LANDMARK PROJECT – Annual Report
Project number: R001
Project title: Innovative Intensive Care Unit Family Service System
-Take National Cheng Kung University Hospital as an Example Submitting organization: Institute of Creative Industrial Design
Period covered: From 08/01/2009 to 07/31/2010 Grant amount: NTD 684,960
Grant utilized:NTD 678,995 Date of report:07/31/2010
Principal investigator and Co-PI’s names, titles and organizations:
PI Ding-Bang
Luh
Associate professor
Department of Industrial
Design
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS 1. Itemized goals of the project:
(1) To provide an overall and functional service system to assist the hospital to scheme the ICU patients’ families’ rest area, taking NCKU Hospital as the study subject.
(2) To build a product-service system for ICU patients’ families, which may bring low impact on the hospital and create high connectivity for patients and their families.
(3) To establish a Technology-Based Self-Service (TBSS) system for patient’s families of ICU by utilizing the technology to fulfill the needs of patients’ families.
(4) To build up a system to better meet the patient’s family’s physical and psychological needs. (5) To promote this service program and product service system to other hospitals.
2. Achieved ”Landmark” accomplishments directly related to this project and how it is compared to the state-of-the-art (no more than 750 words in total):
A special designed Product Service System (PSS) is developed as a customized personal system, which integrates the considerate rest unit and comprehensive Technology-Based Self-Service (TBSS). The system may fulfill the existing and future needs of the patients’ families by providing functional space, supportive equipments and various services. For the needs of environment, a multi-function rest unit is proposed as the product system, and the TBSS is adopted to be the service system to fulfill the information and assurance needs of ICU patients’ families. The combination of all systems provides a comfortable waiting unit that helps the families to feel at ease during the time of waiting.
To clearly illustrate the design concept of rest unit, a 1:10 scaled model was built. Utilize the semicircle at the end of the rest seat as a turn table for dining and reading. A semi-opened rest seat and curtain allow family members to decide the degree of openness and create privacy when needed. The designed rest unit includes a bed, three storage options, electric outlets, dividers, a TBSS screen, a table with reading light, a towel rack, and aisle light. The bed contains soft cushion, patients’ families can bring their own linens, pillows, and blankets. Various storage options include an open air strip underneath the bed for shoes and large packaged items, a pull-out drawer for miscellaneous items and a flip up storage space underneath the head board to place valuable items while sleeping to prevent overnight thief. Bedding and linens can be placed allowing a clear bed surface during the day. Electric outlets are designed in each seat for patients’ families to charge their electric equipment. Semi-open dividers are for privacy and ventilation. A touch pad screen is equipped in each unit for patients’ families to have technology-based self-service. A flip up table is installed with an inset reading light for reading or dining. A towel rack underneath the seat is provided for patients’ families to dry their towels. Aisle light is located on the ground to guide the patients’ families to the exit during the night when the overhead light is off. With the rest unit, ICU patients’ families can use it as a waiting space, rest space, discussion space, dining space and have
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
a comfortable stay.
A prototype of TBSS was constructed to present the complete services. The interface design of TBSS main menu is user friendly and understandable. Besides, the font size and button size are easily readable. Several icons and pictures are added to make the interface more attractive to the families. The color and design would provide families with peace and ease. The services of TBSS are developed based on the generalized needs. According to previous studies and investigation result, the needs of ICU patients’ families can be generalized to information and assurance dimensions, which form eight kinds of service options of TBSS, namely Hospital Related Information, ICU Related Information, ICU Patient’s Family Related Information, Living Information, Patient Nursing Information, Medical Information, Consultation Hotlines, and Religious and Spiritual Support. The services are conveyed through texts and pictures. Additionally, audio and video materials are also included to further consolidate the integrity of TBSS, especially for the services of instruction, religious and spiritual support. The design of rest unit for families provide a wider rest space, and more living-functioned equipments to support 3 to 7 days stay, besides, some relieved design elements are adopted, and the service option of TBSS also contains complete information and supportive material to assist patients’ families in facing the hard time.
Most of the existing ICU related studies focus on medical quality or needs of patients’ families, but a total solution to practically assist patients’ families is seldom seen. Few projects have
proposed improved plan for family service, such asCritical Care Family Assistance Program (CCFAP), which provides individual solution for different domains, an integrated and complete service for ICU patients’ families is lack and neglected. ICU family service system of this project adopted the concept of Product Service System, utilized a multi-function rest unit, user-friendly TBSS system to fulfill various needs of patients’ families at the same time, in other words, the system can be efficiently provided and managed than existing service.
Physical installation and usage evaluation.
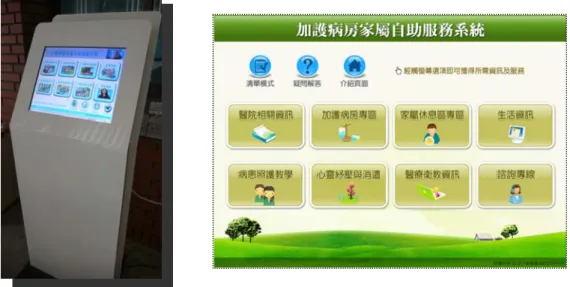
The information retrieve kiosk prototype “ICUinfo” has already completed in the end of the first year’s project. It was approved by NCKU Hospital for implementation and has been well installed in ICU family rest area since July, 2009. After system testing and promoting, its performance was evaluated. Since ICUinfo is Web-based system, an internet statistic tool was adopted to observe user behaviors and browsing rate of ICUinfo pages from November to December, 2009, to find out which pages are browsed more frequently. Result showed that patients’ families inclined to use “Religious and Spiritual Support” more frequently than other information related pages. The self-service can be more suitable to comfort and release patients’ families’ anxiety; while as for information needs, they would like to ask medical personnel for
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
immediate information feedback and uncertainty reduction. Since the services for assurance needs do not suit in public devices, a personal and comfortable using environment should be provided. The rest unit (FamilyAID) is built for this purpose to better meet patients’ families’ assurance needs, especially in Chinese culture society.
Filing a patent application
FamilyAID is a multi-functional rest unit that provides major living utilities with a personal information technology device (Table and Service on demand, TASOD), which has great potential to apply for invention patent. With the help from JEPAT International Patent and Trademark Office (展一國際專利商標事務所), an application was filed and currently in pending (“Multi-Functional Furniture for Sitting and Lying”, Taiwan invention patent, application no. 098135529, submission date:2009.10.21). This invention consists of three seat components with cushions capped on them and auxiliary seats on the bottom. These three seat components could be converted into different shapes for different purposes, working, sleeping, discussing, to name a few. A special information device is fixed to the middle seat, which contains a foldable stand and a power supply. Particularly, this device is expected to be equipped in other furniture for expanding applications.
