pylori, a common human pathogen, infects
about 50% of the world’s population (9, 10). Many studies have confirmed that the pathogenesis of H. pylori infection is prob-ably due largely to the host immune system, particularly the cellular immune response. However, the mechanism by which
H. pylori negatively regulates the immune response against the
bacteria is not completely understood.
In recent years, regulatory T cells (Tregs) and related neg-ative regulatory molecules have been a focus of research on the immune mechanisms of diseases. Evidence indicates that re-moval or reduction of Tregs can enhance immune responses against infectious microbes (1, 2, 5, 6, 8, 11–13, 16). Expression of programmed cell death 1 (PD-1, also called CD279), a negative regulatory molecule in the CD28/B7 family, is in-duced on CD4⫹T cells, CD8⫹T cells, natural killer T cells, B cells, and activated monocytes during the course of many eases. B and T lymphocyte attenuator (BTLA), a newly dis-covered member of the CD28 family of costimulatory mole-cules, may have inhibitory function similar to that of PD-1.
The PD-1 signaling pathway is involved in chronic bacterial infection and may be a potential therapeutic target. However, the role of BTLA in H. pylori infection has not been investi-gated. In this study, we analyzed the frequency of gastric infil-trating CD4⫹CD25highTregs in patients with H. pylori infec-tion, as well as the expression of PD-1 and BTLA on gastric infiltrating CD4⫹T cells, and their relationships with H. pylori-related clinical markers.
Biopsy specimens of the gastric antrum were obtained from patients undergoing gastric endoscopy for dyspepsia at China
Medical University Hospital. There were 38 H. pylori-infected subjects enrolled in this study. Peripheral blood samples from the same patients served as the control. The presence of H.
pylori infection was determined by histopathologic examination
(including Giemsa staining) and/or by a positive result for a rapid urease test performed on at least one additional biopsy sample. The density of H. pylori was analyzed as suggested by the updated Sydney system (4): 0, absent; 1, mild; 2, moderate; and 3, marked. The degree of inflammation present in the histological specimens was also classified according to the up-dated Sydney system. Biopsy specimens of the gastric antrum were collected into sterile collection medium (calcium- and magnesium-free Hanks’ balanced salt solution [HBSS] with 5% fetal calf serum and penicillin plus streptomycin). The collected tissues were immediately placed in ice-cold RPMI 1640 complete medium (Gibco BRL, Gaithersburg, MD) which contained 10% fetal calf serum supplemented with pen-icillin (50 IU/ml), streptomycin (50 g/ml), L-glutamine (2
mM), and sodium pyruvate (1 mM). Gastric infiltrating lym-phocytes were isolated using a modified protocol according to a reported technique (15).
Flow cytometry analysis was performed using a technique described previously (14). The CD4⫹T cells were gated from the FSC low versus CD4⫹ T cells, which correspond to the lymphocyte population according to our previous data (15). All data were analyzed using SPSS version 13.0 for Windows (SPSS Inc., Chicago, IL). Mann-Whitney U tests were used for comparison between groups. Pearson correlation tests were performed for correlation analysis. All tests were two tailed, and P values of⬍0.05 were considered significant.
Initially, we determined the percentage of CD25⫹T cells in the total CD4⫹T-cell population in each of the 38 patients with H. pylori infection (Fig. 1A). The CD4⫹CD25high popu-lation represented 3.37 to 12.78% of CD4⫹T cells, and the CD4⫹CD25⫹T cell population represented 12.00 to 31.02% of CD4⫹T cells in gastric infiltrating lymphocytes (Fig. 1B).
* Corresponding author. Mailing address: Department of Medi-cal Laboratory Science and Biotechnology, China MediMedi-cal Univer-sity and Hospital, No. 91 Hsueh-Shih Rd., Taichung 404, Taiwan. Phone: 886 4 22053366, ext. 7228. Fax: 886 4 22057414. E-mail: [email protected].
† Contributed equally.
䌤Published ahead of print on 11 May 2011.
1
AUTHOR: Publication of this article cannot proceed without the signature of the person who read and corrected the proof on behalf of all the authors:
signature date
zcd00711/zcd4148d11z xppws S⫽1 5/30/11 Art: 0422-10
zjs / DOCHEAD⫽NOTE zjss / DOCTOPIC⫽MICROBIAL IMMUNOLOGY FROM COVER SHEET: Editor: Litwin Article No.: N Section: Microbial
AQ: A
Fn2
AQ: G
AQ: B
These data indicate that the frequency of CD4⫹ CD25high Tregs in gastric infiltrating lymphocytes (mean ⫾ standard deviation [SD], 7.38%⫾ 2.02%) was significantly higher than that in peripheral blood lymphocytes (mean⫾ SD, 4.58% ⫾ 1.04%) (P⫽ 0.008) (Fig. 1C).
