Enterovirus infection associated with increased risk of childhood type 1 diabetes in Taiwan: nationwide population-based cohort study
Hsiao-Chuan Lin,1,2,3 Chung-Hsing Wang,2,3 Fuu-Jen Tsai,3,4,5 Kao-Pin Hwang,2,3
Walter Chen,2,3 Cheng-Chieh Lin,2,4,6# Tsai-Chung Li7,8#
1. Department of Public Health, College of Public Health, China Medical University, Taichung, Taiwan
2. School of Medicine, College of Medicine, China Medical University, Taichung, Taiwan
3. Department of Pediatrics, China Medical University Hospital, Taichung, Taiwan 4. Department of Medical Research, China Medical University Hospital, Taichung,
Taiwan
5. College of Chinese Medicine, China Medical University, Taichung, Taiwan 6. Department of Family Medicine, China Medical University Hospital, Taichung,
Taiwan
7. Graduate Institute of Biostatistics, College of Management, China Medical University, Taichung, Taiwan
8. Department of Healthcare Administration, College of Medical and Health Science, Asia University, Taichung, Taiwan
#Correspondence and reprints: Tsai-Chung Li and Cheng-Chieh Lin
China Medical University, 91 Hsueh-Shih Road, Taichung, 40421, Taiwan, Tel: 886-4-22053366 ext. 6605, Fax: 886-4-22078539, e-mail: [email protected]
E-mail: [email protected]
Running title: Enterovirus infection increases childhood type 1 diabetes risk Word count:
Abstract: 228 words Main text: 2,943 words
Abstract
Aims/hypothesis To compare incidence rate of type 1 diabetes in children diagnosed with enterovirus (EV) infections with incidence rates in age- and sex-matched children without EV infection via population-based cohort and to examine whether direction or magnitude of association between EV infection and type 1 diabetes differs according to atopic disease status in children.
Methods We used insurance claims data from Taiwan's National Health Research Institutes Dataset to derive type 1 diabetes incidence in children aged up to 18 years with or without diagnosis of EV infection during 2000-2008. Incidence and hazard ratios of type 1 diabetes for EV infection were estimated by Poisson regression and Cox’s proportional hazard regression model.
Results Overall incidence of type 1 diabetes was higher in the EV than in the non-EV infection cohort (5.73 vs. 3.89 per 100,000 person-years, incidence rate ratio=1.48; 95% CI=1.19, 1.83) with adjusted hazard ratio of 1.48 (95% CI=1.19, 1.84). Among those with and without EV, incidence increased with age at diagnosis of EV infection, except in those aged below 1 year. Hazard ratios of type 1 diabetes according to allergic rhinitis or bronchial asthma had larger variation across subgroups.
Conclusions/interpretation The nationwide retrospective cohort study found positive correlation of type 1 diabetes with EV infection. Results suggest that preventive strategy, such as effective vaccine against EV infection, may lessen incidence of type 1 diabetes in Taiwan.
Abbreviations
IRR Incidence rate ratio
HR Hazard ratio
IR Incidence rate
EV Enterovirus
CVB Coxsackievirus B
NHIRD National Health Insurance Research Database NHI National Health Insurance
PIN Personal identification number
ICD-9- CM International Classification of Disease, 9th Revision, Clinical Modification
Introduction
Diabetes is one of the most common pediatric chronic diseases. Recent studies have shown a rapid global increase in childhood type 1 diabetes mellitus, particularly in those under age 5 [1-5]. Incidence varies greatly among ethnic groups: age-adjusted incidence ranges from 0.1 per 100,000/year in China and Venezuela [4] to 64.3 per 100,000/year in Finland in 2011 [6]. In Taiwan, average yearly crude incidence was 3.75/100,000 in children aged 0-14 years during 1992-1996 [7].
