© 2009 The American Association of Suicidology
Development of a Chinese Version
of the Suicide Intent Scale
Susan S.F. Gau, MD, PhD, Chin-Hung Chen, MD, Charles T.C. Lee, PhD, Jung-Chen Chang, PhD,
and Andrew T.A. Cheng, MD, PhD, DSc (London), FRCPsych
This study established the psychometric properties of the Chinese version of the Suicide Intent Scale (SIS) in a clinic- and community-based sample of 36 patients and 592 respondents, respectively. Results showed that the Chinese SIS demonstrated good inter-rater and test-retest reliability. Factor analysis generated three factors (Precautions, Planning, and Seriousness) explaining 92.9% of the total variance with high internal consistency. It was moderately correlated with depressive symptoms. Results suggest that the Chinese SIS is a reliable and valid instrument for use in assessing the extent of suicidal intention among subjects with deliberate self-harm in ethnic Chinese populations.
Suicide has become an important global pub- attempt suicide by the year 2020 (Bertolote & Fleischman, 2002). The Chinese popula-lic health issue since the last decade and its
impact on the entire society is still increasing tions in China (Wang et al., 2003), Hong Kong (Yip, Law, & Law, 2003), and Taiwan (Hawton, 2000). The WHO has predicted
that the global incidence of suicide will reach have also experienced a recent increase of suicide.
approximately 1.53 million people per year,
and 10 to 20 times as many individuals will To identify major predictive factors for suicide is an important component in suicide prevention, and the extent of suicide intent, defined as the seriousness or intensity of Susan S.F. Gau, MD, PhD, is with the
one’s wish to terminate one’s own life (Beck Department of Psychiatry, College of Medicine,
National Taiwan University and National Taiwan & Herman, 1974), has been reported to sig-University Hospital; Chin-Hung Chen, MD, is nificantly predict subsequent suicides (Hjelme-with Tsao-Tun Psychiatric Center, Nantou, Tai- land et al., 1998; Lo¨nnqvist & Tolppanen, wan; Jung-Chen Chang, PhD, is with Ching Kuo
1985; Pallis, Gibbons, & Pierce, 1984; Pierce, Institute of Management and Health, Keelung,
1981; Suokas & Lonnqvist, 1991). The pre-Taiwan; and Andrew T.A. Cheng, MD, PhD,
DSc, FRCPsych, and Charles T.C. Lee, PhD, dictive power of suicide intent on eventual are with the Institute of Biomedical Sciences, Aca- suicide is even stronger than previous at-demia Sinica (Drs Cheng and Lee), Taipei, tempts or hopelessness (Zhang & Norvilitis, Taiwan.
2002). It has thus been suggested that mea-The authors would like to thank all
mem-surement of suicide intent should be rou-bers of the research team and the 12 interviewers
who conducted the interviews among 592 com- tinely included in clinical practice in the sui-munity respondents. This study received no cide prevention program (Harriss & Hawton,
funding. 2005; Hjelmeland et al., 2002; Pierce, 1981).
Address correspondence to Professor
An-Few studies have comprehensively as-drew Cheng, Institute of Biomedical Sciences,
Ac-sessed the severity of suicide intent among ademia Sinica, Taipei, Taiwan; E-mail: bmandrew
(SIS) has been one of the most commonly of our knowledge, there has been no report of using the SIS in other parts of the world, used instruments measuring suicide intent in
clinical settings (Beck & Herman, 1974). The where the characteristics of suicidal act and the expression of suicide intent might be SIS has intentionally excluded items
regard-ing medical lethality or the effectiveness of considerably different from that in western societies (Cheng & Lee, 2000).
the suicide act in its construct (Beck, Beck, &
Kovacs, 1975). Previous studies reported broadly
sim-ilar risk factors for suicide in Taiwan and in Several studies have evaluated the
psy-chometric properties of the SIS (Beck & Les- western countries, including depressive dis-order, alcoholism, personality disorder char-ter, 1976; Beck & Herman, 1974; Diaz et al.,
2003; Kingsbury, 1993; Mieczkowski et al., acterized by impulsivity, life events, family history of suicide, and previous suicide at-1993; Spirito, Sterling, Donaldson, &
Arri-gan, 1996; Wetzel, 1976). These studies re- tempt(s) (Cheng, 1995; Cheng, Mann, & Chan, 1997; Cheng, Chen, Chen, & Jenkins, ported high internal reliability of the SIS
with Cronbach’s alpha coefficients ranging 2000). However, little is known about the level of suicide intent among suicides and its from 0.86 (Diaz et al., 2003) to 0.95 (Beck
& Herman, 1974), as well as high inter-rater possible contribution to differential suicide rates in Chinese populations around the reliability with kappa coefficients ranging
from 0.81 (Mieczkowski et al., 1993) to 0 .95 globe (Phillips et al., 2002). In order to accu-rately measure suicide intent in Chinese pop-(Beck & Herman, 1974). For construct
valid-ity, factor analyses have demonstrated two ulations, we have developed a Chinese ver-sion of the SIS and examined its reliability (Diaz et al., 2003; Mieczkowski et al., 1993),
three (Spirito et al., 1996), or four factors and validity in two samples of respondents with a history of recent deliberate self harm (Beck & Lester, 1976; Kingsbury, 1993;
Wet-zel, 1976), suggesting that suicidal intent may (DSH) in this study. We have also examined the feasibility for nonphysician mental health not only contain a single dimension.