Building a full-scaled prototype
“FamiliyAID” is designed for bring information life into ICU rest area for more convenience. In the first half year of our project, we did some detail modification of the function-oriented draft of FamilyAID, making it more aesthetic. Ten revised drafts were designed with different materials, seat tilts, color, etc. After extensive discussions, the final version was determined for further prototyping. According to the developed context map, a 3D model was built for clear illustration of the design concept. Accordingly, a full scaled FamilyAID prototype was built for testing. Virtual religion analysis
With the rapid expansion of internet use, all religions started to utilize internet as their means of religious communication and practices so that there are a variety of ways in which people can use the Internet to pursue and express their faith. The online applications of religion can be clustered into four main categories (Campbell, 2003): Online community (interactive online group discussions about religious topics), Religious cyber (churches, temples, mosques websites), E-mail list community (religious discussion through e-mail lists), and Online prayer and practice (members gather at a specific given time for praying and religious practices).
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
The above categories all feature with interaction, which can be viewed as the most valuable part of religion. “Service of Religious and Spiritual Support” of ICUinfo assembles articles, music or video to create peaceful atmosphere in the form of virtual pray room for calming down patients’ families’ anxieties, but this praying room only provides one-way information which lack of bidirectional communication. Therefore, this study refers to some “online interactive religion” applications to enrich virtual religion content in ICUinfo to provide more considerate supportive services. A research and analysis report about virtual religion has been done in the first halt of the second year. Accordingly, we can better understand the status of virtual religion and its development potentials, which could help improve the virtual praying room in development.
Figure 1 ICUinfo system and the web-based self-service interface.
Figure 2 FamilyAID and TASOD system (for working and for sleeping)
Questionnaire Survey
system in May, 2010, a questionnaire survey was conducted. A total of 68 responses (Table 1) were received. The result shows that a majority of them are their first time awaiting outside of ICU and that ICU information and nursing education are considered most important, and most respondents think that this system does provide the information one need, can satisfy one’s information need when medical personnel is busy, and an overall satisfaction and willingness to use the system again. It can be posited that the system can provide sufficient hospital-related information and reduce need for medical personnel while enhancing self-service.
Table 1 Descriptive statistics of the respondents
Gender Male:Female = 29:39
Under 20 21‐30 31‐40 41‐50 51‐60 61‐70 70Up Age
3 20 23 12 9 1 0
Marriage Married:Unmarried = 43:26
Primary school Junior High Vocational College Master Others Education
3 4 17 14 21 7 2
First time Second Third other(more than 3 times) Blank Times of
Waiting 36 13 9 8 2
1 Day 2 Days 3 Days 4 Days 5 Days 6 Days 1 week >1 week Others Days
awaited
45 7 3 1 0 1 1 6 4
Family Relative Friend Customer Others Relationship
46 10 7 1 3
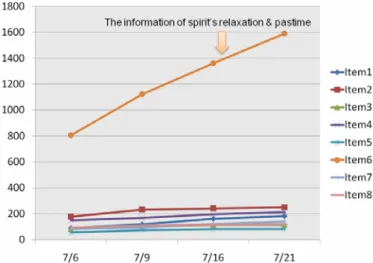
According to accumulated browsing frequency dated on July 21, 2010 (Figure 3), noticeably, the Information of Spiritual Relaxation & Pastime (1590 times) is far more than all of the rest. It can be asserted that Religious and Spiritual Support information is strongly needed by patients’ families. However, for medical and nursing information, they incline to go directly to medical personnel for professional opinions.
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
Extended development
Based on FamilyAID concept, an extended design is developed, namely Companion Furniture (ComFUR), which integrates all features of FamilyAID into a bed room device. It enables users, including disables and elderly, to design all functions they need, including
measuring pulse, taking medicines, lighting for reading, dining on bed, watching TV, working with computer, and so forth. Its full-scale prototype was made for testing b the public for a period of ten days in July 2010. A total of 131 subjects were invited. The result showed that the design is satisfactory with many implications. Interviews were also conducted for refinement suggestions. The new design was reviewed by patent expert and found with great potential for invention patents. An additional application was filed and currently in pending (“Multi- Functional Bedroom Device”, Taiwan invention patent, application no.099211902, dated on 2010.06.23).
Figure 4 Extended development ComFUR and subjects using ComFUR
Publications
Research findings were reorganized and submitted to international conferences. Currently, three international conferences were presented, one received the best paper award and another is cited by EI. Major findings of the previous two conference papers were integrated into one article for submission to the Journal of Nursing Research. It has been blind reviewed and currently in revision.
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS 3. Which items stated above are the best in the world, Asia, or Taiwan?
The services and environments for ICU patients’ families in nine major hospitals in Taiwan have been investigated in person. Most of the hospitals did not provide sufficient space, facility, and supportive services. E-Da Hospital is one exception, which equips bunk beds and facilities such as lockable storage and praying room for ICU patients’ families, on the other hand, out-sourced employees are hired to explain regulations and manage the environment. However, there are
several limitations in the rest area and services of E-Da Hospital, the bunk beds are inconvenient for elder families, facilities are insufficient for long stay, and the out-sourced employees are less professional.
According to the investigation for services of ICU patients’ families in other countries, the result indicated that most hospitals abroad provide similar families supportive services. In Japan, nurses have to provide reaffirmation for the families' constant expectation of the patients’ recovery, facilitate their realization that reliable medicine was available, ensure that various aids were easily accessible to them, and encourage their acceptance of long-term care (Sato Ogata, 2004). In Korea,
technology-based service has been infused into ICU service domain, an intelligent call center using Computer Telephony Integration (CTI) and agent technology was developed for sending messages to patients’ families of ICU efficiently and automatically through various communication media. With the service, patients’ families don’t have to stay outside the ICU every day. Instead, they can leave to work and come back when necessary (Han and Lee, 2001). In Australia, the concept of
family-focused nursing of ICU is highly concerned, such as information booklets, videos, visiting policies, waiting facilities and family support groups are suggested to provide for families (Coyer, et al., 2007). In London, the Family Liaison Service on Pediatric Intensive Care Unit (PICU) and Neonatal Intensive Care Unit (NICU) was proposed in 2003 to share the responsibility of medical personnel and assist the patients’ families. The Family Liaison Team comprises of three full-time equivalent sisters providing practical and emotional support to family members, and even bereavement services.
The ICU patients’ families’ care issue has been paid attention recently. Hospitals over the world start to plan relative projects for comforting these anxious families with loved-ones in intensive care units (ICUs), such as Japan, Korea, Australia, London, and USA. Among these projects, some bring up staff retraining suggestion to give families necessary support and consolation, and some propose message sending system idea so that patients’ families’ don’t have to stay there all day. USA is the leading nation to develop technology-based self services system.