Type 1 diabetes is considered to be caused by complex interaction between genetic susceptibility, the immune system, and environmental factors [8, 9]. Though the cue for genetic predisposition has been elucidated, evidence points to involvement of enterovirus (EV) infection: i.e., poliovirus, Coxsackievirus A, Coxsackievirus B, and echovirus [10]. Gamble et al. (1969) first reported a possible link of EV infection with type 1 diabetes [11, 12]. Evidence for the contribution of group B Coxsackievirus infections abounds [13-15], yet several EVs species, including Coxsackievirus A [16-18], echoviruses [16, 17] and EVs of A-D species [19], may also take part in pathogenesis of type 1 diabetes. Cases of new-onset diabetes occurred in seasonal patterns [11, 20],sometimes in cluster or small outbreaks, often peaking 1-2 months after highest EV infection activity [21]. Recent study on intrafamilial spread of EV infections disclosed 20% siblings of diabetic probands acquired type 1 diabetes with 3-25 months latency [19]. Evidence for this association is supported by detection of
EVs in blood [13, 14, 17, 22], pancreas [15, 23-26] and gut mucosa [27] of type 1 diabetics. Histopathologic evidence indicating expression of enteroviral capsid protein VP1 in islet cells of such patients has been related to induction of protein kinase R and downregulation of Mcl-1 [23, 24]. Despite 40-plus years of research, the role of EVs in type 1 diabetes is far from established; chief obstacles stem from difficulty in obtaining pancreatic tissue from patients [25, 28]. A recent large meta-analysis of observational molecular studies re-affirmed association between human EV infection and type 1 diabetes [10]. Most such molecular studies came from Western countries [10], Cuba [29], Australia [30], Egypt [31] and/or Japan [32]; none explained rising tendency of association between EV infection and type 1 diabetes in Han Chinese [10]. In Finland, prospective birth-cohort study suggested Coxsackievirus B1 linked with induction of -cell autoimmunity that heralds type 1 diabetes [13]. Using virus antibody survey, case-control study alluded to association between Coxsackievirus B1 and type 1 diabetes [14]. Prior explorations of this angle (case-controls and cohorts), were limited by small clinical samples. Besides EV infection, inverse association was found between atopic diseases and childhood type 1 diabetes [33].
To link EV infection and subsequent type 1 diabetes, our nationwide population-based cohort utilized large-scale dataset available from Taiwan’s National Health Insurance. The aim of this study is to compare incidence rate of type 1 diabetes in children diagnosed with EV infections with incidence rate in age- and sex-matched
children without EV infection via population-based cohort. We also examined interaction of EV infection and atopic diseases, a possible etiologic factor.
Methods Data sources
Dataset of claims from the National Health Research Institutes database (NHRID) was obtained from Taiwan’s National Health Insurance (NHI) program, a universal health insurance system implemented by the Department of Health as of March 1995 and now covering approximately 99% of the 23.74 million of residents of Taiwan [34]. Data in the NHRID includes all claims data for 2000-2008 of children aged 18 years or younger, these randomly sampled with selection probability of 0.5 from the whole population of the same age: i.e., comprehensive information on demographics, dates of clinical visits, diagnostic codes, details of prescriptions, expenditure amounts, etc. Every individual has a unique personal identification number (PIN). To protect privacy, data on patient identities were scrambled cryptographically by NHIRD. All datasets can be interlinked through individual PINs. International Classification of Disease, 9th Revision, Clinical Modification (ICD-9-CM) identified diagnoses.
Study Subjects
We conducted a nationwide population-based cohort study that included two groups. Children with EV infection (aged < 18 years) during 2000-2007 were
identified and were followed up until December 31, 2008 or until first occurrence of type 1 diabetes. Subjects with EV infection should have had at least two ambulatory claims or at least one inpatient claim with diagnosis of ICD-9-CM codes 008.67 (enteritis due to enterovirus, n=97), 047 (meningitis due to enterovirus, n=8198), 047.0 (meningitis due to Coxsackievirus, n=252), 047.1 (meningitis due to echovirus, n=22), 048 (other enterovirus diseases of central nervous system, n=509), 074 (specific diseases due to Coxsackievirus, n=5179), 074.0 (herpangina, n=436372), 074.1(epidemic pleurodynia, n=89),074.2 (Coxsackievirus carditis, n=38), 074.20 (Coxsackievirus carditis, unspecified, n=18), 074.21 (pericarditis due to Coxsackievirus, n=1), 074.23 (myocarditis due to Coxsackievirus, n=31), 074.3 (hand-foot-and-mouth disease, n=116441), 074.8 (other specified diseases due to Coxsackievirus, n=2043), 079.1 (Echovirus infection in conditions classified elsewhere and of unspecified site, n=168) or 079.2 (Coxsackievirus infection in conditions classified elsewhere and of unspecified site, n=673) during 2000-2007, with first diagnosis as index date. We then excluded those children with incomplete information on sex and residential area (n =191). A total of 576,967 children with EV infection were eligible. The group without EV infection comprised half of all insured children of the same age and without a diagnosis of EV infection. After excluding those EV infected from 1996-2008 (n=868,831), a total of 3,129,171 children without EV were included. Using frequency-matching with sex and birth year, children without EV infection were selected from those eligible. Further excluding those with prior type 1 diabetes (n=206) before index date left 570,133 with and without EV infection in final analysis (Figure 1). The baseline or index date for the EV group was first outpatient visit or inpatient admission for EV infection. For the non-EV group, an index date between January 1, 2000 and December 31, 2007 was randomly assigned
according to index date distribution of the EV group. This study was approved by the Ethical Review Board of China Medical University Hospital.