Regard-ing concurrent validity, the SIS is moderately staffs to administer the interview items of the Chinese SIS.
correlated with measures of depression (Chance, Kaslow, & Baldwin, 1994; Minkoff, Bergman, Beck, & Beck, 1973; O’Brien,
Hol-ton, Hurron, Watt, & Hassanyeh, 1987; Platt METHODS & Dyer, 1987; Silver, Bohnert, Beck, &
Mar-cus, 1971), hopelessness (Beck & Herman, Development of the Chinese Version of the SIS
1974; Platt & Dyer, 1987), and lethality of suicide attempts (Haw, Hawton, Houston, &
Townsend, 2003). A higher SIS score is noted The SIS consists of 8 items (objective circumstances section) for interview and 7 in suicide attempters with major depression
(Astruc et al., 2004). However, findings con- items for self-report. The former (objective circumstances) inquires about the factual as-cerning predictive validity of the SIS is
con-flicting (Samuelsson, Jokinen, Nordstrom, & pects of the attempt and the surrounding events. The latter (self-report section) con-Nordstrom, 2006; Suominen, Isometsa,
Os-tamo, & Lonnqvist, 2004) with a low positive cerns the subject’s thoughts and feelings about the former, which might be more vul-predictive power, which might be explained
by the low incidence rate of suicide (Harriss nerable to distortion by people with self-harm who might wish to enhance the social & Hawton, 2005).
Although the SIS has been used in al- desirability of suicidal behavior or exaggerate the wish to die. Each of the SIS items is rated most all studies investigating suicide intent in
western societies (O’Donnell, Farmer, & on a 3-point Likert-type scale (0–2) with a total score of 0–30.
Catalan, 1996; Suominen, Isometsa, Heila,
psychiatrists and five other mental health cide and parasuicide, would be subsumed within this definition.
professionals conducted the development of
the SIS. A two-stage translation was first car- The 36 patients were aged 18 years and over without any obvious cognitive or ried out by two research psychiatrists fluent
in English. The other three psychiatrists psychotic symptoms. Among them, 18 were interviewed using the first 8 items of the ob-then independently examined these two
ver-sions. Comparing with the original English jective circumstances section in the Chinese SIS by one of the team members. These in-version, the back-translated English version
did not demonstrate any semantic distortion terviews were audio taped and subsequently rated by the other 9 raters. Ratings for the or any missing of the content. A pretest
among 40 psychiatric patients with DSH was first three interviews from all raters were compared and any discrepancies were dis-then conducted with subsequent
modifica-tions for psycholinguistic equivalents. All the cussed item by item in a team meeting with-out changes made to the ratings. The rest of 15 items are found to be relevant and
under-standable by respondents. However, the word- the 18 patients were asked to fill out the 7 self-reported items twice, with the second ings and examples of actions given in some
item questions need to be modified (details of one done 7 to 14 days (Mean= 9.1, SD = 2.9) after the first reports.
the modification are available from A.T.A.C.
upon request). For example, the original The internal consistency, construct va-lidity and convergent vava-lidity were then con-question for item 7 (suicide note) was
modi-fied to include both suicide note and “last ducted among the 592 subjects with DSH recruited from a community-based suicide words” (more frequently used by the elderly).
The original question for item 5 (final acts register system in Nantou County, Taiwan, aiming at the identification of all inhabitants in anticipation of death) was modified with
common acts observed in Taiwan, including who had a DSH. Nantou County encom-passes suburban and rural areas with a total seeing significant family members or favorite
possessions, putting personal belongings in a population of approximately 500,000. The DSH acts were identified using a whole pop-good order, giving instructions for important
things, etc. ulation approach in two stages. In the first
stage, subjects with DSH were reported by informants to the case register system set up Study Subjects and Procedures
by Nantou Health Bureau. Informants in-cluded people working in places where cases were seen or assessed, that are (1) health per-The institutional review board of the
Tsaotun Psychiatric Center, Nantou, Taiwan sonnel, including emergency room nurses in hospitals, general practitioners as well as lo-approved this study. Informed consent was
obtained from each study subject in advance cal public health nurses; and (2) social service providers such as firefighters, police, social after explanation of the purpose and
proce-dure of this study and reassurance of confi- workers, and NGO workers. DSH cases were then approached by the staff of Nantou dentiality.