In American, a multidisciplinary program that provides support for families and education to the health-care teams is now expanding across the country. The Critical Care Family Assistance Program (CCFAP), created by The CHEST Foundation and the Eli Lilly and Company Foundation,
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
was developed in 2001 to respond to the unmet needs of families of critically ill patients in hospital ICUs. Program elements include a computerized kiosk that provides information about specific diseases, hospital services, and the critical care environment; staff, pastoral, and social services; parking and wayfaring maps; and recommendations for local hotel accommodations and dining. Moreover, there is another company called CareNet which also provides a multimedia education and information product (ICU STAT GUIDE) to support families of intensive care patients. It is an information providing kiosk which features with opt-in text messages services which are delivered directly to the family spokesperson's registered mobile phone, offering their loved one's status, updating, delivering important notifications and requests. Similarly, ICU-USA.com is another website which is provided by ICU-USA, Inc and founded by doctors and nurses. It also provides information kiosks on site of hospitals and is designed for seated use which can easily be converted for use while standing.
Many hospitals around the world gradually pay attention to ICU patients’ families and modified waiting environment. This project refers to all these experiences and integrates them to build up ICU patients’ families’ service system. According to the service investigation conducted by our project, there are lacks of sufficient services about caring ICU patients’ families in Taiwan. Even in Asia or in the world, although similar projects (mentioned above) have brought up technology-based self service concept to build information kiosks, they emphasize mainly on information needs. The special virtual religion concept brought in ICUinfo makes our project more remarkable. It considers not only patients’ families’ information needs but also the assurance services which play important role in the critical time to release their anxieties. In addition, the rest unit design (FamilyAID and TASOD) and its extended development (ComFUR) are innovative and with great potential for industrial utilization. It can be concluded that the designed ICU family service system so far is the most comprehensive services system for ICU patients’ family in Taiwan, Asia, and the world.
4.Extramural funding currently active, applied or to be applied for supporting the work or related subjects stated above.
The prototypes of ICUinfo and FamilyAID have been officially presented to the doctors, nurses and decision making department of NCKU Hospital, they highly appreciated and acclaimed the accomplishment. Numerous assistance and abundant resource were provided by NCKU Hospital, such as arrangement of medical personnel interviews, allowance for patients’ families questionnaire interview, and several related documents for reference, which all supported the design of the intended system.
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
prototypes of FamilyAID and ComFUR have been demonstrated and tested by the public and received positive responses. They will be proposed to other hospitals for further development and collaboration. Moreover, we may also collaborate with some reputed religious institutes for enriching the content of virtual religion.
5. Utilization of grant for this year: (Units: Thousand NT Dollars; %)
Category Amount Spent %
Operational Fee
$ 678,995
99%Machine and Equipment
No Machine and Equipmentpurchased this year
0%
Total
$ 678,995
99%6. List names of faculty and researchers funded by this project and amount of support.
Ding-Bang Luh (eight hours per week) and Shiann-Far Kung (two hours per week)
7. Publications by faculty and researchers list above based on work supported by this grant (indicate impact factor, journal ranking and citation number):
(1) Luh, D.B., 2009, Design of Technology-Based Self-Service for ICU Patients Families, 2009 IEEE 10th International Conference on Computer-Aided Industrial Design and Conceptual Design, Zhejian University (25-29, November, Wengzho, China)
(2) Wu, M. H., Luh, D. B., and Kung S. F., 2009, A Technology-Based Self-Service for Intensive Care Unit Patients’ Families - National Cheng Kung University Hospital As an Example, 5th International Conference on Planning and Design, College of Planning and Design, National Cheng Kung University ( 25-29 May, Tainan, Taiwan). (Best paper award)
(3) Wang, K. Y, Wu, M. H., Yang, H. P., Luh, D. B. and Kung, S. F. ,2008, Innovative Intensive Care Unit Family Service System, 2008 International Service Innovation Design Conference, Dongseo
University (22, October, Busan, Korea), pp.263-275.
8. List of invited presentations by faculty and researchers shown in item 6: z Ding-Bang Luh and Shiann-Far Kung:
(1) Chiu, Y. H., Luh, D. B., and Kung S. F., 2008, Medical Tourism- The Innovation of Outsourcing Medicine, 2008 International Service Innovation Design Conference, Dongseo University (21, October, Busan, Korea), pp.98-107.
(2) Wang, Y. R., Luh, D. B., and Kung S. F., 2008, On Cultural Innovation for cultural Tourism in
Taiwan – an Initial Thought on Cultural Tourism Discourse and Practice, 2008 International Service Innovation Design Conference, Dongseo University (21, October, Busan, Korea), pp. 124-133. (3) Wu, S. C., Luh, D. B., and Kung S. F., 2008, Recycle Yourself – Organ Donation Contract Service
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
System, 2008 International Service Innovation Design Conference, Dongseo University (21, October, Busan, Korea), pp.134-141.
(4) Wang, Y. T., Kung S. F. and Luh, D. B., 2008, Creative Reuse and Service Design of Old Buildings, 2008 International Service Innovation Design Conference, Dongseo University (21, October, Busan, Korea), pp.214-221.
z Ding-Bang Luh:
(1) Luh, D.B., 2009, User-oriented design and innovation, 2009 IEEE 10th International Conference on Computer-Aided Industrial Design and Conceptual Design, Zhejian University (25-29,
November, Wengzho, China)
(2) Luh, D.B., 2009, Exhibition Design and Marketing, Southern Creative Living Association Alliance, Corporation Synergy Development Center. (9, November, Tainan, Taiwan)
(3) Luh, D.B., 2009, How do Taiwan's local characteristic industries to upgrade the industry attraction by the application of a new life industrial design aesthetics to? “The Development And Prospect Of Taiwan’s Local Characteristic Industries - To Master The Local DNA Of Charming Economic” International Conference, Corporation Synergy Development Center (3, November, Taiwan) (4) Luh, D.B., 2009, Resolving the Way of Traditional Industries Upgrading from the View of Product
Design, “Southern Traditional Industries Technological Caring Plan” Industrial Exchange Conference, Southern Taiwan Innovation Park. (18, September, Taiwan)
(5) Luh, D.B., 2009, Dialogue with Creation – Humor Product Design, a series learning activities of a multimedia “Joy, Colorfulness”, National Education Archive. (30, July, Taiwan)
(6) Luh, D.B., 2009, Living and Design, the Department of Fashion Design, Tainan Technology University. (3, July, Taiwan)
(7) Luh, D.B., 2009, Business-Oriented Design Process, Research and Development Center of Bicycle and Healthy Technology Industry (29, April, Taiwan)
(8) Luh, D.B., 2009, Creative Design in Culture Industry, R&D Center Cultural & Creative Industry of Communication University of China (24, April, Beijing, China)
(9) Luh, D.B., 2009, Reviewing and Prospects of Doctoral Education in Design, Tsinghua International Design Doctor Forum, Tsinghua University (23, April, Beijing, China)
(10) Luh, D.B., 2009, Product Design in Literature, Kaohsiung First University of Science and Technology, Mechanical and Automation Engineering and Industrial Design Institute (5, March, Taiwan)
(11) Luh, D.B., 2009, Design Research, National Yunlin University of Science and Technology Design Institute (25, February, Taiwan)
(1) Luh, D.B., 2009, A New Standard of Designers and their Cultivation, International Design Symposium, Japan Industrial Design Promotion Organization (29-30, January, Tokyo, Japan)
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
z Shiann-Far Kung:
(1) Kung, S. F. and C. S. Chen, 2008, “Healthy City Indicators, Settings Approach and Urban Planning – Methodological Thinking Based on Tainan Experience”, The Third Global Conference of the Alliance for Healthy Cities (23-26 October, Ichikawa).