Outcome measures and comorbidities
Follow-up person-years were derived for a child from index date to December 2008 or until onset of type 1 diabetes, death, or withdrawal from the insurance system. Outcome event was type 1 diabetes (ICD-9-CM codes 250.x1, 250.x3). Those with atopic dermatitis (ICD-9-CM codes 691.8), allergic rhinitis (ICD-9-CM code 477), or bronchial asthma (ICD-9-CM codes 493) identified within one year of index date were considered as having comorbidity.
Statistical Analysis
Distributions of demographic data and comorbidities (age at entry, sex, atopic dermatitis, allergic rhinitis, and bronchial asthma) were compared between groups.
Differences were examined using
χ
2
test for categorical variables and t -test for
continuous variables. Follow-up time served to estimate incidence rates of type 1 diabetes; Poisson regression assessed incidence rate ratio (IRR) of type 1 diabetes and its 95% confidence interval (CI) by comparing individuals with and without EV infection. Cumulative incidence of type 1 diabetes was computed by Kaplan-Meier
method, differences in cumulative incidence between groups were tested using a log-rank test. Cox proportional hazard regression models assessed the association between EV infection and type 1 diabetes adjusting for potential confounders. Adjusted hazard ratios (HRs) and their 95% CI were estimated. Interaction of EV infection status with age at entry, sex, atopic dermatitis, allergic rhinitis and bronchial asthma at baseline was examined by adding product terms into the full model, and likelihood ratio tested significance. SAS version 9.3 (SAS Institute, Cary, NC) was used for data analyses; two-sided tests were performed, p <0.05 was considered statistically significant. Results
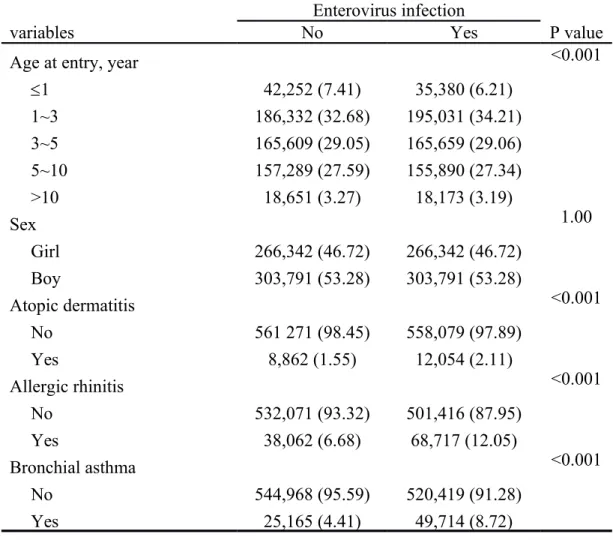
We identified 570,133 children with EV infection from 2000-2007 as EV group and frequency-matched 570,133 children without EV infection by sex and birth year as non-EV group. Mean age at entry and sex distribution was similar in both groups. Compared with non-EV, the EV group had a significantly higher prevalence of atopic dermatitis, allergic rhinitis, and bronchial asthma (Table 1). The incidence rate of type 1 diabetes was lower in the non-EV than EV group (4 vs. 6 per 100,000 person-years, IRR=1.48; 95% CI=1.19, 1.83) (Table 2). Incidence rate for both groups was further stratified based on age at entry, sex, allergic rhinitis, and bronchial asthma. Incidence rate proved consistently lower for the non-EV group, except for children aged 10 years and over, as well as in those with allergic rhinitis, or bronchial asthma. Median
follow-up time was 6.4 years overall. EV infection status is strongly associated with type 1 diabetes, exerting a 50% increase of risk after one year of follow-up (log-rank p<0.001, Figure 2).