The reliability and validity of the Chi- Community Mental Health Center.
The 592 study subjects who gave their nese SIS were examined in two samples with
a recent history of DSH: one of 36 psychiat- consent to participate in this study occupied 36.4% of a total of 1,627 cases identified dur-ric patients and one of 592 representative
re-spondents recruited from the community. ing June, 2001, and October, 2005. Their mean age was 38.66 years (SD= 15.87, rang-DSH means all acts of deliberate
self-poisoning or self-injury, irrespective of the ing from 12 to 88), with males (40.69, SD= 17.72) older than females (37.55, SD= 14.66), degree of suicidal intent (NHS Centre for
Reviews and Dissemination, 1998). The other (t= 0.021, p = 0.021). The mean age (37.18, SD= 15.32) of our sample was slightly lower terms in general use, namely attempted
sui-than the total cases (t= 2.262, p = 0.024] and 0.89 and 0.92 in a community sample of 2,919 adults aged 18 to 40 in Taiwan (per-the gender distribution was (per-the same as (per-the
total cases (92 female, 64.8%; p= 0.97). The sonal communication), and a college-based sample of 273 students in China (Zhang & distributions of educational levels of 577
par-ticipants (15 missing data) were 14 illiterate Norvilitis, 2002), respectively. (2.4%), 125 primary school (21.7%), 188
ju-nior high (32.6%), 299 seju-nior high (39.7%), Statistical Analysis and 21 college and higher (3.6%). All of
them were invited to receive a detailed inter- The pre-selected alpha value was 0.05. For the first 8 SIS items, the overall agree-view assessment within one month of the
in-dex event, conducted either in hospital (if ad- ment and the generalized kappa values were calculated for inter-rater reliability among 10 mitted) or in their own homes.
The interview assessments covered the raters on 18 patients. The Cronbach’s alpha coefficient was calculated for internal consis-Chinese SIS, alcohol problems, life events,
family history, and past history of suicide/ tency. Spearman rank correlation, intraclass correlations, and paired t-test were computed DSH, the Chinese version of the Center for
Epidemiologic Studies-Depression Scale (CES- to test the stability of the repeated measures (test-retest reliability) of the last 7 self-reported D). The interviews were conducted by
psy-chiatric nurses, social workers, and clinical items in the SIS. Exploratory factor analysis was conducted by taking the polychotomous psychologists (N= 12) who received a
train-ing in the use of the instrument. They also data scale into consideration. We calculated the matrix of polychoric correlation coeffi-carried out an inter-rater reliability of the
Chinese SIS (objective circumstance) using cient on 15 SIS items, and then performed principal component analysis with extraction the same 18 psychiatric patients.
method, followed by oblimin rotation method which took into consideration the inter-factor The Chinese CES-D
correlation. Pearson correlation was com-puted for the correlations between the sub-The CES-D, a 20-item self-reported
depression symptom scale, was developed by scales and total scores of the SIS, and CES-D scores by gender. The difference in these the Center for Epidemiologic Studies in the
States (Weissman, Sholomskas, Pottenger, correlations between male and female sub-jects was statistically tested. The mean scores Prusoff, & Locke, 1977). It was used to screen
for current depressive symptoms during the of the subscales of the SIS were compared between male and female subjects and among past week. Each item is rated on a 4-point
Likert scale from 0 for Rarely (less than one the four age groups (≤20, 21 to 40, 41 to 60, ≥61) using one-way analysis of variance day per week) to 3 for Always (5 days or more
per week), generating a total score of the 20 (ANOVA) and nonparametric methods. The Kolmogorov-Smirnov normality tests showed items ranging from 0 to 60. The scale has
been proved to be a reliable and valid tool that the distribution of all of the variables vi-olated the normality assumption (all p< for detecting depressive symptoms and their
changes over time in the general population 0.001). Therefore, in addition to ANOVA with Bonferron’s adjustment for post hoc and psychiatric settings (Weissman et al.,
1977). The sensitivity and specificity of the multiple comparisons, we also used nonpara-metric methods (Mann-Whitney test and Chinese CES-D in screening for depressive
illness in community respondents was re- Kruskal-wallis test) to test the mean differ-ences of these variables between male and fe-ported to be 92% and 91%, respectively, with
a classification rate of 91.8% at a cut-off male subjects and among the four age groups, respectively. Cohen’s d was used to compute point of 15 (Chien & Cheng, 1985). The
in-ternal consistency (Cronbach α coefficient) the effect size (standardized difference be-tween the two means) for the males and fe-of the Chinese CES-D were reported to be
males (Cohen, 1988). Statistical analyses Test-Retest Reliability were performed with SAS, version 9.1 (SAS
The 7 self-reported items of the Chi-Institute, Cary, N.C.).