(2) Kung, S. F. and C. W. Chen, 2008, “Adaptive and Innovative Development Planning in Southern Taiwan Science Park”, 2008 IASP-ASPA Joint Conference (22-24 October, Beijing).
(3) Kung, S. F., 2008,Discussion of Relation Between Development of University Campus and Change of Urban,「2008 Academic Conference of University in Taiwan and China」(18-19 October,
Hangzhou).
(4) Kung, S. F. and C. W. Chen, 2008, “Role of Science Parks in the Formation of High Technology Industrial Clusters – the Case of Southern Taiwan Science Park”, XXV IASP World Conference on Science & Technology Parks (14-17 September, Johannesburg).
(5) Kung, S. F. and Y. C. Yen, 2008, “The Planning Experience of TFT-LCD Industrial Cluster in Southern Taiwan Science Park”, XXV IASP World Conference on Science & Technology Parks (14-17 September, Johannesburg).
(6) Kung, S. F. and S. C. Hu, 2008, “Healthy City Tainan 2003-2007”, Planning for Healthy Cities – The International Symposium on Jinju Healthy City (25 January 2008, Jinju, Korea), pp. 21-37.
9. List all currently funded contracts and grants for PI and each faculty and researchers funded by the project shown in item 8.
z Shiann-Far Kung
Funded Project Name Position Period Covered
Grant Amount (10 thousands) Strengthened Using Plan for the Land of
Industrial Park
Principal Investigator
2008/01~
2008/12 450
Environment Conservation and Activation Plan for the Village Culture Heritage of Jiang Family
in Nanxi, Tainan County
Principal Investigator
2007/03~
2007/07 142.5
z Ding-Bang Luh
Funded Project Name Position Period Covered
Grant Amount (10 thousands) “LiWiArt arts teaching and learning platform”
Creative case implementation plan (the academic technology special program)
Principal Investigator &
Advisor
2009/12
The Status and Development Investigation Analysis of Creativity & Design Research Methods
Principal Investigator
2009/08
2009/12 20
Green Design of Public Bike Principal
Investigator
2009/09
2009/11 20
The User Identification Interface Accessible Design Study
- Bicycle Design as Example
Principal Investigator
2009/06
2009/11 20
Guagua Handy Gift and High Level Healthy Product Design
Principal Investigator
2008/07
2008/12 10
Buddhism Gift Design 97S-218
Principal Investigator
2008/07~
2009/02 19.6
Training of Ph.D Teaching Ability Program Adviser 2008/10~
2009/01 9.0
Research on Model of Design Knowledge Management -From a User’s Perspective
NSC 97-2221-E-006-162-MY2
Principal Investigator
2008/08~
2010/07 146.4
Overseas Cultivation Plan of Art and Design Elite Students Principal Investigator 2008/5~ 2009/4 1300 Cooking Class – Community-Oriented Innovation NSC 97-2218-E-006-012 Co-PI 2008/02~ 2009/01 29.4
Ubiquitous Bonding, Interaction and Intelligent Prototyping Design for Human Centered Digital
Life (HCDL) 96-EC-17-A-02-S1-024 Principal Investigator Of Sub-Project 6 2006/12~ 2009/11 97.4
10. Appendices (reprints of most important recent papers related to this project published by PI & Co-PIs)
M-H Wu, D-B Luh and S-F Kung (2009.11.27-29), "Design of Technology-Based Self-Service for ICU Patients’ Families", Proceedings 2009 IEEE 10th International Conference on Computer-Aided Industrial Design and Conceptual Design, IEEE Catalog Number: CFP0949B-CDR, ISBN 978-1-4244-5268-2, Nov. 27-29, IEEE Press, Zhejian, China, pp. 1965-1971.
Design of Technology-Based Self-Service for ICU Patients’
Families
Mu-Hsuan Wu 1, Ding-Bang Luh2, and Shiann-Far Kung 3 1
Institute of Creative Industry Design, National Cheng Kung University, Tainan, Taiwan 2
Department of Industrial Design, National Cheng Kung University, Tainan, Taiwan 3
Department of Urban Planning, National Cheng Kung University, Tainan, Taiwan
Caring in intensive care unit (ICU) is taken seriously in the whole medical process. Past research usually focused on satisfying ICU patients or medical personnel’s needs, requirements of patients’ families were often been ignored. To establish “CarePlus” - a comprehensive technology-based self-service (TBSS) for ICU patients’ families - is the objective of this research. Based on the finding through literature review and investigation on needs of patients’ families, design of services were developed, which include Hospital Related Information, ICU Related Information, ICU Patient’s Family Related Information, Living Information, Patient Nursing Information, Medical Information, Consultation Hotlines, Religious and Spiritual Support. ICU of NCKU Hospital was employed for evaluation, where target subject tested the dedicated TBSS and their feedbacks were analyzed quantitatively. The result indicates that patients’ families show high affirmation toward CarePlus, and their need gaps will be reduced after trying this service.
Keywords: Technology-Based Self-Service, ICU patients’ families, Service Design, Technology Design
I. INTRODUCTION
P
atients’ families play important roles in supporting the patients to face the hard time, so it is
important to maintain the equilibrium of the patients’ families under the crisis [Leung et al.,
2000]. A thorough observation has been done for eight major hospitals in Taiwan to find out
current environment and service providing for ICU patient’s families, the findings show that
almost all of the hospitals currently do not provide needed space, facility and service for ICU
patients’ families. As a result, providing necessary help for ICU patients’ families has overall
advantages and should be promoted to every hospital. Technology-based self-service
(hereinafter as “TBSS”) is usually adopted by companies for supporting insufficient labor,
increasing customers’ satisfaction and saving operation cost. Those services have already been
implemented in many industries; fewer cases focus on designing specific TBSS for patients’
families to provide them with needed and related services in Taiwan.