Multivariate-adjusted HRs also demonstrated that EV infection and older age at entry were associated with higher risk of type 1 diabetes (Table 3): compared with non-EV children, those in the EV group were more susceptible (HR: 1.48; 1.19, 1.84). Children aged more than 10 years at entry showed elevated risk (HR: 2.18; 1.17, 4.04). However, HRs of type 1 diabetes according to allergic rhinitis, bronchial asthma, or any one of them had larger variation across subgroups (both p<0.05 for interactions of EV infection with allergic rhinitis or with bronchial asthma by likelihood ratio tests) (Figure 3). These HRs were greater in children with allergic rhinitis, bronchial asthma or any one atopic disease than those in corresponding counterpart.
Discussion
The present study identifies increased risk of type 1 diabetes among patients with and without EV infection, first and largest nationwide retrospective cohort study on association of type 1 diabetes with EV infections ever reported. The DIAMOND Project worldwide [4], and EURODIAB [2], multicenter prospective registration study in Europe, showed accelerating epidemic of type 1 diabetes across races and
geographic areas. This trend in different countries and among races may be explained by genetic background, chemical exposure and/or infectious pathogens among persons with diverse demographic characteristics [35]. Genetic factors alone cannot explain this rise. The Environmental Determinants of Type 1 Diabetes in the Young (TEDDY) [36] study may provide an answer on how environmental factors influence onset of type 1 diabetes in susceptible patients. Large prospective birth-cohort study disclosed CVB1 as associated with such risk in Finland [13]. Another virus antibody survey in diverse European populations suggested a link between CVBs and type 1 diabetes [14]. In Finland, which shows highest incidence of type 1 diabetes (64.3 per 100,000 person-years during 2006-2011) [6] and a low prevalence of EV infection [37], genetic background may play a major role [38, 39]. Hermann’s study found DQB1*0302/*0603 genotype positively correlated with risk of type 1 diabetes [40], DQB1*0603 linked with protection in other population [41, 42]. This phenomenon may explain high incidence of type 1 diabetes in Finland. However, Asia, Africa, and South America have low but increasing incidence of type 1 diabetes [5, 43] and high prevalence of EV infection; environmental factors like EV infection may play a vital role [37]. To estimate average yearly crude incidence of type 1 diabetes in children, a study in Taiwan [7] reported an increasing trend among patients under 18 years of age, with an overall rate of 3.75 (boys 3.15 and girls 4.39) per 100,000 person-years
during 1992-1996. Increasing incidence of type 1 diabetes by decreasing incidence of EV infection has been hypothesized [44]. Taiwan has relatively low type 1 diabetes incidence; we believe that marked escalation of said incidence in recent decades can be largely attributed to highly endemic spread of EV infection in Taiwanese children, given a stasis of gene flow and genetic drift in such a short period: NHIRD dataset revealed EV infection fluctuating in 2000-2008, with overall 10.5% increase from 1.24% in 2000 to 1.37% in 2008, which aver increasing incidence of EV infection.
Estimates of type 1 diabetes incidence in this study were consistent with those of earlier ones, indicating peaks in first presentation of type 1 diabetes appear in two age groups: 5-7 years and puberty [45]. The first peak may correspond to time of frequent infection due to the beginning of school attendance, the second with pubertal growth spurt induced by gonadal steroids and increased pubertal growth hormone secretion that antagonizes insulin [45].
We were also interested in connections between atopic disease (dermatitis, allergic rhinitis and bronchial asthma) and type 1 diabetes incidence. HRs showed an obvious trend toward lower risk in atopic than in non-atopic patients (Figure 2). We postulated that in atopic groups, deviation of the immune system toward the Th2 pathway may confer protective effects that prevent these patients from developing type 1 diabetes (a Th1 pathway autoactivity disease) [46, 47]. Case-control study has
shown negative correlation between childhood eczema and subsequent type 1 diabetes [33].
Animal studies have documented the concept of virus-induced diabetes, which increases biological plausibility of linkage between EV infection and type 1diabetes. In 1968, Craighead reported that picornavirus could induce diabetes in adult mice [48]. Many studies since then have used rodent models of spontaneous diabetes, with much attention has been focused on EVs, especially Coxsackievirus B4 [15]. Also, concrete evidence illustrates a range of EVs infecting, replicating, and lysing cultured human islets and insulin-producing cell lines in vitro [49] and markers of EV has also been found in the pancreas of type 1 diabetic patients [24]. A large prospective birth-cohort study disclosed CVB1 is associated with the risk of type 1 diabetes in Finland [13]. Another virus antibody survey in different European populations suggested an association between CVBs and type 1 diabetes [14].