nese SIS demonstrated good test-retest reli-ability with the Spearman rank correlation ranging from 0.72 to 1.00 (Table 1). There RESULTS
were no statistical differences between the first and second measurements of the 7 items Inter-Rater Reliability
(p values ranging from 0.163 to 1 in paired t-tests), indicating the stability of the repeated For the 8 interview items, their per- measures.
cent agreements were high, ranging from
0.73 to 0.94 and 0.76 to 0.91 in the 10 re- Factor Structure of the Chinese SIS search team members and the 12
interview-ers, respectively. The generalized kappa, Table 2 presents results from factor analysis. There were 3 factors with eigenval-which takes the chance agreement into
con-sideration, ranged from 0.38 to 0.83 and 0.42 ues exceeding unity, accounting for a cumula-tive total variance of 92.9%. All the items in to 0.69, respectively, in the two groups (Table
1). The results indicated a comparable and each of the factors loaded high (>0.50). Fac-tor I, Precautions, contains items 1–4; FacFac-tor acceptable inter-rater reliability between the
two groups. II, Planning, includes items 5–7; and Factor
TABLE 1
Inter-Rater and Test-Retest Reliability of the Chinese Suicide Intent Scale (SIS) Inter-rater Reliability (N= 18)
Test-retest Agreement Generalized Reliability
(%) Kappa (N= 18)
SIS Group Group Group Group
Items Description Ia IIb Ia IIb γ ICC
1 Isolation 91 89 0.73 0.68
2 Timing 73 79 0.38 0.47
3 Precautions Against Discovery 83 86 0.62 0.63
4 Act to Gain Help 87 82 0.57 0.53
5 Final Acts 86 76 0.54 0.42
6 Degree of Planning 89 88 0.69 0.65
7 Writing a Note 94 91 0.83 0.69
8 Overt Communication of Intent 83 80 0.61 0.54
9 Purpose of Attempt — — — — 1.00 1.00
10 Expectation Regarding Fatality — — — — 0.86 0.88
11 Concept of Lethality — — — — 0.89 0.87
12 Seriousness — — — — 1.00 1.00
13 Ambivalence to Living — — — — 0.72 0.74
14 Concept of Reversibility — — — — 0.89 0.88
15 Degree of Premeditation — — — — 1.00 1.00
Abbreviations:γ = Spearman Rank Correlation, ICC = intraclass correlation.
aamong 10 research team members;bamong 12 interviewers conducting the interviews
TABLE 2
Factor Structure of the Chinese SIS Among 592 Community Respondents with Deliberate Self Harm
Factor Loadings
Items Precautions Planning Seriousness
1 Isolation 0.77 0.26 0.41
2 Timing 0.75 0.22 0.40
3 Precautions Against Discovery 0.81 0.34 0.45
4 Act to Gain Help 0.67 0.13 0.33
5 Final Acts 0.31 0.87 0.57
6 Degree of Planning 0.42 0.73 0.59
7 Writing a Note 0.20 0.87 0.44
8 Overt Communication of Intent 0.10 0.40 0.50
9 Purpose of Attempt 0.45 0.43 0.80
10 Expectation Regarding Fatality 0.42 0.53 0.88
11 Concept of Lethality 0.46 0.54 0.84 12 Seriousness 0.48 0.51 0.95 13 Ambivalence to Living 0.48 0.43 0.89 14 Concept of Reversibility 0.45 0.36 0.73 15 Degree of Premeditation 0.42 0.69 0.76 Eigenvalue 1.44 1.05 7.31
Internal consistency (Cronbach’s alpha ) 0.74 0.73 0.89 Extraction Method: Principal Component Analysis.