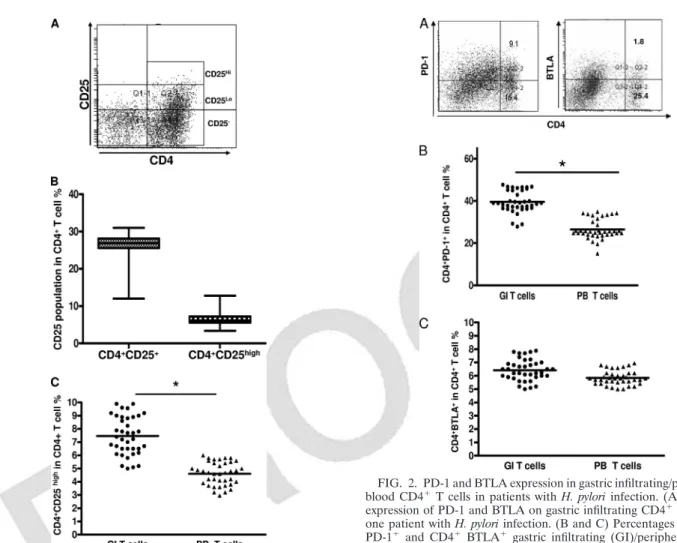
PD-1 and BTLA are important negative-immune-regulatory molecules. The percentage of CD4⫹PD-1⫹T cells in gastric infiltrating lymphocytes (Fig. 2A) (mean ⫾ SD, 39.62% ⫾ 10.09%) was significantly higher than that in peripheral blood lymphocyte controls (mean⫾ SD, 26.64% ⫾ 10.47%) (P ⫽ 0.0012) (Fig. 2B). However, the percentage of CD4⫹BTLA⫹ T cells in gastric infiltrating lymphocytes (Fig. 2A) (mean⫾ SD, 6.68%⫾ 0.18%) did not differ significantly from that in
peripheral blood lymphocytes (mean ⫾ SD, 6.2750% ⫾ 0.3709%) (P⫽ 0.085) (Fig. 2C).
We divided the H. pylori-positive gastric biopsy samples into three groups based on their histology scores for chronic in-flammation (marked, moderate, and mild). Patients with marked inflammation had a higher mean percentage of gastric infiltrating CD4⫹CD25highTregs than patients with moderate degree of inflammation (7.84% ⫾ 1.07% versus 5.76% ⫾ 1.23%, respectively; P⫽ 0.0043). There were also significant differences in CD4⫹CD25highTreg populations between the marked or moderate group and the mild group (Fig. 3A). Although the level of PD-1 expression on gastric infiltrating CD4⫹T cells in patients with marked inflammation was higher than that in patients with moderate inflammation, there was no significant difference in the number of gastric infiltrating CD4⫹ T cells expressing PD-1 between patients with marked inflam-mation and those with moderate inflaminflam-mation (52.07% ⫾ 11.01% versus 48.25% ⫾ 6.77%, respectively; P ⫽ 0.0552). There were significant differences in percentage of gastric in-filtrating CD4⫹PD-1⫹T cells between patients with marked
FIG. 1. Frequency of gastric infiltrating/peripheral blood CD4⫹ CD25⫹regulatory T cells (Tregs) in patients with H. pylori infection. (A) Gastric infiltrating CD4⫹ T cells were separated into CD25high, CD25low, and CD25⫺ T-cell subsets, as defined by the fluorescence intensity of CD25 obtained using isotypic control antibody. (B) Fre-quency of gastric infiltrating CD4⫹CD25highand total gastric infiltrat-ing CD4⫹CD25⫹T cells in patients with H. pylori infection. Data are expressed as box plots in which the horizontal lines represent the 25th, 50th, and 75th percentiles of the measured frequencies of Tregs. (C) Percentages of gastric infiltrating (GI)/peripheral blood (PB) CD4⫹CD25highTregs in patients with H. pylori infection. The hori-zontal bars indicate the median percentages of Tregs. The individual frequency for each subject included in the analysis is shown. Significant of differences were calculated using the Mann-Whitney U test.*, P⬍ 0.05.