Advantages of our study merit attention. First, administrative database avoids under-reporting of medical visits and hospitalizations [34]. Prior epidemiological and molecular studies are restricted by small sample size, even those from high-incidence countries, with no extensive epidemiological study design similar to ours. Second, nationwide population-based study prevents selection bias. Third, our study adjusted confounding factors: e.g., age, sex, co-morbidity. While race was not included in
adjustments, over 98% of Taiwanese are of Han Chinese stock; such homogenous background cohort sharply lessens likelihood of results confounded by ethnicity.
The current study has certain limitations. First, precision of diagnoses based on ICD-9 obtained in administrative data described by doctors, without confirmation by virus culture, serology or molecular methods, might matter. Though the Bureau of NHI regularly mockups patients’ charts to randomly confirm claims from all hospitals, bias may arise from miscoding and misclassification. Second, laboratory confirmation or even subtype of EV infection are not available from the database. Diagnoses of EV infections are based solely on clinical phenotypes. Clinical diagnoses of herpangina and hand-foot-and-mouth disease, easy and certain to diagnose by phenotype, account for nearly 97% of EV infection. On the other hand, most EV infections present without clear symptoms, and these asymptomatic infections could not be identified in this study. Third, selecting patients younger than 18 years may underestimate true numbers of type 1 diabetes patients in Taiwan, since onset is not limited to this age bracket. Fourth, low incidence of type 1 diabetes coupled with small sample size for cases of atopic dermatitis, allergic rhinitis, and bronchial asthma, limit ability to associate EV infection with type 1 diabetes under subgroups of such atopic diseases or to rate effect modification on association.
with EV infection in patients younger than 18 years to clarify the latter’s role in pathogenesis. While evidence of association between EV infection and pathogenesis is observational, conclusions are solid enough to guide further research on said association. This study suggests vaccination strategy against EV to slow rising incidence of type 1 diabetes.
Funding
This study was supported primarily by the Bureau of National Health Insurance (DOH99-HP-1205) and Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW103-TDU-B-212-113002).
Duality of interest
The authors declare no duality of interest associated with this manuscript. Contribution statement
CCL, TCL and HCL were responsible for conception and design of study. TCL and HCL acquired data; TCL analyzed. CHW, FJT, KPH, CCL and WC interpreted data. HCL and TCL were responsible for drafting the article. All authors revised the manuscript and approved final version. TCL and HCL are responsible for the integrity of the work as a whole.
References
[1] EURODIAB ACE Study Group (2000) Variation and trends in incidence of childhood diabetes in Europe. EURODIAB ACE Study Group. Lancet 355: 873-876 [2] Patterson CC, Dahlquist GG, Gyurus E, Green A, Soltesz G (2009) Incidence trends for childhood type 1 diabetes in Europe during 1989-2003 and predicted new cases 2005-20: a multicentre prospective registration study. Lancet 373: 2027-2033 [3] Chong JW, Craig ME, Cameron FJ, et al. (2007) Marked increase in type 1 diabetes mellitus incidence in children aged 0-14 yr in Victoria, Australia, from 1999 to 2002. Pediatr Diabetes 8: 67-73