In the United States, American College of Chest Physicians-Critical Care Institute developed
a program, the Critical Care Family Assistance Program [2001], which aims at supporting the
families of the critically ill patients with a complete support by providing TBSS. The program
has been promoted to eight hospitals in the United States for several years, and the feedbacks
from all the hospitals were highly positive. However, the successful TBSS adopted by the
hospitals in the United States for western people are not completely suitable for Chinese
patients’ families. Hence, a comprehensive TBSS specially designed for ICU patients’ families
in Taiwan should be considered. To ICU patients’ families, they can easily acquire needed
information and supporting services through the TBSS at anytime. To medical personnel in ICU,
the TBSS should be able to answer routine questions and offer basic information for families,
which allows them to pay more attention to the patients. This study therefore tries to design and
establish a TBSS for ICU patients’ families in Taiwan. According to the background and
motivation above, the objectives of this study can be divided into three points:
(1) To analyze and integrate the needs of ICU patients families, particularly southern Taiwanese.
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
(2) To develop an innovative TBSS for ICU patients’ families
(3) To introduce a TBSS for patients’ families in National Cheng Kung University (NCKU)
Hospital and to evaluate the TBSS design for future improvement.
II. TECHNOLOGY-BASEDSELF-SERVICE
Technology-Base Self-Service (TBSS) was defined by Meuter et al. [2000] as a technological
interface that enables customers to produce a service independently without direct service
employee involvement. It allows customers to do for themselves and provide their own service.
Bitner et al. [2002] stated that a customer-focused design of technology and process are critical
for a successful TBSS. Through an overall needs investigation, the service can be
comprehensive and satisfactory to the customers’ needs.
Service design problem refers that TBSS does not response as the expected function [Meuter
et al., 2000]. On the other hand, technology performs in a way that users are unhappy with the
encounter can be described as technology design problem [Meuter et al., 2000], which relates to
system design and interface design. Interface is a visible software which can be used by users to
interact with computers [Weinschenk, et al., 1997], while system design refers to the
information system which can organize designed system and process the command. Information
kiosk is one kind of self service technology station with interactive information processing
capacity, and located in a public concourse [Rowley, et al., 2007], which is commonly used by
people. In recent years, many companies started to adopt networked TBSS. The web-based
system is able to create an information system for electronic publishing and the provision of
information service, and the system can be accessed and used by everyone [Grize, et al. 1997].
Though this convenient and efficient TBSS is wildly adopted in various industries, a specialized
TBSS for ICU patients’ families is still under development. Therefore this study tries to utilize
kiosk technology to design a considerate TBSS for ICU patients’ families.
III. NEEDSOFICUPATIENTS’FAMILIES
General needs
Intensive care unit (ICU) also named as critical care unit (CCU), is a special medical unit
which collects human support and material resource to provide 24 hours enhanced medical care
[Lin, 2002]. In 1979, the study of Molter was the first to focus on the needs of relatives of
critically ill patients. Several researches were built on the contribution of Molter and proposed a
45-item needs self-report scale for ICU patients’ families, which termed Critical Care Family
Needs Inventory (CCFNI). In 1991, Leske clarified the CCFNI and grouped the 45-item
questionnaire into five domains of need, those are support, comfort, proximity, information, and
assurance, and Bryan et al. [1998] has indicated five categories to depict the needs of ICU
patients’ families: “Assurance,” the need to feel hope for a desired outcome; “Information,” the
need for consistent, realistic, and timely information; “Proximity,” the need for personal contact,
and to stay physically and emotionally with the patient; “Support,” the need for resources,
support systems, and ventilation, and; “Comfort,” the need for family members’ personal
comfort.
Studies by various scholars indicate that the needs of Chinese ICU patients’ families
distinguish from different cultures. Lederer et al. [2007] analyzed the inclinations for Chinese
Families and Westerner Families. In China, the need for assurance and information were
strongly expressed by family members, moreover, the importance of need for hope was
intensified by the families of Chinese culture than of Western culture. Therefore, the
requirements of Chinese ICU patients’ families can be generalized to information needs and
assurance needs, and which could be further inferred to the needs of ICU patients’ families in
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
Taiwan.
Information needs
The information need is addressed by both Chinese and Western ICU patients’ families. As
Halme [1990] mentioned, providing continuous and consistent information for patients’ family
members can significantly reduce the anxiety. Furthermore, Azoulay et al. [2002] found out that
the providing information effectively to family members would affect their comprehension and
satisfaction. Dowling et al. [2005] stated that in order to improve communication, some specific
information should be emphasized and provided, which are listed below:
(1) Educational Information: the information of medical procedures or treatments that usually
be observed in ICU or the information on specific diseases or medical conditions of patients.
(2) Anticipatory Information: the information which medical personnel have anticipated
patients’ families will want to have under a panic circumstance and unfamiliar environment,
such as area restaurants, transportation services, hotels, other community resources, and
specific policies and procedures related to the ICU.
(3) Reinforcement Information: reinforcement information is provided after families conference
with the medical personnel or ICU team, which would be supportive to the information
received in the conference.
(4) Contact Information: the information that contains the picture, name, and contact
information of ICU medical personnel, which is usually provided by business cards or listing
on the bulletin board.
Dowling and Lederer [2007] also introduced other needed information for ICU patient’s
families, which are local city information, including restaurants, local events, day care centers,
respite care information, health clubs, maps etc. A wide variety of additional practical
information, such as advanced medical directions, tutorials on home care equipment displayed
by streaming video and subtitles, and information about the hospital which contains pictures and
biographic summaries of critical care team members.
Assurance needs
The need of assurance is the need to feel hope for a desired outcome. Ruppert et al. [1996]
has issued that promotion of realistic hope to ICU patients’ families is an important intervention
to provide the need of assurance. In addition, according to the study of Leung et al. [2000], the
strong belief of Chinese ICU patients’ families about external forces such as luck, fate, chance,
and strong values in the Buddhist and Taoist traditions would be further explained as a need for
maintaining hope and seeking assurance. According to the study of Patel [1996], hope-inspiring
strategies for ICU patients’ families include spiritual/ religious activities, support from
significant others, positive relationship with caregivers, devotion (for patient), optimistic attitude,
physical presence at the bedside, talking to others, and distraction mechanisms. Among those
strategies, spiritual and religious activities were identified as the most essential hope inspiring
strategies. The hope could encourage and help individuals to deal with the crisis, and further
support the patients to go through the critical condition and recover smoothly.
Needs in southern Taiwan
A thorough and comprehensive needs investigation was conducted to clarify specific information and assurance needs of ICU patients’ families in southern Taiwan. According to related studies and actual observations, a semi-structured questionnaire was developed to carry out in-depth interviews with 30 patients’ families and a total of 33 ICU medical personnel (surgical 18, medical 15) of NCKU hospital. The questionnaire contained various need options, separating into two major parts, information need item and assurance need item. Each item was answered by 5-point Likert-type scale: -2 (very disagree), -1 (disagree), 0 (no opinion), 1 (agree), 2 (very agree). By calculating the score of each need option, the one obtained higher score represented that it was perceived more important by patients’ families and medical personnel. The results from questionnaires of patients’ families and medical personnel would be added to gain the top 5 essential
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS information needs and assurance needs of ICU patients’ families (Table 1).