Rotation Method: Oblimin (tau= 0). Cumulative variance= 92.9% Au: Please explain boldface
III, Seriousness, comprises items 8–15. They in participants with an education level of ju-nior high school (9 years) or lower and seju-nior can be treated as three subscales of the
Chi-nese SIS. high school or higher were 0.88 and 0.87 for
the total scale, 0.73 and 0.74, 0.72 and 0.75, and 0.89 and 0.87 for subscales Precautions, Internal Consistency
Planning, and Seriousness, respectively. The corresponding figures ranged from 0.85 to The Cronbach’s alpha coefficients for
the total SIS and the three subscales (Precau- 0.89, 0.68 to 0.77, 0.70 to 0.84, and 0.86 to 0.89 in subjects with ages≤20, 21 to 40, 41 tions, Planning, and Seriousness) among all
592 subjects were 0.88, 0.74, 0.73, and 0.89, to 60, and≥61, respectively. respectively (Table 2). The internal
consis-tency of the total and subscales of the Chi- Correlations among SIS and between SIS and CES-D
nese SIS did not differ between male and fe-male patients, between subjects with higher
and lower educational levels, or across the The correlations between the total scale and subscales of the Chinese SIS were four age groups. The Cronbach’s alpha
coef-ficients in men and women were 0.88 and high, ranging from 0.62 (Planning) to 0.94 (Seriousness), and were moderate among the 0.87 for the total scale, and were 0.74 and
0.73, 0.72 and 0.73, and 0.89 and 0.88 for 3 subscales, ranging from 0.27 to 0.44. The Seriousness subscale had the relatively high subscales Precautions, Planning, and
explaining about 70% of the total SIS score p < 0.05 by Bonferroni adjustment). The scores of the Precautions and Planning sub-variance. The correlations were low to
mod-erate between CES-D and the total (0.35) scales did not differ across the four age groups. The effect of age and gender on the and subscales of the Chinese SIS (0.19 for
Precautions, 0.26 for Planning, and 0.35 for Chinese SIS scores was further examined us-ing Mann-Whitney and Kruskal-Wallis test. Seriousness).
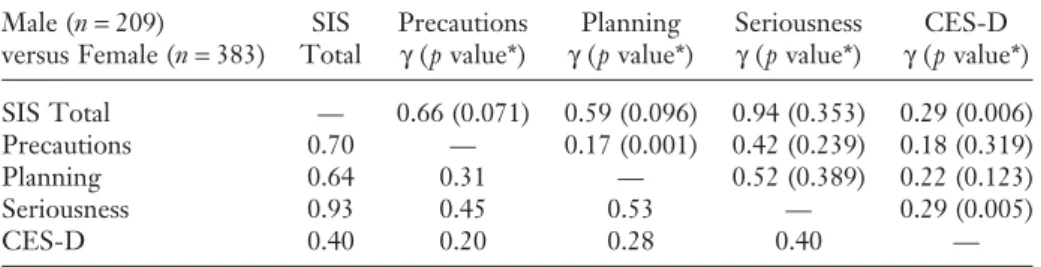
Table 3 lists the correlation coefficients The results were similar to those using the ANOVA (Table 4).
between the Chinese SIS and CES-D for males (upper right) and females (lower left). The patterns of correlations in males and
fe-males were largely similar to that observed in DISCUSSION the total sample with three exceptions.
Com-pared to their male counterparts, female re- Methodological Consideration spondents demonstrated significantly higher
correlations between the CES-D and the to- This is the first study to examine the psychometric properties of the SIS in a non-tal scale and Seriousness subscale of the
Chi-nese SIS and between the Precaution and Western country. The study includes a large representative sample of community respon-Planning subscales of the Chinese SIS.
dents with DSH, and major psychometric properties (inter-rater reliability, test-retest Gender and Age Effect
reliability, internal consistency, psycholin-guistic equivalence, construct validity, and Table 4 shows that gender and age
have significant effects on the total score of concurrent validity) have been examined with acceptable results. However, several limita-the Chinese SIS and limita-the score of limita-the
Serious-ness subscale. These two scores were signifi- tions in this study need to be taken into con-sideration while interpreting the findings. cantly higher in men than in women. There
was no gender difference in scores for both There is no follow-up information to exam-ine the predictive validity of the Chexam-inese SIS Precautions and Planning subscales. Among
the four age groups, these two scores were (Chien & Cheng, 1985; Mieczkowski et al., 1993). Without recruitment of control sub-significantly higher in the eldest (≥61) than
in the other three groups, particularly for jects, we cannot examine the discriminant va-lidity of the instrument between subjects scores of the Seriousness subscale (Adjusted
TABLE 3
Correlations Between the Chinese SIS and CES-D for Males (Upper Right) and Females (Lower Left) Among 592 Community Respondents with Deliberate Self Harm
Male (n= 209) SIS Precautions Planning Seriousness CES-D
versus Female (n= 383) Total γ (p value*) γ (p value*) γ (p value*) γ (p value*) SIS Total — 0.66 (0.071) 0.59 (0.096) 0.94 (0.353) 0.29 (0.006)
Precautions 0.70 — 0.17 (0.001) 0.42 (0.239) 0.18 (0.319)
Planning 0.64 0.31 — 0.52 (0.389) 0.22 (0.123)
Seriousness 0.93 0.45 0.53 — 0.29 (0.005)
CES-D 0.40 0.20 0.28 0.40 —
p value of 2-tailed zero correlation tests were all less than 0.001.
Abbreviations:γ = Spearman rank correlation coefficients, SIS = Suicide Intent Scale, CES-D= Center for Epidemiologic Studies-Depression Scale
*p value of differences of correlation coefficient test between male and female subjects in parenthesis.