[4] The DIAMOND Project Group (2006) Incidence and trends of childhood Type 1 diabetes worldwide 1990-1999. Diabet Med 23: 857-866
[5] Patterson CC, Gyurus E, Rosenbauer J, et al. (2012) Trends in childhood type 1 diabetes incidence in Europe during 1989-2008: evidence of non-uniformity over time in rates of increase. Diabetologia 55: 2142-2147
[6] Harjutsalo V, Sund R, Knip M, Groop P-H (2013) Incidence of Type 1 Diabetes in Finland Letters. JAMA 310: 427-428
[7] Tseng CH (2008) Incidence of type 1 diabetes mellitus in children aged 0-14 years during 1992-1996 in Taiwan. Acta Paediatr 97: 392-393
[8] Hober D, Sauter P (2010) Pathogenesis of type 1 diabetes mellitus: interplay between enterovirus and host. Nat Rev Endocrinol 6: 279-289
[9] Tauriainen S, Oikarinen S, Oikarinen M, Hyoty H (2011) Enteroviruses in the pathogenesis of type 1 diabetes. Semin Immunopathol 33: 45-55
[10] Yeung WC, Rawlinson WD, Craig ME (2011) Enterovirus infection and type 1 diabetes mellitus: systematic review and meta-analysis of observational molecular studies. BMJ 342: d35
[11] Gamble DR, Kinsley ML, FitzGerald MG, Bolton R, Taylor KW (1969) Viral antibodies in diabetes mellitus. Br Med J 3: 627-630
[12] Gamble DR, Taylor KW (1969) Seasonal incidence of diabetes mellitus. Br Med J 3: 631-633
[13] Laitinen OH, Honkanen H, Pakkanen O, et al. (2014) Coxsackievirus B1 is associated with induction of beta-cell autoimmunity that portends type 1 diabetes. Diabetes 63: 446-455
[14] Oikarinen S, Tauriainen S, Hober D, et al. (2014) Virus antibody survey in different European populations indicates risk association between coxsackievirus B1 and type 1 diabetes. Diabetes 63: 655-662
[15] Jaidane H, Hober D (2008) Role of coxsackievirus B4 in the pathogenesis of type 1 diabetes. Diabetes Metab 34: 537-548
of Coxsackie A and echo viruses in the pathogenesis of type I diabetes mellitus studied by IgM analysis. J Infect 24: 13-22
[17] Helfand RF, Gary HE, Jr., Freeman CY, Anderson LJ, Pallansch MA (1995) Serologic evidence of an association between enteroviruses and the onset of type 1 diabetes mellitus. Pittsburgh Diabetes Research Group. J Infect Dis 172: 1206-1211 [18] Roivainen M, Knip M, Hyoty H, et al. (1998) Several different enterovirus serotypes can be associated with prediabetic autoimmune episodes and onset of overt IDDM. Childhood Diabetes in Finland (DiMe) Study Group. J Med Virol 56: 74-78 [19] Salvatoni A, Baj A, Bianchi G, Federico G, Colombo M, Toniolo A (2013) Intrafamilial spread of enterovirus infections at the clinical onset of type 1 diabetes. Pediatr Diabetes 14: 407-416
[20] Gleason RE, Kahn CB, Funk IB, Craighead JE (1982) Seasonal incidence of insulin-dependent diabetes (IDDM) in Massachusetts, 1964-1973. Int J Epidemiol 11: 39-45
[21] Huff JC, Hierholzer JC, Farris WA (1974) An "outbreak" of juvenile diabetes mellitus: consideration of a viral etiology. Am J Epidemiol 100: 277-287
[22] Oikarinen S, Martiskainen M, Tauriainen S, et al. (2011) Enterovirus RNA in blood is linked to the development of type 1 diabetes. Diabetes 60: 276-279
[23] Richardson SJ, Leete P, Bone AJ, Foulis AK, Morgan NG (2013) Expression of the enteroviral capsid protein VP1 in the islet cells of patients with type 1 diabetes is associated with induction of protein kinase R and downregulation of Mcl-1.