According to the survey, needs for consultation and medical nursing information can be seen as the most needed information, the relief materials and spiritual supports as the most important assurance needs.
Table 1
Top 5 important needs of ICU patients’ families
Rank Information needs Rank Assurance needs
1 Information of consultation service 1 Psychology consultation service 2 Lecture of spiritual support
3 Pressure relief service 2*
3* 4 *
Information of professional home caring consultation Information of rehabilitation instruction
Information of medical lecture 4 Reading material 5 Information of funeral and
burial consultation service
5 Pressure relief music * no ranking difference among these 3 information needs
IV. CAREPLUS –THEDESIGNEDTBSS
According to previous findings and analyses, the design of TBSS for ICU patients’ families
can be discussed in two dimensions, namely service design and technology design. The
development of service design should be based on the needs of ICU patients’ families, which is
separated to information needs and assurance needs. To confirm the information and assurance
needs, a thorough needs investigation was conducted to patients’ families and medical personnel
in ICU of NCKU hospital. Technology design has to consider interface design and system
design of TBSS. Some general interface design guidelines were analyzed and existing systems
used in various hospitals were investigated, hence the system could be easily adopted and
updated. For easy discussion, the proposed TBSS for ICU patients’ families is called as
“CarePlus” hereinafter.
Service design
Previous studies indicate that the needs of information and assurance are the most
important needs perceived by ICU patients’ families in Chinese societies. According to the
literature review and investigation outcome, generalized needs can be further developed into
eight service options, namely Hospital Related Information, ICU Related Information, ICU
Patient’s Family Related Information, Living Information, Patient Nursing Information, Medical
Information, Consultation Hotlines, and Religious and Spiritual Support. Related services would
be included in the options. (Table 2)
For the services of Hospital Related Information, ICU Related Information, and ICU Patient’s
Family Related Information, environment introduction, visitation procedure and relevant
regulation are provided to help families who wait outside of ICU the first time to be familiar
with the area and direction quickly. The service of Living Information collects information of
restaurants, hotels and transportation around the hospitals for daily needs of families. Patient
Nursing Information and Medical Information services integrate professional nursing and
common medical information, with the basic knowledge and further understanding, medical
personnel can instruct and communicate with patients’ families easily. Consultation Hotlines is
provided with organized information of various services, such as insurance, home caring,
psychologist and funeral arrangement, which can help patients’ families to acquire supportive
services immediately. Service of Religious and Spiritual Support assembles articles, music or
video of encouragement and confidence for patients’ families to deal with despair and
uncertainty, and entertainment channels are provided for long stay families for distraction and
recreation.
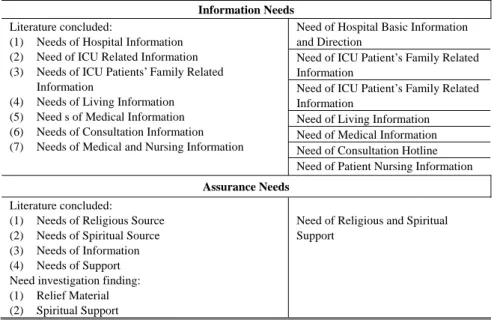
Table 2
Generalized needs of ICU patient’s families Needs from literature Review and Investigation Result Generalized Needs
Information Needs
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
Need of Hospital Basic Information and Direction
Literature concluded:
(1) Needs of Hospital Information (2) Need of ICU Related Information (3) Needs of ICU Patients’ Family Related
Information
(4) Needs of Living Information (5) Need s of Medical Information (6) Needs of Consultation Information (7) Needs of Medical and Nursing Information
Need of ICU Patient’s Family Related Information
Need of ICU Patient’s Family Related Information
Need of Living Information Need of Medical Information Need of Consultation Hotline Need of Patient Nursing Information Assurance Needs
Literature concluded:
(1) Needs of Religious Source (2) Needs of Spiritual Source (3) Needs of Information (4) Needs of Support Need investigation finding: (1) Relief Material (2) Spiritual Support
Need of Religious and Spiritual Support
Technology design
The technology design contains two dimensions, one is interface design, and the other is
system design. The following will focus on the interface design of CarePlus first and then come
to the system development.
According to the needed services, a main menu prototype was constructed to illustrate the
interface design of CarePlus (Figure 1). According to the guidelines proposed by Maguire
[1999], the interface design of TBSS main menu should be user friendly and understandable.
Besides, the font size and button size are easily readable. Properly designed icons and pictures
are added to make the interface more attractive to the families.
To establish a web-based kiosk, HTML is adopted to build up the system. HTML is the
abbreviation of Hyper Text Markup Language, which is used to create documents on the World
Wide Web, incorporating text, graphics, sound, video, and hyperlinks (Weberster). HTML is
written in the form of tags, surrounded by angle brackets, can also describe some degree,
appearance and semantics of a document, and can include embedded scripting language code
(such as JavaScript). The system design of CarePlus is based on a web-site concept, a click by
intuition can bring the patients’ families needed service, which makes the innovative system
easily accepted by general public effortlessly. For instance, a
Fig. 1 Designed interface of CarePlus (English version)
services are conveyed through texts and pictures.Audio and video materials are included to
consolidate the integrity, especially for the services of instruction, religious and spiritual support.
For families with different religions, the contents include not only Eastern religions but also
Western religions, which can be easily changed and more details should be provided. Such
design can provide one with any religion a dedicated space for spiritual relief.
Fig. 2 Pages of Religion service (English version)
V. EVALUATIONOFCAREPLUS
As a representative hospital in southern Taiwan, National Cheng Kung University Hospital was chosen to be the place to evaluate the service system for ICU patients’ families. A CarePlus prototype was built to demonstrate the service system concept.
Evaluation process and tool
Two sets of questionnaires were designed for investigation, which are questionnaire A (QA),
given before using CarePlus, and questionnaire B (QB), given after briefing on CarePlus and
using. QA aims at recognizing the needs satisfaction of ICU patients’ families before using the
service system and is based on the concept of Leske’s [1991] CCFNI(Critical Care Family
Needs Inventory), which is a well-developed needs inventory consisting of 45 questions to
assess the needs of ICU patients’ families. QA has two elements, one for the needs satisfaction
assessment of existing services, and another for collecting basic demographic data.
QB is used to assess the conversion of the needs satisfaction condition after ICU patients’
families tried CarePlus. It also consists of two components, the first one is identical to the first
part of QA, of which goal is for comparison analysis on needs satisfaction before and after using
the new service system. Since the services of CarePlus were developed from the needs of
patients’ families, the comparison of needs satisfaction conversion would refer to if the designed
CarePlus can fulfill their information and assurance needs, which also indicates the performance
of service design. The second part is for evaluation of the technology design of CarePlus, of
which questions were generated from Dabholkar’s attribute-based model [1996], which contains
five dimensions, including speed of delivery, ease of use, reliability, enjoyment and control.