TABLE 4 Mean Scores of the Chinese SIS by Gender and Age Groups Gender Age group Male Female pp Cohen <= 2 0 2 1–4 0 4 1–6 0 6 1+ p value Mean (SD )( N = 209) (N = 383) value a value b d (N = 60) (N = 295) (N = 171) (N = 66) value a SIS Total 10.05(6.22) 8.49(6.21) 0.004 0.004 0.25 7.78(5.69) 8.76(6.23) 9.02(6.44) 11.47(5.88) 0.004 0.005 Precautions 2.53(2.16) 2.27(2.11) 0.148 0.147 0.12 2.35(2.02) 2.25(2.15) 2.55(2.15) 2.55(2.08) 0.737 0.807 Planning 0.82(1.35) 0.74(1.30) 0.473 0.304 0.06 0.68(1.43) 0.79(1.31) 0.74(1.29) 0.82(1.32) 0.439 0.917 Seriousness 6.69(4.21) 5.48(4.23) <0.001 <0.001 0.29 4.75(3.56) 5.58(4.25) 6.03(4.30) 8.11(4.11) <0.001 <0.001 a One-way analysis of variance; b Mann-Whitney test; c Kruskal-Wallis test
with DSH and normal controls. The concur- iors in the English SIS (Spirito et al., 1996). Item 15 (degree of premeditation) included rent validity was only conducted with a
screening tool for depression (CES-D), and in the factor Planning Activities of the En-glish SIS (items 5, 6, & 15) loaded highest in the correlation between Chinese SIS and
le-thality of suicide methods used by respon- the factor Seriousness of the Chinese SIS. Item 7 (writing a note) and item 8 (overt dents was not examined.
Finally, without information about the communication of intent) excluded in the English SIS (Spirito et al., 1996) were as-psychiatric diagnosis of respondents, we were
not able to examine the association between signed to the factors Planning and Serious-ness of the Chinese SIS, respectively. We also diagnostic categories and the extent of
sui-cide intent. These limitations will be tackled found similar mean total scores of the Chi-nese and English SIS versions (Spirito et al., in our further studies of the Chinese SIS.
1996) among subjects with DSH. Reliability
Concurrent Validity Our findings showed that the ratings
The moderate correlations of SIS of the Chinese SIS were rather stable over
scores with measures of depression (Chance time for the self-report items and were not
et al., 1994; Minkoff et al., 1973; O’Brien et influenced by individual raters for the inter- al., 1987; Platt & Dyer, 1987; Silver et al., viewer-judged items with one exception:
se-1971) and hopelessness (Beck & Herman, lection of the timing for suicidal acts. The 1974; Platt & Dyer, 1987) in previous reports relatively lower agreement in “timing”
im-was replicated in this study. We have further plies that there is a need to improve the
judg-found a moderate correlation between the ment regarding whether subjects making
CES-D and two factors of the Chinese SIS DSH thought that their acts could be found
(Seriousness and Planning) and a low correla-or not. In contrast, “writing a note” had the
tion between CES-D and one Chinese SIS highest kappa coefficient as there was
objec-factor (Precaution). The low correlation with tive evidence about the presence/absence of “Precaution” might indicate that isolation wills or last words. The high internal
consis-behavior and prevention of discovery may be tency of the Chinese SIS was observed in less related to the severity of depressive both female and male respondents and across
symptoms. different age groups, regardless of
educa-tional levels. The high stability of the
Chi-Gender and Age Effect nese SIS indicates that changes in its score in
clinical studies can be well interpreted as due Our finding of a significantly stronger to intervention effects, rather than due to
suicidal intention in male subjects with DSH, random temporal fluctuations in scale scores. particularly in the seriousness dimension, than their female counterparts is consistent
Construct Validity with most previous studies (Diaz et al., 2003;
Hawton, 2000). However, no gender differ-ence in suicidal intention was reported in an Previous studies of the factor structure
of SIS in western populations identified two international study in Europe among suicide attempters (Hjelmeland et al., 2002). Con-to four facCon-tors (Diaz et al., 2003). Similar Con-to
a study with the English SIS (Silver et al., versely, our female respondents had a signifi-cantly higher correlation than their male 1971), this study found a three-factor
solu-tion with the Chinese SIS. Comparing these counterparts between the CES-D and the Chinese SIS. This may suggest that the in-two studies, exactly the same items 1–4
loaded high in the factor Precautions in the tensity of suicide intention is more related to depressive symptoms in women (Hesketh, Chinese SIS and the factor Isolation
Behav-Ding, & Jenkins, 2002), and early detection Implications and management of depression might be
more important for suicide prevention in the Results from this study have suggested that the Chinese SIS is a reliable and valid female population. For males, in addition to
depression, it might be crucial to identify instrument for assessing suicide intention in the Chinese populations. They might also other symptoms correlated with their suicide
intention for suicide prevention. Our finding suggest that the core phenomenon of suicide intent is likely to be culture-general across of a higher score of seriousness in suicide
in-tent among subjects older than 60 with DSH East and West. The Chinese SIS can be used in clinical settings and in community surveys indicates that more attention should be paid
to them, as a stronger suicide intent ascribe to assess the extent of suicide intent for its contribution to the risk of suicide and for sui-an increased risk for suicide in this group
(Suominen et al., 2004). cide prevention.