Diabetologia 56: 185-193
[24] Willcox A, Richardson SJ, Bone AJ, Foulis AK, Morgan NG (2011)
Immunohistochemical analysis of the relationship between islet cell proliferation and the production of the enteroviral capsid protein, VP1, in the islets of patients with recent-onset type 1 diabetes. Diabetologia 54: 2417-2420
[25] Krogvold L, Edwin B, Buanes T, et al. (2014) Pancreatic biopsy by minimal tail resection in live adult patients at the onset of type 1 diabetes: experiences from the DiViD study. Diabetologia 57: 841-843
[26] Campbell-Thompson ML, Atkinson MA, Butler AE, et al. (2013) The diagnosis of insulitis in human type 1 diabetes. Diabetologia 56: 2541-2543
[27] Oikarinen M, Tauriainen S, Oikarinen S, et al. (2012) Type 1 diabetes is associated with enterovirus infection in gut mucosa. Diabetes 61: 687-691 [28] Campbell-Thompson M, Wasserfall C, Kaddis J, et al. (2012) Network for Pancreatic Organ Donors with Diabetes (nPOD): developing a tissue biobank for type 1 diabetes. Diabetes Metab Res Rev 28: 608-617
[29] Sarmiento L, Cabrera-Rode E, Lekuleni L, et al. (2007) Occurrence of
cell autoantibody-positive subjects in a population with a low incidence of type 1 diabetes. Autoimmunity 40: 540-545
[30] Craig ME, Howard NJ, Silink M, Rawlinson WD (2003) Reduced frequency of HLA DRB1*03-DQB1*02 in children with type 1 diabetes associated with
enterovirus RNA. J Infect Dis 187: 1562-1570
[31] Maha MM, Ali MA, Abdel-Rehim SE, Abu-Shady EA, El-Naggar BM, Maha YZ (2003) The role of coxsackieviruses infection in the children of insulin dependent diabetes mellitus. J Egypt Public Health Assoc 78: 305-318
[32] Kawashima H, Ihara T, Ioi H, et al. (2004) Enterovirus-related type 1 diabetes mellitus and antibodies to glutamic acid decarboxylase in Japan. J Infect 49: 147-151 [33] Stene LC, Ronningen KS, Bjornvold M, Undlien DE, Joner G (2010) An inverse association between history of childhood eczema and subsequent risk of type 1 diabetes that is not likely to be explained by HLA-DQ, PTPN22, or CTLA4 polymorphisms. Pediatr Diabetes 11: 386-393
[34] Lu JF, Hsiao WC (2003) Does universal health insurance make health care unaffordable? Lessons from Taiwan. Health Aff (Millwood) 22: 77-88
[35] Newhook LA, Penney S, Fiander J, Dowden J (2012) Recent incidence of type 1 diabetes mellitus in children 0-14 years in Newfoundland and Labrador, Canada climbs to over 45/100,000: a retrospective time trend study. BMC Res Notes 5: 628 [36] TEDDY Study Group (2008) The Environmental Determinants of Diabetes in the Young (TEDDY) Study. Ann N Y Acad Sci 1150: 1-13
[37] Viskari H, Ludvigsson J, Uibo R, et al. (2004) Relationship between the incidence of type 1 diabetes and enterovirus infections in different European populations: results from the EPIVIR project. J Med Virol 72: 610-617
[38] Noble JA, Erlich HA (2012) Genetics of type 1 diabetes. Cold Spring Harb Perspect Med 2: a007732
[39] Stankov K, Benc D, Draskovic D (2013) Genetic and epigenetic factors in etiology of diabetes mellitus type 1. Pediatrics 132: 1112-1122
[40] Hermann R, Turpeinen H, Laine AP, et al. (2003) HLA DR-DQ-encoded genetic determinants of childhood-onset type 1 diabetes in Finland: an analysis of 622 nuclear families. Tissue Antigens 62: 162-169
[41] Pugliese A, Gianani R, Moromisato R, et al. (1995) HLA-DQB1*0602 is associated with dominant protection from diabetes even among islet cell antibody-positive first-degree relatives of patients with IDDM. Diabetes 44: 608-613
[42] Sanjeevi CB (2000) HLA-DQ6-mediated protection in IDDM. Hum Immunol 61: 148-153
[43] Stanescu DE, Lord K, Lipman TH (2012) The epidemiology of type 1 diabetes in children. Endocrinol Metab Clin North Am 41: 679-694
[44] Viskari HR, Koskela P, Lonnrot M, et al. (2000) Can enterovirus infections explain the increasing incidence of type 1 diabetes? Diabetes Care 23: 414-416 [45] Achenbach P, Bonifacio E, Koczwara K, Ziegler AG (2005) Natural history of type 1 diabetes. Diabetes 54 Suppl 2: S25-31