These dimensions provide a complete evaluation framework for interface and system designs.
Questionnaire A : Needs satisfaction assessment of existing service I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS Comparison analysis to assess the conversion of need satisfaction Questionnaire B :
Needs satisfaction assessment after trying CarePlus
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
Fig. 3 The simplified research design
Both sets of questionnaires were rated on a 5-point Likert-type scale: -2 (very disagree), -1 (disagree), 0 (no opinion), 1 (agree), 2 (very agree), and demographic questions were provided with multiple choices. Standard Package for the Social Sciences Program (SPSS) was adopted for analysis. Group mean and ANOVA (T-Test) would be applied for measuring.
Evaluation results
A total of 30 effective samples from 30 families answered the questionnaires. Most of them are female (73%), and the largest age group is between 21~30 years old (40%), the second is 41~50 years old (33.3%). Up to 40% of the patients’ families received high school education. Some families were the first time to wait outside of the ICU (53.3%). Almost half of the samples have stayed outside of the ICU for 2~7 days (46.7%). Nearly half of the samples are the children of the patients. Families who had experience of using other TBSS is 53.3%.
The Cronbach’s alpha coefficient of QA (0.9412) and of QB (0.9205) both exceeded the minimum reliability standard of 0.70, which showed high internal consistency. For survey of needs satisfaction before and after using CarePlus, mean scores of both QA and QB were reckoned. (Table 3) Mean scores of QA reveal that almost all of the needs of ICU patients’ families are unsatisfactory. The top 3 unsatisfied needs were “Contact the specific medical personnel” (-0.73); “Have a positive think” (-0.47) and “Realize what kind of medical personnel can provide what kind of information” (-0.47). The average mean scores of QB showed a positive conversion of 1.10 that CarePlus service can help increase the needs satisfaction of the patients’ families. The dimensions improved most are “Understand the medical condition of patient in detail” (1.40); “After reviewing related information, I can assist to take care of patient” (1.33) and; “Have introduction of ICU environment at first time entering ICU” (1.27).
Table 3
Mean Score of Questionnaires A and B (N=30; scoring range: -2, 2)
No Item Mean of
QA
Mean of QB
1 Contact the specific medical personnel -0.73 1.13
2 Have a positive thinking -0.47 1.00
3 Realize what kind of medical personnel can provide what kind of information -0.47 1.00 4 Obtain related information of ICU medical personnel -0.40 1.07 5 Be informed who can assist to solve the problem -0.40 0.93 6 Have introduction of ICU environment at first time entering ICU -0.27 1.27 7 After reviewing related information, I can assist to take care of patient -0.27 1.33 8 Obtain illustration of what should do in the bedside -0.20 1.00 9 Assure that the patient is under the best caring in ICU 0.13 1.07 10 Understand the medical condition of patient in detail -0.07 1.40
11 Obtain the understandable explanation 0.07 1.07
12 Understand the expected outcome of patient 0.07 0.93
13 Understand the medical treatment of patient 0.40 1.20 14 Understand why the patient took the kind of medical treatment 0.53 1.00
Average mean score -0.15 1.10
The comparison evaluation of needs satisfaction before using and after using CarePlus would be analyzed by ANOVA (T-Test), the assumptions are: H0: there is no difference, and H1: there is a difference. According the analysis (Table 4), the P-value of all questions is less than 0.05, which refers to that H0 is eliminated. The result shows the needs satisfaction of ICU patients’ families changed significantly after using CarePlus, particularly in five aspects: (1) Contact the specific medical personnel; (2) After reviewing related information, I can assist to take care of patient; (3) Have introduction of ICU environment at first time entering ICU; (4) Obtain related information of ICU medical personnel and (5) Be informed who can assist to solve the problem. These are the dimensions which have the remarkable difference.
The evaluation result of the technology design (Table 5) indicates that the patients’ families
had a positive feedback to the technology design of CarePlus. Especially, the dimension of easy
to use, of which related items are “ TBSS is simple and easy” , “TBSS operation needs less
mental and physical effort”, gains a positive mean score (1.4), and shows that most of the
families considered CarePlus can be operated and learned easily. Beside, the other four
dimensions, “speed of delivery”, “reliability”, “enjoyment” and “control”, all have agreeable
performance, which illustrates the technology design of CarePlus is favorable.
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
gained positive feedbacks. The patients’ families would increase their satisfaction after using the designed service system.
Table 4
Comparison analysis of needs satisfaction before using and after using CarePlus (N=30)
Item Mean StD T P
Contact the specific medical personnel 1.867 0.730 14.0 0.000
After reviewing related information, I can assist to take care of patient 1.600 1.276 6.87 0.000 Have introduction of ICU environment at first time entering ICU
1.533 1.224 6.86 0.000
Be informed who can assist to solve the problem 1.400 1.221 6.28 0.000 Obtain related information of ICU medical personnel 1.467 1.280 6.28 0.000 Realize what kind of medical personnel can provide what kind of information
1.467 1.330 6.03 0.000
Obtain illustration of what should do in the bedside
1.200 1.126 5.83 0.000
Obtain the understandable explanation 1.000 1.114 4.92 0.000
Understand the expected outcome of patient 0.867 1.042 4.56 0.000
Have a positive thinking 1.067 1.311 4.46 0.000
Understand the medical condition of patient in detail
0.800 1.186 3.69 0.001
Understand the medical treatment of patient 0.800 1.243 3.53 0.001 Assure that the patient is under the best caring in ICU 0.933 1.596 3.20 0.003 Understand why the patient took the kind of medical treatment 0.467 1.224 2.09 0.046
Table 5
Mean Score of technology design survey (N=30; scoring range: -2, 2)
Item Mean Score
TBSS can provide the service for me in a short time 1.27
TBSS can response fast 1.20
TBSS is simple and easy 1.40
TBSS operation needs less mental and physical effort 1.40
TBSS operation is smooth and precise 1.40
TBSS operation outcome is reliable 1.27
TBSS service quality is positive 1.33
I like to use the TBSS 1.27
I think it is interesting to use the TBSS 1.13
I can control the operation and process of the TBSS 1.27
I can control the outcome of the TBSS 1.13
In addition to above analyses, there is one more appreciated service comparing to the Critical Care Family Assistance Program in America. Religion services are set based on the assurance needs, which provide spiritual support by constructing a few virtual praying rooms for various religions. This virtual religions praying room might be first seen in the world. Through this consideration, CarePlus is surely more comprehensive and innovative than similar TBSS abroad.