REFERENCES䉳
pression in Taiwan: Epidemiological survey utiliz-Astruc, B., Torres, S., Jollant, F.,
Jean-ing CES-D. Seishin Shinkeigaku Zasshi—Psychia-Baptiste, S., Castelnau, D., Malafosse, A., &
tria et Neurologia Japonica, 87, 335–338. Courtet, P. A. (2004). History of major
depres-Cohen J. (1988). Statistical power analysis for sive disorder influences intent to die in violent
the behavioral sciences (2nd ed.). Hillsdale, NJ: Law-suicide attempters. J Clin Psychiatry, 65, 690–695.
rence Earlbaum Associates. Beck, A. T., Beck, R., & Kovacs, M.
Diaz, F. J., Baca-Garcia, E., Diaz-Sastre, (1975). Classification of suicidal behaviors: I.
C., Garcia Resa, E., Blasco, H., Braquehais Quantifying intent and medical lethality. Am J
Conesa, D., et al. (2003). Dimensions of suicidal Psychiatry, 132, 285–287.
behavior according to patient reports. Eur Arch Beck, A. T., & Lester, D. (1976).
Compo-Psychiatry Clin Neurosci, 253, 197–202. nents of suicidal intent in completed and
at-Department of Health, Executive Yuan, tempted suicides. J Psychol, 92, 35–38.
Taiwan. (2006). Retrieved October 14, 2006, Beck, A. T. Schuyler, D., & Herman, I.
from http://www.doh.gov.tw/statistic/index.htm. (1974). Development of suicidal intent scales. In
Harriss, L., & Hawton, K. (2005). Sui-A.T. Beck & D.J. Lettieri (Eds.). The Prediction of
cidal intent in deliberate self-harm and the risk of Suicide. Bowie, MD: Charles Press.
suicide: The predictive power of the suicide intent Bertolote, J. M., & Leischman, F. A.
(2002). A global perspective in the epidemiology scale. J Affect Disord, 86, 225–233.
Haw, C., Hawton, K., Houston, K., & of suicide. Suicidologi, 7, 6–7.
Chance, S. E., Kaslow, N. J., & Baldwin, Townsend, E. (2003). Correlates of relative le-thality and suicidal intent among deliberate self-K. (1994). Anxiety and other predictors of severity
of suicidal intent in urban psychiatric inpatients. harm patients. Suicide Life Threat Behav, 33, 353– 364.
Hosp Community Psychiatry, 45, 716–718.
Cheng, A.T.A. (1995). Mental illness and Hawton, K. (2000). Sex and suicide. Gen-der differences in suicidal behaviour. Br J Psychia-suicide. A case-control study in east Taiwan. Arch
Gen Psychiatry, 52, 594–603. try, 177, 484–485.
Hesketh, T., Ding, Q. J., & Jenkins, R. Cheng, A.T.A., Chen, T. H., Chen, C. C.,
& Jenkins, R. (2000). Psychosocial and psychiatric (2002). Suicide ideation in Chinese adolescents. Soc Psychiatry Psychiatr Epidemiol, 37, 230–235. risk factors of suicide: A case-control
psychologi-cal autopsy study. Br J Psychiatry, 177, 360–365. Hjelmeland, H., Hawton, K., Nordvik, H., Bille-Brahe, U., De Leo, D., Fekete, S., et Cheng, A.T.A., Mann, A. H., & Chan, A.
(1997). Personality disorder and suicide: a case- al. (2002). Why people engage in parasuicide: A cross-cultural study of intentions. Suicide Life control study. Br J Psychiatry, 170, 441–446.
Cheng, A.T.A., & Lee, C. S. (2000). Sui- Threat Behav, 32, 380–393.
Hjelmeland, H., Stiles, T., Bille-Brahe, cide in Asia and the Far East. In K. Hawton ed.
The international handbook of suicide and attempted U., Ostamo, A., Renberg, E. S., & Wasserman, D. (1998). Parasuicide. The value of suicidal in-suicide. (pp. 29–48). Chichester, England: John Wiley
& Sons. tent and various motives as predictors of future suicidal behavior. Arch Suicide Res, 4, 209–225. Chien, C. P., & Cheng, T. A. (1985).