[46] Cakir M, Akcay S, Karakas T, Gedik Y, Okten A, Orhan F (2008) Prevalence of atopy in children with type 1 diabetes mellitus, hepatitis B virus carriers, and healthy children: role of T helper 1 (Th1)-type immune response. Allergy Asthma Proc 29: 166-170
[47] Tzeng ST, Hsu SG, Fu LS, Chi CS (2007) Prevalence of atopy in children with type 1 diabetes mellitus in central Taiwan. J Microbiol Immunol Infect 40: 74-78 [48] Craighead JE, McLane MF (1968) Diabetes mellitus: induction in mice by encephalomyocarditis virus. Science 162: 913-914
[49] Ylipaasto P, Smura T, Gopalacharyulu P, et al. (2012) Enterovirus-induced gene expression profile is critical for human pancreatic islet destruction. Diabetologia 55: 3273-3283
Figure Legends
Figure 1: Flowchart of recruitment procedures
Figure 2: Cumulative risk of Type 1 DM based on enterovirus infection status Figure 3: HRs of Type 1 diabetes for enterovirus infections stratified by atopic dermatitis, allergic rhinitis, bronchial asthma, and any one of them
Table 1. The comparisons of sociodemographic factors and comorbidity according to enterovirus status (N = 1,140,266)
Enterovirus infection
variables No Yes P value
Age at entry, year <0.001
1 42,252 (7.41) 35,380 (6.21) 1~3 186,332 (32.68) 195,031 (34.21) 3~5 165,609 (29.05) 165,659 (29.06) 5~10 157,289 (27.59) 155,890 (27.34) >10 18,651 (3.27) 18,173 (3.19) Sex 1.00 Girl 266,342 (46.72) 266,342 (46.72) Boy 303,791 (53.28) 303,791 (53.28) Atopic dermatitis <0.001 No 561 271 (98.45) 558,079 (97.89) Yes 8,862 (1.55) 12,054 (2.11) Allergic rhinitis <0.001 No 532,071 (93.32) 501,416 (87.95) Yes 38,062 (6.68) 68,717 (12.05) Bronchial asthma <0.001 No 544,968 (95.59) 520,419 (91.28) Yes 25,165 (4.41) 49,714 (8.72)
Calculates the P value from chi-square test. Data are presented as n (%).
Table 2. Incidence rates and incidence rate ratio of type 1 DM according to enterovirus status stratified by sociodemographic factors and comorbidity
Without enterovirus infection With enterovirus infection
variables No. of event Person-years IR No. of event Person-years IR IRR (95%CI)
All 141 3,627,392 3.89 208 3,626,979 5.73 1.48 (1.19, 1.83)
Age at entry, year
1 7 294,658 2.38 15 253,019 5.93 2.50 (1.02, 6.12) 1~3 40 1,245,225 3.21 68 1,302,442 5.22 1.63 (1.10, 2.40) 3~5 46 1,047,282 4.39 52 1,045,108 4.98 1.13 (0.76, 1.68) 5~10 38 935,671 4.06 64 924,243 6.92 1.71 (1.14, 2.55) >10 10 104,557 9.56 9 102,166 8.81 0.92 (0.37, 2.27) Sex Girl 61 1,684,340 3.62 101 1,684,114 6.00 1.66 (1.21, 2.28) Boy 80 1,943,052 4.12 107 1,942,864 5.51 1.34 (1.00, 1.79) Allergic rhinitis No 130 3,415,308 3.81 182 3,227,963 5.64 1.48 (1.18, 1.86) Yes 11 212,084 5.19 26 399,016 6.52 1.26 (0.62, 2.54) Bronchial asthma No 158 3,606,177 4.38 227 3,358,232 6.76 1.54 (1.26, 1.89) Yes 4 47,662 8.39 11 295,297 3.73 0.44 (0.14, 1.39)
IR, incidence rate, per 100,000 person-years
Table 3: Crude and adjusted hazard ratios (HRs) of type 1 DM for enterovirus infection, demographic characteristics, and comorbidity
Crude Adjusted
Variable HRs (95% CI) HRs (95% CI)
Enterovirus infection No 1.00 1.00 Yes 1.48 (1.19, 1.83)*** 1.48 (1.19, 1.83)*** Age, year 1 1.00 1.00 1~3 1.04 (0.66, 1.65) 1.03 (0.65, 1.62) 3~5 1.14 (0.72, 1.81) 1.13 (0.71, 1.79) 5~10 1.33 (0.84, 2.11) 1.31 (0.82, 2.08) >10 2.24 (1.21, 4.15)* 2.18 (1.18, 4.04)* Sex Girl 1.00 1.00 Boy 1.00 (0.81, 1.24) 1.01 (0.82, 1.24) Allergic rhinitis No 1.00 1.00 Yes 1.27 (0.90, 1.79) 1.30 (0.90, 1.87) Bronchial asthma No 1.00 1.00 Yes 0.78 (0.48, 1.27) 0.64 (0.38, 1.08)
**:p<0.01; ***:p<0.001; Adjusted HR: each variable in Cox proportional hazards regression considering enterovirus infection, age, sex, allergic rhinitis, and bronchial asthma was adjusted for all variables in the model except itself.