CONCLUSIONANDSUGGESTION
From above discussions, the following conclusions and suggestions can be drawn:
(1) Needs of ICU patients’ families in southern Taiwan: The most important needs of Chinese
ICU patients’ families are information needs and assurance needs. The top five most
essential and urgent information needs of ICU patients’ families are information of
consultation service, rehabilitation instruction, medical lecture, professional home caring
consultation, and funeral and burial consultation. The top five most important assurance
needs are psychological consultation service, lecture of spiritual support, pressure relief
service, reading material, and pressure relief music.
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
(2) Current service for ICU patients’ families in most hospitals: Most hospitals in Taiwan do
not provide basic and necessary services or space for ICU patients’ families. The survey
shows more than half of the ICU patients’ families would stay overnight to accompany
with the patients, and most of the ICU patients’ families are in fact asked by doctors to wait
for 24 hours in case of accidence of the patients. Providing considerate services for ICU
patients’ families is not only a helpful solution for ICU patients’ families but also a
necessary mission of hospitals.
(3) Design of TBSS for ICU patients’ families: Both service design and technology design are
essential. Eight services are developed based on the users needs. A significant difference of
needs satisfaction before and after using CarePlus indicates that the service design is
appreciated by target users. A remarkable positive feedback can be seen in the assessment
of technology design, showing that both service design and technology design are well
constructed and being satisfied with target users. By utilizing pressure relief resource and
psychology support materials, CarePlus can be embedded into personal TBSS in the near
future, providing a peaceful and hopeful atmosphere for the stressed patients’ families,
catering to individual religious need.
(4) Survey tools and evaluation results: Based on the concept of CCFNI and Attribute-Based
Model, survey tools tailored to test service design and technology design respectively are
proposed and useful.
(5) Development of value added service, a win-win strategy for both patients’ families and
hospital: Patients’ families can rely on CarePlus for assistance and solution. With a
supervised mechanism, hospital can select qualified advertisers (e.g. legitimate
home-caring service providers, near restaurants, funeral consulting agents, to name a few
qualified service suppliers) and promote to patients’ families by displaying the
advertisement on CarePlus. CarePlus can not only assist ICU patients’ families, but also
bring hospital additional benefit, which makes CarePlus more valuable.
(6) The unique service in Taiwan and the world: In Taiwan and to the best knowledge of the
authors, no similar TBSS service for ICU patients’ families has been found yet. The
proposed CarePlus can easily substitute for existing services which are insufficient and less
organized in many aspects. Moreover, the proposed service is more comprehensive and
innovative than the similar service abroad.
ACKNOWLEDGMENT
This research is partially supported by the Landmark Program of National Cheng Kung
University Top University Project (R001). Special thanks to project assistant, Jie Jiang, who
helped edit and revise this article for submission. Appreciations to Georgia Wang and Hsin-Pei
Yang who helped conduct preliminary research.
REFERENCES
[1] Anitsal, I., Flint, D. J. 2005. "Exploring customers' perceptions in creating and delivering value: technology-based self-service as an illustration." Services Marketing Quarterly 27(1): 57-72.
[2] Azoulay, elie, F. P., Sylvie Chevret, Merce Jourdain, Caroline Bornstain, Anne Wernet, D. A. Isabelle Cattaneo, FRreferic Brun, Pierre-Edouard Bollaert, Jean-Ralph Zahar, et al. (2002). "Impact of a Family Information Leaflet on Effectiveness of Information Provided to Family Members of Intensive Care Unit Patients." American Journal of Respiratory and Critical Care Medicine 165: 438–442.
[3] Bitner, Mary Jo.1995. “Building Service Relationships: It’s All About Promises.” Journal of the Academy of Marketing Science 23 (4): 246-251.
[4] Bitner, M. J., Brown, Stephen W. and Meuter, Matthew L. 2000. "Technology Infusion in Service Encounters." Journal of the Academy of Marketing Science 28(138): 138-149.
[5] Bitner, M. J., Ostrom, Amy L., Meuter, Matthew L. 2002. "Implementing successful self-service technologies." Academy of Management Executive 16(4): 96-108.
[6] Dabholkar, Pratibha A., 1991, “Using Technology-Based Self-Service Options to Improve Perceived Service Quality.” In AMA Summer Educator’s Conference Proceedings. Eds. Mary C. Gilly, ThomasW. Leigh, Marsha L. Richins, AlladiVenkatesh, Roby Roy Dholakia, F. Robert Dwyer, Alan J. Dubinsky, David Curry, Masaaki Kotabe, and Gerald E. Hills. Chicago: American Marketing Association,
I. ANNUAL REPORT FOR NCKU LANDMARK PROJECTS
534-535.
[7] Dabholkar, P. A. 1996. "Consumer evaluations of new technology-based self-service options: An investigation of alternative models of service quality." International Journal of Research in Marketing 13(1): 29-51.
[8] Dabholkar, P. A., L. M. Bobbitt, et al. 2003. "Understanding consumer motivation and behavior related to self-scanning in retailing." International Journal of Service Industry Management 14(1): 59.
[9] Dowling, J. and W. Baofeng, 2007, "Impact on Family Satisfaction: The Critical Care Family Assistance Program." Chest 128(3): 76S-80S.
[10] Halme,M. A. , 1990, “Effects of support groups on anxiety of family members during critical illness”. Heart and Lung 19(1): 62-70 [11] Leung, K.-K., Chien, Wai-Tong, Mackenzie, Ann E., 2000, "Needs of Chinese Families of Critically Ill Patients " Western Journal of
Nursing Research 22(7): 826-840.
[12] Maguire, M. C., 1999, "Review of user-interface design guidelines for public information kiosk systems." International Journal of Human-Computers Studies in Hong Kong." Journal of Clinical Nursing 9: 46-54.
[13] Meuter, M. L., A. L. Ostrom, et al. (2000). "Self-Service Technologies: Understanding Customer Satisfaction with Technology-Based Service Encounters." Journal of Marketing 64(3): 50-64.
[14] Molter, N. C. (1979). "Needs of relatives of critically ill patients: a descriptive study." Heart & Lung: The Journal Of Critical Care 8(2): 332-339
[15] Patel, C. T. (1996). "Hope-inspiring strategies of spouses of critically ill adults." Journal Of Holistic Nursing: Official Journal Of The American Holistic Nurses' Association 14(1): 44-65.
[16] Rowley, J., Slack, Frances (2007). "Information Kiosks: A Taxonomy." Journal of Documentation 63(6): 879-897. [17] Weinschenk, S. & Jamar, P. & Yeo, S. C. (1997). GUI design essentials, New York: Wiley Computer Publishing.
[18] 林玉如(Yeu-Ru Lin) “成人加護病房病患家屬之壓力感受與因應策略之探討"(Perceived Stress and Coping Strategies of Family Members of Patients in Adult Intensive Care Unit) , National Yang-Ming University Institute of Clinical Nursing Master Thesis, January, 2002.