FIG. 2. PD-1 and BTLA expression in gastric infiltrating/peripheral blood CD4⫹T cells in patients with H. pylori infection. (A) Surface expression of PD-1 and BTLA on gastric infiltrating CD4⫹T cells in one patient with H. pylori infection. (B and C) Percentages of CD4⫹ PD-1⫹ and CD4⫹ BTLA⫹ gastric infiltrating (GI)/peripheral blood (PB) T cells in patients with H. pylori infection. Horizontal bars indi-cate the median percentages of CD4⫹ PD-1⫹ T cells and CD4⫹ BTLA⫹T cells. The individual frequency for each subject included in the analysis is shown. Significance was calculated using the Mann-Whitney U test.*, P⬍ 0.05.
2 NOTES CLIN. VACCINEIMMUNOL.
zcd00711/zcd4148d11z xppws S⫽1 5/30/11 Art: 0422-10
F2
F3
inflammation or moderate inflammation and patients with mild inflammation (Fig. 3B).
We measured the density of H. pylori in each patient in order to investigate whether the increase in gastric infiltrating CD4⫹ CD25highTregs and gastric infiltrating CD4⫹PD-1⫹T cells correlated with density of H. pylori. Spearman analysis showed that the frequencies of gastric infiltrating CD4⫹ CD25high Tregs (r⫽ 0.524; P ⫽ 0.0282) and gastric infiltrating CD4⫹ PD-1⫹T cells (r⫽ 0.431; P ⫽ 0.016) were positively correlated with density of H. pylori (Fig. 3C and D). These results suggest
that an increased frequency of gastric infiltrating CD4⫹ CD25highTregs and gastric infiltrating CD4⫹PD-1⫹T cells may be associated with a weaker immune response, leading to poor bacterial clearance in patients with H. pylori infection. We show PD1/CD25 costaining and proportions of CD25high/PD-1 double and single positive T cells to clarify the relationship in Fig. 3E. In addition, there was no correlation between histol-ogy scores for chronic inflammation and density of H. pylori in patients (P⫽ 0.096) (Fig. 3F).
A recent study found that expression of the PD-1 on gastric
FIG. 3. Association between inflammation degree or density of H. pylori and gastric infiltrating CD4⫹CD25highTreg frequency or gastric infiltrating CD4⫹PD-1⫹T cells in patients with H. pylori infection. Gastric infiltrating lymphocytes were divided into three groups based on inflammation degree (A and B). Significance of differences between inflammation degree and gastric infiltrating CD4⫹CD25highTreg frequency or gastric infiltrating CD4⫹PD-1⫹T cells was analyzed using nonparametric Mann-Whitney U tests. The correlation between density of H. pylori and gastric infiltrating CD4⫹CD25highTreg frequency (C) or gastric infiltrating CD4⫹PD-1⫹T-cell populations (D) was analyzed using Spearman correlation analysis. (E) Correlation of gastric infiltrating (GI)/peripheral blood (PB) T cells in patients with H. pylori infection. The correlation between density of H. pylori and histology scores for chronic inflammation (F) was also analyzed using Spearman correlation analysis.*, P⬍ 0.05.
VOL. 18, 2011 NOTES 3
zcd00711/zcd4148d11z xppws S⫽1 5/30/11 Art: 0422-10
AQ: D
epithelial cells after H. pylori exposure promotes development of CD4⫹CD25⫹FoxP3⫹regulatory T cells (3). In addition, H.
pylori-specific CD4⫹T cells were shown to accumulate in the human H. pylori-infected gastric mucosa (7). Further studies are needed to clarify the relationship between PD-1 expression and high-level expression of CD25 on gastric infiltrating CD4⫹ T cells. Our findings demonstrate that the frequency of gastric infiltrating CD4⫹CD25highTregs and PD-1 expression levels on CD4⫹T cells were significantly increased in patients with
H. pylori infection and that these variables were positively
correlated with the degree of inflammation and the density of
H. pylori. Tregs and PD-1, as negative regulators of immunity,
may not only contribute to the persistence of chronic H. pylori infection but also be potential therapeutic targets for the treat-ment of chronic H. pylori gastritis patients.