De-䉳Au: Pls
Kingsbury, S. J. (1993). Clinical compo- of early suicide in male high-risk suicide attempt-ers. Acta Psychiatr Scand, 113, 44–47.
nents of suicidal intent in adolescent overdose. J
Am Acad Child Adolesc Psychiatry, 32, 518–520. Silver, M. A., Bohnert, M., Beck, A. T., & Marcus, D. (1971). Relation of depression of Lo¨nnqvist, J., & Tolppanen, E.-M.
(1985). Outcome of attempted suicide. In P. attempted suicide and seriousness of intent. Arch Gen Psychiatry, 25, 573–576.
Pichot, P. Berner, R. Wolf, and K. Thau (Eds.).
Psychiatry—the state of the art (pp. 889–894). New Spirito, A., Sterling, C. M., Donaldson, D. L., & Arrigan, M. E. (1996). Factor analysis York: Plenum Press.
Mieczkowski, T. A., Sweeney, J. A., Haas, of the suicide intent scale with adolescent suicide attempters. J Pers Assess, 67, 90–101.
G. L., Junker, B. W., Brown, R. P., & Mann,
J. J. (1993). Factor composition of the Suicide In- Suokas, J., & Lonnqvist, J. (1991). Out-come of attempted suicide and psychiatric consul-tent Scale. Suicide Life Threat Behav, 23, 37–45.
Minkoff, K., Bergman, E., Beck, A. T., & tation: Risk factors and suicide mortality during a five-year follow-up. Acta Psychiatr Scand, 84, 545– Beck, R. (1973). Hopelessness, depression, and
at-tempted suicide. Am J Psychiatry, 130, 455–459. 549.
Suominen, K., Isometsa, E., Heila, H., NHS Centre for Reviews and
Dissemi-nation. (1998). Effective Health Care Bulletin: Lonnqvist, J., & Henriksson, M. (2002). Gen-eral hospital suicides—a psychological autopsy Deliberate self-harm. Effective Health Care, 4,
1–12. study in Finland. Gen Hosp Psychiatry, 24, 412–
416. O’Brien, G., Holton, A. R., Hurren, K.,
Watt, L., & Hassanyeh, F. (1987). Deliberate Suominen, K., Isometsa, E., Ostamo, A., & Lonnqvist, J. (2004). Level of suicidal intent self harm—correlates of suicidal intent and
sever-ity of depression. Acta Psychiatr Scand, 75, 474– predicts overall mortality and suicide after at-tempted suicide: A 12-year follow-up study. BMC 477.
O’Donnell, I., Farmer, R., & Catalan, J. Psychiatry, 4, 11.
Wang, L. J., Phillips, M., Huang, Z. J., (1996). Explaining suicide: The views of survivors
of serious suicide attempts. Br J Psychiatry, 168, Zhang, Y. P., Zhao, Y. X., & Yang, G. H. (2003). [Evaluation on the accuracy of reported suicides 780–786.
Pallis, D. J., Gibbons, J. S., & Pierce, in the Chinese population]. Zhonghua Liu Xing Bing Xue Za Zhi, 24, 889–892.
D. W. (1984). Estimating suicide risk among
at-tempted suicides. II. Efficiency of predictive scales Weissman, M. M., Sholomskas, D., Pottenger, M., Prusoff, B. A., & Locke, B. Z. after the attempt. Br J Psychiatry, 144, 139–148.
Pierce, D. W. (1981). The predictive vali- (1977). Assessing depressive symptoms in five psy-chiatric populations: A validation study. Am J Epi-dation of a suicide intent scale: A five year
follow-up. Br J Psychiatry, 139, 391–396. demiol, 106, 203–214.
Wetzel, R. D. (1976). Factor structure of Platt, S. D., & Dyer, J. A. (1987).
Psy-chological correlates of unemployment among Beck’s Suicide Intent Scale. Psychol Rep, 40, 295– 302.
male parasuicides in Edinburgh. Br J Psychiatry,
151, 27–32. Yip, P. S., Law, C. K., & Law, Y. W. (2003). Suicide in Hong Kong: Epidemiological Phillips, M. R., Yang, G., Zhang, Y.,
Wang, L., Ji, H., & Zhou, M. (2002). Risk factors profile and burden analysis, 1981 to 2001. Hong Kong Med J, 9, 419–426.
for suicide in China: A national case-control
psy-chological autopsy study. Lancet, 360, 1728–1736. Zhang, J., & Norvilitis, J. M. (2002). Measuring Chinese psychological well-being with Samuelsson, M., Jokinen, J., Nordstrom,
A. L., & Nordstrom, P. (2006). CSF 5-HIAA, Western developed instruments. J Pers Assess, 79, 492–511.