This work was supported by grants from the National Science Coun-cil, Taiwan (NSC 98-2320-B-039-012-MY3), National Taiwan Univer-sity, Taiwan (100F008-406), and China Medical UniverUniver-sity, Taiwan (DMR-100-012, DMR-100-018, and CMU99-NTU-05). All authors declare no conflicts.
REFERENCES
1. Aseffa, A., et al. 2002. The early IL-4 response to Leishmania major and the resulting Th2 cell maturation steering progressive disease in BALB/c mice are subject to the control of regulatory CD4⫹CD25⫹ T cells. J. Immunol.
169:3232–3241.
2. Belkaid, Y., C. A. Piccirillo, S. Mendez, E. M. Shevach, and D. L. Sacks. 2002. CD4⫹CD25⫹ regulatory T cells control Leishmania major persistence and immunity. Nature 420:502–507.
3. Beswick, E. J., I. V. Pinchuk, S. Das, D. W. Powell, and V. E. Reyes. 2007. Expression of the programmed death ligand 1, B7-H1, on gastric epithelial cells after Helicobacter pylori exposure promotes development of CD4⫹ CD25⫹ FoxP3⫹ regulatory T cells. Infect. Immun. 75:4334–4341.
4. Dixon, M. F., R. M. Genta, J. H. Yardley, and P. Correa. 1996. Classification and grading of gastritis. The updated Sydney System. International Work-shop on the Histopathology of Gastritis, Houston 1994. Am. J. Surg. Pathol.
20:1161–1181.
5. Hori, S., T. L. Carvalho, and J. Demengeot. 2002. CD25⫹CD4⫹ regulatory T cells suppress CD4⫹ T cell-mediated pulmonary hyperinflammation driven by Pneumocystis carinii in immunodeficient mice. Eur. J. Immunol.
32:1282–1291.
6. Iwashiro, M., et al. 2001. Immunosuppression by CD4⫹ regulatory T cells induced by chronic retroviral infection. Proc. Natl. Acad. Sci. U. S. A.
98:9226–9230.
7. Lundgren, A., C. Trollmo, A. Edebo, A. M. Svennerholm, and B. S. Lundin. 2005. Helicobacter pylori-specific CD4⫹ T cells home to and accumulate in the human Helicobacter pylori-infected gastric mucosa. Infect. Immun. 73: 5612–5619.
8. Montagnoli, C., et al. 2002. B7/CD28-dependent CD4⫹CD25⫹ regulatory T cells are essential components of the memory-protective immunity to Can-dida albicans. J. Immunol. 169:6298–6308.
9. Parsonnet, J. 1997. Molecular mechanisms for inflammation-promoted pathogenesis of cancer—the Sixteenth International Symposium of the Sap-poro Cancer Seminar. Cancer Res. 57:3620–3624.
10. Parsonnet, J., et al. 1991. Helicobacter pylori infection and the risk of gastric carcinoma. N. Engl. J. Med. 325:1127–1131.
11. Raghavan, S., E. Suri-Payer, and J. Holmgren. 2004. Antigen-specific in vitro suppression of murine Helicobacter pylori-reactive immunopathologi-cal T cells by CD4CD25 regulatory T cells. Scand. J. Immunol. 60:82–88. 12. Shevach, E. M. 2000. Regulatory T cells in autoimmmunity. Annu. Rev.
Immunol. 18:423–449.
13. Singh, B., et al. 2001. Control of intestinal inflammation by regulatory T cells. Immunol. Rev. 182:190–200.
14. Wu, Y. Y., et al. 2010. Increased programmed death-ligand-1 expression in human gastric epithelial cells in Helicobacter pylori infection. Clin. Exp. Immunol. 161:551–559.
15. Wu, Y. Y., et al. 2007. Upregulation of CCL20 and recruitment of CCR6⫹ gastric infiltrating lymphocytes in Helicobacter pylori gastritis. Infect. Im-mun. 75:4357–4363.
16. Xu, D., et al. 2003. CD4⫹CD25⫹ regulatory T cells suppress differentiation and functions of Th1 and Th2 cells, Leishmania major infection, and colitis in mice. J. Immunol. 170:394–399.
4 NOTES CLIN. VACCINEIMMUNOL.
zcd00711/zcd4148d11z xppws S⫽1 5/30/11 Art: 0422-10
JOBNAME: AUTHOR QUERIES PAGE: 1 SESS: 3 OUTPUT: Mon May 30 21:12:17 2011 /rich4/zcd-cvi/zcd-cvi/zcd00711/zcd4148d11z